

Abstract
A gastrointestinal fistula is a common occurrence, especially after surgery. Patients who develop a fistula may have an infection, surgically altered anatomy, nutritional deficiency, or organ failure, making surgical revision more difficult. With advancements in flexible endoscopic devices and technology, new endoscopic options are available for the management of gastrointestinal fistulae. Endoscopically deployable stents, endoscopic suturing devices, through-the-scope and over-the-scope clips, sealants, and fistula plugs can be used to treat fistulae. These therapies are even more effective in combination. Despite the inherent challenges in patients with fistulae, endoscopic therapies for treatment of fistulae have demonstrated safety and efficacy, allowing many patients to avoid surgical fistula repair. In this paper, we review the emerging role of endoscopy in the management of gastrointestinal fistulae.
Keywords: Fistula, endoscopy, endoscopic suturing, stent, clip
The first report of a gastrointestinal fistula came in the 1800s when Alexis St. Martin was shot in the chest and abdomen by a musket and developed a gastrocutaneous fistula. He became the subject of Dr William Beaumont’s experiments in gastric physiology. However, it was not possible to treat the fistula with medicine or surgery, so St. Martin had to live with his condition for the remaining 58 years of his life.1 Despite significant advances that have occurred since, the management of gastrointestinal fistulae remains challenging. Because the majority of fistulae result from surgical procedures, the surgeon often makes the diagnosis; however, a multidisciplinary approach is usually required for optimal treatment of gastrointestinal fistulae.
Historically, surgery was the sole option for management of gastrointestinal fistulae, but it is associated with high morbidity and mortality.2 Medical management has emerged as an important adjunct, and, recently, interventional radiology has taken a prominent role in the management of these complex patients.3 As flexible endoscopic technology has improved and new endoscopic devices have been developed, endoscopists are expanding their role in the management of gastrointestinal fistulae. Endoscopically deployable stents, endoscopic suturing devices, through-the-scope (TTS) and over-the-scope (OTS) clips, sealants, fistula plugs, and vacuum sponges are among the technologies currently being used to treat fistulae. These therapies allow many patients to avoid surgical fistula repair. In this paper, we will review the emerging role of endoscopy in the management of gastrointestinal fistulae.
Definition and Classification
Fistulae can be internal or external. External fistulae involve a communication between the gastrointestinal tract and skin, whereas internal fistulae connect the gastrointestinal tract to the peritoneal space, retroperitoneal space, thorax, or another internal area.4
Fistulae are classified by etiology, anatomy (origin and ending site), and fluid output (low is <500 mL/day and high is >500 mL/day).5 End fistulae are distinguished from lateral (side) fistulae. End fistulae have complete loss of continuity of the gastrointestinal tract beyond themselves and require surgical repair. Complex fistulae are multiple connected fistulae arising from different organs.
Etiology
The majority of fistulae develop after surgical procedures (75%-85%).4 The rate of fistulization or leak varies dramatically among surgical procedures: pancreaticoduodenectomy has a rate of 5% to 8%; liver transplantation, 2% to 9%; choledochoduodenostomy, 5% to 19%; total gastrectomy, 0% to 28%; esophagectomy, 2%; elective colectomy, 5%; laparoscopic Roux-en-Y gastric bypass (RYGB), 2% to 5%; open RYGB, 2% to 3%; and sleeve gastrectomy, 5%.6,7 The remaining 15% to 25% of fistulae form without surgical intervention; other causes include inflammatory bowel disease, diverticulosis, malignancy, and radiation therapy. A gunshot or stab wound, blunt trauma, or other types of trauma can also lead to fistulae.5
Endoscopic Management
Localization and Preparation
Localization of the fistula opening may be challenging, though imaging can help. A gastrocutaneous fistula with a drain in place can be localized using methylene blue.8 If an external drain is in place, it can be submerged under water. Carbon dioxide insufflated through the endoscope should produce bubbles from the drain. Next, methylene blue and radiopaque contrast can be injected into the drain for endoscopic and fluoroscopic visualization of the fistula tract and opening. The anatomy of the gastrointestinal tract surrounding the fistula opening is an important determinant of the optimal therapy for fistula closure. Stents, for example, are not likely to be effective for treatment of a fistula in a recessed area, such as the blind portion of the Roux limb.9 In preparation for fistula closure, foreign bodies should be removed from the fistula tract, and distal stenoses should be dilated.
Sealants
Fibrin sealant, a biodegradable compound, has been used in surgery for attachment of skin grafts, colostomy closure, hemostasis, and even prevention of gastrointestinal fistulae.10 Fibrin sealant can block the passage of gastrointestinal contents through the fistula and can promote cellular migration, angiogenesis, and tissue repair via fibroblast and keratinocyte growth.
Endoscopic application of fibrin sealant can be performed via a catheter.9 After excoriating granulation tissue that has formed over the opening of the fistula, argon plasma coagulation (APC) should be used to ablate the tissue surrounding the fistula opening. Endoscopic application of fibrin can be performed using a double-lumen catheter. However, a rapid-exchange catheter is unsuitable, as it may allow leakage inside the instrument channel. If this type of catheter is used, the more viscous component should be inserted through the catheter’s larger-diameter lumen. Care must be taken when applying fibrin sealant, as the 2 components have different viscosities and will pass through the catheter at different rates. The amount of adhesive needed depends on the size of the fistula. Multiple applications are sometimes required.
Multiple studies have evaluated the efficacy of fibrin sealant for treating gastrointestinal fistulae. In a series of 52 patients, Lippert and colleagues reported success in 36.5% with fibrin alone, and 55.7% were cured with additional endoscopic therapy.11 Success was more likely in patients without an infection. Avalos-González and colleagues evaluated 70 patients with postoperative enterocutaneous fistulae, with 23 patients undergoing fibrin sealant treatment vs 47 controls.12 Patients in the fibrin group experienced fistula closure in 12.5±14.2 days vs 32.5±17.9 days for controls (P<.001). Furthermore, morbidity from nutritional support was significantly reduced in the fibrin group (8.6% vs 42.5%; P<.01). Papavramidis and colleagues reported use of fibrin sealant in patients developing high-output fistulae after bariatric surgery.13 Of 96 patients, 6 developed fistulae and 4 were treated with fibrin sealant. All patients who were treated with fibrin glue experienced healing of their fistula in 15 to 26 days. Rábago and colleagues examined the use of endoscopically delivered fibrin sealant in 15 patients with gastrointestinal fistulae and reported an 86.6% healing rate.14 Patients required an average of 2.5 treatments and 16 days for fistula closure. Success was more frequent in low-output fistulae.
Kowalski and colleagues examined 354 consecutive RYGB patients and reported that 8 had developed a fistula requiring treatment.15 Of these fistulae, 3 were unstable and required immediate surgery, whereas the remaining 5 were treated with fibrin sealant. Of these, 4 required a single treatment, whereas 1 required 2 treatments. Patients treated endoscopically had a mean hospital stay of 13.5 days vs 66.5 days for surgically treated patients. Hwang and colleagues treated 13 patients with gastrointestinal fistulae that were unresponsive to 2 to 4 weeks of conservative therapy; 6 underwent injection of fibrin glue, whereas 7 received only total parenteral nutrition (TPN) therapy.16 All patients in the fibrin group experienced fistula closure within 4 days vs 7 to 21 days for the TPN group (P<.01). Böhm and colleagues examined adding a mesh (Vicryl, Ethicon) when injecting fibrin glue in 15 patients with fistulae after esophagectomy or gastrectomy and reported an 87% closure rate.17 After covering the defect with mesh, fibrin was injected into the submucosa at the edges of the defect. Wong and colleagues reported a 100% successful treatment rate of fistulae in 9 patients with injection of fibrin glue into the fistulous tract using a 5-mm choledochoscope and, when needed, irrigation or debridement.18 Closure was achieved in a mean of 18.7 days and was maintained in all patients for the following year.
Large prospective trials of fibrin sealant are necessary to confirm its usefulness in the treatment of gastrointestinal fistulae. Further research could elucidate which types of fistulae are most amenable to treatment with fibrin sealant. At this time, endoscopic treatment of gastrointestinal fistulae with fibrin sealant appears to be safe and effective.
Stent Placement
Endoscopic placement of self-expanding stents allows exclusion of gastrointestinal contents from fistulae and permits healing while enteral nutrition is resumed.19 Covered self-expanding metal stents (SEMS) and self-expanding plastic stents (SEPS) have been studied for the treatment of fistulae.
After endoscopic identification of the fistula opening and fluoroscopic confirmation, the stent is deployed to exclude the fistula. In the esophagus, the stent should be deployed below the upper esophageal sphincter to avoid inducing globus. The distal end should not impact the enteral wall. Once the stent is deployed, its position can be adjusted with forceps, and it can be clipped or sutured into place.20 Beyond 8 weeks, stent removal can become challenging. When stents cannot be removed with forceps due to tissue ingrowth, APC may be needed to fulgurate tissue to facilitate stent removal. Placement of SEPS within metal stents for 1 week can induce necrosis of tissue ingrowth and ease subsequent stent removal.7 Other complications of stent placement include pain, occlusion, migration, perforation, bleeding, aspiration, and inadequate exclusion of the defect. Esophageal stents may be complicated by tracheoesophageal fistulae and reflux.21
SEMS and SEPS have been studied extensively in the treatment of gastrointestinal fistulae and leaks. Swinnen and colleagues examined 88 patients treated with a total of 135 partially covered SEMS for the treatment of benign esophageal leaks.22 Stent treatment was initially successful in 77.6% of patients, and prolonged endoscopic treatment with additional stenting and adjunctive treatments raised the success rate to 84.6%. The authors typically placed plastic stents within metal stents for 1 to 3 weeks to induce tissue necrosis and facilitate removal, which was successful in 97.8% of cases. Major complications, including bleeding, perforation, and tracheal compression, occurred in 5.9% of patients, and stent migration occurred in 11.1%. Eisendrath and colleagues evaluated stent placement for the treatment of fistulae in 21 patients following bariatric surgery.7 The overall closure rate was 81%, although adjunctive endoscopic treatments were required in 4 patients. Treatment of anastomotic fistulae was 100% effective, whereas treatment of gastrocutaneous fistulae was only 60% effective. Three patients required surgical reintervention and died during follow-up, while a fourth patient died of pulmonary embolism. Reported minor complications included thoracic pain, dysphagia requiring balloon dilation, stent migration, and esophageal strictures. Tuebergen and colleagues studied 32 patients with postsurgical esophageal leaks that were treated with partially covered SEMS.23 Functional closure was successful in 78% of patients, although mortality in this group remained high at 15.6%.
Hünerbein and colleagues studied postesophagectomy patients with esophagogastric leaks.24 The use of SEPS in 9 patients resulted in decreased mortality, intensive care unit stay, total hospital stay, and time to oral feeding compared with standard therapy in 10 patients. Langer and colleagues examined 24 patients with postsurgical anastomotic leaks and found that SEPS were effective in closure in 89% of patients.25 Freeman and colleagues used SEPS to treat 21 postoperative esophageal leak patients and found successful leak closure in 95%.26 Nowakowski and colleagues reported successful fistula closure with covered SEMS in 6 patients after esophagogastrostomy and esophagoenterostomy.27 A meta-analysis of 7 studies using SEMS and SEPS for the treatment of leaks after bariatric surgery found leak closure in 87.8%, and only 9% of patients required surgical revision.28 The pooled proportion for stent migration was 16.9%. Therefore, endoscopic stent placement appears to be safe and effective for the treatment of gastrointestinal fistulae and leaks. Further studies with novel stent types are ongoing.
Endoscopic Suturing
Novel suturing devices have made endoscopic apposition of tissue possible.29 Intraluminal closure of gastrointestinal fistulae is one potential use of these devices. However, procedural complexity and the need for specialized technical skills have limited its adoption.
Sutured fistula closure is especially applicable in the treatment of fistulae that develop after bariatric surgery. After RYGB, patients can develop fistulae between the surgically created gastric pouch and the defunctionalized gastric remnant. This can result in reflux of acid into the pouch, causing gastroesophageal reflux or marginal ulceration.6 The return of weight can also occur as food is diverted into the gastric remnant. Chronic gastrogastric fistulae occur more commonly with the open approach, when the pouch is contiguous with the excluded stomach.30
Fernandez-Esparrach and colleagues reported on the use of endoluminal gastroplication (EndoCinch, CR Bard) for gastrogastric fistula repair after RYGB.31 APC was used to ablate the margin tissue surrounding the fistula opening. Most fistulae were treated with fibrin glue after sutured closure. Although the initial success rate was 95%, only 35% of fistulae remained closed, and no fistula with an aperture greater than 20 mm remained closed. There was 1 episode of significant bleeding and 1 esophageal perforation. The endoluminal gastroplication device placed superficially thick stitches, which may have resulted in the failure of fistula closure. A new endoscopic suturing system (OverStitch, Apollo Endosurgery), which creates full-thickness plications, showed early success in an abstract presented by Watson and Thompson; durable closure was achieved in 3 of 7 gastrogastric fistulae (Figure 1), and no complications were noted.32 This technique is promising, as both morbidity and cost are far lower than with surgical revision. Further research is ongoing to determine closure rates after full-thickness sutured fistula closure.
Figure 1.
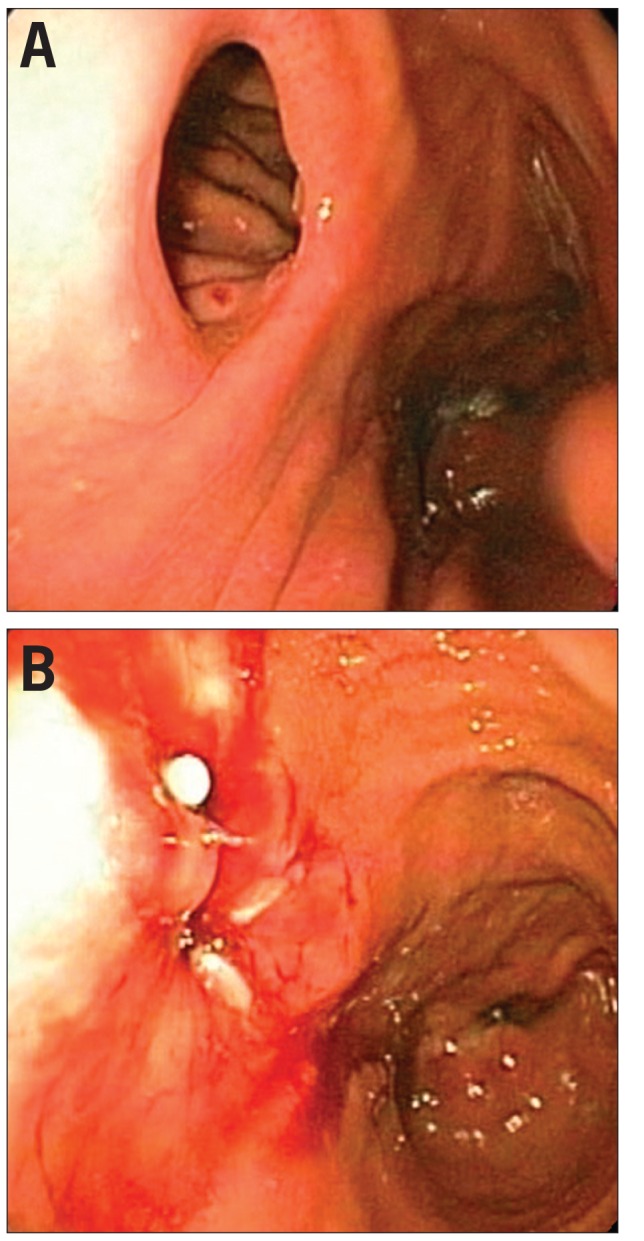
A gastrogastric fistula before (A) and after (B) endoscopic sutured closure.
Reprinted from Clinical Gastroenterology and Hepatology, volume 11, Kumar N, Thompson CC, Endoscopic management of complications after gastrointestinal weight loss surgery, pages 343-353, copyright 2013, with permission from Elsevier
Endoscopic Clips
Endoscopic clips are available in various shapes and sizes and can be deployed either TTS or OTS. TTS clips are primarily used for hemostasis in the management of gastrointestinal bleeding but have been studied for multiple other uses in the gastrointestinal tract.33,34
TTS clips are comprised of 2 arms that form a 10- to 12-mm wide span when open. The clips are placed across the fistula opening under endoscopic guidance and deployed in a configuration perpendicular to the defect’s long axis to approximate its edges. Multiple clips can be deployed sequentially from the edges to the center. Thermal ablation or scraping around the defect prior to apposition results in more durable closure.35
Rodella and colleagues described the use of endoscopic clips for the closure of fistulae (ranging from 1 to 2 cm in size) in 7 patients after gastric surgery.36 Fistula closure was successful in all 7 patients, with a mean follow-up of 9.6 months. Five patients needed 1 endoscopic session, 1 patient needed 2 sessions, and another patient needed 3 sessions. Raymer and colleagues described successful closure of esophageal fistulae with endoscopic clipping in 3 consecutive patients.37 Additional literature has shown that endoscopic clipping can be effective for treating iatrogenic perforation, such as that seen during endoscopic procedures.38 However, the limited strength and capability of TTS clips make them less useful for closing large fistulae.
To overcome the limitations of TTS clips, the over-the-scope clip (OTSC, Ovesco Endoscopy) was developed, which is larger in size and applies higher force. This clip is mounted on a plastic cap that is secured to the endoscope tip. The tissue surrounding the fistula opening is suctioned into the cap at the endoscope tip, and then the nitinol OTSC is deployed.39 The clip apposes and traps all tissue that lies between its arms (Figure 2). The larger size and additional force application of these arms better permit closure of larger mucosal defects compared with TTS clips. Unlike TTS clips, the OTSC can be used for full-thickness apposition.40 Closure of a gastrogastric fistula is shown in Figure 3.
Figure 2.
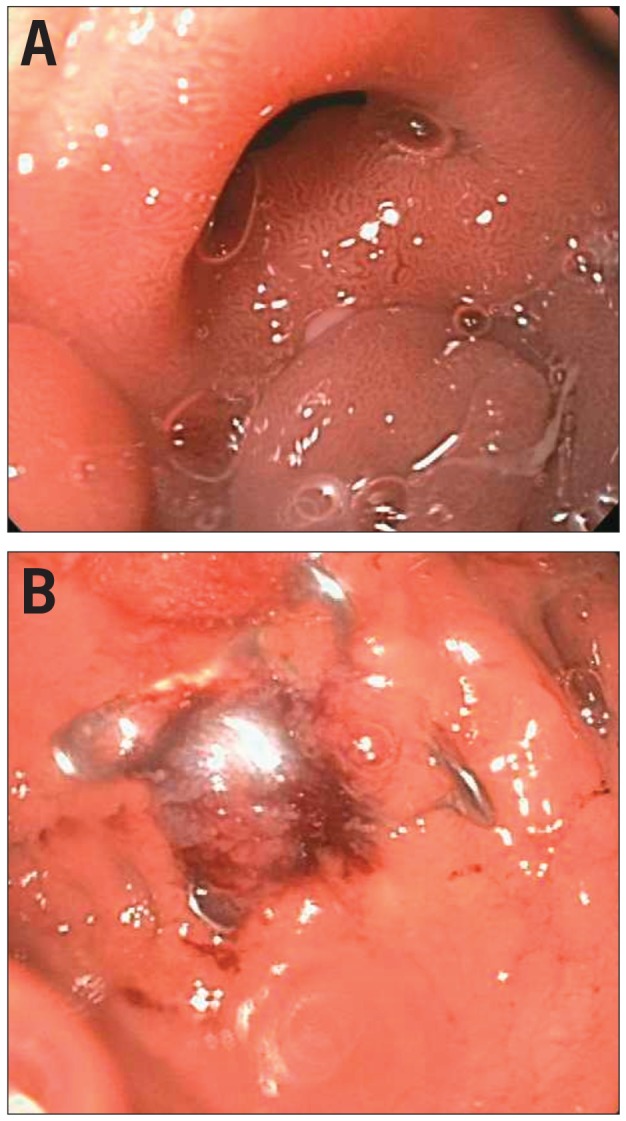
A fistula before (A) and after (B) using the over-the-scope clip.
Figure 3.
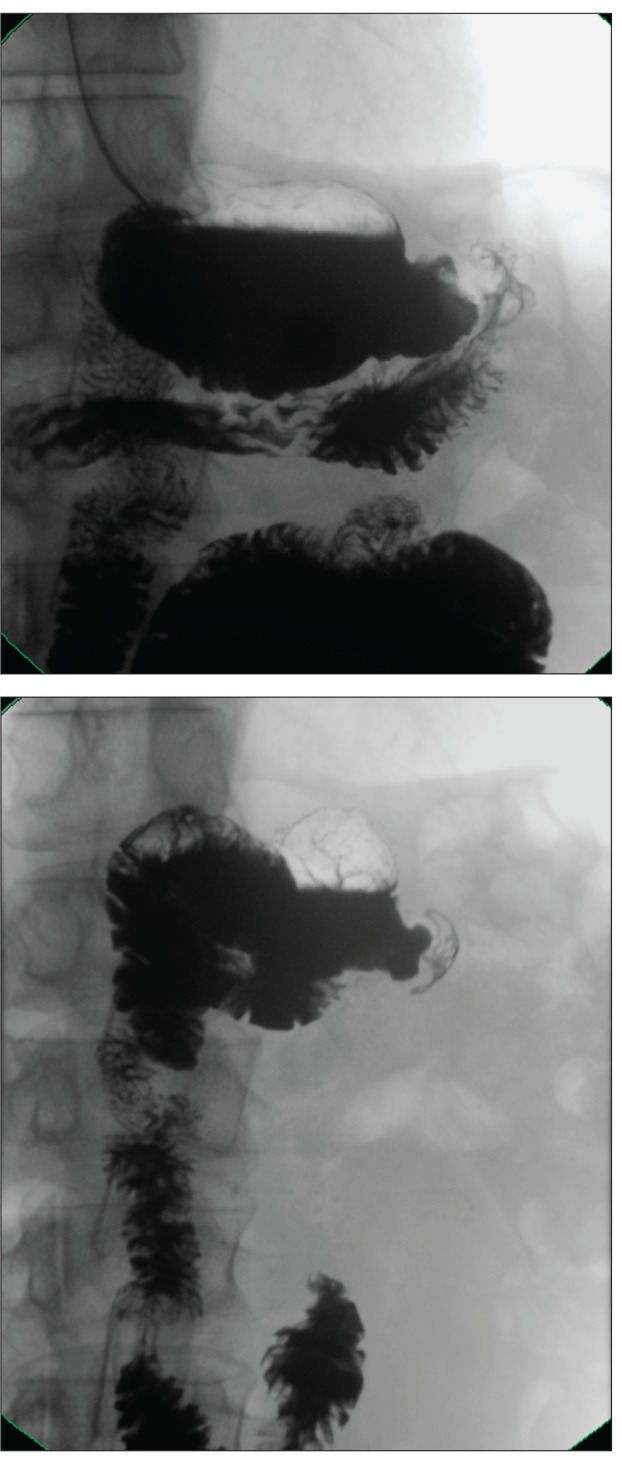
An upper gastrointestinal series demonstrating closure of the same gastrogastric fistula with the over-the-scope clip.
Reprinted from Clinical Gastroenterology and Hepatology, volume 11, Kumar N, Thompson CC, Endoscopic management of complications after gastrointestinal weight loss surgery, pages 343-353, copyright 2013, with permission from Elsevier
In case series, the OTSC has demonstrated closure rates of 72% to 91% for gastrointestinal fistulae.39,41,42 In case reports, this clip has been successful at closing gastrocolic, gastrocutaneous, choledochoduodenal, duodenal, and tracheoesophageal fistulae; fistulae following percutaneous endoscopic gastrostomy; postoperative esophageal leaks; and gastric fistulae following sleeve gastrectomy or gastric band penetration.43-51 It appears that the OTSC is more effective at closing acute gastrointestinal fistulae and leaks rather than chronic fistulae, which generally involve chronic fibrotic changes and scarring. Further research is necessary to understand the fistula types that are most responsive to this clip and to compare it to other treatments for gastrointestinal fistulae.
Fistula Plugs
The anal fistula plug (Surgisis AFP, Cook Biotech) is made from acellular fibrogenic matrix, which prevents inflammatory foreign-body reactions (Figure 4). This device was developed for the treatment of anorectal fistulae and has performed better than fibrin sealant in that role.52,53 Endoscopic insertion for the treatment of gastrocutaneous fistulae begins with fluoroscopic localization of the fistula tract with contrast injection. A guidewire is inserted into the external fistula opening and advanced through the fistula tract under fluoroscopic guidance until it is visualized endoscopically. The end of the wire is grasped with a snare and pulled out through the mouth. The fistula tract can be abraded over the guidewire until bleeding occurs. Next, a snare is attached to the guidewire and passed through the fistula to the outside. The snare is used to grasp the narrower end of the fistula plug, which is pulled into the fistula tract and released. Multiple plugs may be needed to occlude large-bore fistulae.
Figure 4.
A fistula plug.
Reprinted from Song KH. New techniques for treating an anal fistula. J Korean Soc Coloproctol. 2012;28(1):7-12
Table.
Comparison of Endoscopic Fistula Closure Techniques
| Advantage(s) | Disadvantage(s) | |
|---|---|---|
| Sealant | Easily placed; can be used more than once | Rarely successful as monotherapy |
| Stent | Easily placed | Chance of migration and/or ulceration; limited by gastrointestinal tract geometry |
| Suturing | Can be applied at complex gastrointestinal tract geometry | Technically demanding; must be within reach of double-channel endoscope |
| Clip | Easily applied | Limited to smaller openings |
| Plug | Easily placed | Requires cutaneous opening |
| Sponge | Noninvasive; can be customized for leak cavity | Requires external drainage, monitoring, and repeat procedures |
Toussaint and colleagues reported on the treatment of 5 postsurgical enterocutaneous fistulae, of which 4 healed.54 Two closed with a single procedure, and 2 required a second procedure. SEMS were placed in some patients to cover the fistula tracts once the fistula plug was inserted. A larger study demonstrated the use of Surgisis strips and fistula plugs to treat gastrocutaneous fistulae in 25 patients after RYGB.55 The plugs were deployed in 5 patients (as above), and the strips were inserted via polypectomy snare into the lumenal opening of the fistulae of 20 patients. Closure was achieved in all patients with plugs and in 75% of patients treated with strips.
Vacuum Closure
Vacuum-assisted sponge closure is an emerging technique that has demonstrated effectiveness in the closure of postsurgical leaks. This device is comprised of an open-cell sponge and a tube attached to external vacuum suction (Figure 5). The suction improves perfusion and removes secretions, while the sponge induces formation of granulation tissue.56 A standard feeding tube is inserted trans-nasally and then is externalized through the mouth. The sponge, which has been cut to be smaller than the fistula cavity, is sutured to the tip of the feeding tube. Endoscopic forceps are used to grasp the sponge, and the endoscope is advanced to the internal defect. The sponge is placed within the tract, and the feeding tube is connected to continuous vacuum suction. The sponge should be changed every 3 to 4 days. This vacuum sponge method has been successfully used to close rectal anastomotic leaks.57,58 It was successful for the treatment of intrathoracic anastomotic leaks in a prospective trial; closure was achieved in 7 of 8 patients at an average of 23 days.59 Ahrens and colleagues demonstrated closure of gastroesophageal anastomotic leaks in all 5 study participants at a median of 42 days with an average of 9 sponge changes.60 Two patients developed stenosis requiring dilation, and 1 patient experienced a hemorrhage following dilation.
Figure 5.

A sponge used for vacuum sponge closure.
Reprinted from Gastrointestinal Endoscopy, volume 67, Wedemeyer J, Schneider A, Manns MP, Jackobs S, Endoscopic vacuum-assisted closure of upper intestinal anastomotic leaks, pages 708-711, copyright 2008, with permission from Elsevier
Conclusion
Gastrointestinal fistulae are a common occurrence after surgery, but surgical revision is associated with high morbidity. Patients with fistulae may already have concurrent infection, nutritional deficiency, or organ failure, making surgical revision more difficult. Despite the inherent challenges in this patient population, endoscopic therapies for fistula closure have demonstrated safety and efficacy. These techniques can be used alone but are even more effective when used in combination. The relative advantages and disadvantages of these techniques are listed in the Table. Further research is ongoing to determine which fistula types are most suitable for a specific endoscopic therapy. As evidence builds for the efficacy of these endoscopic techniques relative to surgical management, gastroenterologists will play a more prominent role in the treatment of gastrointestinal fistulae.
Footnotes
Dr Kumar and Dr Larsen have no relevant conflicts of interest to disclose. Dr Thompson is a consultant for Olympus, Bard (Davol), Boston Scientific, and Apollo Endosurgery.
References
- 1.Rutkow IM. Beaumont and St Martin: a blast from the past. Arch Surg. 1998;133(11):1259. doi: 10.1001/archsurg.133.11.1259. [DOI] [PubMed] [Google Scholar]
- 2.Schecter WP, Hirshberg A, Chang DS, et al. Enteric fistulas: principles of management. J Am Coll Surg. 2009;209(4):484–491. doi: 10.1016/j.jamcollsurg.2009.05.025. [DOI] [PubMed] [Google Scholar]
- 3.Kwon SH, Oh JH, Kim HJ, Park SJ, Park HC. Interventional management of gastrointestinal fistulas. Korean J Radiol. 2008;9(6):541–549. doi: 10.3348/kjr.2008.9.6.541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Falconi M, Pederzoli P. The relevance of gastrointestinal fistulae in clinical practice: a review. Gut. 2001;49;(suppl 4):iv2–iv10. doi: 10.1136/gut.49.suppl_4.iv2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.González-Pinto I, González EM. Optimising the treatment of upper gastrointestinal fistulae. Gut. 2001;49(suppl 4):iv22–iv31. doi: 10.1136/gut.49.suppl_4.iv21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Elder KA, Wolfe BM. Bariatric surgery: a review of procedures and outcomes. Gastroenterology. 2007;132(6):2253–2271. doi: 10.1053/j.gastro.2007.03.057. [DOI] [PubMed] [Google Scholar]
- 7.Eisendrath P, Cremer M, Himpens J, Cadière GB, Le Moine O, Devière J. Endotherapy including temporary stenting of fistulas of the upper gastrointestinal tract after laparoscopic bariatric surgery. Endoscopy. 2007;39(7):625–630. doi: 10.1055/s-2007-966533. [DOI] [PubMed] [Google Scholar]
- 8.Kumar N, Thompson CC. Endoscopic management of complications after gastrointestinal weight loss surgery. Clin Gastroenterol Hepatol. 2013;11(4):343–353. doi: 10.1016/j.cgh.2012.10.043. [DOI] [PubMed] [Google Scholar]
- 9.Kumar N, Thompson CC. Endoscopic therapy for postoperative leaks and fistulae. Gastrointest Endosc Clin N Am. 2013;23(1):123–136. doi: 10.1016/j.giec.2012.10.002. [DOI] [PubMed] [Google Scholar]
- 10.Silecchia G, Boru CE, Mouiel J, et al. Clinical evaluation of fibrin glue in the prevention of anastomotic leak and internal hernia after laparoscopic gastric bypass: preliminary results of a prospective, randomized multicenter trial. Obes Surg. 2006;16(2):125–131. doi: 10.1381/096089206775565249. [DOI] [PubMed] [Google Scholar]
- 11.Lippert E, Klebl FH, Schweller F, et al. Fibrin glue in the endoscopic treatment of fistulae and anastomotic leakages of the gastrointestinal tract. Int J Colorectal Dis. 2011;26(3):303–311. doi: 10.1007/s00384-010-1104-5. [DOI] [PubMed] [Google Scholar]
- 12.Avalos-González J, Portilla-deBuen E, Leal-Cortés CA, et al. Reduction of the closure time of postoperative enterocutaneous fistulas with fibrin sealant. World J Gastroenterol. 2010;16(22):2793–2800. doi: 10.3748/wjg.v16.i22.2793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Papavramidis TS, Kotzampassi K, Kotidis E, Eleftheriadis EE, Papavramidis ST. Endoscopic fibrin sealing of gastrocutaneous fistulas after sleeve gastrectomy and biliopancreatic diversion with duodenal switch. J Gastroenterol Hepatol. 2008;23(12):1802–1805. doi: 10.1111/j.1440-1746.2008.05545.x. [DOI] [PubMed] [Google Scholar]
- 14.Rábago LR, Ventosa N, Castro JL, Marco J, Herrera N, Gea F. Endoscopic treatment of postoperative fistulas resistant to conservative management using biological fibrin glue. Endoscopy. 2002;34(8):632–638. doi: 10.1055/s-2002-33237. [DOI] [PubMed] [Google Scholar]
- 15.Kowalski C, Kastuar S, Mehta V, Brolin RE. Endoscopic injection of fibrin sealant in repair of gastrojejunostomy leak after laparoscopic Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2007;3(4):438–442. doi: 10.1016/j.soard.2007.02.012. [DOI] [PubMed] [Google Scholar]
- 16.Hwang TL, Chen MF. Randomized trial of fibrin tissue glue for low output enterocutaneous fistula. Br J Surg. 1996;83(1):112. doi: 10.1002/bjs.1800830135. [DOI] [PubMed] [Google Scholar]
- 17.Böhm G, Mossdorf A, Klink C, et al. Treatment algorithm for postoperative upper gastrointestinal fistulas and leaks using combined vicryl plug and fibrin glue. Endoscopy. 2010;42(7):599–602. doi: 10.1055/s-0029-1244165. [DOI] [PubMed] [Google Scholar]
- 18.Wong SK, Lam YH, Lau JY, Lee DW, Chan AC, Chung SC. Diagnostic and therapeutic fistuloscopy: an adjuvant management in postoperative fistulas and abscesses after upper gastrointestinal surgery. Endoscopy. 2000;32(4):311–313. doi: 10.1055/s-2000-7378. [DOI] [PubMed] [Google Scholar]
- 19.Morales MP, Miedema BW, Scott JS, de la Torre RA. Management of postsurgical leaks in the bariatric patient. Gastrointest Endosc Clin N Am. 2011;21(2):295–304. doi: 10.1016/j.giec.2011.02.008. [DOI] [PubMed] [Google Scholar]
- 20.Vanbiervliet G, Filippi J, Karimdjee BS, et al. The role of clips in preventing migration of fully covered metallic esophageal stents: a pilot comparative study. Surg Endosc. 2012;26(1):53–59. doi: 10.1007/s00464-011-1827-6. [DOI] [PubMed] [Google Scholar]
- 21.de Wijkerslooth LR, Vleggaar FP, Siersema PD. Endoscopic management of difficult or recurrent esophageal strictures. Am J Gastroenterol. 2011;106(12):2080–2091. 2092. doi: 10.1038/ajg.2011.348. quiz. [DOI] [PubMed] [Google Scholar]
- 22.Swinnen J, Eisendrath P, Rigaux J, et al. Self-expandable metal stents for the treatment of benign upper GI leaks and perforations. Gastrointest Endosc. 2011;73(5):890–899. doi: 10.1016/j.gie.2010.12.019. [DOI] [PubMed] [Google Scholar]
- 23.Tuebergen D, Rijcken E, Mennigen R, Hopkins AM, Senninger N, Bruewer M. Treatment of thoracic esophageal anastomotic leaks and esophageal perforations with endoluminal stents: efficacy and current limitations. J Gastrointest Surg. 2008;12(7):1168–1176. doi: 10.1007/s11605-008-0500-4. [DOI] [PubMed] [Google Scholar]
- 24.Hünerbein M, Stroszczynski C, Moesta KT, Schlag PM. Treatment of thoracic anastomotic leaks after esophagectomy with self-expanding plastic stents. Ann Surg. 2004;240(5):801–807. doi: 10.1097/01.sla.0000143122.76666.ae. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Langer FB, Wenzl E, Prager G, et al. Management of postoperative esophageal leaks with the Polyflex self-expanding covered plastic stent. Ann Thorac Surg. 2005;79(2):398–403. doi: 10.1016/j.athoracsur.2004.07.006. discussion 404. [DOI] [PubMed] [Google Scholar]
- 26.Freeman RK, Ascioti AJ, Wozniak TC. Postoperative esophageal leak management with the Polyflex esophageal stent. J Thorac Cardiovasc Surg. 2007;133(2):333–338. doi: 10.1016/j.jtcvs.2006.10.008. [DOI] [PubMed] [Google Scholar]
- 27.Nowakowski P, Ziaja K, Ludyga T, et al. Self-expandable metallic stents in the treatment of post-esophagogastrostomy/post-esophagoenterostomy fistula. Dis Esophagus. 2007;20(4):358–360. doi: 10.1111/j.1442-2050.2007.00688.x. [DOI] [PubMed] [Google Scholar]
- 28.Puli SR, Spofford IS, Thompson CC. Use of self-expandable stents in the treatment of bariatric surgery leaks: a systematic review and meta-analysis. Gastrointest Endosc. 2012;75(2):287–293. doi: 10.1016/j.gie.2011.09.010. [DOI] [PubMed] [Google Scholar]
- 29.Kumar N, Thompson CC. A novel method for endoscopic perforation management by using abdominal exploration and full-thickness sutured closure. Gastrointest Endosc. 2014;80(1):156–161. doi: 10.1016/j.gie.2014.02.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Lee S, Carmody B, Wolfe L, et al. Effect of location and speed of diagnosis on anastomotic leak outcomes in 3828 gastric bypass cases. J Gastrointest Surg. 2007;11(6):708–713. doi: 10.1007/s11605-007-0085-3. [DOI] [PubMed] [Google Scholar]
- 31.Fernandez-Esparrach G, Lautz DB, Thompson CC. Endoscopic repair of gastrogastric fistula after Roux-en-Y gastric bypass: a less-invasive approach. Surg Obes Relat Dis. 2010;6(3):282–288. doi: 10.1016/j.soard.2010.02.036. [DOI] [PubMed] [Google Scholar]
- 32.Watson RR, Thompson CC. Applications of a novel endoscopic suturing device in the GI tract [abstract] Gastrointest Endosc. 2011;73(4):AB105. [Google Scholar]
- 33.Cipolletta L, Bianco MA, Marmo R, et al. Endoclips vs heater probe in preventing early recurrent bleeding from peptic ulcer: a prospective and randomized trial. Gastrointest Endosc. 2001;53(2):147–151. doi: 10.1067/mge.2001.111386. [DOI] [PubMed] [Google Scholar]
- 34.Gevers AM, De Goede E, Simoens M, Hiele M, Rutgeerts P. A randomized trial comparing injection therapy with hemoclip and with injection combined with hemoclip for bleeding ulcers. Gastrointest Endosc. 2002;55(4):466–469. doi: 10.1067/mge.2002.112613. [DOI] [PubMed] [Google Scholar]
- 35.Felsher J, Farres H, Chand B, Farver C, Ponsky J. Mucosal apposition in endoscopic suturing. Gastrointest Endosc. 2003;58(6):867–870. doi: 10.1016/s0016-5107(03)02312-5. [DOI] [PubMed] [Google Scholar]
- 36.Rodella L, Laterza E, De Manzoni G, et al. Endoscopic clipping of anastomotic leakages in esophagogastric surgery. Endoscopy. 1998;30(5):453–456. doi: 10.1055/s-2007-1001307. [DOI] [PubMed] [Google Scholar]
- 37.Raymer GS, Sadana A, Campbell DB, Rowe WA. Endoscopic clip application as an adjunct to closure of mature esophageal perforation with fistulae. Clin Gastroenterol Hepatol. 2003;1(1):44–50. doi: 10.1053/jcgh.2003.50007. [DOI] [PubMed] [Google Scholar]
- 38.Mangiavillano B, Viaggi P, Masci E. Endoscopic closure of acute iatrogenic perforations during diagnostic and therapeutic endoscopy in the gastrointestinal tract using metallic clips: a literature review. J Dig Dis. 2010;11(1):12–18. doi: 10.1111/j.1751-2980.2009.00414.x. [DOI] [PubMed] [Google Scholar]
- 39.Surace M, Mercky P, Demarquay JF, et al. Endoscopic management of GI fistulae with the over-the-scope clip system (with video) Gastrointest Endosc. 2011;74(6):1416–1419. doi: 10.1016/j.gie.2011.08.011. [DOI] [PubMed] [Google Scholar]
- 40.von Renteln D, Denzer UW, Schachschal G, Anders M, Groth S, Rösch T. Endoscopic closure of GI fistulae by using an over-the-scope clip (with videos) Gastrointest Endosc. 2010;72(6):1289–1296. doi: 10.1016/j.gie.2010.07.033. [DOI] [PubMed] [Google Scholar]
- 41.Parodi A, Repici A, Pedroni A, Blanchi S, Conio M. Endoscopic management of GI perforations with a new over-the-scope clip device (with videos) Gastrointest Endosc. 2010;72(4):881–886. doi: 10.1016/j.gie.2010.04.006. [DOI] [PubMed] [Google Scholar]
- 42.Manta R, Manno M, Bertani H, et al. Endoscopic treatment of gastrointestinal fistulas using an over-the-scope clip (OTSC) device: case series from a tertiary referral center. Endoscopy. 2011;43(6):545–548. doi: 10.1055/s-0030-1256196. [DOI] [PubMed] [Google Scholar]
- 43.Murino A, Despott EJ, Vaizey C, et al. First report of endoscopic closure of a gastrocolic fistula using an over-the-scope clip system (with video) Gastrointest Endosc. 2012;75(4):893–894. doi: 10.1016/j.gie.2011.12.013. discussion 894. [DOI] [PubMed] [Google Scholar]
- 44.Kouklakis G, Zezos P, Liratzopoulos N, et al. Endoscopic treatment of a gastrocutaneous fistula using the over-the-scope-clip system: a case report. Diagn Ther Endosc. 2011;2011:384143. doi: 10.1155/2011/384143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Neumann H, Nägel A, Bernatik T, Wickles N, Neurath MF, Raithel M. Endoscopic closure of large, spontaneous, choledochoduodenal fistula by using an over-the-scope clip. Gastrointest Endosc. 2011;74(1):200–202. doi: 10.1016/j.gie.2011.01.057. discussion 202. [DOI] [PubMed] [Google Scholar]
- 46.Bini R, Coppola F, Recchia S, Fusca M, Gaia S, Leli R. Endoscopic treatment of postgastrectomy duodenal fistula with an over-the-scope clip. Surg Innov. 2011;18(1):102–104. doi: 10.1177/1553350610392244. [DOI] [PubMed] [Google Scholar]
- 47.Iacopini F, Di Lorenzo N, Altorio F, Schurr MO, Scozzarro A. Over-the-scope clip closure of two chronic fistulas after gastric band penetration. World J Gastroenterol. 2010;16(13):1665–1669. doi: 10.3748/wjg.v16.i13.1665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Traina M, Curcio G, Tarantino I, et al. New endoscopic over-the-scope clip system for closure of a chronic tracheoesophageal fistula. Endoscopy. 2010;42(suppl 2):E54–E55. doi: 10.1055/s-0029-1243824. [DOI] [PubMed] [Google Scholar]
- 49.Turner JK, Hurley JJ, Ketchell I, Dolwani S. Over-the-scope clip to close a fistula after removing a percutaneous endoscopic gastrostomy tube. Endoscopy. 2010;42(suppl 2):E197–E198. doi: 10.1055/s-0030-1255693. [DOI] [PubMed] [Google Scholar]
- 50.Pohl J, Borgulya M, Lorenz D, Ell C. Endoscopic closure of postoperative esophageal leaks with a novel over-the-scope clip system. Endoscopy. 2010;42(9):757–759. doi: 10.1055/s-0030-1255634. [DOI] [PubMed] [Google Scholar]
- 51.Conio M, Blanchi S, Repici A, Bastardini R, Marinari GM. Use of an over-the-scope clip for endoscopic sealing of a gastric fistula after sleeve gastrectomy. Endoscopy. 2010;42(suppl 2):E71–E72. doi: 10.1055/s-0029-1215199. [DOI] [PubMed] [Google Scholar]
- 52.Champagne BJ, O’Connor LM, Ferguson M, Orangio GR, Schertzer ME, Armstrong DN. Efficacy of anal fistula plug in closure of cryptoglandular fistulas: long-term follow-up. Dis Colon Rectum. 2006;49(12):1817–1821. doi: 10.1007/s10350-006-0755-3. [DOI] [PubMed] [Google Scholar]
- 53.Johnson EK, Gaw JU, Armstrong DN. Efficacy of anal fistula plug vs. fibrin glue in closure of anorectal fistulas. Dis Colon Rectum. 2006;49(3):371–376. doi: 10.1007/s10350-005-0288-1. [DOI] [PubMed] [Google Scholar]
- 54.Toussaint E, Eisendrath P, Kwan V, Dugardeyn S, Devière J, Le Moine O. Endoscopic treatment of postoperative enterocutaneous fistulas after bariatric surgery with the use of a fistula plug: report of five cases. Endoscopy. 2009;41(6):560–563. doi: 10.1055/s-0029-1214606. [DOI] [PubMed] [Google Scholar]
- 55.Maluf-Filho F, Hondo F, Halwan B, de Lima MS, Giordano-Nappi JH, Sakai P. Endoscopic treatment of Roux-en-Y gastric bypass-related gastrocutaneous fistulas using a novel biomaterial. Surg Endosc. 2009;23(7):1541–1545. doi: 10.1007/s00464-009-0440-4. [DOI] [PubMed] [Google Scholar]
- 56.Holle G, Riedel K, von Gregory H, Gazyakan E, Raab N, Germann G. Vacuum-assisted closure therapy. Current status and basic research [in German] Unfallchirurg. 2007;110(6):490–504. doi: 10.1007/s00113-007-1267-x. [DOI] [PubMed] [Google Scholar]
- 57.Weidenhagen R, Gruetzner KU, Wiecken T, Spelsberg F, Jauch KW. Endoscopic vacuum-assisted closure of anastomotic leakage following anterior resection of the rectum: a new method. Surg Endosc. 2008;22(8):1818–1825. doi: 10.1007/s00464-007-9706-x. [DOI] [PubMed] [Google Scholar]
- 58.van Koperen PJ, van Berge Henegouwen MI, Rosman C, et al. The Dutch multicenter experience of the endo-sponge treatment for anastomotic leakage after colorectal surgery. Surg Endosc. 2009;23(6):1379–1383. doi: 10.1007/s00464-008-0186-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Wedemeyer J, Brangewitz M, Kubicka S, et al. Management of major postsurgical gastroesophageal intrathoracic leaks with an endoscopic vacuum-assisted closure system. Gastrointest Endosc. 2010;71(2):382–386. doi: 10.1016/j.gie.2009.07.011. [DOI] [PubMed] [Google Scholar]
- 60.Ahrens M, Schulte T, Egberts J, et al. Drainage of esophageal leakage using endoscopic vacuum therapy: a prospective pilot study. Endoscopy. 2010;42(9):693–698. doi: 10.1055/s-0030-1255688. [DOI] [PubMed] [Google Scholar]