

TO THE EDITOR:
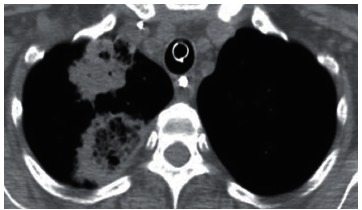
Recent studies conducted in Brazil 1 - 3 have stressed the importance of the reversed halo sign (RHS) in the diagnosis of lung diseases in immunocompetent patients. However, the RHS in immunocompromised patients has not received the same emphasis. Here, we report the case of a 51-year-old female patient who presented with a 10-day history of generalized ecchymosis and weakness. A complete blood count revealed a hemoglobin concentration of 9.0 g/dL, a white blood cell count of 60 × 109/L, a neutrophil count of 1 × 109/L (peripheral blasts, 20%), and a platelet count of 80 × 109/L. A diagnosis of acute leukemia was suspected. A bone marrow biopsy was performed and confirmed a diagnosis of acute myeloid leukemia. Treatment was started with cytarabine and daunorubicin. The patient experienced dry cough and right-sided pleuritic pain during the treatment period. A CT scan of the chest showed a right upper lobe mass with the characteristics of an RHS (Figure 1). Bronchoscopy revealed no abnormalities. Aspergillus fumigatus was isolated by cultures from an open lung biopsy sample. The patient was started on oral voriconazole and responded well to treatment, with symptom improvement and resolution of the pulmonary lesion.
Figure 1. Axial CT image (mediastinal window setting) showing two right upper lobe masses, one of which has the characteristics of the reversed halo sign. The posterior lesion has irregular thickened walls, and a reticular pattern is visible within the reversed halo.
The RHS is a chest CT finding defined as a focal, rounded area of ground-glass opacity surrounded by a nearly complete ring of consolidation. The RHS has been reported in a wide spectrum of diseases, including noninfectious diseases and infectious diseases such as invasive fungal infections (IFIs). 4 , 5 Because of this broad differential diagnosis, the RHS is considered a nonspecific sign. However, certain morphological characteristics of the RHS can aid in establishing a diagnosis. In immunocompromised patients, a reticular pattern within the halo and a thick rim of consolidation are highly suggestive of IFI. 4 , 5
With regard to the reticular RHS, information regarding the immunological status of the patient is fundamental for the differential diagnosis. In immunocompetent patients, the reticular RHS corresponds, as a rule, to pulmonary infarction, usually secondary to thromboembolic disease. Suspicion of infarction from thromboembolic disease requires immediate confirmation by D-dimer testing and CT angiography. In severely immunocompromised patients (e.g., stem cell transplant recipients and patients with hematological malignancy), the reticular RHS is taken to indicate the presence of IFI (in particular, pulmonary zygomycosis or angioinvasive pulmonary aspergillosis), which is treated as such without culture or histological confirmation. Although the final diagnosis should be based on the clinical manifestations, a lung biopsy is required in some cases. 4 , 5
IFIs are associated with high morbidity and mortality. Therefore, patients with IFI should be treated immediately, given that early administration of high-dose antifungal therapy has been associated with improved outcomes. 4 , 5 Diagnosis can be challenging, especially for general radiologists encountering patients outside the context of transplantation centers, and any delay in treatment can significantly increase mortality. In conclusion, a reticular pattern within the RHS and a thick rim of consolidation in an immunocompromised patient are highly suggestive of IFI.
REFERENCES
- 1.Souza AS, Jr, Souza AS, Soares-Souza L, Zanetti G, Marchiori E. Reversed halo sign in acute schistosomiasis. J Bras Pneumol. 2015;41(3):286–288. doi: 10.1590/S1806-37132015000004444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Marchiori E, Zanetti G, Hochhegger B. Reversed halo sign. J Bras Pneumol. 2015;41(6):564–564. doi: 10.1590/S1806-37562015000000235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Queiroz RM, Gomes MP, Valentin MV. Pulmonary paracoccidioidomycosis showing reversed halo sign with nodular/coarse contour. Radiol Bras. 2016;49(1):59–60. doi: 10.1590/0100-3984.2015.0071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Marchiori E, Marom EM, Zanetti G, Hochhegger B, Irion KL, Godoy MC. Reversed halo sign in invasive fungal infections criteria for differentiation from organizing pneumonia. Chest. 2012;142(6):1469–1473. doi: 10.1378/chest.12-0114. [DOI] [PubMed] [Google Scholar]
- 5.Godoy MC, Viswanathan C, Marchiori E, Truong MT, Benveniste MF, Rossi S. The reversed halo sign update and differential diagnosis. Brit J Radiol. 2012;85(1017):1226–1235. doi: 10.1259/bjr/54532316. [DOI] [PMC free article] [PubMed] [Google Scholar]