

Abstract
Elongation of the styloid process occurs in 4–7% of individuals. In the majority this elongation is asymptomatic. Presence of oropharyngeal pain and dysphagia with such elongation is known as Eagle syndrome. The aetiology of Eagle syndrome is believed to be a reactive osseus hyperplasia of the styloid process in response to pharyngeal trauma or surgical intervention, such as tonsillectomy. We present a case of a 72-year-old lady with a twelve month history of left sided oropharyngeal pain and worsening dysphagia, presenting with a long, slender, bony intraoral projection found to be an elongated styloid process. She previously underwent tonsillectomy and radiotherapy on the left side for a tonsillar carcinoma. Surgical reduction of the elongated styloid process via intraoral approach led to immediate post-operative pain relief and normal swallowing. We conclude that this atypical presentation of Eagle syndrome was caused by the patient's prior treatment for tonsillar carcinoma.
INTRODUCTION
The styloid process is described as a slender outgrowth of bone arising from the base of the temporal bone at the junction of the petrous and temporal portions. There has been much debate in the literature on what length is deemed normal. Quoted lengths from published studies vary including:
Elongation of the styloid process was first described in 1652 by Italian surgeon Pietro Marchetti. There have been several studies quoting incidence of elongation. In 1978, Massey reported an incidence rate of 0.55% based on 2000 cranial dissections [5]. Studies by Eagle in 1948 and Harma in 1966 quote an incidence rate of 4–7% [6, 7].
A vast majority of individuals with elongation of the styloid process are asymptomatic. In 1937, Watt Eagle, an otolaryngologist, described a syndrome of clinical signs and symptoms associated with an elongated process. His studies highlighted symptoms of facial pain, ear pain, dysphagia, voice changes and a globus sensation in the throat that prompts frequent swallowing [6, 8]. These symptoms are now referred to as Eagle's syndrome. Murtagh et al. [9] stated 4–10.3% incidence of symptoms in patients with an elongated styloid process. In this case report, we describe an atypical case of Eagle's syndrome presenting with intraoral signs and symptoms.
CASE REPORT
A 72-year-old Caucasian lady presented to the Maxillofacial outpatient clinic via her general practitioner with a 12-month history of tenderness around the left side of the oropharynx. She reported painful swallowing mostly with solid foods and felt it was getting worse. She also reported that she was unable to lie flat due to severe pain. Based on these symptoms, the patient had been diagnosed with gastroesophageal reflux and had been placed on regular proton pump inhibitor (esomeprazole) by her general practitioner. This medication failed to control or improve her symptoms. It was also noted from her medical history that she had previously suffered with a tonsillar carcinoma on the left side and had been treated with surgery and radiotherapy years earlier.
Physical examination revealed an edentulous patient with an irregular red lesion in the left side of the soft palate with a bony hard, slender mass protruding into the mouth covered by mucosa (Fig. 1). There was no evidence of ulceration, induration or any other lesions present in the mouth. Extraoral examination was completely normal with no clinical evidence of cervical lymphadenopathy. An orthopantomogram demonstrated an elongated styloid process.
Figure 1:

Appearance at initial presentation with intraoral projection of styloid process.
The patient was clinically diagnosed with an elongated, medially deflected and symptomatic styloid process. The proposed management plan was for surgical reduction of the protruding process via an intraoral approach.
Under a general anaesthetic, a mucosal incision over the protruding process was made with monopolar diathermy. Periosteal elevators were used to free all the soft tissue attachments off the styloid process (Fig. 2). Once cleared, 2.5 cm of the styloid was removed with a Rongeurs bone nibbling forceps. This was judged clinically to be a sufficient length to clear the oral cavity of any interference from the protruding styloid process. Bleeding was controlled with bipolar-diathermy forceps and the mucosal incision closed with 3.0 vicryl interrupted sutures.
Figure 2:
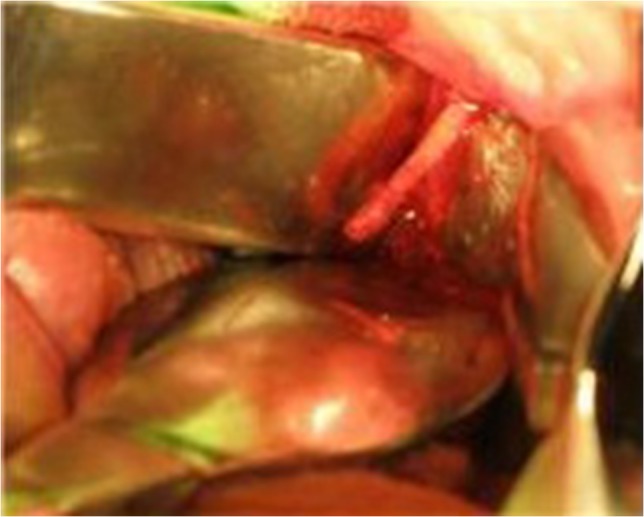
Intraoperative view of the styloid process with the soft tissues reflected.
The patient stayed overnight and was discharged home on the following day. Post operatively she was reviewed after one week and after 6 months following surgery. She reported complete relief of her symptoms and had normal swallowing was back on a normal diet. She was subsequently discharged.
DISCUSSION
There continues to be much debate about the aetiology of Eagle syndrome. This is with regard to both the cause of the styloid elongation and the pain patients report. Eagle hypothesized that pharyngeal trauma or iatrogenic procedures, like tonsillectomy, led to irritation of the styloid process. His theory was that that irritation induced an osteitis and subsequent reactive ossifying hyperplasia with elongation of the styloid process [6, 8]. Another theory in the literature, proposed by Lentini [10], states that surgical trauma induces osseus metaplasia of remnants of the embryological tissue that forms the styloid process, Reichart's cartilage from the second branchial arch.
Regarding the symptoms, Eagle [8] stated the pain was due to fibres of the glossopharyngeal nerve being trapped in scar tissue following tonsillectomy. Furthermore, pain can be exacerbated if the scar tissue traps fibres of other cranial nerves whose extracranial course brings them close to the styloid ligament including trigeminal, facial, vagus and accessory nerves [3, 4]. All together, these symptoms along with ipsilateral otalgia, globus sensation and dysphagia make up the classic Eagle syndrome.
It is imperative that prior to diagnosing a patient with Eagle syndrome, differential diagnoses of ipsilateral oropharyngeal pain and a palpable mass be considered. Conditions that can mimic this are listed below:
Unerupted or impacted molar teeth
Otitis
Temporomandibular joint disorders
Dental prosthesis traumatizing the soft tissues
Salivary gland disease
Trigeminal neuralgia
Glossopharyngeal neuralgia
Sphenopalatine neuralgia
Cervical arthritis
Temporal arteritis
Hyoid bursitis
Pharyngeal, laryngeal and/or base of skull tumours
As well as a complete history, especially surgical history, and a thorough physical examination, head and neck imaging is usually required to confirm styloid elongation. This can be plain views; orthopantomogram, antero-posterior views or lateral skull views. Alternatively, computerized tomography would be the gold standard imaging modality. Our patient had an orthopantomogram on presentation. Due to the intraoral position of the styloid process, no further imaging was deemed necessary.
In conclusion, based on the literature and our patient's symptoms, we postulate that she suffered with Eagle syndrome brought about by her previous tonsillectomy and radiotherapy for the ipsi-lateral tonsillar carcinoma. The pronounced medially deflected and elongated styloid process contributed to the pain from the marked intraoral projection.
CONFLICT OF INTEREST STATEMENT
None declared.
ETHICAL APPROVAL
Not required.
FUNDING
None.
REFERENCES
- 1. Kaufman SM, Elzay RP, Irish EF. Styloid process variation. Radiologic and clinical study. Arch Otolaryngol 1970;91:460–3. [DOI] [PubMed] [Google Scholar]
- 2. Moffat DA, Ramsden RT, Shaw HJ. The styloid process syndrome: aetiological factors and surgical management. J Laryngol Otol 1977;91:279–94. [DOI] [PubMed] [Google Scholar]
- 3. Langlais RP, Miles DA, Van Dis ML. Elongated and mineralized stylohyoid ligament complex: a proposed classification and report of a case of Eagle's syndrome. Oral Surg Oral Med Oral Pathol 1986;61:527–32. [DOI] [PubMed] [Google Scholar]
- 4. Monsour PA, Young WG. Variability of the styloid process and stylohyoid ligament in panoramic radiographs. Oral Surg Oral Med Oral Pathol 1986;61:522–6. [DOI] [PubMed] [Google Scholar]
- 5. Massey EW. Facial pain from an elongated styloid process (Eagle's syndrome). South Med J 1978;71:1156–9. [DOI] [PubMed] [Google Scholar]
- 6. Eagle W. Elongated styloid process: further observation and a new syndrome. Arch Otolaryngol 1948;47:630–40. [DOI] [PubMed] [Google Scholar]
- 7. Harma R. Stylalgia: clinical experiences of 52 cases. Acta Otolaryngol 1966;224:149+. [DOI] [PubMed] [Google Scholar]
- 8. Eagle W. Elongated styloid process. Report of two cases. Arch Otolaryngol 1937;25:584–7. [DOI] [PubMed] [Google Scholar]
- 9. Murtagh RD, Caracciolo JT, Fernandez G. CT findings associated with Eagle syndrome. Am J Neuroradiol 2001;22:1401–2. [PMC free article] [PubMed] [Google Scholar]
- 10. Lentini A. The clinical and radiological abnormalities of the stylus-joideo. Radiol Med 1975;61:337–3640. [Google Scholar]