

Abstract
Background:
We aimed to understand the curative effect of liposuction curettage (LC) in the treatment of bromhidrosis.
Methods:
Relevant studies published before January 2017were searched from the PubMed, Embase, Cochrane Library, Wanfang, VIP, and China National Knowledge Infrastructure databases. Parameters including recurrence, complications, complete response, and overall response were assessed. Meta-analysis was performed using the R 3.12 statistical package. Odds ratio (OR) and 95% confidence interval (95% CI) were used for dichotomous data. Heterogeneity was assessed using Cochran's Q-statistic and I2 test. In addition, Egger's test was conducted to detect publication bias.
Results:
Ten studies with a total of 1124 participants (545 cases and 579 controls) were included. There was no statistical difference in recurrence (OR = 1.19, 95% CI: 0.51–2.74), complete response (OR = 0.66, 95% CI: 0.25–1.74), or overall response (OR = 0.63, 95% CI: 0.21–1.87) between the case and control groups. The incidence of complications in the case group was lower than that in the control group (OR = 0.24, 95% CI: 0.08–0.67) and open excision group (OR = 0.11, 95% CI: 0.07–0.19). Publication bias existed for the recurrence index in the open excision group (t = 3.3979, P = .04), but no publication bias was found in other subgroups, indicating stable results.
Conclusions:
LC, which has fewer complications, can be considered the primary choice in the treatment of patients with bromhidrosis compared with other surgical procedures.
Keywords: bromhidrosis, curative effect, liposuction curettage, meta-analysis
1. Introduction
Bromhidrosis, also referred to as axillary osmidrosis, is characterized by excessive malodor stemming from the apocrine glands.[1] It does not affect physical health but has a strong negative effect on one's professional and social life, particularly in Asians.[2,3] Thus, it is necessary to completely eradicate bromhidrosis. Drug treatment of this disease is often only temporarily effective.[2] At present, the elimination of the apocrine glands by surgical procedures seems to be the most effective and logical therapeutic method.[4]
Liposuction curettage (LC) is performed at the dermal–subcutaneous interface using a liposuction device and a sharp, rasping-type cannula.[5] Liposuction was first described in 1983 by Kesselring for axillary hyperhidrosis therapy.[6] At present, minimally invasive surgical techniques including LC have been widely used to treat bromhidrosis.[7] Tsai[8] indicated that axillary liposuction has high efficacy and low complication rates in the treatment of bromhidrosis. Li et al[9] showed that both LC and micro-incision super-thin flap are effective in the treatment of bromhidrosis. Chen et al[7] suggested that LC has better improvement and longer recurrence duration in the treatment of osmidrosis than a subcutaneous laser. However, 1 study showed that compared with LC, axillary skin resection, and small-incision minimally invasive aspiration, CO2 lasers have a higher cure rate, lower recurrence rate, and lower complication rate.[10] Other studies have indicated that the efficacy of small-incision cut-off procedures is better than that of LC.[11,12] Therefore, it is currently unclear whether LC is a better choice for treating bromhidrosis than other surgical techniques.
In order to understand the efficacy of LC in the treatment of bromhidrosis, we searched published studies in the PubMed, Embase, Cochrane Library, Wanfang, VIP, and China National Knowledge Infrastructure (CNKI) databases before January 2017 and performed this meta-analysis.
2. Methods
2.1. Source of materials
We searched the PubMed, Embase, Cochrane Library, Wanfang, VIP and CNKI databases for studies published before January 2017. The keywords “bromhidrosis” OR “underarm odor” OR “osmidrosis” OR “bromidrosis” AND “liposuction curettage” were used for searching. In addition to the database search, a literature review was conducted to find related clinical research. The publication language was not restricted in our search.
2.2. Inclusion and exclusion criteria
Studies were included in our meta-analysis if they met the following criteria: (1) published studies on the treatment of bromhidrosis with LC (case group: LC; control group: nonliposuction curettage including laser treatment and open excision) and (2) studies that could provide data about the quantitative distribution of efficacy in the 2 groups (parameters: recurrence, complications, complete response, and overall response). Reviews, reports, comments, and letters were excluded.
2.3. Data extraction
Two reviewers independently extracted data from the included studies. For each study, data including the first author name, publication year, study location, study year, intervention type, numbers, male/female number, mean age, and follow-up time were collected. Disagreements were resolved by discussion with a third reviewer.
2.4. Statistical analyses
The meta-analysis was performed using the R 3.12 statistical package (R Foundation for Statistical Computing, Beijing, China, meta package [version 4.4–1]). Odds ratio (OR) and 95% confidence interval (95% CI) were used for dichotomous data. Heterogeneity was assessed using Cochran's Q-statistic[13] and I2 test. When P < .05 or I2 > 50%, indicating significant heterogeneity, a random-effects model was used to estimate the pooled effect of outcomes. Otherwise, a fixed-effects model was used. Egger's test was conducted to detect publication bias.
3. Results
3.1. Characteristics of eligible studies
Figure 1 shows the flow chart of study selection. A total of 181 studies were identified after the initial database search. First, 46 duplicates were excluded. Then, after screening titles and abstracts, 103 obviously irrelevant studies were excluded. Subsequently, 22 studies (3 letters, 2 case series/reports, 6 literature reviews, 5 with no relevant data, 4 with no control group, and 2 reduplicative studies) were excluded by reviewing the full text of studies. Finally, 10 studies[4,7,9–12,14–17] were included in this meta-analysis.
Figure 1.
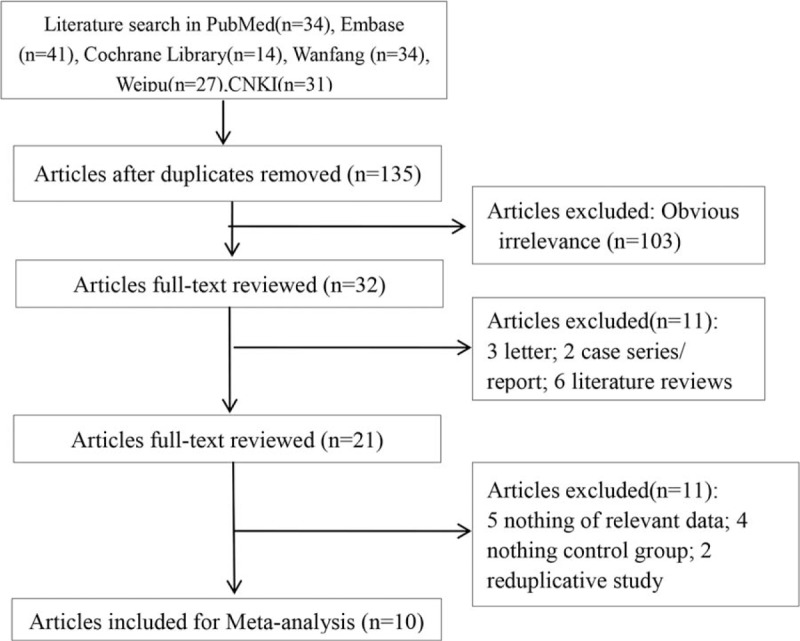
Flow chart of study selection.
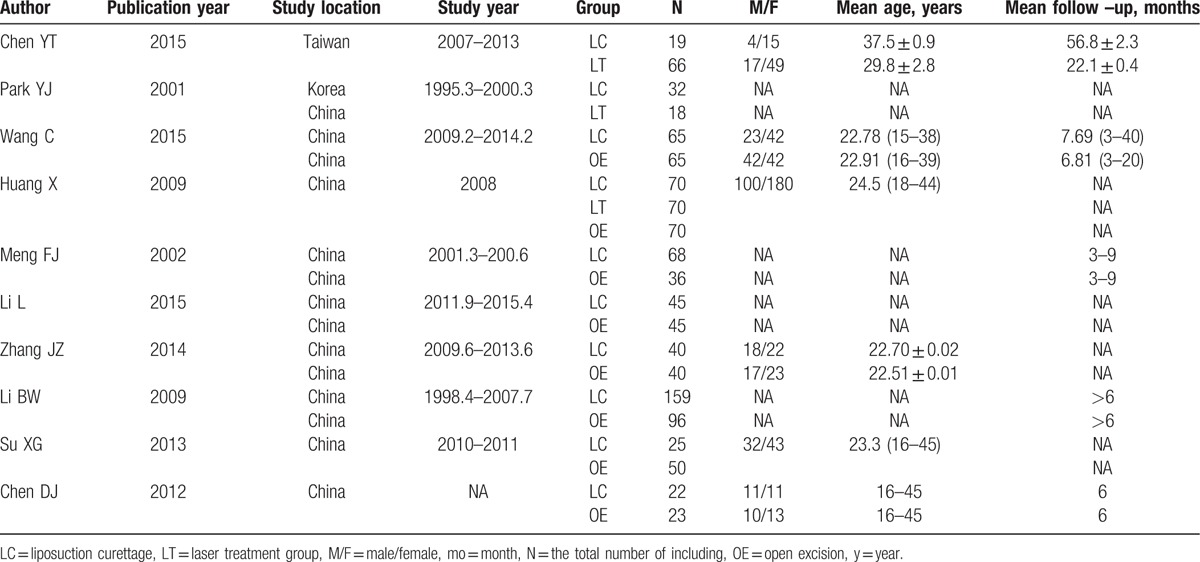
In total, 1124 participants (545 cases and 579 controls) were included. The characteristics of the included studies are shown in Table 1. The included studies were published between 2002 and 2015, and study years ranged from 1995 to 2015. China was the most common study location. More females were included in the studies than males, and most participants were middle-aged. In addition, the follow-up time was approximately 6 months.
Table 1.
The characteristics of the included studies.
3.2. Meta-analysis
Indices, including recurrence, complication, complete response, and overall response, were analyzed. Significant heterogeneity was found, and a random-effects model was, therefore, used to estimate the pooled effect of outcomes. There was no statistical difference in recurrence (OR = 1.19, 95% CI: 0.51–2.74; Fig. 2A), complete response (OR = 0.66, 95% CI: 0.25–1.74; Fig. 2B), or overall response (OR = 0.63, 95% CI: 0.21–1.87; Fig. 2C) between the case and control groups. The incidence of complications in the case group was lower than that in the control group (OR = 0.24, 95% CI: 0.08–0.67; Fig. 3). Further analysis of the control group (laser treatment and open excision) revealed that the incidence of complications in the case group was lower than that in the open excision group (OR = 0.11, 95% CI: 0.07–0.19; Fig. 3). The curative effect of LC was equivalent to that of the other 2 methods (laser treatment and open excision), but the incidence of complications in LC was less than that in laser treatment and open excision. Thus, LC can be considered the primary choice in the treatment of patients with bromhidrosis.
Figure 2.
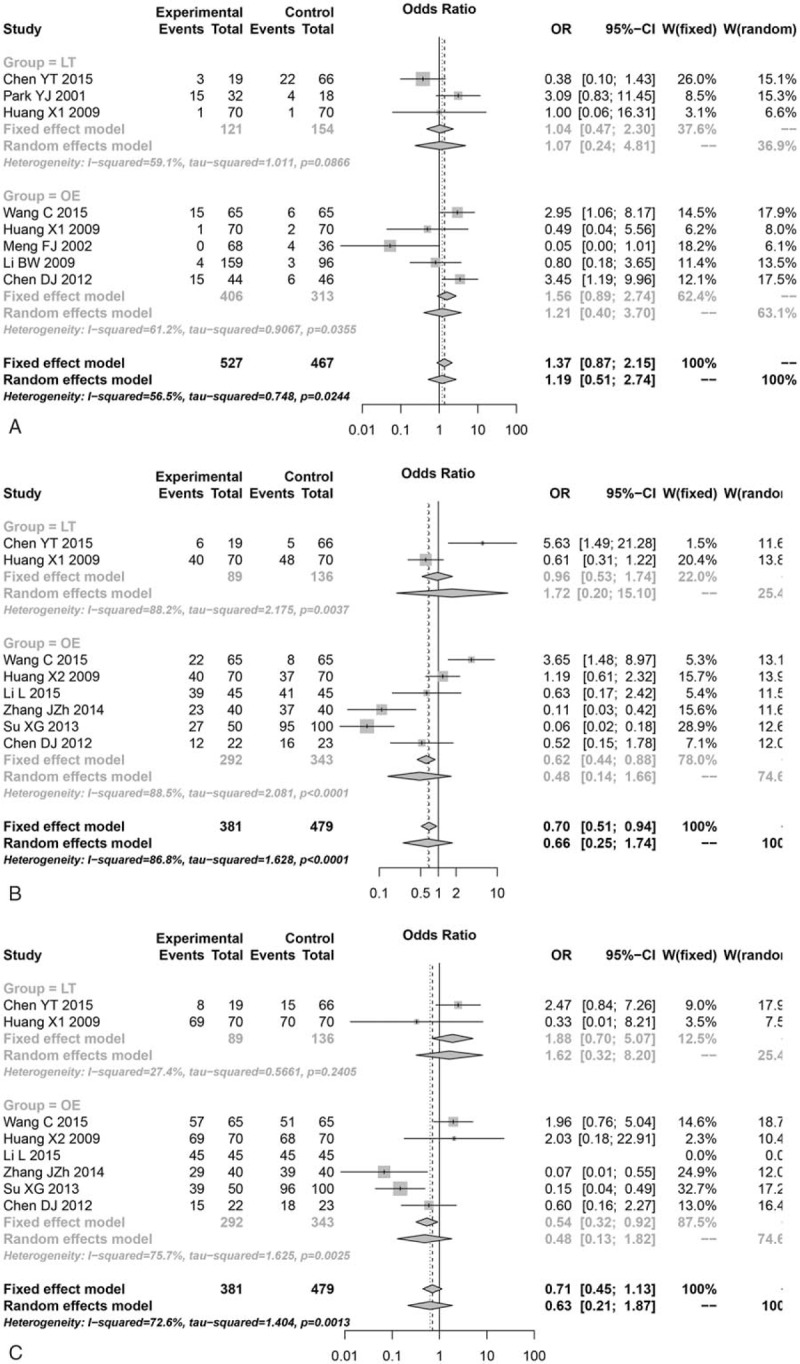
Meta-analysis results for (A) recurrence, (B) complete response, and (C) overall response.
Figure 3.
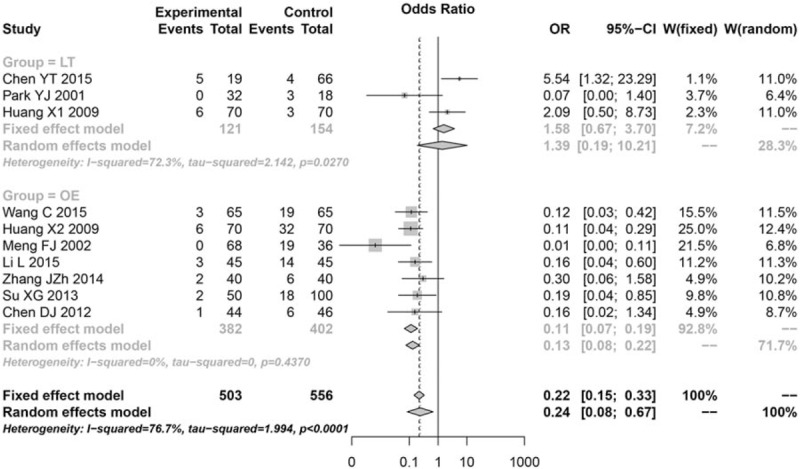
Results of the meta-analysis for complications.
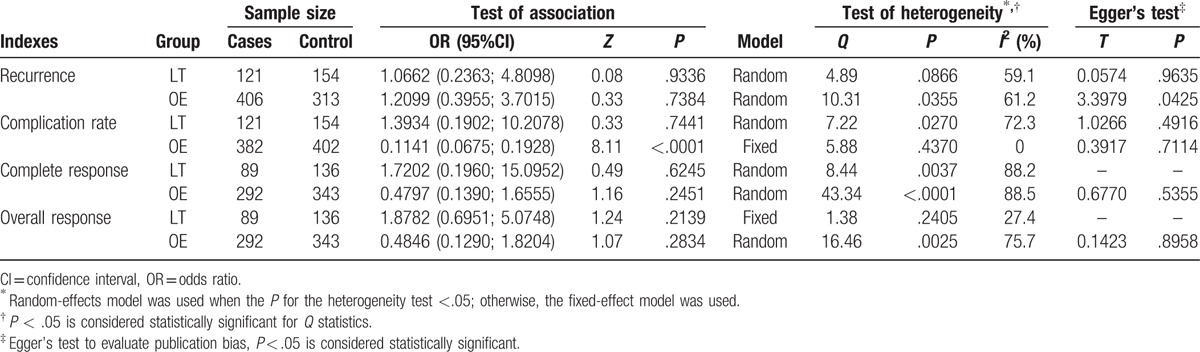
Egger's test showed that there was publication bias for the recurrence index in the open excision group (t = 3.3979, P = .04). No publication bias was found in other subgroups, indicating stable results (Table 2).
Table 2.
The results for meta-analysis.
4. Discussion
Previous studies showed mixed results, suggesting a discrepancy as to whether LC is a better choice for treating bromhidrosis than other surgical techniques. In the present study, we searched for relevant studies to clarify the curative effect of LC in the treatment of bromhidrosis via a meta-analysis. The present meta-analysis showed that the curative effect of LC was equivalent to the other 2 methods but that the complication rate in LC was less than those in laser treatment and open excision.
Methods with modest success rates and few complications are favorable in the treatment of diseases such as bromhidrosis that affect patients more mentally than physically.[18] The present study found no statistical difference in recurrence, complete response, or overall response between the LC group and the laser treatment or open excision group. However, the incidence of complications in the LC group was lower than that in the laser treatment and open excision groups, suggesting that LC is the primary choice in the treatment of patients with bromhidrosis. A previous study reported that tumescent superficial LC is a safe and effective therapy for bromhidrosis and that this method is a good choice for treating bromhidrosis.[19] Lee et al[20] also mentioned that tumescent liposuction with dermal curettage is a safe and effective procedure for treating bromhidrosis. Another study demonstrated that suction curettage combined with 2 different cannulae had a high success rate (low complications) and high satisfaction (minimal scarring and rapid recovery).[21] Perng et al[18] indicated that the treatment of bromhidrosis with liposuction had fewer complications than open excision and that 80% of patients who received liposuction treatment were satisfied with the results. Suction curettage with minimal invasiveness and minimal scarring has greater advantages than excisional surgery.[22] Therefore, we believe that LC is the primary choice in the treatment of patients with bromhidrosis compared with other surgical procedures such as laser treatment and open excision.
The present study discussed the curative effect of LC in the treatment of bromhidrosis using a meta-analysis, which improved the reliability of conclusions. Despite the strengths of the study, some limitations should be discussed. First, heterogeneity is a common limitation of meta-analyses.[23] Sources of heterogeneity may include different surgical methods, differences in location and/or ethnic groups, and the effects of demographic factors such as gender and age. Some unknown source of heterogeneity might also affect the results of the meta-analysis. Second, because of incomplete demographic characteristics in the included literature, further subgroup analysis and meta-regression analysis for age and race were not performed. Third, publication bias existed for some results, and greater numbers of samples are therefore needed to perform related analyses. In addition, the relatively small number of included studies may have affected the combined results of our subgroup analysis. Thus, it is necessary to identify a greater number of related studies to make more accurate conclusions.
In conclusion, the results of this meta-analysis suggest that LC, which has fewer complications, can be considered as the primary choice in the treatment of patients with bromhidrosis compared with other surgical procedures. For more detailed evaluations, further studies with larger sample sizes and fewer limitations are needed in the future.
Footnotes
Abbreviations: 95% CI = 95% confidence interval, CNKI = China National Knowledge Infrastructure, LC = liposuction curettage, OR = odds ratio.
Funding: The study was supported by National Natural Science Foundation of China (NSFC) [Project No. 81372068].
The authors have no conflicts of interest to disclose.
References
- [1].Guillet G, Zampetti A, Aballaincolloc ML. Correlation between bacterial population and axillary and plantar bromidrosis: study of 30 patients. Eur J Dermatol 2000;10:41. [PubMed] [Google Scholar]
- [2].Li Z-R, Sun C-W, Zhang J-Y, et al. Excision of apocrine glands with preservation of axillary superficial fascia for the treatment of axillary bromhidrosis. Dermatol Surg 2015;41:640–4. [DOI] [PubMed] [Google Scholar]
- [3].Chen YT, Shih PY, Chen HJ, et al. Treatment of axillary osmidrosis: a comparison between subcutaneous laser and superficial liposuction curettage. J Eur Acad Dermatol Venereol 2015;29:2019–23. [DOI] [PubMed] [Google Scholar]
- [4].Park YJ. What is the best method for treating osmidrosis? Ann Plast Surg 2001;47:303. [DOI] [PubMed] [Google Scholar]
- [5].Glaser DA, Galperin TA. Local procedural approaches for axillary hyperhidrosis. Dermatol Clin 2014;32:533–40. [DOI] [PubMed] [Google Scholar]
- [6].Kesselring UK. Regional fat aspiration for body contouring. Plast Reconstr Surg 1983;72:610–9. [DOI] [PubMed] [Google Scholar]
- [7].Chen YT, Shih PY, Chen HJ, et al. Treatment of axillary osmidrosis: a comparison between subcutaneous laser and superficial liposuction curettage. J Eur Acad Dermatol Venereol 2015;29:2019–23. [DOI] [PubMed] [Google Scholar]
- [8].Tsai R-Y. Treatment of excessive axillary sweat syndromes (hyperhidrosis and osmidrosis or bromhidrosis) with liposuction. 2016;Liposuction: Springer, 473–480. [Google Scholar]
- [9].Li L, Su BX. Comparative study on the efficacy of two different micro-invasive treatment for axillary bromhidrosis. Chin J Aesthetic Med 2015;24:17–9. [Google Scholar]
- [10].Huang X. The clinical curative effect comparison in different body odor removal. Med Inf 2009;1:74–5. [Google Scholar]
- [11].Zhang JZ, Yu L. Comparison among two small incision procedures in treating axillary osmidrosis. China Medical Herald 2014;26:62–4. [Google Scholar]
- [12].Su XG, Li QH, Zhao XL, et al. Comparison of efficacy and complications among three small incision procedures in treatment of axillary osmidrosis. Chin J Aesthetic Med 2013;19:168–70. [Google Scholar]
- [13].Lau J, Ioannidis JP, Schmid CH. Quantitative synthesis in systematic reviews. Ann Int Med 1997;127:820–6. [DOI] [PubMed] [Google Scholar]
- [14].Chen DJ, Shen G, Li C, et al. Minimally invasive fat suction and subcutaneous pruning technique in the treatment of axillary osmidrosis: clinical observation of 23 cases. Chin J Aesthetic Med 2012;21:2140–2. [Google Scholar]
- [15].Li BW, Tao HW, Wang MJ. Comparision of three methods in treatment of osmidrosis. Chin J Aesthetic Med 2009;15:107–9. [Google Scholar]
- [16].Meng FJ, Sun Y, Zhang XC, et al. Large sweat gland removal of bromhidrosis radical by suction-assisted lipoplasty. Chin J Plast Surg 2003;19:87–187. [Google Scholar]
- [17].Wang C. Axillary osmidrosis treatment using an aggressive suction-curettage technique: a clinical study on paired control. Aesthetic Plast Surg 2015;39:608–15. [DOI] [PubMed] [Google Scholar]
- [18].Perng C-K, Yeh F-L, Ma H, et al. Is the treatment of axillary osmidrosis with liposuction better than open surgery? Plast Reconstr Surg 2004;114:93–7. [DOI] [PubMed] [Google Scholar]
- [19].Seo SH, Jang BS, Oh CK, et al. Tumescent superficial liposuction with curettage for treatment of axillary bromhidrosis. J Eur Acad Dermatol Venereol 2008;22:30–5. [DOI] [PubMed] [Google Scholar]
- [20].Lee D, Cho SH, Kim YC, et al. Tumescent liposuction with dermal curettage for treatment of axillary osmidrosis and hyperhidrosis. Dermatol Surg 2006;32:505–11. [DOI] [PubMed] [Google Scholar]
- [21].Kim W, Song Y, Kil H, et al. Suction–curettage with combination of two different cannulae in the treatment of axillary osmidrosis and hyperhidrosis. J Eur Academy Dermatol Venereol 2008;22:1083–8. [DOI] [PubMed] [Google Scholar]
- [22].Wollina U, KÖstler E, Schoenlebe J, et al. Tumescent suction curettage versus minimal skin resection with subcutaneous curettage of sweat glands in axillary hyperhidrosis. DermatolSurg 2008;34:709–16. [DOI] [PubMed] [Google Scholar]
- [23].Moreno SG, Sutton AJ, Thompson JR, et al. A generalized weighting regression-derived meta-analysis estimator robust to small-study effects and heterogeneity. Stat Med 2012;31:1407–17. [DOI] [PubMed] [Google Scholar]