

Abstract
Background
Previous research has indicated a unique profile of executive function (EF) in children and adolescents with Down syndrome (DS). However, there is a paucity of research on EF in adults with DS. This study aimed to gain a broader understanding of strengths and weaknesses in EF in DS from 2–35 years.
Method
Parents of 112 individuals with DS between 2–35 years participated in this study. Parents either completed the Behavior Rating Inventory of Executive Function—for individuals 6+ years—or the BRIEF-Preschool—for children 2–5 years.
Results
Results suggest overall difficulties, but also patterns of strength and weakness, within EF for individuals with DS. For the 2–5-year-old group, Emotional Control and Shift were relative strengths, Planning/Organization and Inhibit were intermediate skills, and Working Memory was a relative weakness. For the 6–18-year-old group, Emotional Control and Organization of Materials were relative strengths, Inhibit and Initiate were intermediate skills, and Working Memory, Monitor, Planning/Organization, and Shift were relative weaknesses. Most abilities were consistent from 2–18 years, except Shift, which decreased in preadolescence before beginning to recover in adolescence. Across the full age range (2–35 years), composite scores indicated quadratic trends in Inhibit, Working Memory, and Planning/Organization, and a cubic trend in Shift, with EF abilities generally declining in middle childhood before recovering in adulthood.
Conclusions
This study extends previous research on EF in DS by providing an initial description of EF profiles across the lifespan. More longitudinal and behavioural research is needed to further characterise the development of EF in DS.
Keywords: executive function, Down syndrome, cognition, behavioural phenotype, BRIEF, BRIEF-P
Down Syndrome (DS)—a genetic disorder caused by an extra copy of chromosome 21—is the most common neurogenetic syndrome associated with intellectual disability (ID), affecting 1 in 691 live births (Parker et al. 2010). Over the past several decades, research has led to a better understanding of the behavioural phenotype, or developmental profile, associated with DS (see Chapman & Hesketh, 2000; Fidler, 2005). Subsequently, researchers observed that several areas of relative weakness in DS (e.g., verbal short-term memory, problem solving) could be related to difficulties with executive function (EF; Daunhauer & Fidler, 2013; Kogan et al., 2009; Lanfranchi, Jerman, Dal Pont, Alberti, & Vianello, 2010; Lee et al., 2011; Rowe, Lavender, & Turk, 2006). EF has important implications for adaptive functioning, social interactions and academics. Therefore, the purpose of the present study is to extend previous research on the behavioural phenotype associated with DS by further elucidating patterns of strength and weakness in EF across the lifespan.
EF is an umbrella term used to describe the self-regulatory cognitive processes integral to adaptive, goal-directed actions, including working memory, inhibition, shifting, and planning (Blair, Zelazo, & Greenberg, 2005; Carlson, 2005). These skills can also be divided into cool and hot EF. Cool EF refers to cognitive-based processes, such as working memory and planning (Hongwanishkul, Happaney, Lee, & Zelazo, 2005). Hot EF refers to processes that are tied to affect and the reward system, such as behavioural inhibition and emotional control (Hongwankishkul et al. 2005; Zelazo, Qu, & Muller, 2005). Together EF skills enable individuals to manage complex cognitive processes (Cartwright, 2012) and are important for day-to-day functioning, social interactions, and academic achievement (Blair & Razza, 2007; Gilotty, Kenworthy, Sirian, Black, & Wagner, 2002; Gioia, Isquith, Guy, & Kenworthy, 2002; Zingerevich & LaVasser, 2009). Identifying areas of strength and weakness in EF is essential to understanding the developmental profile of individuals with DS across the lifespan, ultimately leading to greater cognitive, academic, and social success.
Several studies of EF in DS have focused on children and adolescents using the Behavior Rating Inventory of Executive Function (BRIEF; Gioia, Isquith, Guy, & Kenworthy, 2000) and the BRIEF–Preschool (BRIEF-P; Gioia, Espy, & Isquith, 2003). These are parent and/or teacher rating scales designed to assess multiple facets of EF in children ages 6–18 and 2–5 years, respectively. Both include clinical subscales (e.g. Working Memory), as well as broad indices (e.g. Metacognition) and an overall EF composite (see Table 1).
Table 1.
Description of BRIEF-P and BRIEF Scales
| Overlapping BRIEF-P & BRIEF Clinical Subscales | |
|---|---|
|
| |
| Scale Name | Description |
| Inhibit | Ability to stop/control behaviour at the appropriate time |
| Shift | Ability to move freely from one situation, activity, aspect of a problem to another |
| Emotional Control | Ability to modulate emotional responses |
| Working Memory | Capacity to hold information in the mind for purpose of completing a task/making a response |
| Planning & Organization | Ability to manage current and future-oriented task demands within the situational context |
| Additional BRIEF Subscales | |
|
| |
| Initiate | Ability to generate ideas, responses, problem solving strategies |
| Organization of Materials | Orderliness of work, play, and storage spaces |
| Monitor | Work checking habits and personal monitoring |
| BRIEF-P Broad Indices | |
|
| |
| Inhibitory Self-Control (ISCI) | Inhibit + Emotional Control |
| Emergent Metacognition (MCI) | Working Memory + Plan/Organize |
| Flexibility (FI) | Shift + Emotional Control |
| BRIEF Broad Indices | |
|
| |
| Behavioral Regulation (BRI) | Inhibit + Shift + Emotional Control |
| Metacognition (MI) | Initiate + Working Memory + Plan/Organize + Organization of Materials + Monitor |
| BRIEF & BRIEF-P Overall Composite | |
|
| |
| Global Executive Composite (GEC) | Overall EF - Summary of all clinical subscales |
Although the BRIEF-P is designed to measure EF in children 2–5 years, it has been used more broadly with individuals with DS, including children within the age range and older individuals with DS outside of the normed age range (Daunhauer, Fidler, Hahn, Will, Lee, & Hepburn., 2014; Lee et al., 2011; Pritchard, Kalback, McCurdy, & Capone, 2015). Given developmental delays typically associated with DS, previous researchers felt the BRIEF-P was a closer match to participants’ mental ages (e.g. Daunhauer et al., 2014; Lee et al., 2011).
Studies using the BRIEF-P with participants with DS have begun to identify an EF profile in DS (Daunhauer & Fidler, 2013). Based on these studies, EF overall appears impaired relative to mental age (Daunhauer et al., 2014; Lee et al., 2011), but participants with DS demonstrate strengths and weaknesses across different domains. Specifically, emotional control and shifting appear to be areas of relative strength (Daunhauer et al., 2014). In contrast, aspects of metacognition, including working memory and the ability to plan and organise, appear to be areas of relative weakness based on both parent and teacher report (Daunhauer et al., 2014; Lee et al., 2011; Pritchard et al., 2015). Parents have also identified inhibition as an area of difficulty, though teachers have not (Daunhauer et al., 2014). Behavioural studies of EF seem consistent with this pattern, also reporting that working memory (see Jarrold & Baddeley, 2001), planning (e.g., Fidler, Hepburn, Mankin, & Rogers, 2005; Lanfranchi et al., 2010; Kasari & Freeman, 2001), problem solving, shifting, and inhibition (Lanfranchi et al., 2010) are areas of weakness relative to mental age.
The BRIEF, in contrast to the BRIEF-P, is a better chronological age match for older individuals with DS because it includes questions pertaining to school and employment, which are relevant for their chronological age. Additionally, the BRIEF includes three clinical subscales not found in the BRIEF-P: Organization of Materials, Monitor, and Initiate. These abilities are important to keep workspaces and materials in order, stay on task, check work, and assess performance. As such, they are especially important for academics and employment as individuals with DS get older, regardless of mental age.
Across a series of studies, Lee et al. (2015) examined cool and hot aspects of EF and the relationship between age and EF in individuals with DS using the BRIEF. The Metacognition and Behavioral Regulation indices were used to measure cool and hot EF skills, respectively. Results indicated that participants with DS 7–17 years had greater difficulty with cool versus hot EF. In comparison to typically developing (TD) controls matched on chronological age and maternal education, participants with DS also showed greater difficulty on all subscales of the BRIEF, except for Organization of Materials. Additional within-group analyses revealed that participants with DS demonstrated relative strengths in Organization of Materials and Emotional Control and relative weaknesses in Working Memory and Monitor.
Next, to examine the relationship between age and EF, Lee et al. (2015) used the BRIEF and BRIEF-P with participants with DS from ages 4–24. The decision of which version to administer depended on the protocol in place at various institutions that participated in the study (i.e., some administered versions based on participants’ mental ages, others used chronological age). Because of overlap across versions, composite scores were created to combine items from the two forms, including Emotional Control, Inhibit, Shift, Planning/Organization, and Working Memory. Across the five composites, only Inhibit showed improvement with age. Lee et al. suggested that inhibition may continue to improve into adulthood (i.e., mid-20s to early-30s) and may even reach levels similar to TD norms, but at older chronological ages not included in their study.
Given the paucity of knowledge on EF in DS across the lifespan, especially in adults with DS, more research is needed to replicate previous findings and to gain a broader understanding of strengths and weaknesses relative to chronological age. A needed next step is to analyse EF in DS using the version of the BRIEF that corresponds to chronological age for all participants. Previous research has either used the BRIEF-P to examine EF in older individuals with DS based on younger mental-ages (e.g. Daunhauer et al., 2014), or used a mix of the BRIEF and BRIEF-P for participants across sites (e.g. Lee et al., 2015). The present study will extend previous research by examining a wider age range than previously reported and by examining the pattern of strengths and weakness relative to chronological age rather than mental age. Specifically, we aim to address three research questions:
Do individuals with DS ages 2–5 and 6–18 years demonstrate difficulties with EF as measured by standardised T-scores when using the version of the BRIEF associated with their chronological age?
Are relative strengths and weaknesses in EF consistent in DS across the ages of 2–18 years?
Do EF skill levels remain consistent in DS across the ages of 2–35 years?
Method
Participants
Parents of 131 individuals with DS participated in the study; 112 were included in data analysis. Participants were recruited from the University of Alabama Intellectual Disabilities Registry (UAIDPR), the Participant Recruitment and Management Core (PARC) at the University of Kansas, and parent support groups across the United States.
There was one criterion to participate in this study - to be the primary caregiver of a person with DS over the age of 2 years. Due to low numbers of parents/caregivers with a son or daughter over the age of 35 years (n=4), these participants were excluded from data analysis. Nine participants were excluded because they scored in the elevated range on the inconsistency scale, which indicates the extent to which a respondent answers similar items in an inconsistent manner. Also, consistent with standardised scoring instructions, six participants were excluded because of missing responses (>12 BRIEF-P; >14 BRIEF).
Of the 112 individuals with DS reported on in data analysis, 55.4% were female and 44.6% male. Almost all raters were mothers (96%). Demographic information was available for 88 of the 112 individuals with DS (see Table 2).
Table 2.
Demographic Characteristics of Individuals with Down syndrome
| Overall (n=112) | Ages 2–5 (n=22) | Ages 6–18 (n=64) | Ages 19–35 (n=26) | |
|---|---|---|---|---|
| Age - Mean | 12.8 | 3.6 | 11.5 | 24.0 |
| - Standard Deviation | 7.7 | 1.2 | 3.3 | 5.0 |
| Male | 44.6% | 40.9% | 43.7% | 50.0% |
| Female | 55.4% | 59.1% | 56.3% | 50.0% |
| Vision Impairment | 61.3% | 38.1% | 67.2% | 68.0% |
| Corrective Glasses or Contact Lenses | 58.2% | 23.8% | 64.1% | 72.0% |
| Hearing Impairment | 38.4% | 33.3% | 34.4% | 53.8% |
| Hearing Aid | 12.6% | 19.1% | 10.9% | 12.0% |
Measures
Behavior Rating Inventory of Executive Function – Preschool Version (BRIEF-P)
The BRIEF-P (Gioia et al., 2003) is a standardised rating scale designed to measure EF in children ages 2–5 years. Parents and/or primary caregivers were asked to complete the BRIEF-P for their child with DS. The BRIEF-P provides parents with a series of 63 statements regarding their child’s behaviour, such as, “Needs to be told to begin a task even when willing to do it.” For each statement, parents are asked to rate how often (never=1, sometimes=2, or often=3), in the past six months, each of the listed behaviours has been a problem. Higher scores indicate greater difficulty. The BRIEF-P yields T-scores, which are standardised scores based on the reported individual’s age and sex. A mean T-score is 50, and T-scores of 65 or higher are considered “clinically elevated”. See Table 1 for an overview. Both raw and T-scores were used in the present study.
The BRIEF-P parent form has good internal consistency (.80–.95) and good test-retest reliability (.78–.90; Gioia et al., 2003). It correlates significantly with subscales from the ADHD-Rating Scale-IV-Preschool Version (McGouey, DuPaul, Haley, & Shelton, 2007), Child Behavior Checklist (Achenbach & Rescorla, 2000), and Behavior Assessment System for Children Parent Rating Scales (Reynolds & Kamphaus, 1992).
Behavior Rating Inventory of Executive Function (BRIEF)
The BRIEF (Gioia et al., 2000) is a standardised rating scale designed to measure EF in individuals ages 6–18 years. The BRIEF parent form consists of 86 items. The rating format and T-score norms are the same as the BRIEF-P. In the present study, raw and T-scores were used for parents/guardians of a son or daughter with DS age 16–18 years. Raw scores were used for those older than 18 years.
The BRIEF parent form has good internal consistency (.80–.98) and good test-retest reliability (.72–.88). It correlates significantly with subscales from the ADHD-Rating Scale-IV (DuPaul, Anastopoulous, Power, Reid, Ikeda, & McGoey, 1998), Child Behavior Checklist (Achenbach, 1991), Behavior Assessment System for Children Parent Rating Scales (Reynolds & Kamphaus, 1992), and Conners’ Rating Scale (Conners, 1989). Further, the BRIEF has been successfully used with parents of individuals with DS before (e.g. Edgin et al., 2010; Memisevic & Sinanovic, 2013; 2014).
Parent Questionnaire
A questionnaire designed by our lab was used to measure parents’ perceptions of their child’s reading, hearing, vision, and language abilities, and to gather other background information (i.e., race/ethnicity).
Procedure
Parents were given the option of completing the surveys via postal mail (n=97) or over the phone (n=15) with an investigator. Those who completed the survey via mail were sent the surveys, instructions, and a return envelope. Those who completed the study over the phone were read the instructions and questions. Investigators then recorded verbal answers.
Results
Data Analysis
Descriptive statistics, repeated measures ANOVAs, and regression-based curve estimation analyses were used in the following analyses. An alpha level for significance was set at .05.
Preliminary Analyses
We searched for outliers by looking for scores that were more than three standard deviations (SD) from the mean for each variable. While there were no outliers on the Global Executive Composite (GEC) or broad indices, there were three outliers (3.03–3.36 SD) found on clinical subscales (n=1 Inhibit; n=2 Emotional Control). Because these represented less than .003 of 1182 scores in the dataset, they were retained for analysis.
A small number of parents/guardians completed the BRIEF-P (n=2) or the BRIEF (n=13) over the phone. To ensure that this did not alter the pattern of results, all analyses were re-run without these participants. The pattern of results did not change for any analyses; thus, they are included in all reported results.
Means, SDs, and percent of clinically elevated T-scores (≥ 65) are presented in Table 3. For individuals with DS age 2–5 years, over half of the sample had clinically elevated T-scores on Working Memory and the Emergent Metacognition Index. In contrast, only 15% of the sample showed clinically elevated T-scores on Emotional Control and less than 20% on the Flexibility Index. For individuals with DS age 6–18 years, the highest percentage of clinically elevated scores included Working Memory (45%), Monitor (45%), Shift (40%), and Planning/Organization (40%). Emotional Control appeared to be an area of relative strength for this group as well, with only 11% of the sample scoring in the elevated range, along with Organization of Materials (14%).
Table 3.
Percent of Clinically Elevated T-Scores, Means, Standard Deviations, and One-Sample T-Test Results for Children 2–5 years on the BRIEF-P and Individuals 6–18 years on the BRIEF
| BRIEF-P (ages 2–5) | αa | %CEb | Mean | SD | tc | p-value | Cohen’s dd |
|---|---|---|---|---|---|---|---|
| Inhibit | .90 | 31.82 | 55.64 | 13.83 | 1.91 | 0.070 | 0.41 |
| Shift | .85 | 19.05 | 51.59 | 11.16 | 0.67 | 0.511 | 0.14 |
| Emotional Control | .86 | 15.00 | 48.09 | 13.81 | −0.65 | 0.524 | −0.14 |
| Working Memory | .88 | 60.00 | 65.59 | 12.78 | 5.72* | <0.001 | 1.22 |
| Planning & Organization | .80 | 31.58 | 57.23 | 12.26 | 2.76 | 0.012 | 0.59 |
| Inhibitory Self-Control Index | .92 | 29.41 | 52.59 | 13.92 | 0.87 | 0.392 | 0.19 |
| Flexibility Index | .89 | 18.75 | 49.77 | 12.11 | −0.09 | 0.931 | −0.02 |
| Emergent Metacognition Index | .91 | 73.33 | 63.27 | 13.30 | 4.68* | <0.001 | 1.00 |
| GEC | .95 | 52.94 | 58.27 | 13.76 | 2.82 | 0.010 | 0.60 |
|
| |||||||
| BRIEF (ages 6–18) | αa | %CEb | Mean | SD | tc | p-value | Cohen’s dd |
|
| |||||||
| Inhibit | .91 | 29.69 | 59.16 | 12.14 | 6.03* | <0.001 | 0.75 |
| Shift | .81 | 40.63 | 62.05 | 9.66 | 9.98* | <0.001 | 1.25 |
| Emotional Control | .89 | 10.94 | 52.36 | 10.43 | 1.81 | 0.075 | 0.23 |
| Initiate | .80 | 25.00 | 57.86 | 10.24 | 6.14* | <0.001 | 0.77 |
| Working Memory | .89 | 45.31 | 63.03 | 10.96 | 9.51* | <0.001 | 1.19 |
| Planning & Organization | .90 | 40.63 | 61.22 | 9.83 | 9.13* | <0.001 | 1.14 |
| Organization of Materials | .87 | 14.06 | 52.13 | 9.80 | 1.74 | 0.088 | 0.22 |
| Monitor | .83 | 45.31 | 62.53 | 10.82 | 9.27* | <0.001 | 1.16 |
| Behavioural Rating Index | .94 | 21.88 | 58.36 | 10.69 | 6.26* | <0.001 | 0.78 |
| Metacognition Index | .96 | 37.50 | 61.14 | 9.41 | 9.47* | <0.001 | 1.18 |
| GEC | .97 | 32.81 | 60.77 | 9.36 | 9.20* | <0.001 | 1.15 |
Internal consistency coefficients, based on normative sample
Percentage of individuals with DS reported in the clinically elevated range (≥65)
Comparison to normative mean T-score of 50.
Sample SD were used to calculate Cohen’s d.
Significant after Bonferroni correction.
EF Profiles by Chronological Age
Age-Normed Profile for 2–5 Years
T-scores for the GEC were significantly above the norm of 50, indicating overall difficulty with EF relative to chronological age peers, t(21) = 2.82, p = .010. Of the three index scores, however, only the Emergent Metacognition Index was significantly above the norm of 50, t(21) = 4.68, p < .001, suggesting that the main EF difficulty in this age range is in emerging metacognition. T-scores for the five subscales were also compared to the norm of 50, using a Bonferroni correction (α .05/5=.01). Some but not all subscales showed significant difficulty, suggesting a profile of strengths and weaknesses (see Table 3 for results). A repeated measures ANOVA comparing T-scores across scales confirmed that there were areas of relative strength and weakness, F(4, 84) = 13.53, p < .001, η2 = .392. An examination of mean T-scores suggests that the greatest difficulty was in Working Memory (Mean = 65.59; significantly different from 50), followed by Planning/Organization and Inhibition (Means = 57.23 and 55.64, respectively; marginally significant), followed by Shift and Emotional Control (Means = 51.59 and 48.09, respectively; nonsignificant).
Age-Normed Profile for 6–18 Years
T-scores for the GEC were significantly above the norm of 50, indicating overall difficulty with EF relative to chronological age peers, t(63) = 9.20, p < .001. Also, T-scores for both the Behavioral Rating Index, t(63) = 6.26, p < .001, and the Metacognitive Index, t(63) = 9.47, p < .001, were significantly above 50. T-scores for each of the eight subscales were compared to the norm of 50, using a Bonferroni correction (α .05/8=.00625). Most, but not all, subscales showed significant difficulty (see Table 3). A repeated measures ANOVA comparing T-scores across scales confirmed that there were areas of relative strength and weakness, F(7, 441) = 20.18, p < .001, η2 = .027. Based on mean T-scores, the areas of greatest weakness were Working Memory, Monitor, Shift, and Planning/Organization (Means = 63.03, 62.53, 62.05, and 61.22, respectively; all significantly different from 50). Areas of moderate weakness were Inhibit and Initiate (Means = 59.16 and 57.86, respectively, both significantly different from 50). Areas of relative strength were Organization of Materials and Emotional Control (Means = 52.13 and 52.36, respectively, nonsignificant).
Strengths and Weaknesses in EF Cross-sectionally from 2–18 years
To better understand the development of EF in DS from ages 2–18, we used regression-based curve estimation to examine the profile of T-scores from the GEC and the overlapping subscales on the BRIEF and BRIEF-P. The overlapping subscales included Inhibit, Shift, Emotional Control, Working Memory, and Planning/Organization. With age entered as an independent variable there were no significant trends (linear, quadratic, or cubic) from 2–18 years on the GEC (p’s > .46). Inhibit, Emotional Control, Working Memory, and Planning/Organization were also nonsignificant (p’s > .12). However, there was a significant quadratic trend on Shift, R2 = .15, F(2, 83) = 7.25, p = .001 (see Figure 1). Specifically, T-scores increased slightly from age 2 to preadolescence before beginning to decline slightly to age 18.
Figure 1.
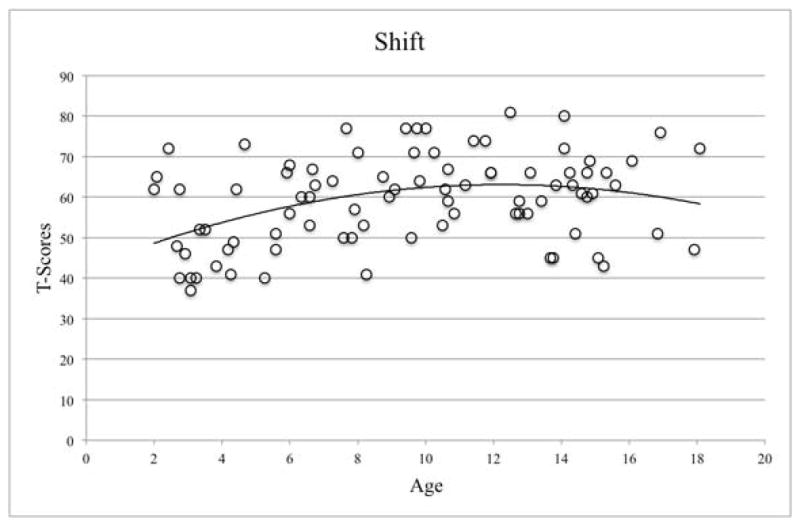
Significant quadratic trend in T-scores for Shift for individuals 2–18 years.
Consistency of Strengths and Weaknesses Cross-sectionally from 2–35 years
To better understand the development of EF in DS across the lifespan we used regression-based curve estimation to examine the profile of calculated composite scores from individuals ages 2–35 years. Using the same method as Lee et al. (2015), common questions from the BRIEF-P and the BRIEF were used to calculate composite scores for Inhibit, Shift, Emotional Control, Working Memory, and Planning/Organization. We entered age as an independent variable and the five composite scores as dependent variables (one for each analysis). Higher scores indicate greater difficulty.
Emotional Control was the only composite with no significant trend. There were significant quadratic trends for Inhibit, R2 = .07, F(2, 109) = 3.87, p = .024; Working Memory, R2 = .09, F(2, 109) = 5.37, p = .006; and Planning/Organization, R2 = .09, F(2, 109) = 5.26, p = .007 (see Figure 2). In each case, difficulty increased across individuals from age 2 to late childhood, then declined to about age 30. There was also a significant cubic trend for Shift, R2 = .13, F(3, 108) = 3.91, p = .011, in which difficulty begins to increase again from 30–35 years.
Figure 2.

Significant quadratic (Shift) and cubic (Planning/Organization, Inhibit, Working Memory) trends in calculated raw composite scores for individuals 2–35 years.
Discussion
The present study utilised the BRIEF-P and BRIEF to examine EF in individuals with DS ages 2–35 years. Results indicated that individuals with DS have difficulties in EF overall, but areas of relative strength and weakness across domains. Using age-normed T-scores, strengths and weaknesses were largely consistent across individuals from 2–18 years. However, by using raw scores and extending to age 35, a distinct developmental pattern of change across ages emerged.
We first examined EF in individuals with DS ages 2–5 years and 6–18 years using standardised T-scores from the version of the BRIEF that corresponded to their chronological age. Children 2–5 years showed significant difficulties overall, as indicated by the GEC, and with emerging cognition in general, as indicated by the Emergent Metacognition Index. The profile that emerged across EF indicated Emotional Control and Shift as the strongest skills, Planning/Organization and Inhibit as intermediate skills, and Working Memory as the weakest skill. To our knowledge, these are the first data from the BRIEF-P on children with DS specifically with a chronological age of 2–5 years.
Individuals with DS between 6–18 years also demonstrated difficulties in EF, based on the GEC and the Behavioral Regulation and Metacognition Indices. The profile that emerged from this group included Emotional Control and Organization of Materials as strongest, Inhibit and Initiate as intermediate, and Working Memory, Monitor, Planning/Organization, and Shift as weakest. This profile is highly consistent with Lee et al. (2015, Experiment 1).
The profiles of the two age groups were similar in that individuals with DS were reported to have their greatest EF strength in modulating their emotional responses, to be intermediate in controlling their behaviour, and to have their greatest difficulties in holding information in mind while completing tasks. Thus, there was a tendency toward strengths in hot EF and weaknesses in cool EF. This pattern replicates results from school-age children with DS with the BRIEF and BRIEF-P (Daunhauer et al., 2014; Lee et al., 2011; Lee et al., 2015).
A minor difference between the profiles of the two age groups is that Planning/Organization was intermediate in the younger individuals with DS, but a relative weakness in the older individuals. Previous researchers have consistently identified Planning/Organization as a weakness (Daunhauer et al., 2014; Lee et al., 2011; 2015). However, no previous studies have looked specifically at subscale performance in the 2–5-year age range. Perhaps, difficulties in planning/organisation become more apparent relative to same-age TD peers as children enter the school environment.
The greatest difference between the two age groups was that Shift was one of the strongest EF skills for children 2–5, but one of the weakest for individuals 6–18. Past studies have reported Shift as either intermediate (Lee et al., 2011; 2015) or a strength (Daunhauer et al., 2014). However, none of these studies included children as young as ours and none made a direct comparison between younger and older children on T-scores. Our results suggest that preschool-age children with DS may transition from one activity to another without becoming upset, or at least parents do not report this as a problem. However, older children were reported to have difficulty with such transitions and/or with changes in plans and routines. It could be argued that demands of the school environment make these difficulties apparent when they previously were unnoticed. However, the drastic change from strength to weakness could suggest something more complex - it is possible that shifting skills begins to slow during middle childhood. This finding warrants further investigation.
To examine differences in EF from 2–18 years, we looked at trajectories of T-scores across both groups combined for the five overlapping subscales. T-scores were highly consistent across this age range, except Shift. Relative to chronological-age norms, individuals with DS had more difficulty shifting as they approached preteen years, but then recovered in adolescence. These findings are consistent with the pattern of results in the 2–5 and 6–18 age group analyses and suggest that, in DS, development of shifting skills may slow in middle childhood, and then resume pace in the teenage years. This EF skill may have different rates of growth at different stages of childhood. This intriguing finding also warrants replication.
Lee et al.’s (2015) cross-sectional data largely supported a developmental stability hypothesis, suggesting that the magnitude of difficulty in EF skills is stable across age in DS. Our data are also largely consistent with this developmental stability hypothesis—T-scores, except in Shift, did not change much from 2–18. However, because T-scores in Shift changed with age, we must recognise the possibility that there is developmental stability for some EF skills, perhaps most, but variability for others.
To observe a larger age range, trajectories of EF skills were examined from 2–35 years. Each of five calculated composite scores (after Lee et al., 2015) was analysed cross-sectionally. Unlike age-normed T-scores, composites reflect raw abilities. Whereas Lee et al. (Experiment 3) examined linear trends in raw composite scores across ages 4–24 years, we examined linear and curvilinear trends. Consistent with Lee et al., individuals with DS in the present study were reported to have similar scores in Emotional Control across age. This suggests that parents viewed their children’s emotional control as not being problematic regardless of age.
In contrast, there were significant curvilinear trends for Shift, Inhibit, Working Memory, and Planning/Organization. For each, scores increased (indicating more difficulty) from preschool to middle childhood, then decreased (indicating less difficulty) in the early to mid-30’s. The greater difficulty from preschool to middle childhood may be associated with transitioning to the more challenging school environment and/or parents’ corresponding greater awareness of their children’s challenges. We do not necessarily interpret this as a loss of ability. After children and parents have fully acclimated to the school environment, abilities seem to improve, and continue to do so into the mid-30’s. After that, however, there appears to be the beginning of a decline in Shift, and possibly Inhibit, though with a cut-off of 35 years, this is speculative (see Adams & Oliver, 2010; Ball, Holland, Watson, & Huppert, 2010).
Considering that individuals with DS are at an increased risk of developing early-onset Alzheimer’s disease (Zigman & Lott, 2007), there are many unanswered questions regarding patterns of EF skills in individuals with DS who do or do not develop Alzheimer’s disease. Future research exploring associations between EF and aging in DS may provide additional insight into the scores we observed in the older individuals with DS in our sample.
Limitations
While the present study was the first, to our knowledge, to measure EF across such a wide age range in DS, the data are cross-sectional and warrant longitudinal replication. Also, we were unable to include a measure of overall cognitive abilities (i.e., IQ) or direct behavioural measures of EF in the present study. We were, therefore, unable to examine how IQ might have impacted trends in EF or to determine the extent to which parents’ opinions corresponded to children’s actual abilities (e.g., Toplak, West, & Stanovich, 2013).
Further, the quadratic and cubic curves should be interpreted with caution. Using the age-appropriate BRIEF scale meant that there were differences in some items for parents who completed the BRIEF versus the BRIEF-P. While paired questions in the composite scores were very similar, and in many cases identical, they were not always perfect matches. Thus, parents of children ages 2–5 years answered slightly different questions than parents of older individuals.
The present study also relied on parent report. Because parents may have different expectations depending on their child’s age, this may have influenced their responses. Also, some questions may not have been relevant to individuals with DS over the age of 18 (the BRIEF-A for adults was not yet published when this study began). Now that the BRIEF-A is available, future studies will be able to use the form that is appropriate for individuals over the age of 18. It is also possible that the structure of EF abilities (e.g., unitary vs. multifactorial) is different depending on age, as has been shown for TD children (e.g. Miller, Giesbrecht, Müller, McInerney, & Kerns, 2012). Replication using direct measures of EF would be helpful in determining the developmental trajectories of EF skills. Finally, the sample size was not consistent across ages, with fewer individuals with DS in the older range (age 25–35) than in the rest of the sample.
Implications
Understanding strengths and weaknesses of EF in DS, as well as possible changes in these skills with age, could be beneficial for parents and professionals. First, understanding specific difficulties can provide targets for interventions and indicate areas where extra supports may be needed. For example, our results indicate that working memory is one area that is especially difficult for individuals with DS that could be targeted for intervention. Further, caregivers, teachers, employers, and/or clinicians may need to offer visual supports and reminders (e.g. a reference list of tasks to accomplish at work or school) to aid individuals with DS when they are required to store information in working memory. Similarly, extra supports may be needed to help individuals with DS when planning and organising tasks, as well as monitoring their progress towards completing tasks. In contrast, understanding strengths in EF can allow parents and professionals to capitalize and build on these EF skills, such as emotional control and organisation of materials. Finally, parents and teachers should be aware of changes in skills and expectations across different age groups. For example, Shift changed from a relative strength in 2–5-year-olds to a weakness in older children. It is unknown whether this is indicative of changes in abilities with age or due to increased expectations. Regardless, this is something parents and teachers should discuss to allow for clear expectations and goal setting.
References
- Achenbach TM. Manual for the Child Behavior Checklist/4 – 18 and 1991 Profile. Burlington, VT: University of Vermont Department of Psychiatry; 1991. [Google Scholar]
- Achenbach TM, Rescorla LA. Manual for the ASEBA Preschool Forms & Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families; 2000. [Google Scholar]
- Adams D, Oliver C. The relationship between acquired impairment of executive function and behavior change in adults with Down syndrome. Journal of Intellectual Disability Research. 2010;54:393–405. doi: 10.1111/j.1365-2788.2010.01271.x. [DOI] [PubMed] [Google Scholar]
- Ball SL, Holland AJ, Watson PC, Huppert FA. Theoretical exploration of the neural bases of behavioural disinhibition, apathy, and executive dysfunction in preclinical Alzheimer’s disease in people with Down’s syndrome: Potential involvement of multiple frontal-subcortical neuronal circuits. Journal of Intellectual Disability Research. 2010;54:320–336. doi: 10.1111/j.1365-2788.2010.01261.x. [DOI] [PubMed] [Google Scholar]
- Blair C, Razza RP. Relating effortful control, executive function, and false belief understanding to emerging math and literacy ability in kindergarten. Child Development. 2007;78(2):647–63. doi: 10.1111/j.1467-8624.2007.01019.x. [DOI] [PubMed] [Google Scholar]
- Blair C, Zelazo PD, Greenberg MT. The measurement of executive function in early childhood. Developmental Neuropsychology. 2005;28:561–571. doi: 10.1207/s15326942dn28021. [DOI] [PubMed] [Google Scholar]
- Carlson SM. Developmentally sensitive measures of executive function in preschool children. Developmental Neuropsychology. 2005;28(2):595–616. doi: 10.1207/s15326942dn2802_3. [DOI] [PubMed] [Google Scholar]
- Cartwright K. Insights from cognitive neuroscience: The importance of executive function for early reading development and education. Early Education and Development. 2012;23(1):24–36. doi: 10.1080/10409289.2011.615025. [DOI] [Google Scholar]
- Chapman RS, Hesketh LJ. Behavioral phenotype of individuals with Down syndrome. Mental Retardation and Developmental Disabilities Research Reviews. 2000;6(2):84–95. doi: 10.1002/1098-2779(2000)6:2<84::AID-MRDD2>3.0.CO;2-P. [DOI] [PubMed] [Google Scholar]
- Conners CK. Manual for Conners’ Rating Scale. North Towanda, NY: MultiHealth Systems; 1989. [Google Scholar]
- Daunhauer LA, Fidler DJ, Hahn L, Will E, Lee NR, Hepburn S. Profiles of everyday executive functioning in young children with Down syndrome. American Journal on Intellectual and Developmental Disabilities. 2014a;119(4):303–18. doi: 10.1352/1944-7558-119.4.303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Daunhauer LA, Fidler DJ. Executive functioning in individuals with Down syndrome. In: Barrett KC, Fox NA, Morgan GA, Fidler DJ, Daunhauer LA, editors. Handbook of self-regulatory processes in development: New directions and international perspectives. New York, NY: Psychology Press; 2013. pp. 453–472. [Google Scholar]
- DuPaul GJ, Anastopoulos AD, Power TJ, Reid R, Ikeda MJ, McGoey KE. Parent ratings of Attention-Deficit/Hyperactivity Disorder symptoms: Factor structure and normative data. Journal of Psychopathology and Behavioral Assessment. 1998;20:83–102. doi: 10.1037/pas0000166. [DOI] [Google Scholar]
- Edgin JO, Mason GM, Allman MJ, Capone GT, DeLeon I, Maslen C, Reeves RH, Sherman SL, Nadel L. Development and validation of the Arizona Cognitive Test Battery for Down syndrome. Journal of Neurodevelopmental Disorders. 2010;2:149–164. doi: 10.1007/s11689-010-9054-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fidler DJ. The emerging Down syndrome behavioral phenotype in early childhood: implications for practice. Infants & Young Children. 2005;18(2):86–103. doi: 10.1097/00001163-200504000-00003. [DOI] [Google Scholar]
- Fidler DJ, Hepburn SL, Mankin G, Rogers SJ. Praxis skills in young children with Down syndrome, other developmental disabilities, and typically developing children. The American Journal of Occupational Therapy. 2005;59(2):129–38. doi: 10.5014/ajot.59.2.129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gilotty L, Kenworthy L, Sirian L, Black DO, Wagner AE. Adaptive skills and executive function in autism spectrum disorders. Child Neuropsychology. 2002;8(4):241–248. doi: 10.1076/chin.8.4.241.13504. [DOI] [PubMed] [Google Scholar]
- Gioia GA, Isquith PK, Guy SC, Kenworthy L. Behavior Rating Inventory of Executive Function. Odessa, FL: Psychological Assessment Resources; 2000. [Google Scholar]
- Gioia GA, Isquith PK, Guy SC, Kenworthy L. Profiles of everyday executive function in acquired and developmental disorders. Child Neuropsychology. 2002;(2):121–137. doi: 10.1076/chin.8.2.121.8727. [DOI] [PubMed] [Google Scholar]
- Gioia GA, Espy KA, Isquith PK. Behavior rating inventory of executive function-preschool version. Lutz, FL: Psychological Assessment Resources; 2003. [Google Scholar]
- Hongwanishkul D, Happaney KR, Lee WS, Zelazo PD. Assessment of hot and cool executive function in young children: Age-related changes and individual differences. Developmental Neuropsychology. 2005;28(2):617–644. doi: 10.1207/s15326942dn2802_4. [DOI] [PubMed] [Google Scholar]
- Jarrold C, Baddeley AD. Short-term memory in Down syndrome: applying the working memory model. Down Syndrome Research and Practice. 2001;7(1):17–23. doi: 10.3104/reviews.110. [DOI] [PubMed] [Google Scholar]
- Kasari C, Freeman SFN. Task-related social behavior in children with Down syndrome. American Journal on Mental Retardation. 2001;106(3):253–264. doi: 10.1352/0895-8017(2001)106<0253:TRSBIC>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Kogan CS, Boutet I, Cornish K, Graham GE, Berry-Kravis E, Drouin A, Milgram NW. A comparative neuropsychological test battery differentiates cognitive signatures of Fragile X and Down syndrome. Journal of Intellectual Disability Research. 2009;53(2):125–142. doi: 10.1111/j.1365-2788.2008.01135.x. [DOI] [PubMed] [Google Scholar]
- Lanfranchi S, Jerman O, Dal Pont E, Alberti A. Executive function in adolescents with Down Syndrome. Journal of Intellectual Disability Research. 2010;54(4):308–319. doi: 10.1111/j.1365-2788.2010.01262.x. [DOI] [PubMed] [Google Scholar]
- Lee NR, Anand P, Will E, Adeyemi EI, Clasen L, Blumenthal J, Giedd J, Daunhauer LA, Fidler D, Edgin JO. Everyday executive functions in Down syndrome from early childhood to young adulthood: Evidence for both unique and shared characteristics compared to youth with sex chromosome trisomy (XXX and XXY) Frontiers in Behavioral Neuroscience. 2015;9:264. doi: 10.3389/fnbeh.2015.00264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee NR, Fidler DJ, Blakeley-Smither A, Daunhauer L, Robinson C, Hepburn SL. Caregiver report of executive functioning in a population based sample of young children with Down syndrome. American Journal on Intellectual and Developmental Disabilities. 2011;116(4):290–304. doi: 10.1352/1944-7558-116.4.290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGoey KE, DuPaul GJ, Haley E, Shelton TL. Parent and teacher ratings of attention-deficit/hyperactivity disorder in preschool: the ADHD Rating Scale-IV Preschool Version. Journal of Psychopathology and Behavioral Assessment. 2007;29(4):269–276. doi: 10.1007/s10862-007-9048-y. [DOI] [Google Scholar]
- Memisevic H, Sinanovic O. Executive functions as predictors of visual-motor integration in children with intellectual disability. Perceptual and Motor Skills: Physical Development and Measurement. 2013;117:913–922. doi: 10.2466/15.25.PMS.117x25z4. [DOI] [PubMed] [Google Scholar]
- Memisevic H, Sinanovic O. Executive function in children with intellectual disability – the effects of sex, level and aetiology of intellectual disability. Journal of Intellectual Disability Research. 2014;58(9):830–837. doi: 10.1111/jir.12098. [DOI] [PubMed] [Google Scholar]
- Miller MR, Giesbrecht GF, Müller U, McInerney RJ, Kerns KA. A latent variable approach to determining the structure of executive function in preschool children. Journal of Cognition and Development. 2012;13(3):395–423. doi: 10.1080/15248372.2011.585478. [DOI] [Google Scholar]
- Parker SE, Mai CT, Canfield MA, Rickard R, Wang Y, Meyer RE, et al. Updated national birth prevalence estimates for selected birth defects in the United States, 2004–2006. Birth Defects Research Part A, Clinical and Molecular Teratology. 2010;88(12):1008–16. doi: 10.1002/bdra.20735. [DOI] [PubMed] [Google Scholar]
- Pritchard AE, Kalback S, McCurdy M, Capone GT. Executive functions among youth with Down syndrome and co-existing neurobehavioural disorders. Journal of Intellectual Disability Research. 2015;59:1130–1141. doi: 10.111/jir.12217. [DOI] [PubMed] [Google Scholar]
- Reynolds CR, Kamphaus RW. Behavior Assessment System for Children. Circle Pines, MN: American Guidance Service; 1992. [Google Scholar]
- Rowe J, Lavender A, Turk V. Cognitive executive function in Down’s syndrome. The British Journal of Clinical Psychology. 2006;45:5–17. doi: 10.1348/014466505X29594. [DOI] [PubMed] [Google Scholar]
- Toplak ME, West RF, Stanovich KE. Practitioner review: Do performance-based measures and ratings of executive function assess the same construct? Journal of Child Psychology and Psychiatry. 2013;54(2):131–143. doi: 10.1111/jcpp.12001. [DOI] [PubMed] [Google Scholar]
- Zelazo PD, Qu L, Müller U. Hot and cool aspects of executive function: relations in early development. In: Schneider R, Wolfgang, Schumann-Hengsteler, editors. Young Children’s Cognitive Development: Interrelationships Among Executive Functioning, Working Memory, Verbal Ability and Theory of Mind. Mahwah, New Jersey: Lawrence Erlbaum Associates Inc; 2005. pp. 71–95. [Google Scholar]
- Zigman WB, Lott IT. Alzheimer’s disease in Down syndrome: Neurobiology and risk. Mental Retardation and Developmental Disabilities Research Reviews. 2007;13:237–246. doi: 10.1002/mrdd.20163. [DOI] [PubMed] [Google Scholar]
- Zingerevich C, LaVesser PD. The contribution of executive functions to participation in school activities of children with high functioning autism spectrum disorder. Research in Autism Spectrum Disorders. 2009;3(2):429–437. doi: 10.1016/j.rasd.2008.09.002. [DOI] [Google Scholar]