

Abstract
Purpose:
As they grow, children develop their attitude and behavior related to tooth brushing by taking their parents’ oral-dental health behavior as an example. The purpose of this study was to assess whether there was a similarity in tooth brushing between primary school-age children and their parents presenting to the Department of Oral, Dental and Jaw Diseases and Surgery and the Department of Pedodontics, School of Dental Medicine, Istanbul University.
Patients and Methods:
The study included 126 children and their parents, as totally 252 subjects. The data on oral hygiene of the subjects were obtained using a questionnaire form including questions on the qualitative-quantitative tooth brushing habits of the children and their parents and the socio-demographic characteristics of their families.
Results:
In most of the cases, there was a similarity between children and their parents in terms of the frequency of dentist visits, the therapy they underwent in their last dentist visit, the cause of caries, the frequency of tooth brushing, the material used for oral hygiene, the duration of tooth brushing, method of tooth brushing, and tooth sites most brushed, which showed a significant association between children and their parents (p<0.01).
Conclusion:
Correct knowledge given to the children by their families will positively affect the oral-dental health of the children. Thus, firstly, correct knowledge should be given to the parents so that they can successfully carry out their responsibility in being the correct model for their children in oral-dental health.
Keywords: School-age children, oral hygiene, oral-dental health, tooth brushing habits
Introduction
Oral and dental hygiene is an important part of the concept of general health, which is influenced by the individual’s attempts to provide and maintain oral hygiene. The main aim in providing oral and dental hygiene is the control of the microbial dental plaque which is the primary etiologic factor. The other factors affecting oral and dental health are age, gender, race, habits, systemic condition, and the socioeconomic and cultural status (1). Accumulation of the complex-structured microbial plaque on dental surfaces and its ineffective removal lead to deterioration of oral-dental health caused by the toxins of the plaque microorganisms (2, 3, 4, 5). Currently, caries and periodontal diseases caused by microbial dental plaque are among the basic health problems of a great part of the world population (6). In 1981, as one of the global aims, The World Health Organization (WHO) and the World Dental Federation (FDI) suggested a Decayed, Missing, Filled Tooth (DMF-T) value not surpassing 3 at age 12 to be reached by the year 2000 (7). According to the Global Oral Health Data Bank, our country is still represented by the results of the first study performed in 1988. Based on this report, the rate of no caries is 16% in children aged 6, 19% in children aged 12, and 3% in the 30-35 age group. The DMF-T values have been reported to be 3.16 for age 12, 7 for age 20-24, and 12.24 for age 35-44 (8, 9). The aims of WHO related to oral-dental health for the 21st century are a rate of 80% without caries in children aged 6 and a DMT value of 1.5 in children aged 12 (10). Tooth brushing is a simple, effective, and the most preferred method for removal of microbial dental plaque (11, 12). As risk factors, when the attitudes and habits related to oral hygiene are considered, the families are greatly responsible for training their children on oral hygiene, starting at a very young age and thus, for establishing a positive behavior towards oral-dental hygiene.
Patients and Methods
Population characteristics
The study included 126 children of primary schoolage and their parents presenting to the Department of Oral Medicine and Surgery and Department of Pedodontics, Faculty of Dentistry, Istanbul University. Of the children, 9.5% had presented for control, 9.5% for tooth extraction, 17.5% for orthodontic therapy, 27.8% for tooth filling, and 35.7% for pain. The subjects were asked to fill in a questionnaire that consists of 23 questions on socio-demographic features of the family, habits and awareness of tooth brushing. Subsequently, the subjects’ DMF-T indices were determined through intra-oral examination.
Statistical analysis
The SPSS (Statistical Package for Social Sciences) for Windows 15.0 software was used for the statistical analysis of the data obtained. Apart from the descriptive statistical methods (mean, standard deviation, frequency), since the parameters did not demonstrate a normal distribution compared to the qualitative data, the Kruskal-Wallis test was used for the comparison of parameters between the groups and the Mann-Whitney U test was used for the determination of the group causing the difference. The Mann-Whitney U test was performed for comparison of the parameters in the two groups. The Chi-square test and the Fisher’s exact chi-square test were used for the comparison of qualitative data. P values of p<0.05 were accepted as statistically significant.
Results
The study group included 126 children and their parents, totally 252 subjects. Of the children, 19.8% (n=25) were aged 4-7, 60.3% (n=76) aged 8-11, and 19.8% (n=25) were aged 12-15, and 57.1% (n=72) were girls and 42.9% (n=54) were boys. Of the parents, 15.9% (n=20) were in the 25-30 age group, 24.6% (n=31) in the 30-35, 46% (n=58) in the 35-45, and 13.5% (n=17) in the 45-55 age group. Among the parents, only 1 was illiterate; 75.4% (n=95) were in primary school, 19% (n=24) were in senior high school, and 4.8% (n=6) were university graduates. The parents and children were grouped according to their health status as follows: healthy parents + healthy children, 102 groups; healthy parents + children with health problems, 17 groups; parents with health problem + healthy children, 6 groups; and parents with health problem + children with health problem, 1 group (Figure 1).
Figure 1.
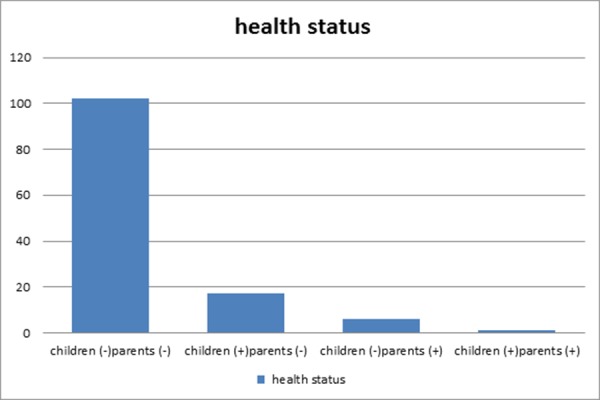
Health status of children and parents.
The frequency of dentist visits by parents was determined as follows: 1 parent visited the dentist once every 3 months, 4 parents visited the dentist once every 6 months, 5 parents once a year, 111 parents visited the dentist when a dental problem occurred, 3 parents never visited a dentist, and 2 could not visit the dentist due to dentist phobia. The frequency of dental visits by children who had been taken to the dentist by their parents was as follows: 11 children had been taken to the dentist once every 3 months, 25 children once every 6 months, 12 children once a year, 68 children when a dental problem occurred, and 10 children had been taken to the dentist for the first time (Figure 2). When the frequency of dental visits by groups of parents+children was evaluated, it was seen that each of the 71 groups shared the same frequency. Among these 71 groups, 66 groups had visited the dentist only when they had a dental problem and 3 groups had visited the dentist once every 6 months. Among the groups where parents and children gave different answers, the most frequent situation (30.9%) was parents visiting the dentist when a dental problem occurred and their children visiting the dentist once every 6 months. There was a statistically significant relationship in the frequency of visits between the parents and their children. The children whose parents visited the dentists when a dental problem occurred; the children who visited the dentist upon a dental problem, like their parents (p<0.01); the children whose parents made dental visits every 3-6 months the children who made visits to the dentists once every 3-6 months like their parents (p<0.05), and the children whose parents visited the dentist at other times went to the dentist once every 3-6 months (p<0.05).
Figure 2.
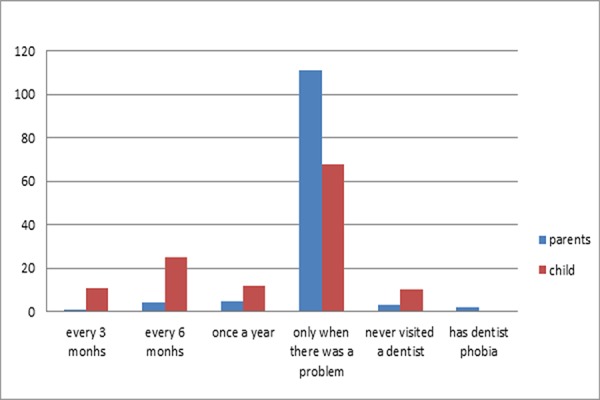
Frequency of dental visit by parents and their children.
There was no significant difference in the frequency of dentist visits by parents in terms of educational level (p>0.05). The rates of dental visits upon a dental problem by primary school graduates as well as by high school and university graduates were determined to be high. When the parents were asked to answer the question “What do you think is the cause of caries?” by scoring from 1 to 10, the multiple choices already given and/ or added by themselves, the reply in the first line in 69% of the cases was insufficient oral hygiene. As the cause of caries, 12.7% of the parents gave the highest score to junk food, 7.9% to genetic disposition, 3.2% to irregular nutrition, 2.4% to medications, and 2.4% to dental structure. The other answers, with a rate of under 1% for each, were pregnancy, eating cold and warm food together, and no idea. When the children were asked “What do you think is the cause of caries?”, the answers and their rates were as follows: insufficient oral hygiene by 46.8%; eating junk food by 44.4%; irregular nutrition by 3.2%, dental structure by 3.2%; genetic by 1.6%; and biting hard things-food by 0.8%. Thus, there was a significant association between the parents and their children in terms of what they thought as the cause of caries. The children whose parents answered junk food as the cause of caries, gave the answer of junk food like their parents (p<0.01); the children whose parents answered insufficient oral hygiene like their parents, gave the answer of insufficient oral hygiene (p<0.01); and the children whose parents stated other reasons gave the answer of other reasons like their parents (p<0.01) (Table 1).The frequencies of tooth brushing by the parents were as follows: 51.6% twice a day, 33.3% once a day, 7.9% every other day, 4% more than twice a day, 1.6% twice a week, and 1.6% never. The frequencies of tooth brushing by the children were as follows: 45.2% twice a day, 35.7% once a day, 8.7% every other day, 8.7% twice a week, and 1.6% more than twice a day. When the parents and their children were asked to answer the question, “How frequently do you brush your teeth?”, 70 parents and their children stated the same frequency.
Table 1.
The causes of tooth decay.
| Children | |||||
|---|---|---|---|---|---|
| Eating junk food | Poor oral hygiene | Others | |||
| n(%) | n(%) | n(%) | p | ||
| Parents | Eating junk food | 15(26.8%) | 1(1.7%) | 0(0%) | |
| Poor oral hygiene | 31(55.4%) | 52(88.1%) | 4(36.4%) | 0.001 | |
| Others | 10(17.9%) | 6(10.2%) | 7(63.6%) | ||
There was a statistically significant association in the frequency of tooth brushing between the parents and their children The children whose parents brushed their teeth once a day, brushed their teeth once or more than twice a day, like their parents (p<0.01), and the children whose parents brushed teeth twice a day, like their parents, brushed their teeth twice a day (p<0.01). There was no significant difference in the frequency of tooth brushing between the parents in terms of educational level (p>0.05). The rates of tooth brushing twice a day were high in primary school graduates as well as in high school and university graduates. To the question “At what times of the day do you brush your teeth?”, 50% of the parents aswered before breaksfast in the morning and before going to bed. Of the parents, 15.1% brushed their teeth only after breakfast in the morning, and 19% only before going to bed. Again of the parents, 3.2% brushed their teeth only in the evening, 0.8% at noon and in the evening, 2.4% before breakfast and before going to bed, 2.4% at changing times, and 2.4% after breakfast, in the evening, and before going to bed. It was found that those brushing their teeth twice a day, did the brushing after breakfast and before going to bed. Of the children, 45.2% stated that they brushed their teeth after breakfast and before going to bed, 19% after breakfast, 15.9% before going to bed, 12.7% at changing times, 2.4% after breakfast and in the evening, and 1.6% before breakfast; 1 child answered “at noon and in the evening”, 1 child “only in the evening”, 1 child “before breakfast and before going to bed”, and 1 child answered “after breakfast, in the evening, and before going to bed”. It was determined that timewise, both parents and their children preferred to brush teeth after breakfast and before going to bed. To the question “At what times of the day do you brush your teeth?”, the same time was shared within each of the 70 groups.
The results showed that there was a statistically significant association between the parents and their children in terms of the tooth brushing time. The children whose parents brushed their teeth after breakfast and before going to bed, did the tooth brushing at the times their parents did (p<0.01), and the children whose parents did the brushing at other times, also did the brushing at the times their parents did (p<0.01). Of the parents, 80.2% stated that they used only toothbrush and tooth- paste for oral hygiene. Among the parents, 9.5% used toothbrush, toothpaste, and mouthwash; 5.6% used toothbrush, toothpaste, and dental floss; 1.6% used toothbrush, toothpaste, and toothpicks, and only 1 parent used toothbrush,toothpaste, dental floss, and toothpick; 3 parents used no material for oral hygiene. Among the children, for oral hygiene, 96.8% used toothbrush and toothpaste and 3.2% used mouthwash additionally. When the materials used by both the parents and their children were considered, it was determined that 104 parents and their children used toothbrush and toothpaste for oral hygiene. Thus, there was a statistically significant association between the parents and their children in terms of the material used for oral hygiene. The children whose parents used toothbrush and toothpaste for oral hygiene, like their parents, used toothbrush and tooth- paste (p<0.01).
When the duration of tooth brushing was inquired, it was found that 53.2% (n=67) of the parents brushed for more than 2 minutes, 21.4% for less than 2 minutes, 19.8% for less than 1 minute, 3.2% for 2 minutes, and 0.8% at variable durations. Of the children, 41.3% brushed their teeth for more than 2 minutes, 35.7% for less than 1 minute, 21.4% for less than 2 minutes, and 1.6% for 2 minutes. When the duration of tooth brushing was evaluated, it was found that within each of 76 groups, the same length of time was shared. Thus, of the groups comrising the parent and the child, 41 groups brushed their teeth for more than 2 minutes, 17 groups for less than 1 minute, 16 groups for less than 2 minutes, and 2 groups for 2 minutes. The children whose parents brushed teeth for 2 minutes or longer, did tooth brushing for 2 minutes or longer, like their parents. The rates of tooth brushing for 2 minutes or longer and renewing the toothbrush once every 3 months by children of high school and university graduate parents were higher than those of children of primary school graduates, but the difference was insignificant (p>0.05). The answers of the parents to the question “ Which part of your teeth do you care to be the cleanest?” were as follows: 54%, all teeth; 24.6%, front teeth; 9%, back teeth; 1.6% vestibular/buccal surfaces; and 0.8%, palatinal/ lingual surfaces.
Of the children, 35.7% cared for brushing all teeth, 4.9% for mostly the front teeth, and 24.9% for mostly the back teeth. When the most brushed part of the teeth was inquired, the parent-child answers were the same in 60 groups. Accordingly, the parents and their children in 32 groups cared most for cleanliness of all teeth, in 16 groups, mostly for the back teeth, and in 12 groups, mostly for the front teeth. There was a significant relationship between the parents and their children in terms of teeth that they most cared for. The children whose parents cared for the cleanliness of all teeth, like their parents, cared for the cleanliness of all teeth. As to the technique of brushing, of the parents 27% brushed their teeth with circular movements, 25.4% with right-left/up-down/circular movements, 18.3% with right-left/up-down movements, 17.5% with up-down movements, and 10.3% with right-left movements. Of the children, 31.7% did tooth brushing with circular, 23% with up-down/right-left, 20.6% with up-down, 12.7% with right-left, and 11.9% with right-left/up-down/circular movements. The parents and their children brushed their teeth with the same technique. The children whose parents brushed teeth with circular movements, brushed their teeth with circular movements, like their parents, (p<0.01), and the children whose parents brushed their teeth with up and down movements, like their parents, did brushing with up and down movements (p<0.01). The children whose parents brushed their teeth with right-left movements, did brushing with rightleft movements, like their parents (p<0.01, and the children whose parents brushed teeth with right-left/ up-down/circular movements, like their parents, brushed their teeth with right-left/up-down/circular movements (p<0.01) (Table 2).
Table 2.
The technique of brushing.
| Children | ||||||
|---|---|---|---|---|---|---|
| Brushing technique | circular | up-down | right-left | right-left/up-down | p | |
| n(%) | n(%) | n(%) | n(%) | |||
| Parents | circular | 49(%89,1) | 10(%38,5) | 4(%25,0) | 3(%11,1) | 0.001 |
| up-down | 3(5.5%) | 15(57.7%) | 2(12.5%) | 2(7.4%) | ||
| right-left | 3(5.5%) | 1(3.8%) | 10(62.5%) | 22(81.5%) | ||
According to the results of the questionnaire, 55.6% of the children were not controlled by their parents as they brushed their teeth, 35.7% were controlled, and 8.7% were sometimes controlled. When the parents were asked “Does your child regularly brush teeth? If not, what is the reason?”, 18.3% answered that their children regularly brushed their teeth; the reason for irregular brushing was given by 2.4% of the parents as lack of training, by 23% as lack of motivation, by 15.9% as forgetfullness, by 38.9% as overlooking, and by 18.3% as lack of oral hygiene material. All children had their own toothbrushes and did not use the toothbrushes of other family members. Among the parents, 121 stated that they changed their own and their children’s toothbrushes at the same intervals of time. The children whose parents changed their toothbrushes once every 3 months, like their parents, had their toothbrushes renewed once in 3 months. Of the children, 92.1% had learnt tooth brushing from their parents, 3.2% by themselves, 4% at school, and 0.8% from a dentist. According to the statements of the parents, 38.9% of the children first started brushing their teeth at age 2-3, 40.5% at age 3-5,18.3% at age 5-7, and 1.6% at age 9-11. Only 1 child started tooth brushing after age 11.
According to the parents’ DMF-T index results, 18 and 14 parents had the highest values of DMF-T=5 and DMF-T=6, respectively. When the parents’ highest DMF-T values were compared with the children’s DMF-T and dmf-t values, the following were found: In groups where the parents had DMF-T=5, there were 4 children with dmft=0, whose DMF-T values were 1, 3, 4, and 5, respectively. Furthermore, in 18 groups, where the parents had DMF-T=5, the DMF-T values of 10 children were 0. Five children with DMF-T=0, whose parents had DMF-T=5, had dmf-t index values of 2, 4, 5, 6, 7, and 9, respectively. In 14 groups where the parents had DMF-T=6, there were 4 children with a dmf-t value of 0, and the DMF-T values of these children were 0, 1, 2, and 3, respectively. Eight children in the 14 groups where the parents had DMF-T=6, were determined to have DMF-T=0, and in this group only 1 child had both dmf-t=0 and DMF-T=0 values. In 13 groups where the parents had DMF-T=9, there were only 3 children with DMF-T=0 and dmf-t values of 3, 5, and 6, respectively. Among the 13 groups, there were 2 children with dmf-t=0 and DMF-T values of 1 and 4, respectively. The mean DMF-T and dmf-t values of children whose parents had DMF-T=5 were 1.27 and 3.22, respectively. The mean DMF-T and dmf-t values of children whose parents had DMF-T=6, were calculated as 1.07 and 2.28, respectively. The mean DMF-T and dmf-t values of children whose parents had DMF-T=9 were determined as 1.15 and 5.3, respectively. The mean DMF-T and dmf-t values of children whose parents had DMF-T=10, were calculated as 1 and 4.8, respectively.
There was a statistically significant difference between the DMFT values of the children in terms of frequency of tooth brushing (p<0.05). The DMFT values of children brushing their teeth once a day were significantly higher than those of children brushing their teeth twice a day (p:0.028) and more than twice a day (p<0.05). There was no statistically significant difference in dmft and DMFT values between children brushing teeth twice a day and those brushing more than twice a day (p>0.05). Furthermore, there was no statistically significant difference between dmft and DMFT values of children in terms of the duration of brushing (p>0.05).
Discussion
The aim of the WHO with regard to dental caries for the year 2000 was over 50% prevalence of no caries in 5-6 year-old children (13). The aim of the WHO for the year 2020 is an 80% prevalence of no caries in the 6-age group children (14). Milnes (15) has reported that the dental caries prevalence is 1-12% in developed countries, whereas it rises up to 70% in developing countries. Bilgili (16) has stated that 90.7% of the parents take their children to the dentist when a dental problem occurs, but 9.3% take their children to the dentist for a dental control once or twice a year. The results of our study are similar to these results. We found that generally, both the parents and their children visited the dentist when a dental problem occurred.
Astrom and Jakobsen (17) have reported that the behavior of the parents towards dental health is a model copied by their children. Positive behavior of the parents, such as tooth brushing, is an important model for the children in the family (17). The intensity and duration of communication between the child and the parents are important for the formation of this model, and the parents’ behavior towards oraldental health directly affects the child’s oral hygiene behavior until adolescence (16). In our study, the data found on behavior similarities between parents and their children are consitent with the results of Astrom and Jakobsen (17).
About 40% of our population occasionally brush teeth and 26% of them brush their teeth 2-3 times a day (18). In our study, most of the parents and children stated that they brushed teeth 2 times a day. Those individuals brushing their teeth at least twice a day and those who had learned this practice at early age have relatively fewer dental caries. Brushing teeth once a day does not provide sufficient cleaning and leads to reformation of bacterial plaque (19). In our study, we found that the DMFT values of children who brushed their teeth twice or more than twice a day were lower than those of children who brushed teeth less often, a result which is compatible with the results of the mentioned study. Children in families of low educational level brush their teeth less frequently. Oral health is associated with life standards and educational level (20). Tulunoğlu et al. (1) and Güngör et al. (2) have reported that the habitual practice of tooth brushing increases with the increase in educational level, leading to improved oral-dental health. In our study, there was no significant difference in the frequency of tooth brushing by parents in terms of educational level. Moreover, we found no association between the educational level of the parents and their children’s tooth brushing habits. We think that these results are caused by the primary school-graduate parents who comprised the majority in our study. Namal et al. (21) have reported an association between the mother’s level of knowledge of dental health, and DMFT, which shows the level of dental health and child’s dental health level. Parallel to this finding, we determined that the parent’s oral-dental health knowledge and attitude affected the child’s behavior towards oral-dental health and its results. According to Al-Omiri et al. (22), only 26% of the parents follow and guide their children during tooth brushing. The results of our study is consistent with this finding.
Conclusion
According to our findings, with children copying the model of parents’ knowledge, positive attitude and behavior related to oral-dental health, it can be possible to realize the aim “health for all” of the WHO. Correct knowledge given to the children by their families will positively affect the oral-dental health of the children. When the level of knowledge of the parents is insufficient for the correct guidance of their children, the responsibility of the second socialization will increase, and thus the children’s positive attitude and behavior, which should start at an early age, will be delayed. Consequently, wrong habits related to oral-dental health will be acquired. There are similarities and a significant association between most parents and their children in terms of the frequency of dentist visits, the therapy given in the last dentist visit, the cause of dental caries, the frequency of tooth brushing, the duration of tooth brushing, the technique of tooth brushing, and the teeth most brushed. Thus, correct knowledge should be given to the parents so that they can successfully carry out their responsibility of being the correct role-models for their children.
Footnotes
Source of funding: None declared.
Conflict of interest: None declared.
This study was presented in 2012 as a graduation thesis under the supervision of Prof.Dr.Meral Unur in Istanbul University, Faculty of Dentistry.
References
- 1.Tulunoglu O, Bodur H, Akal N. Aile eğitim düzeyinin okul öncesi çocuklardaki ağız diş sağlığı uygulamaları üzerine etkisinin değerlendirilmesi. Gazi Üniv Diş Hekim Fak Derg. 1999;16(2):27–32. [Google Scholar]
- 2.Güngor K, Tüter G, Bal B. Eğitim düzeyi ile ağız sağlığı arasındaki ilişkinin değerlendirilmesi. Gazi Üniv Diş Hekim Fak Derg. 1999;16(1):21–25. [Google Scholar]
- 3.Kallestal C, Matsson L. Periodontal conditions in a group of Swedish adolescents. (II) Analysis of data. J Clin Periodontol. 1990;17(9):609–612. [PubMed] [Google Scholar]
- 4.Özmeriç N, Göfteci B, Kutiş B, Bal B. Arayüz bakımı ve periodontal sağlık. Gazi Üniv Diş Hekim Fak Derg. 1994;11(2):33–38. [Google Scholar]
- 5.Öztunç H, Haytaç MC, Özmeriç N, Uzel I. Adana ilinde 6-11 yaş grubu çocukların ağız ve diş sağlığı durumlarının değerlendirilmesi. Gazi Üniv Diş Hekim Fak Derg. 2000;17(2):1–6. [Google Scholar]
- 6.Kouzmina E, Janushevitch O, Smirnova T, Kuzmina I. Oral health status of 12 year-old children in Russia. Pravention und Gesundheitsförderung. 2009;4:131–134. [Google Scholar]
- 7.Global goals for oral health in the year 2000. Fédération Dentaire Internationale. Int Dent J. 1982;32(1):74–77. [PubMed] [Google Scholar]
- 8.Saydam G, Oktay I, Möller I. Dünya Sağlık Örgütü Avrupa Bölgesi. Sağlık Bakanlığı; Ankara: 1990. Türkiyede Ağız Diş Sağlığı Durum Analizi. [Google Scholar]
- 9.Petersen PE, Ogawa H. Strengthening the prevention of periodontal disease: The WHO approach. J Periodontol. 2005;76(12):2187–2193. doi: 10.1902/jop.2005.76.12.2187. [DOI] [PubMed] [Google Scholar]
- 10.Mann ML. In: Planning for community dental programs Jong’s community dental health. Gluck GM, Morganstein WM, editors. St. Louis: Mosby Year Book Inc; 1990. pp. 3–24. [Google Scholar]
- 11.Fischman SL. The history of oral hygiene products: how far have we come in 6000 years? Periodontol 2000. 1997;15:7–14. doi: 10.1111/j.1600-0757.1997.tb00099.x. [DOI] [PubMed] [Google Scholar]
- 12.Koivusilta L, Honkala S, Honkala E, Rimpela A. Toothbrushing as part of the adolescent lifestyle predicts education level. J Dent Res. 2003;82(5):361–366. doi: 10.1177/154405910308200507. [DOI] [PubMed] [Google Scholar]
- 13.Aggeryd T. Goals for oral health in the year 2000: cooperation between WHO, FDI and the national dental associations. Int Dent J. 1983;33(1):55–59. [PubMed] [Google Scholar]
- 14.WHO Health 21: The health for policy framework for the WHO European Region European Health for all series No.6 [Internet] Copenhagen (Denmark): World Health Organization Regional Office for Europe; 2000. Available from: http://www.euro.who.int/__data/assets/pdf_file/0010/98398/wa540ga199heeng.pdf?ua=1 . [Google Scholar]
- 15.Milnes AR. Description and epidemiology of nursing caries. J Public Health Dent. 1996;56(1):38–50. doi: 10.1111/j.1752-7325.1996.tb02394.x. [DOI] [PubMed] [Google Scholar]
- 16.Bilgili Ş. Kliniğimize başvuran çocuklar ile ebeveynlerinin diş sağlığının değerlendirilmesi ve sosyodemografik faktörlerle ilişkisinin araştırılması [dissertation] Istanbul: T.C. Sağlık Bakanlığı; 2009. 69 p. Available from: http://www.istanbulsaglik.gov.tr/w/tez/pdf/aile_hekimligi/dr_sengul_bilgili.pdf . [Google Scholar]
- 17.Astrom AN, Jakobsen R. Stability of health dental behavior: a 3-year prospective cohort study of 15-, 16- and 18-year-old Norwegian adolescents. Community Dent Oral Epidemiol. 1998;26(2):129–138. doi: 10.1111/j.1600-0528.1998.tb01939.x. [DOI] [PubMed] [Google Scholar]
- 18.Yaramış N, Karataş N, Ekti F, Aslantaş D. Nevşehir il merkezinde bulunan ilköğretim çağındaki çocukların ağız sağlığı durumu ve alışkanlıklarının belirlenmesi. Sted. 2005;14(12):256–259. [Google Scholar]
- 19.Amarente E, Raadal M, Espelid I. Impact of diagnostic criteria on the prevalance of dental caries in Norvegian children aged 5, 12 and 18 years. Community Dent Oral Epidemiol. 1998;26(2):87–94. doi: 10.1111/j.1600-0528.1998.tb01933.x. [DOI] [PubMed] [Google Scholar]
- 20.Haznedaroğlu D. Türkiye'de beslenme durumu ve çalışmalar. III. Uluslar arası beslenme ve diyetetik kongresi. Beslenme ve Diyet Dergisi. 2001;30(1):51–54. [Google Scholar]
- 21.Namal N, Vehid HE, Vehid S, Can G. Altı-on iki yaş grubu çocukların diş sağlığını etkileyen anneye ait faktörlerin araştırılması. Çocuk Dergisi. 2009;9(3):123–126. [Google Scholar]
- 22.Al-Omiri MK, Al-Wahadni AM, Saeed KN. Oral health attitudes, knowledge, and behavior among school children in North Jordan. J Dent Educ. 2006;70(2):179–187. [PubMed] [Google Scholar]