

Abstract
[Purpose] This study assessed the relationships between the ankle dorsiflexion range of motion and foot and ankle strength. [Subjects and Methods] Twenty-nine healthy (young adults) volunteers participated in this study. Each participant completed tests for ankle dorsiflexion range of motion, hallux flexor strength, and ankle plantar and dorsiflexor strength. [Results] The results showed (1) a moderate correlation between ankle dorsiflexor strength and dorsiflexion range of motion and (2) a moderate correlation between ankle dorsiflexor strength and first toe flexor muscle strength. Ankle dorsiflexor strength is the main contributor ankle dorsiflexion range of motion to and first toe flexor muscle strength. [Conclusion] Ankle dorsiflexion range of motion can play an important role in determining ankle dorsiflexor strength in young adults.
Key words: Dorsiflexor strength, Toe flexor, Weight-bearing lunge test
INTRODUCTION
Limited ankle dorsiflexion range of motion (DF ROM) has been associated with several clinical manifestations such as ankle joint equinus1), patellar injuries2), and ankle injuries3). Restricted ankle dorsiflexion may also lead to abnormal lower extremity biomechanics during closed chain strengthening exercises4). Backman et al.5) showed that a low DF ROM in weight-bearing value represents a risk factor for developing patellar tendinopathy in junior elite basketball players because of load-bearing compensation in the patellar tendon. Reduced DF ROM during weight bearing may also increase the risk of patellar tendinopathy in volleyball players2). Moreover, DF ROM during weight bearing was a predictor of dynamic balance in healthy adults and individuals with chronic ankle instability6). Impaired ankle DF ROM during a squat can also result in increased knee valgus and medial knee displacement, as well as reduced activation of the quadriceps and increased activation of the soleus4).
Muscle strength in the lower extremities is an essential element of physical therapy evaluation and can significantly impact activities involving walking ability and the prevention of sports injuries. Intrinsic foot muscles play a key role by supporting the medial longitudinal arch in static stance. Disrupting the function of these muscles through fatigue resulted in an increase in pronation as assessed by navicular drop7). Some studies have shown that intrinsic foot flexors are important for the dynamic stabilization of the arches of the feet, enabling a more efficient exertion of extrinsic foot flexor muscle force, and thus leading to an improvement in walking performance7, 8). Kibler et al.9) compared strength of the ankle joint plantar flexor muscles and the flexibility of the triceps surae in feet with plantar fasciitis to those in feet without plantar fasciitis. These authors reported significant strength deficits and tightness of the triceps surae for the lower extremities in which plantar fasciitis was present.
Reduced toe flexor strength (TFS) is an independent predictor of falls in older people10). TFS is very important for various movements, including standing11) and walking12, 13). When walking, an individual’s toes are in contact with the ground for 75% of the stance phase12) and long toe flexor muscles help control forward progression of the leg over the foot14). Aging is associated with reduced plantarflexion strength (PFS) of the toes15). Yun et al.16) reported that toe flexor muscle strength and DF ROM are the main contributors to countermovement jump performance; however, the associations between DF ROM in weight bearing and TFS, dorsiflexion strength (DFS), and PFS, of the ankle are not well known in young adults. Therefore, the aim of the present study was to investigate the relationships between ankle DF ROM and foot and ankle strength.
SUBJECTS AND METHODS
Twenty-nine active male students (age: 21.2 ± 2.5 years, body weight: 75.9 ± 21.3 kg, height: 170.6 ± 19.9 cm) participated in this study. All participants were injury-free. Exclusion criteria were (1) any cardiovascular, respiratory, abdominal, neurological, musculoskeletal, or other chronic disease, and (2) any symptoms that could affect the musculoskeletal system. This research project was conducted according to the Declaration of Helsinki and was approved by the University Review Board for use of Human Subjects.
Participants began with a warm-up consisting of 5 minutes of low-resistance (85 W; 80 RPM) cycling on an ergometer. Ankle dorsiflexion was evaluated through the LegMotion system (LegMotion, Check your MOtion, Albacete, Spain)3, 17). All subjects started with their hands on the hips and placed the assigned foot on the middle of the longitudinal line just behind the transversal line on the platform. The alternate foot was placed out of the platform with the toes at the edge of the platform. While maintaining this position, subjects were instructed to perform a lunge in which the knee was flexed with the goal of making contact between the anterior knee and the metal stick. When the subjects were able to maintain heel and knee contact, the metal stick was moved away from the knee. The distance achieved was then recorded in centimeters. Three trials were performed for each ankle (i.e., dominant and non-dominant) with 10 seconds of passive recovery between trials. The third value in each ankle was selected for subsequent analysis of weight-bearing DF ROM. The participants’ dominant leg was defined by their preference for kicking.
The subjects sat with hips, knees, and ankles bent to 90 degrees in an adjustable-height chair with the tibia perpendicular to the floor and the foot resting on the floor. Each subject performed maximal voluntary isometric contraction of plantar flexion of the first metatarsophalangeal joint of the big toe (TFS) for 3 seconds to determine maximal voluntary contraction (MVC) torque. MVC torque was measured at a neutral position of the ankle and metatarsophalangeal joints. To ensure accurate positioning of the hallux onto the JTech Medical Commander™ (Midvale, UT, USA) load cell and to minimize the influence of the extrinsic muscles of the foot (ankle plantarflexors and flexor hallucis longus) and the second to fourth toes, a purpose-built wooden platform was constructed and positioned under the load cell. As shown in Fig. 1, this permitted the tested foot to be positioned such that the proximal metatarsophalangeal joint of the big toe was positioned at the edge of the platform. A strap and an examiner stabilized the foot to secure the anterior section of the foot onto the platform.
Fig. 1.
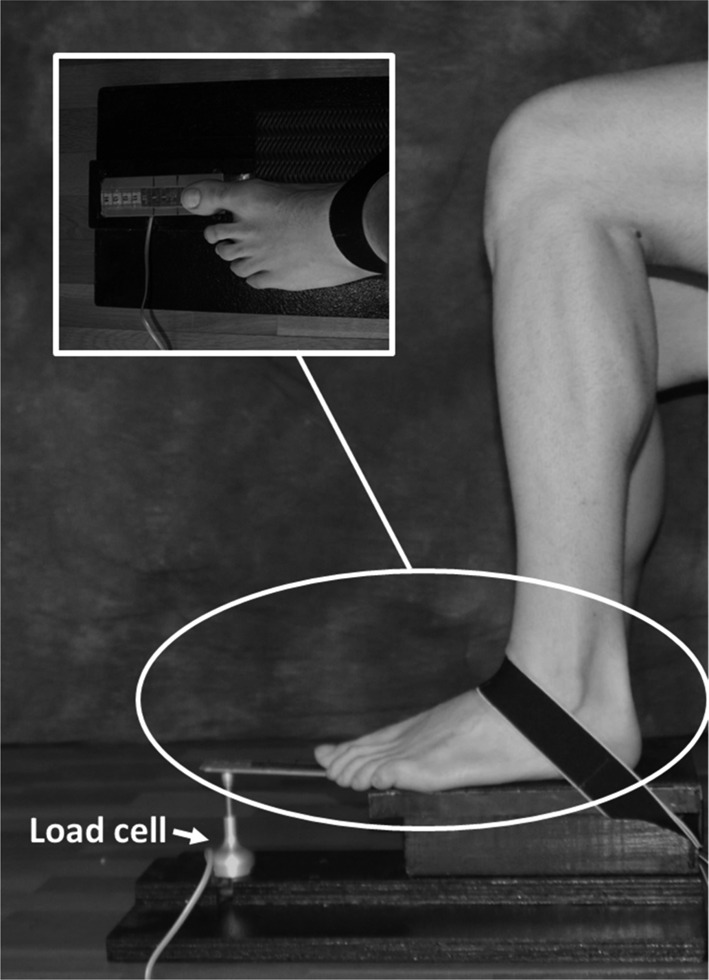
Toe flexor strength setup
A custom-made ankle strength device was used to measure plantarflexion and dorsiflexion torque. Subjects were seated on a chair, with their trunk, thighs, lower thighs, and feet fastened to the chair and the torque meter device. DFS and PFS were calculated as the tensile and compressive force using a strain gauge (Winlaborat V4.20, Buenos Aires, Argentina) (Fig. 2).
Fig. 2.
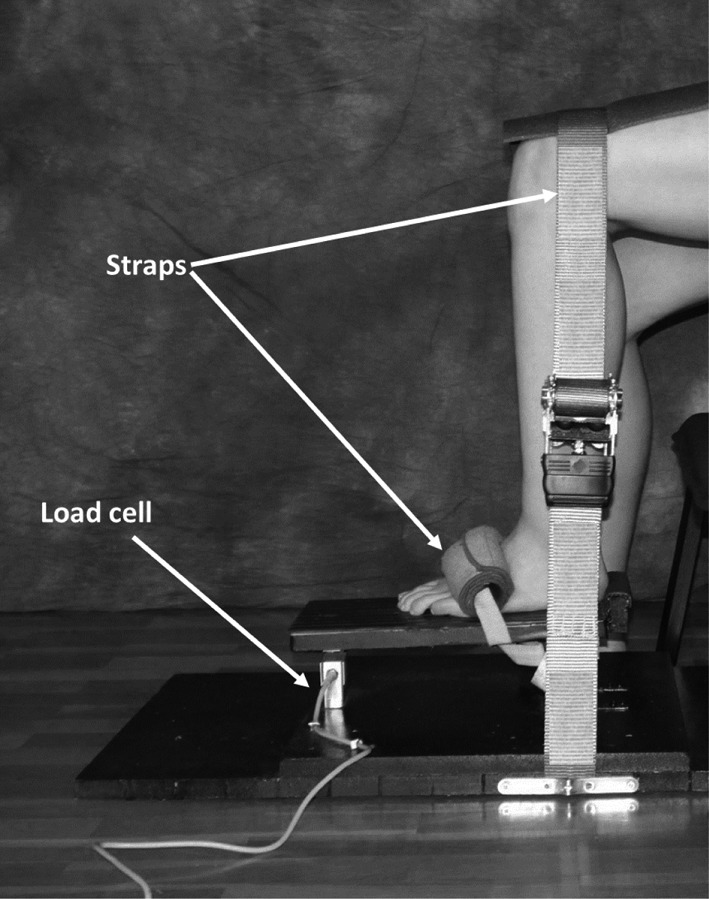
Dorsiflexion and plantarflexion strength setup
Measured MVC torque values were normalized by body weight (kg/bw). Participants then performed three trials at maximal effort with a 1-minute rest period between trials to minimize muscle fatigue. The average of three consistent measures was then calculated. Then, we re-measured MVC torque on a different day to determine the test-retest repeatability of such measurements by calculating intra-class correlation coefficient (ICC).
Data were analyzed using PASW/SPSS Statistics 20 (SPSS Inc., Chicago, IL, USA) for Windows. The paired t-test was used to compare data between the right and left sides. Pearson correlation coefficients (r) were used to determine the strength and directionality of relationships among the different variables (DF ROM, TFS, DFS, and PFS). A correlation coefficient (r) of 0 to 0.4 was considered to represent a weak relationship, a coefficient of 0.4 to 0.7 was considered to represent a moderate relationship, and a coefficient of 0.7 to 1.0 was considered to represent a strong relationship18). All data are presented as means and standard deviations. In all analyses, p<0.05 was understood to indicate statistical significance.
RESULTS
The ICCs of TFS, DFS, and PFS were 0.89, 0.84, and 0.86, respectively.
Table 1 shows variables for the right and left side, along with a comparison of these data. There were no statistically significant differences (p≥0.05) between the dominant and non-dominant side for any variable tested.
Table 1. Mean and standard deviation and the comparison of dominant and non-dominant (n=29).
| DF ROM_Dominant (cm) | 11.41 ± 4.08 | p>0.05 |
| DF ROM_Non-dominant (cm) | 11.36 ± 2.90 | |
| TFS_Dominant (kg/bw) | 0.84 ± 0.38 | p>0.05 |
| TFS_ Non-dominant (kg/bw) | 0.82 ± 0.36 | |
| DFS_ Dominant (kg/bw) | 0.48 ± 0.12 | p>0.05 |
| DFS_ Non-dominant (kg/bw) | 0.48 ± 0.13 | |
| PFS_ Dominant (kg/bw) | 1.42 ± 0.34 | p>0.05 |
| PFS_ Non-dominant (kg/bw) | 1.48 ± 0.43 |
DF ROM: dorsiflexion range of motion; TFS: toe flexor strength; DFS: dorsiflexion strength; PFS: plantarflexion strength
Table 2 shows the Pearson’s correlation coefficients between DF ROM, PFS, PFS, and TFS in the participants tested. DFS showed a moderate correlation with DF ROM (r=0.473, p<0.001) and with TFS (r=0.516, p<0.001). The linear regression equations were between DFS and DF ROM (y=0.0149x + 0.3019; y=DFS) and DFS and TFS (y=0.1529x + 0.3507; y=DFS). However, the relationships between PFS and TFS were weak (r=0.397, p<0.001).
Table 2. Correlation coefficients (n=58 limbs).
| DF ROM | TFS | DFS | PFS | |
|---|---|---|---|---|
| DF ROM | 1.0 | 0.279* | 0.473** | −0.139 |
| TFS | 0.279* | 1.0 | 0.516** | 0.397** |
| DFS | 0.473** | 0.516** | 1.0 | 0.153 |
| PFS | −0.139 | 0.397** | 0.153 | 1.0 |
*p<0.05; **p<0.001. DF ROM: dorsiflexion range of motion; TFS: toe flexor strength; DFS: dorsiflexion strength; PFS: plantarflexion strength
DISCUSSION
The main findings of the present study show a moderate correlation between ankle DF ROM and dorsiflexor strength, as well as a moderate correlation between dorsiflexor strength and flexor muscle strength in the first toe.
Another interesting finding was that none of the variables we measured showed any statistical relevance when compared between the dominant and non-dominant side. Therefore, the present study suggests that there are no important differences between the dominant and non-dominant foot and ankle in healthy subjects. In this sense, similar data were reported by van der Harst et al.19), who found no significant differences in most of the kinematic and kinetic data between the dominant leg and the contralateral leg during multi-articular movement as a single-leg hop for distance.
Ankle dorsiflexion motion is important in multi-directional running tasks to facilitate ground clearance and preparation for foot impact20, 21). Consequently, restricted performance in the ankle dorsiflexion test would suggest potential movement impairment, which could alter the mechanics of movement in multi-directional running tasks.
Kurihara et al.22) reported that maximum isometric toe flexor muscle strength was significantly correlated with the cross-sectional area of the plantar intrinsic and extrinsic muscles. In the present study, first toe flexor muscle strength was significantly corrected with DF ROM. Thus, to increase first toe flexor muscle strength, it is apparent that increases in the DF ROM are required. The specific effects of exercise training on DF ROM are unknown and further studies should now examine the effect of first toe muscle strength.
Fowles et al.23) reported that reduced force generation capacity was an important factor underlying the muscle tendon unit length-tension relationship and/or the plastic deformation of connective tissues. Low ankle DF ROM may thus change the length-tension curve of the dorsiflexor muscles and interfere with the development of dorsiflexor strength in daily life activities.
In the current study, we found no significant correlation between PFS of the ankle and DF ROM. Low ankle DF ROM may not therefore interfere with the development of PFS during regular activities.
While the results from the current study are important in the area of ankle DF ROM, literature suggests that our study is not without limitations. The main limitation of the present study was that the participants were healthy and free of major foot and ankle problems; consequently, the present data should be extrapolated to different participant populations with caution. Future studies will require a larger and more evenly age-distributed population.
In conclusion, ankle DF ROM could play an important role in determining ankle dorsiflexor strength in young adults. The implications of this research could be beneficial for both the rehabilitation and the injury prevention field.
Acknowledgments
The authors wish to thank the participants of this study for their cooperation; also the authors thank Dr. Martín J. Fernández for research assistance.
REFERENCES
- 1.Gatt A, Chockalingam N: Clinical assessment of ankle joint dorsiflexion: a review of measurement techniques. J Am Podiatr Med Assoc, 2011, 101: 59–69. [DOI] [PubMed] [Google Scholar]
- 2.Malliaras P, Cook JL, Kent P: Reduced ankle dorsiflexion range may increase the risk of patellar tendon injury among volleyball players. J Sci Med Sport, 2006, 9: 304–309. [DOI] [PubMed] [Google Scholar]
- 3.Calatayud J, Martin F, Gargallo P, et al. : The validity and reliability of a new instrumented device for measuring ankle dorsiflexion range of motion. Int J Sports Phys Ther, 2015, 10: 197–202. [PMC free article] [PubMed] [Google Scholar]
- 4.Dill KE, Begalle RL, Frank BS, et al. : Altered knee and ankle kinematics during squatting in those with limited weight-bearing-lunge ankle-dorsiflexion range of motion. J Athl Train, 2014, 49: 723–732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Backman LJ, Danielson P: Low range of ankle dorsiflexion predisposes for patellar tendinopathy in junior elite basketball players: a 1-year prospective study. Am J Sports Med, 2011, 39: 2626–2633. [DOI] [PubMed] [Google Scholar]
- 6.Basnett CR, Hanish MJ, Wheeler TJ, et al. : Ankle dorsiflexion range of motion influences dynamic balance in individuals with chronic ankle instability. Int J Sports Phys Ther, 2013, 8: 121–128. [PMC free article] [PubMed] [Google Scholar]
- 7.Headlee DL, Leonard JL, Hart JM, et al. : Fatigue of the plantar intrinsic foot muscles increases navicular drop. J Electromyogr Kinesiol, 2008, 18: 420–425. [DOI] [PubMed] [Google Scholar]
- 8.Fiolkowski P, Brunt D, Bishop M, et al. : Intrinsic pedal musculature support of the medial longitudinal arch: an electromyography study. J Foot Ankle Surg, 2003, 42: 327–333. [DOI] [PubMed] [Google Scholar]
- 9.Kibler WB, Goldberg C, Chandler TJ: Functional biomechanical deficits in running athletes with plantar fasciitis. Am J Sports Med, 1991, 19: 66–71. [DOI] [PubMed] [Google Scholar]
- 10.Mickle KJ, Caputi P, Potter JM, et al. : Efficacy of a progressive resistance exercise program to increase toe flexor strength in older people. Clin Biomech (Bristol, Avon), 2016, 40: 14–19. [DOI] [PubMed] [Google Scholar]
- 11.Endo M, Ashton-Miller JA, Alexander NB: Effects of age and gender on toe flexor muscle strength. J Gerontol A Biol Sci Med Sci, 2002, 57: M392–M397. [DOI] [PubMed] [Google Scholar]
- 12.Hughes J, Clark P, Klenerman L: The importance of the toes in walking. J Bone Joint Surg Br, 1990, 72: 245–251. [DOI] [PubMed] [Google Scholar]
- 13.Mann RA, Hagy JL: The function of the toes in walking, jogging and running. Clin Orthop Relat Res, 1979, (142): 24–29. [PubMed] [Google Scholar]
- 14.Hamel AJ, Donahue SW, Sharkey NA: Contributions of active and passive toe flexion to forefoot loading. Clin Orthop Relat Res, 2001, (393): 326–334. [DOI] [PubMed] [Google Scholar]
- 15.Menz HB, Zammit GV, Munteanu SE, et al. : Plantarflexion strength of the toes: age and gender differences and evaluation of a clinical screening test. Foot Ankle Int, 2006, 27: 1103–1108. [DOI] [PubMed] [Google Scholar]
- 16.Yun SJ, Kim MH, Weon JH, et al. : Correlation between toe flexor strength and ankle dorsiflexion ROM during the countermovement jump. J Phys Ther Sci, 2016, 28: 2241–2244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Romero Morales C, Calvo Lobo C, Rodríguez Sanz D, et al. : The concurrent validity and reliability of the Leg Motion system for measuring ankle dorsiflexion range of motion in older adults. PeerJ, 2017, 5: e2820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Statistical Concepts RG: A second course for education and behavioral sciences, 2nd ed. ed1998. [Google Scholar]
- 19.van der Harst JJ, Gokeler A, Hof AL: Leg kinematics and kinetics in landing from a single-leg hop for distance. A comparison between dominant and non-dominant leg. Clin Biomech (Bristol, Avon), 2007, 22: 674–680. [DOI] [PubMed] [Google Scholar]
- 20.Jönhagen S, Ericson MO, Németh G, et al. : Amplitude and timing of electromyographic activity during sprinting. Scand J Med Sci Sports, 1996, 6: 15–21. [DOI] [PubMed] [Google Scholar]
- 21.Lockie RG, Schultz AB, Callaghan SJ, et al. : The relationship between dynamic stability and multidirectional speed. J Strength Cond Res, 2016, 30: 3033–3043. [DOI] [PubMed] [Google Scholar]
- 22.Kurihara T, Yamauchi J, Otsuka M, et al. : Maximum toe flexor muscle strength and quantitative analysis of human plantar intrinsic and extrinsic muscles by a magnetic resonance imaging technique. J Foot Ankle Res, 2014, 7: 26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Fowles JR, Sale DG, MacDougall JD: Reduced strength after passive stretch of the human plantarflexors. J Appl Physiol 1985, 2000, 89: 1179–1188. [DOI] [PubMed] [Google Scholar]