

Abstract
This study used four waves of data from a longitudinal study of 749 Mexican origin youths to test a developmental cascades model linking contextual adversity in the family and peer domains in late childhood to a sequence of unfolding processes hypothesized to predict problem substance use and risky sexual activity (greater number of sex partners) in late adolescence. Externalizing and internalizing problems were tested as divergent pathways, with youth reported and mother-reported symptoms examined in separate models. Youth gender, nativity, and cultural orientation were tested as moderators. Family risk, peer social rejection, and their interaction were prospectively related to externalizing symptoms and deviant peer involvement, although family risk showed stronger effects on parent-reported externalizing and peer social rejection showed stronger effects on youth-reported externalizing. Externalizing symptoms and deviant peers were related, in turn, to risk-taking in late adolescence, including problem alcohol-substance use and number of sexual partners. Peer social rejection predicted youth-reported internalizing symptoms and internalizing was related, in turn, to problem alcohol and substance use in late adolescence. Tests of moderation showed some of these developmental cascades were stronger for adolescents who were female, less oriented to mainstream cultural values, and more oriented to Mexican American cultural values.
Keywords: externalizing, internalizing, risk-taking, Mexican-American, adolescents
Latino youths in the United States experience heightened vulnerability for multiple types of risk-taking behaviors in adolescence. National high school surveys indicate Latino adolescents had the highest rate of past month alcohol use in 8th, 10th, and 12th grade relative to Caucasians and African-American adolescents (e.g., r = .31; Johnston, O’Malley, Bachman, & Schulenberg, 2012). They also reported the second highest rates of binge drinking (22.6%), the highest rates of consuming 10 or more consecutive drinks (7.1%), and the highest rates of having 4 or more sexual partners compared to all other groups; (Centers for Disease Control and Prevention, 2016). Research has shown that multiple sex partners and alcohol and drug use are the primary causes of HIV/AIDS infection among minority youth and, when these behaviors occur together, risk grows tremendously (Santelli, Lindberg, Abma, McNeely, & Resnick, 2000). Understanding whether and how these behaviors are linked for Latino adolescents is critical to prioritize public health and prevention programming, especially for Mexican American who experience higher rates on these outcomes compared to other Latino subgroups (Child Trends, 2015).
Problem behavior theory, the dominant developmental model for understanding adolescent risk-taking, attributes these behaviors to a common set of risk processes that are set into motion before adolescence (Jessor & Jessor, 1977). These processes involve an interplay between family and peer influences in childhood that lead over time to dysregulated youth behavior, lack of bonding to conventional norms and peers, and a predisposition toward deviance that accounts, in turn, for the co-occurrence of risky behaviors in mid to late adolescence (e.g., (Hawkins, Catalano, & Miller, 1992; Jessor et al., 2003). Although numerous longitudinal studies support cascade models of childhood externalizing and later adolescent risk-taking (Zucker, Donovan, Masten, Mattson, & Moss, 2009), cascading pathways that extend from childhood to late adolescence have rarely been tested with Latinos. This gap is noteworthy because many of the most widely disseminated prevention programs specifically target these linked processes (National Research Council and Institute of Medicine, 2009).
Several studies have supported associations among multiple problem outcomes such as conduct problems, illicit drug use, and risky sexual behavior for Latino youth (Lopez et al., 2008; Prado et al., 2010; Schwartz et al., 2009). However, epidemiologic patterns raise the possibility that these outcomes may not coincide and unfold in similar ways for Latinos. For example, Latino adolescents ages 13 to 19 have substantially higher prevalence of health consequences linked to risky sexual behavior compared to the general population (i.e., birth rates and STIs twice as high, HIV four times greater (Centers for Disease Control and Prevention, 2011, 2012); they do not, however, experience similar disparities in child externalizing problems that are antecedent in models of unfolding risk (Watt & Martinez-Ramos, 2009). Hence, peer-related risk taking may not be explained predominantly by externalizing psychopathology for Latinos. Rather, contextual influences such as greater exposure to deviant peers or limited opportunities in lower income communities (Tolan, Guerra, & Montaini-Klovdahl, 1997) may account for Latino risk-taking independent of externalizing psychopathology. As well, Mexican American adolescents report more symptoms of depression and anxiety than other ethnic groups (Glover, Pumariega, Holzer, Wise, & Rodriguez, 1999; Roberts & Chen, 1995; Roberts, Roberts, & Chen, 1997; Siegel, Aneshensel, Taub, Cantwell, & Driscoll, 1998), owing in part to experiences of discrimination that elevate their risk for internalizing symptoms (Unger, 2014). It is possible these antecedent pathways should also be prioritized as additional prevention targets.
To test whether externalizing and internalizing psychopathology each operate as distinct pathways to Latino youth risk-taking, this study examined a sequence of risk processes linking late childhood contextual risks to late adolescent problem substance use and number of sex partners in a diverse Mexican-origin sample. Data were first collected when the youths were in 5th grade, prior to substance use and sexual onset for most. Informed by conceptual work on developmental cascade models (Masten & Cicchetti, 2010), analyses examined the sequential pathways shown in Figure 1 linking contextual risk within the family and peer ecological domains in late childhood to compromised psychological functioning in early adolescence, specifically externalizing and internalizing problems that were each hypothesized to operate, in turn, as distinct pathways to risky substance use and risky sex in late adolescence. Grounded in ecological systems theory (Bronfenbrenner, 1979; Szapocznik & Coatsworth, 1999), we also examined interactive effects between family and peer contexts that may be important to identify youths most likely to succumb to negative cascades across adolescence (Benson & Buehler, 2012; Lansford, Criss, Pettit, Dodge, & Bates, 2003). Association with deviant peers was included for its role as the context in which risk-taking typically escalates in mid-to-late adolescence (Dodge, Dishion, & Lansford, 2006), and to examine whether deviant peers intervene in externalizing and internalizing pathways to risk-taking during this period.
Figure 1.
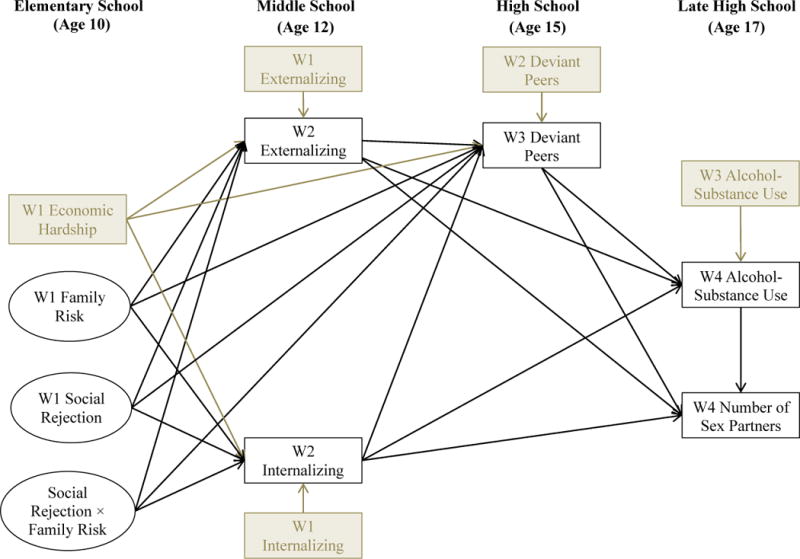
Conceptual model.
Childhood Precursors of Adolescent Psychopathology and Risk Taking
Family Contextual Adversity
Developmental cascade models specify ways in which earlier risk factors unfold through progressive or cascading effects on behaviors and experiences over time, and from one domain and point of assessment to another (Dodge et al., 2009; Haller, Handley, Chassin, & Bountress, 2010; Sitnick, Shaw, & Hyde, 2014). The most common cascades link risky family contexts (harsh, conflictual, and rejecting) to escalation of early externalizing behaviors (aggressive, impulsive, undercontrolled) that predispose and interact with rejecting peer contexts in childhood to set the stage for later involvement in peer-related risk taking. These processes have been supported in multiple studies, even when adjusting for poverty and neighborhood socioeconomic contexts (Burnette, Oshri, Lax, Richards, & Ragbeer, 2012; Patterson, Reid, & Dishion, 1992; Pettit, Bates, Dodge, & Meece, 1999).
Because harsh and hostile family contexts also increases risk for internalizing symptoms such as depression and anxiety, internalizing may offer yet another path through which family contextual adversity leads to later risk-taking (Cicchetti & Carlson, 1989; Davies & Cummings, 1998). (Repetti, Taylor, & Seeman, 2002) reviewed extensive evidence showing children from risky families experience disruptions in psychological competencies and neuroendocrine functioning, especially in response to stress, that cause them to become more physiologically reactive over time. These responses may also make youth more vulnerable to negative peers and more apt to engage in behaviors, like drinking or sex, to compensate for physiological or psychological deficiencies (Dodge, et al., 2009). For example, alcohol abuse frequently co-occurs with affective disorders and a common explanation is that adolescents with anxiety and depressive symptoms may attempt to self-medicate through frequent or heavy drinking (Hussong, Jones, Stein, Baucom, & Boeding, 2011). A few studies with non-Latinos found a positive relationship between internalizing and early sexual intercourse (Donenberg, Emerson, & Mackesy-Amiti, 2011; Monahan & Lee, 2008). Although developmental cascades have not been tested among Latinos, risky family contexts predict internalizing, externalizing and substance use for Latinos (Gonzales, Deardorff, Formoso, Barr, & Barrera, 2006; Pasch et al., 2006; Schwartz et al., 2013; Smokowski, Rose, & Bacallao, 2008). In fact, family conflict is considered a key marker of risk for Latinos because of the high cultural value placed on family harmony (Alegría et al., 2008; Prado, Szapocznik, Maldonado-Molina, Schwartz, & Pantin, 2008).
Peer Contextual Adversity
Considerable research also links various forms of peer social rejection, conflict, and victimization with symptoms of psychopathology in adolescence, including aggression, antisocial behavior, depression and anxiety (Hanish & Guerra, 2002; Kochenderfer‐Ladd & Wardrop, 2001; Lev-Wiesel, Sarid, & Sternberg, 2013; Platt, Kadosh, & Lau, 2013). Rejection and victimization experiences have greater etiological significance as children transition into adolescence because peer relationships become more important (Brown, 2004; Steinberg & Morris, 2001) and peer rejection becomes more prevalent and predictive of psychopathology (Brown, 2004; Coie, Dodge, & Kupersmidt, 1990; Juvonen, Graham, & Schuster, 2003), particularly internalizing symptoms (Larson & Ham, 1993; Masten & Cicchetti, 2010; Nolan, Flynn, & Garber, 2003; Rudolph & Hammen, 1999). Some evidence also links social rejection in childhood to adolescent risk-taking. For example, (Prinstein & La Greca, 2004) found peer rejection in grades 4 to 6 predicted externalizing, substance use, and multiple sex partners in grades 10 to 12.
For Latinos and other cultural minorities, peer social rejection and associated developmental cascades may be especially threatening when they involve hostility, exclusion, and other types of discrimination experiences tied to their ethnic group (Gibbons et al., 2007; Grigsby, Forster, Soto, Baezconde-Garbanati, & Unger, 2014; Okamoto, Ritt-Olson, Soto, Baezconde-Garbanati, & Unger, 2009). Perceived ethnic discrimination has been associated with heightened physiological arousal, anger, and especially internalizing symptoms among Latino adolescents (Greene, Way, & Pahl, 2006; Lorenzo-Blanco, Unger, Ritt-Olson, Soto, & Baezconde-Garbanati, 2011; Umaña-Taylor & Updegraff, 2007; Zeiders, Doane, & Roosa, 2012), including prospective findings showing discrimination experiences precede and predict internalizing more than the reverse (Berkel et al., 2010). Studies also report correlations between perceived discrimination and Latino adolescent substance use (Kulis, Marsiglia, & Nieri, 2009). Cano et al. (2015) examined cultural stressors including discrimination among Latino high school students and showed longitudinal prediction of both internalizing and externalizing problems (i.e., aggression, rule breaking, smoking, and alcohol use). Consistent with our hypothesized model, these authors suggest these experiences may be tied to common underlying processes that link multiple risky outcomes developmentally.
Mixed Evidence for Internalizing Pathways to Adolescent Risk-Taking
In contrast to research on externalizing and risk-taking, the role of internalizing has been studied less often and is far less conclusive, including in research with Latinos (Grigsby, et al., 2014; Kelder et al., 2001). Some studies report negative prospective associations that suggest internalizing may have a protective function to reduce risk-taking for some youth (Rogosch, Oshri, & Cicchetti, 2010; Scalco et al., 2014), similar to the hypothesized “braking effect” of internalizing on antisocial development (Burt, Obradović, Long, & Masten, 2008). Explanations center on core internalizing symptoms. For example, adolescents with internalizing problems and low propensity to risk-taking may be more inclined to avoid drinking and sexual activity due to fear of STIs, unwanted pregnancies, or being caught by parents (Blinn-Pike, Berger, Hewett, & Oleson, 2004; Capaldi, Crosby, & Stoolmiller, 1996). Internalizing also might decrease risk-taking by impeding friendship formation with deviant peers (Boivin, Vitaro, & McCord, 1995). It is possible these prohibiting influences would be stronger in subgroups, such as girls and immigrant youth, who encounter more intense pressures to avoid such behaviors.
All told, evidence for an internalizing pathway to adolescent risk-taking is not only inconsistent but also contradictory, signifying that effects are far from straightforward and may vary across samples and subgroups. Recent studies also suggest the positive effects of internalizing reported in some studies may be inflated because of the strong correlation between internalizing and externalizing that is not controlled in studies that examine them separately (King, Iacono, & McGue, 2004). (Oshri, Rogosch, Burnette, & Cicchetti, 2011) found childhood maltreatment predicted late adolescent substance use problems through externalizing but not internalizing when they were examined as simultaneous cascading paths. The relationship between internalizing and sexual behavior also has been shown to disappear (McLeod & Knight, 2010) when examined in multivariate models. Hence, we examined internalizing and externalizing simultaneously to tease out their “non-overlapping” effects, and moderating variables to test for subgroup or individual differences within our sample.
Gender and Culture as Moderators: Testing Generalizability within Group
We examined differences in hypothesized cascades based on adolescents’ gender, nativity (U.S. vs. Mexico), and two dimensions of cultural orientation (traditional and mainstream). Each of these moderators has been associated with one or more of the cascading variables in Figure 1. However, our emphasis here was not to test these as main effects but, rather, to examine whether downstream cascades from internalizing and externalizing symptoms to later risk-taking varied based on these moderators. While a test of gender differences may be especially important for understanding internalizing pathways, as summarized earlier, gender differences are also relevant to externalizing pathways. For example, there is evidence that boys are more vulnerable to deviant peer processes than girls (Moffitt & Caspi, 2001; Toro, Urberg, & Heinze, 2004), although opposite effects have also been shown (Burnette, et al., 2012). Gender differences in paths to risk-taking may be especially pronounced for Latinos due to more differentiated norms and expectations about drugs, alcohol, and sex for Latino boys and Latina girls (Deardorff, Tschann, Flores, & Ozer, 2010; Raffaelli & Ontai, 2004).
Because externalizing problems and risk-taking behaviors are typically more prevalent among U.S.-born Latinos compared to first-generation immigrants (Alegría, et al., 2008; Almeida, Johnson, Matsumoto, & Godette, 2012; Gonzales, Germán, & Fabrett, 2012) developmental cascades might also vary based on youth nativity. The “immigrant paradox” whereby immigrants have more favorable health outcomes than those born in the U.S. is most robust for risk-taking behaviors (alcohol, drug use, STDs) than for other health outcomes (Alegría, et al., 2008). Explanations often focus on the disruptive effects of acculturation on family and peer processes that may render U.S-born youth more susceptible to deviant peers (Bacio, Mays, & Lau, 2013; Frauenglass, Routh, Pantin, & Mason, 1997; Germán, Gonzales, & Dumka, 2009). However, several scholars suggest that more nuanced cultural dimensions may better account for the heterogeneity and vulnerability of Latino populations than simple measures of nativity (Schwartz, Unger, Zamboanga, & Szapocznik, 2010). A robust findings in the Latino acculturation research is that youth who become more oriented to the mainstream culture, including its language, norms and values, are at increased risk for externalizing, substance use, and sexual risk-taking (for review, see AUTHOR). Hence, mainstream cultural orientation might potentiate the likelihood for developmental cascades to occur. Research also shows a consistent protective effect for youth who retain stronger ties to their traditional culture (Blanco et al., 2013; Unger, 2014) that also may operate to inhibit developmental cascades. Strong cultural ties bolster family support, values, and youth motivation to avoid behaviors that might bring shame to the family (Stein, Gonzalez, Cupito, Kiang, & Supple, 2015). Grounded in bi-dimensional acculturation models (Berry, Trimble, & Olmedo, 1986; Schwartz, et al., 2010), we examined moderating effects of youths’ mainstream cultural values (MCV) and traditional Mexican American cultural values (MACV), in addition to youth nativity, to test these hypotheses.
Current Study and Hypotheses
Although our theoretical model was based in theory and prior research testing developmental cascades with predominantly non-Latino samples, we incorporated culturally informed measures of family and peer contextual adversity and tests of cultural moderation. Using this integrative approach (Garcia Coll et al., 1996) with a diverse Mexican-origin sample, we addressed three novel questions. First, we examined whether childhood contextual adversity predicts risk-taking in late adolescence because it leads to compromised psychological functioning that, in turn, predisposes youths to greater involvement in risk-taking (problem alcohol and drug use, multiple sexual partners). Second, we examined whether externalizing and internalizing psychopathology represent independent pathways to adolescent risk-taking, and whether deviant peers play a role in each. Third, we examined whether the cascading pathways shown in Figure 1 vary based on youth gender, immigrant status, and cultural orientation.
The study utilized four waves of data collected when the youths were in 5th (W1), 7th (W2), 10th (W3), and 12th (W4) grades. Our hypothesized model in Figure 1 examined whether contextual risk at W1 (family risk, peer social rejection, and their interaction) lead to developmental cascades across adolescence in which W2 externalizing and internalizing symptoms provide pathways linking risky family and peer contexts with more problematic substance use (alcohol and other substance use problem symptoms) and higher rates of risky sex (a greater number of past year sex partners) at W4. Family risk and peer social rejection were each latent constructs (indicators are not shown in Figure 1) and the latent variable interaction between these risk domains was included as a predictor. Gender and nativity were dichotomous variables, and mainstream and traditional values were continuous measures in tests of moderation. The following hypotheses guided the study.
We hypothesized family risk and peer social rejection in elementary school (5th grade) would combine as unique and interactive influences to predict increased externalizing and internalizing symptoms in middle school (7th grade) and greater deviant peer involvement in high school (10th grade).
We hypothesized externalizing symptoms would, in turn, predict more substance use problems and a greater number of sexual partners in late high school (12th grade), both directly and indirectly through adolescents’ increased deviant peer involvement (10th grade).
We hypothesized internalizing symptoms would in turn, predict more substance use problems in late high school (12th grade), and internalizing symptoms would be linked indirectly to a greater number of sexual partners through adolescents’ increased alcohol and substance use.
We hypothesized youth gender would moderate internalizing and externalizing paths to risk-taking. Given prior inconsistencies, we tentatively hypothesized stronger positive effects of externalizing and internalizing on deviant peers for males, and increased likelihood for negative effects of internalizing on deviant peers and alcohol-substance use for females.
We hypothesized youth nativity, Mexican American cultural values (MACV), mainstream cultural values (MCV) would moderated internalizing and externalizing paths to risk-taking. Given limited prior evidence, we tentatively hypothesized increased likelihood for negative effects of internalizing on deviant peers and risk-taking for immigrant youths and for those endorsing higher levels of MACV; and stronger developmental cascades linking externalizing, deviant peers, problem alcohol and drug use, and number of sex partners for US-born youth and for youth endorsing higher levels of MCV and lower levels of MACV.
Methods
Participants
The study utilized data from a longitudinal study of culture and context in Mexican American families (Roosa et al., 2008) The sample comprised 749 students and their families that met the following criteria: (a) the family had a fifth grader attending a sampled school; (b) both mother and child agreed to participate; (c) the mother was the child’s biological mother, lived with the child, and identified as Mexican or Mexican American; (d) the child’s biological father was of Mexican origin; (e) the child was not severely learning disabled; and (e) no step-father or mother’s boyfriend was living with the child. Using a stratified random sampling strategy, the research team identified economically, culturally, and socially diverse communities served by 47 public, religious, and charter schools throughout the metropolitan area. Youths were also sampled from different school types to provide an accurate representation of the cultural, socioeconomic, and linguistic diversity of the target populations. All of the study materials were available in English and Spanish. Recruitment materials were sent home with all 5th graders in these schools, and interested families were screened for eligibility. We completed the initial interview with 73 % of eligible families in 47 schools where the mean Latino ethnic concentration was 72.8% (range = 22.4 to 96.1; SD = 22.4); 91% of the Latinos in the state were of Mexican origin (Pew Hispanic Research Center, 2008). This sampling strategy resulted in a diverse representation of 154 neighborhoods (i.e., census tracts) where the mean level of Latino ethnic concentration was 52.9 % (range = 1.08% to 90.71%; SD = 22.8; White et al., 2014).
The resulting sample is diverse on indicators of SES and language. W1 annual family incomes ranged from less than $5,000 to more than $95,000, with a mean of $30,000 – $35,000. At W1, 30.2% of mothers, 23.2% of fathers, and 82.5% of adolescents were interviewed in English and the remainder in Spanish. The mean age of mothers was 35.9 (SD = 5.81) and mothers reported an average of 10.3 (SD = 3.67) years of education. The mean age of adolescents at W1 was 10.42 (SD = 0.55) and 48.7% were female. A majority of mothers were born in Mexico (74.3%), while a majority of adolescents were born in the US (70.3 %).
From the initial sample, 710 (94.8 %) families were re-interviewed at W2, 641 (85.6 %) at W3, and 636 (84.9%) at W4. Attrition analyses compared those families that had dropped out at W4 with those that completed an interview at W4. With only one exception (child gender), results showed no baseline differences on variables in the present study nor on any other mother or child demographic. Families who dropped out of the study were more likely to have a male than a female child (χ2(1) = 8.431, p = .004).
Procedures
Complete sampling and research procedures are described in detail elsewhere (Roosa, et al., 2008), but key features are included here. At each of four waves mothers (required), fathers (optional), and children (required) participated in in-home Computer Assisted Personal Interviews. Interviews lasted approximately 2.5 hours. Interviewers read each survey question and possible responses aloud in participants’ preferred language to reduce problems related to variations in literacy levels. Families were compensated $45, $50, $55, and $60 per participating family member at wave 1, 2, 3, and 4, respectively.
Measures
Reports from the youths and their mothers were used. Specifically, the youth and mother each reported on the youths’ internalizing and externalizing symptoms and these scores were then tested in separate models. Family economic hardship and child nativity were reported by mothers. Youths were selected as the most reliable reporters of peer social rejection, sexual behavior, and substance use, and were also used to assess family risk to achieve a parallel operational perspective on risk within the family and peer contexts.
Economic hardship (W1)
Economic hardship was assessed by mothers report using items from the four economic hardship subscales developed by Barrera, Caples, and Tein (2001) that were based on subscales originally used by Conger and colleagues and validated for Mexican Americans (Conger et al., 1991): Inability to Make Ends Meet (2 items), Not Enough Money for Necessities (7 items), Financial Strain (2 items), and Economic Adjustments/Cutbacks (9 items). Scores were based on item averages from the first three subscales that used a 5-point rating scale (5 = greater hardship), and a count of items on the Economic Adjustment subscale. These scores were standardized and averaged, with higher scores representing greater hardship.
Family risk (W1)
Family risk was a latent variable with three indicators: scores on maternal harsh parenting, parent-adolescent conflict, and family conflict that were each validated for use with Mexican Americans. We utilized an adapted version of the harsh parenting subscale of the Children’s Report of Parent Behavior Inventory (CRPBI; Schaefer, 1965), which has demonstrated cross language equivalence (Nair, White, Knight, & Roosa, 2009).
Youths reported on their perceptions of their mothers’ harsh parenting on 8 items (e.g., “Your mother screamed at you when you did something wrong”). Chronbach’s alpha (α) was .82. Youths rated conflict with their mothers using the Parent–Adolescent Conflict Scale (Ruiz, Gonzales, & Formoso, 1998) that has shown good psychometric properties in multiple studies with Mexican Americans (Corona et al., 2012; Jensen et al., 2014; Telzer, Gonzales, & Fuligni, 2014; Vargas, Roosa, Knight, & O’Donnell, 2013). Adolescents responded to 10 items reporting how often they had experienced minor and serious disagreement (e.g., “How often did you and your mother disagree with each other?”). Chronbach’s alpha was .72. The 9-item family conflict subscale of the Multicultural Events Scale for Adolescents (Gonzales, Tein, Sandler, & Friedman, 2001a) was employed to assess discord or hostility at the family level, including culture-related conflicts among family members. Children rated items like “Your parents had a serious disagreement or fight with each other” and “Family members disagreed about cultural traditions” as “happened” or “did not happen”. A count of the “happened” events was computed.
Peer social rejection (W1)
Peer social rejection was a latent variable with three indicators: scores on perceived peer hassles and conflict, ethnic discrimination, and relational aggression. Self-report (versus parent- or peer-report) is the most common method for assessing experiences of victimization, especially those that are very personal in nature such as relational aggression and discrimination experiences that may only be known by the aggressor and the victim (Siegel, La Greca, & Harrison, 2009). Although self-perceptions are subject to over-reporting (“paranoia”) and under-reporting (“denial”) biases, validity has been established through significant overlap with peer perceptions (e.g., r = .31; Graham & Juvonen, 1998), and by similar relations with child outcomes when compared to peer nominations (Crick & Bigbee, 1998).
The peer hassles/conflict subscale from the MESA (Gonzales, et al., 2001a; Gonzales, Tein, Sandler, & Friedman, 2001b) includes 14 items tapping conflict, victimization, and social rejection experiences with same age peers. Youths responded “happened” or “did not happen” to items (e.g., “kids tried to fight with you.”). A count of “happened” events was computed. A 5-item scale assessed ethnic discrimination experiences from peers (e.g., “kids called you names because you are Mexican or Mexican American”). The measure demonstrated good psychometric properties in samples of Mexican origin youths (Berkel, et al., 2010; Delgado, Updegraff, Roosa, & Umaña-Taylor, 2011). Adolescents indicated how true or how often events happened (e.g., kids called you names because you are Mexican or Mexican American). Chronbach’s alpha at W1 was .78. A mean score was computed. The 5-item Relational Aggression Scale was adapted from (Prinstein, Boergers, & Vernberg, 2001) version of the Revised Peer Experiences Questionnaire (Vernberg, Jacobs, & Hershberger, 1999). Youths indicated how often each behavior had been directed toward him/her. Example items include “A kid your age that you liked would not sit near you at lunch or in class”. Chronbach’s alpha at W1 was .82. A mean score was computed.
Internalizing and externalizing symptoms (W1 & W2)
Mothers and youth separately completed the Diagnostic Interview Schedule for Children (C-DISC-IV;(Shaffer, Fisher, Lucas, Dulcan, & Schwab-Stone, 2000), a structured diagnostic instrument based on the Diagnostic and Statistical Manual of Mental Disorders 4th ed. (American Psychiatric Association, 1994). Internalizing symptoms was a sum of generalized anxiety, major depression, and social phobia symptoms. Externalizing symptoms was a sum of conduct disorder and oppositional defiant disorder symptoms. Interrater reliability was low (r = .23 for externalizing, r = .17 for internalizing), which is expected for child symptom ratings because each reporter has access to different aspects of the child’s functioning and in different settings (De Los Reyes, 2013).
We did not use diagnostic categories in the current study; however, we compared our rates of diagnoses at W1/W2 with rates from the National Health and Nutritional Examination Survey (NHANES; (Merikangas et al., 2010) that reported 12 month prevalence separately for ages 6 to 11 and ages 12 to 15; our sample spanned these two age ranges. To be consistent with their reporting framework, we used youth report for generalized anxiety disorder (GAD) and the combined (either parent “OR” youth) report for Major Depressive Disorder (MDD), Conduct Disorder (CD), and Oppositional Defiant Disorder. Our rates compared to the younger and older national samples, respectively, were 1.2% vs. .1% and .7% for GAD; 3.2% vs. 1.6% and 3.8% for MDD; 4.8% vs. .8% and 1.1% for DD; 2.4% vs. 1.5% and 2.7% for CD. Compared to data available on Hispanics in other national samples, our rates of past year diagnosis were 3.2% vs. 2.4% for MDD, and 7.5% vs. 2.5% for Social Phobia; rates of lifetime diagnoses were 3.6% vs. 3.9% for MDD; 3.4% vs. 3.2% for CD (CDC, 2013).
Deviant peer association (W2 & W3)
Youths responded to the 14-item Peer Delinquent Behavior scale ((Dishion, Patterson, Stoolmiller, & Skinner, 1991; Thornberry, Lizotte, Krohn, Farnworth, & Jang, 1994). They answered statements like “How many of your friends have used alcohol or drugs, or sniffed things to get high or drunk?” and “How many of your friends have purposely damaged, destroyed, or tagged property that did not belong to them?” Alphas were .89 and .92 at W2 and W3, respectively.
Problem alcohol and substance use (W3 & W4)
The youths reported on their past year experiences with alcohol, tobacco, marijuana, and other illicit drugs on the Diagnostic Interview Schedule for Children (C-DISC; (Shaffer, et al., 2000). The combined alcohol and other substance use disorder symptom count score was used. Although diagnoses were not used, our rate of past year Alcohol Use Disorder was 3.9% vs. 4.5% reported for Hispanics in the National Survey on Drug Use; Drug Abuse Disorder was 3.9% vs. 5.7%, respectively ((3.9% vs. 5.7%; CDC, 2013). Our rates of ever use compared to a national Latino high school sample (Kann et al., 2014), were 62.8% vs. 71.2% for alcohol, and 27.7% vs. 48.8% for marijuana.
Number of sexual partners (W4)
Using a computer-assisted method that allowed anonymous responses on the keyboard, youths reported the number of sexual partners they had in the past 12 months, an established measure of risky sex (Prinstein & La Greca, 2004). Our rate of ever having sex was 37.8% vs. 46.6% for a national Latino sample (Kann, et al., 2014).
Gender and nativity (W1)
Mothers reported on adolescent gender (0 = male; 1 = female) and nativity (0 = U.S.-born; 1 = Mexico-born).
Youth cultural orientation (W2)
Adolescents completed the Mexican American Cultural Values Scale (MACVS: Knight et al., 2010) to assess Mexican American values (MACV) and mainstream values (MVS). The MACVS was developed through focus groups with Mexican American mothers, fathers, and adolescents. Two broad factors were validated using CFAs across 3 datasets with Mexican American adolescents and adults. Adolescent indicated their endorsement of each item by responding with a five-point Likert-type scale ranging from (1) not at all to (5) very much. MACV was the mean score across 36 items from the 6 Mexican American value subscales: familism-support, familism-obligation, familism-referents, respect, religiosity, and traditional gender roles. MCV was the mean score across 14 items from the 3 mainstream value subscales: material success, independence/self-reliance, and competition/personal achievement. Cronbach’s α were .89 and .83 for MACV and MCV, respectively.
Analytic Strategy
Figure 1 illustrates our analytical model. W1 economic hardship was included as a covariate when estimating paths from W1 contextual risk (latent constructs of family risk, peer social rejection, and their interaction) to W2 internalizing, W2 externalizing, and W3 deviant peers. When estimating effects of earlier to subsequent domains in the sequential cascade model (contextual risk to mental health symptoms, mental health symptoms to risk-taking), the level of the corresponding construct from the previous measurement wave was included as a covariate, except for the sexual risk outcome because we focused on the number of sexual partners only in the past 12 months. The covariances or residual covariances among constructs within the same assessment period (e.g., W1 internalizing symptoms and W1 externalizing symptoms; W2 internalizing symptoms and W2 externalizing symptoms) were included in the model. W1 peer and family subscales based on the same measure were correlated to control for method effect.
Structural equation modeling (SEM) was used to estimate the hypothesized model, using Mplus 7 (Muthén & Muthén, 1998–2012). Maximum likelihood estimation was used to handle the missing data in the model (Enders, 2010), thus the full sample was included in model testing. We utilized the sandwich estimator in all analyses to adjust the standard errors of path coefficients for nonnormality (Muthén & Muthén, 1998–2012). The latent variable interaction term between W1 family risk and W1 social rejection was created using the XWITH option in Mplus (for testing interaction effects). If the interaction was found to be significant, we would probe simple slopes of W1 social rejection on W2 internalizing, W2 externalizing, or W3 deviant peers at +1 SD/−1 SD of the factor mean of W1 family risk and simple slopes of W1 family risk at +1 SD/−1 SD of the factor mean of W1 social rejection. To obtain interpretable simple intercepts, relevant predictors/covariates were mean-centered1.
We used Poisson regression to model the two outcomes, W4 alcohol-substance use symptom counts and W4 number of sex partners in the previous year, which were count variables and had highly non-normal distributions (Skewness = 6.897, Kurtosis = 59.203 and Skewness = 5.075, Kurtosis = 36.445, respectively)2. Since both outcomes displayed many zero counts3, we compared the zero-inflated Poisson model with the standard Poisson model (using AIC and BIC) to decide which model to use. The zero-inflated Poisson model makes the assumption that the zero counts observed in the data come from two groups (Coxe, West, & Aiken, 2009), those who produce structural zeroes (e.g., non-problem users of alcohol and other substances, who would never get a non-zero count on alcohol-substance use symptoms), and those who produce counts of zero with some probability (e.g., users and occasional users of alcohol and other substances, who happened to have zero alcohol-substance use symptoms in the year before our W4 data collection). With a zero-inflated Poisson model, two regressions are estimated: the first one is a logistic regression that predicts the odds of being in the group with structural zeroes, and the second one is a regular Poisson regression for the count part of the outcome that does not contain structural zeroes (Coxe, et al., 2009; Muthén & Muthén, 1998–2012). When estimating a zero-inflated Poisson model, we used the same set of predictors for these two parts. Note that when being used to predict W4 number of sex partners, the W4 alcohol-substance use symptom count variable was treated as a whole – as a continuous predictor. We reported unstandardized path coefficients because standardized coefficients are not available for Poisson models. The model in Figure 1 was tested in the following order. First, we fit a measurement model for W1 family risk and W1 social rejection, and examined the equivalence of the latent factor structures across youth nativity and gender. Second, we fit the overall model as hypothesized and determined the form of Poisson regression (zero-inflated Poisson vs. standard Poisson) for the two count outcomes, using youth-reported internalizing and externalizing symptoms in the model. Third, we fit the overall model using the form of Poisson regression for the two count outcomes determined in the previous step,4 this time using parent-reported internalizing and externalizing symptoms. Fourth, we used multiple group SEM to examine separately the moderation effects of youth nativity and gender on the hypothesized cascade paths. If the multivariate Wald test showed that the cascade paths differed across groups, we used the Wald test to investigate which paths differed. Then to probe the moderation effect by youth gender or by nativity, we re-ran the multiple group SEM constraining the W1 factor loadings and the invariant cascade paths to be the same across groups, but freely estimating the cascade paths that were different across groups as the final model. Fifth, we examined separately the moderation effects of youth-reported Mexican American cultural values and those of youth-reported mainstream values, on the relations between youth-reported or parent-reported internalizing and externalizing symptoms and downstream outcome variables. The complete standardized coefficients are not available for the models with interactions and cannot be calculated for count outcomes. To gauge the magnitudes of the coefficients, we hand calculated the standardized coefficients using different methods for dependent variables that were continuous variables (e.g., standardized based on both the variances of the predictor and the outcome, i.e., complete standardization) and for dependent variables that were count outcomes (e.g., standardized based on only the variance of the predictor). Since the standardized path coefficients for the continuous outcomes and for the count outcomes were on different metrics, to avoid confusion, we reported only the unstandardized path coefficients (with standard errors) in the text and in Figures 2 and 3. The results with standardized coefficients can be viewed at http://reachinstitute.asu.edu/MexicanAmericanRiskTaking.
Figure 2.
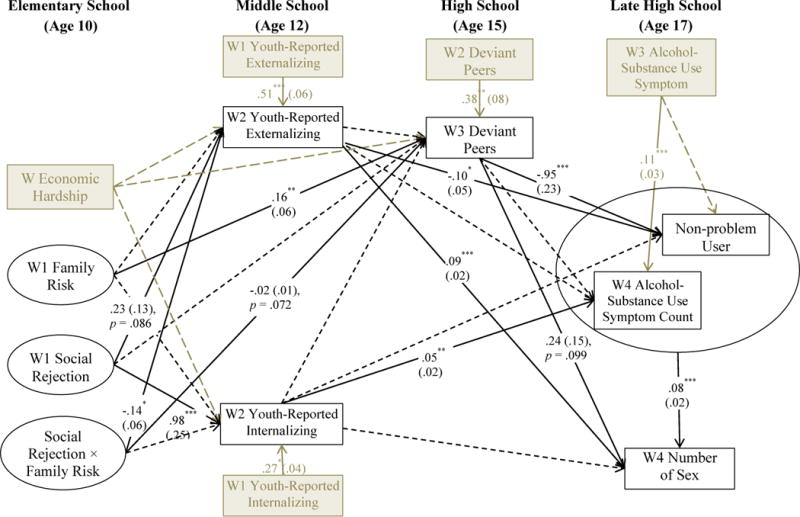
Model based on youth-reported internalizing and externalizing symptoms. Note: Unstandardized path coefficients are reported. Significant or trending paths are solid lines; non-significant paths are dashed. * p < .05. ** p < .01. *** p < .001.
Figure 3.
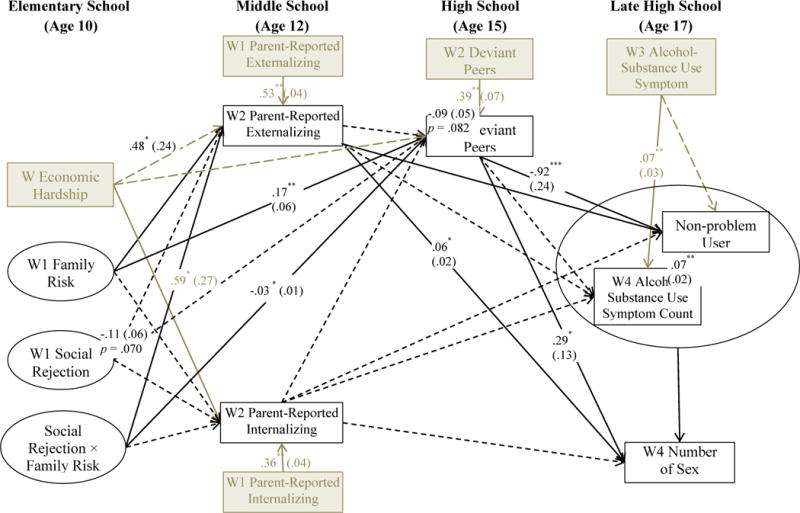
Model based on parent-reported internalizing and externalizing symptoms. Note: Unstandardized path coefficients are reported. Significant or trending paths are solid lines; non-significant paths are dashed. * p < .05. ** p < .01. *** p < .001.
Results
Table 1 provides the means, standard deviations, and correlations of study variables. Most of the correlations involving the contextual risk, internalizing, externalizing, and risk-taking variables were in expected directions.
Table 1.
Sample Correlation Matrix, Means, and Standard Deviations for Study Variables.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | Youth nativity | – | .12** | .24*** | −.16*** | −.20*** | −.10* | .01 | .18*** | −.01 | −.07 | −.05 | .00 | −.03 | .08 | .07 | −.04 | −.10* | −.02 | −.04 | .15** |
| 2. | Youth gender | .12** | – | .00 | .03 | .01 | −.07 | −.05 | .05 | −.03 | .09 | .05 | .00 | −.05 | .10* | .13** | .04 | .00 | .02 | .14** | .20*** |
| 3. | W1 ECON HARD | .24*** | .00 | – | .04 | .01 | .10* | .02 | .16*** | .13** | .00 | .03 | .25*** | .12** | .06 | .13** | .09* | .07 | .08 | .05 | .12** |
| 4. | W1 M HARSH | −.16*** | .03 | .04 | – | .55*** | .33*** | .32*** | .21*** | .32*** | .13** | .09* | .12** | .02 | .11* | .11* | .11* | .11* | .13** | .09* | .05 |
| 5. | W1 CM CONF | −.20*** | .01 | .01 | .55*** | – | .45*** | .34*** | .26*** | .43*** | .18*** | .15** | .07 | .02 | −.07 | .07 | .19*** | .14** | .09 | .05 | .02 |
| 6. | W1 family conflict | −.10* | −.07 | .10* | .33*** | .45*** | – | .50*** | .24*** | .37*** | .11* | .13** | .07 | .04 | −.11* | −.01 | .25*** | .18*** | .04 | .03 | .10* |
| 7. | W1 PHASS/CONF | .01 | −.05 | .02 | .32*** | .34*** | .50*** | – | .48*** | .55*** | .14** | .13** | .06 | .09* | −.01 | .04 | .32*** | .17*** | .04 | .07 | .11* |
| 8. | W1 discrimination | .18*** | .05 | .16*** | .21*** | .26*** | .24*** | .48*** | – | .54*** | .03 | .08 | .05 | .03 | .08 | .12** | .18*** | .06 | .07 | .14** | .08 |
| 9. | W1 REL AGG | −.01 | −.03 | .13** | .32*** | .43*** | .37*** | .55*** | .54*** | – | .12* | .08 | .10* | .07 | .01 | .11* | .19*** | .07 | −.02 | .00 | .03 |
| 10. | W1 externalizing | .01 | .09 | −.01 | .24*** | .26*** | .36*** | .35*** | .20*** | .22*** | (.15**) | .59*** | .32*** | .18*** | .02 | −.05 | .17*** | .15** | .21*** | .25*** | .13** |
| 11. | W2 externalizing | .00 | .01 | .00 | .09 | .13** | .23*** | .31*** | .10* | .10* | .40*** | (.22***) | .24*** | .30*** | −.05 | −.06 | .21*** | .18*** | .20*** | .24*** | .15** |
| 12. | W1 internalizing | −.02 | −.02 | .05 | .19*** | .27*** | .35*** | .45*** | .34*** | .39*** | .39*** | .22*** | (.10*) | .46*** | .04 | .01 | .03 | .09* | .07 | .10* | .05 |
| 13. | W2 internalizing | −.04 | −.04 | .04 | .11* | .15** | .26*** | .36*** | .22*** | .28*** | .19*** | .43*** | .42*** | (.18***) | −.03 | .00 | .05 | .17*** | .08 | .10* | .08 |
| 14. | W2 MACV | .08 | .10* | .06 | .11* | −.07 | −.11* | −.01 | .08 | .01 | −.07 | −.15* | −.02 | −.04 | – | .39*** | −.04 | −.06 | −.01 | −.02 | .06 |
| 15. | W2 MCV | .07 | .13** | .13** | .11* | .07 | −.01 | .04 | .12** | .11* | .02 | −.03 | .00 | .02 | .39*** | – | .00 | −.03 | .04 | .00 | .06 |
| 16. | W2 deviant peers | −.04 | .04 | .09* | .11* | .19*** | .25*** | .32*** | .18*** | .19*** | .21*** | .46*** | .17*** | .29*** | −.04 | .00 | – | .37*** | .13** | .11* | .10* |
| 17. | W3 deviant peers | −.10* | .00 | .07 | .11* | .14** | .18*** | .17*** | .06 | .07 | .18*** | .22*** | .14** | .13** | −.06 | −.03 | .37*** | – | .31*** | .27*** | .14** |
| 18. | W3 ALC-SUB use | −.02 | .02 | .08 | .13** | .09 | .04 | .04 | .07 | −.02 | .16*** | .11* | .01 | −.01 | −.01 | .04 | .13** | .31*** | – | .46*** | .07 |
| 19. | W4 ALC-SUB use | −.04 | .14** | .05 | .09* | .05 | .03 | .07 | .14** | .00 | .20*** | .14** | .06 | .07 | −.02 | .00 | .11* | .27*** | .46*** | – | .19*** |
| 20. | W4 N Sex Partner | .15** | .20*** | .12** | .05 | .02 | .10* | .11* | .08 | .03 | .19*** | .18*** | .02 | .00 | .06 | .06 | .10* | .14** | .07 | .19*** | – |
| N | 749 | 749 | 745 | 749 | 749 | 749 | 749 | 747 | 749 | 733 (720) | 708 (705) | 734 (725) | 708 (706) | 705 | 706 | 710 | 613 | 605 | 567 | 591 | |
| Sample mean | .30 | .51 | .00 | 2.05 | 2.00 | 1.17 | 3.12 | 1.86 | 1.84 | 1.64 (1.96) | 2.71 (2.14) | 11.91 (6.55) | 10.32 (5.15) | 4.16 | 2.75 | 1.34 | 1.65 | .36 | .37 | .94 | |
| Standard deviation | – | – | .81 | .75 | .56 | 1.50 | 2.85 | .86 | .90 | 2.28 (2.87) | 3.23 (2.85) | 8.09 (6.55) | 7.44 (6.06) | .39 | .63 | .44 | .59 | 1.65 | 1.64 | 1.91 | |
Note.
p < .05.
p < .01.
p < .001.
For the sample correlations, sample size = 477 due to list-wise deletion. For the sample mean and sample standard deviation, the sample size for each study variable was included in the table. In the correlation matrix, the lower and upper triangles reflect the sample correlations among variables in the models based on youth-reported versus parent-reported internalizing and externalizing symptoms, respectively. Intercorrelations of youth- and parent-reported internalizing and externalizing symptoms are reported in the parentheses along the diagonal of the correlation matrix. For the sample size, sample mean, and sample deviation of the internalizing and externalizing symptoms, those of the youth report were reported first, followed by those of the parent report in parentheses. Youth nativity was coded 0 = US-born, 1 = Mexico-born; youth gender was coded 0 = female, 1 = male. ECON HARD = economic hardship; M HARSH = mother harsh parenting; CM CONF = child conflict with mother; PHASS/CONF = peer hassles/conflict; REL AGG = relational aggression; MACV = Mexican American cultural values; MCV = mainstream values; ALC-SUB = alcohol-substance; N Sex Partner = number of sex partners.
Measurement Model
Prior to fitting the full SEM model, we fit a measurement model for W1 family risk and W1 peer social rejection. The measurement model suggested good fit of the data [χ2 (7) = 21.97, p < .05; CFI = .98; RMSEA = .05; SRMR = .03]; the resulting standardized factor loadings were all significant, ranging from .53 to .80 for W1 family risk and .66 to .81 for W1 peer social rejection. The two constructs were correlated at .59. Equivalence of the measurement model across youth nativity and gender was tested using multiple group analyses. Two nested models were conducted with one freely estimating all parameters in each comparison group, and the other constraining all factor loadings to be equal across groups. Nested model tests for the W1 measurement model showed the factor loadings were not significantly different across youth nativity, Δχ2 (4) = 2.16, p = .71, and across youth gender, Δχ2 (4) = .68, p = .95.
Cascading Model Based on Youth-Reported Internalizing and Externalizing Symptoms
We fit a zero-inflated Poisson model and a standard Poisson model to W4 alcohol-substance use symptom counts, and the zero-inflated Poisson model produced better fit to the data (AIC = 36680.548 and BIC = 37091.616 for the zero-inflated Poisson model vs. AIC = 37089.762 and BIC = 37477.736 for the standard Poisson model). Fitting a zero-inflated Poisson model to W4 number of sex partners led to non-convergence in many of the follow-up models testing for moderation effects, thus a regular Poisson model was used to model W4 number of sex partners. Therefore, we continued with a zero-inflated Poisson model for W4 alcohol-substance use symptoms and a standard Poisson model for W4 number of sex partners.
Figure 2 shows the results of our SEM model based on youth-reported internalizing and externalizing symptoms. W1 social rejection was positively associated with W2 youth-reported internalizing symptoms. The main effect of W1 social rejection on W2 youth-reported externalizing was marginally significant. Also, the moderation effect of W1 family risk × W1 social rejection on W2 youth-reported externalizing was significant. The relationship between W1 social rejection and W2 youth-reported externalizing symptoms tended to be positive, and the positive relation was stronger at lower levels of W1 family risk. However, W1 family risk was not significantly associated with W2 youth-reported externalizing at low (1 SD below the mean), mean, or high (1 SD above the mean) levels of W1 social rejection.
The main effect of W1 family risk on W3 deviant peers was significant. Also, the moderation effect of W1 family risk × W1 social rejection on W3 deviant peers was marginally significant. The relationship between W1 family risk and W3 deviant peers tended to be positive, and the positive relation was stronger at lower levels of W1 social rejection. However, the relationship between W1 social rejection and W3 deviant peers was not statistically significant at low (1 SD below the mean), mean, or high (1 SD above the mean) levels of W1 family risk.
For the zero-inflated Poisson model of W4 alcohol and substance use problems, higher W2 youth-reported externalizing symptoms was associated with lower odds of being a non-problem user [B = −.10 (.05), p < .05; odds ratio (OR) = .90]; higher W3 deviant peers was associated with lower odds of being a non-problem user [B = −.95 (.23), p < .001; OR = .39]; and higher W2 youth-reported internalizing symptoms was associated with more W4 alcohol and substance use problems, among the problem users of alcohol and substances. The Poisson model of W4 number of sex partners revealed a positive relationship between W2 youth-reported externalizing and W4 number of sex partners, a positive relationship between W4 alcohol and substance use problems and W4 number of sex partners, and a trending positive relationship between W3 deviant peers and W4 number of sex partners.
Cascading Model Based on Parent-Reported Internalizing and Externalizing Symptoms
Figure 3 shows the results of our SEM model based on parent-reported internalizing and externalizing symptoms. The findings were mostly consistent with those based on the youth-reported internalizing and externalizing model. The main effect of W1 family risk on W2 parent-reported externalizing was significant. The moderation effect of W1 family risk × W1 social rejection on W2 parent-reported externalizing was marginally significant. W1 social rejection was not significantly associated with W2 parent-reported externalizing at low (1 SD below the mean), mean, or high (1 SD above the mean) levels of W1 family risk. The relation between W1 family risk and W2 parent-reported externalizing tended to be positive, and this positive relationship was stronger at lower levels of W1 social rejection.
The main effect of W1 family risk on W3 deviant peers was significant. Also, the moderation effect of W1 family risk × W1 social rejection on W3 deviant peers was significant. The relationship between W1 family risk and W3 deviant peers tended to be positive, and the positive relation was stronger at lower levels of W1 social rejection. Although the relationship between W1 social rejection and W3 deviant peers was not significant at the mean or low levels of W1 family risk, the relationship became negative at higher levels of W1 family risk.
For the zero-inflated Poisson model of W4 alcohol and substance use problems, higher W2 parent-reported externalizing symptoms was associated with lower odds of being a non-problem user [B = −.09 (.05), p = .082; OR = .91]; higher W3 deviant peers was associated with lower odds of being a non-problem user [B = −.92 (.24), p < .001; OR = .40]. The Poisson model of W4 number of sex partners revealed positive relationships between W2 parent-reported externalizing and W4 number of sex partners, between W3 deviant peers and W4 number of sex partners, and between W4 alcohol and substance use problems and W4 number of sex partners.
Moderation of the Cascading Paths by Youth Gender
Model based on youth-reported internalizing and externalizing
We assessed the extent to which the cascading model based on youth-reported internalizing and externalizing was equivalent across youth gender. Multivariate Wald test showed the hypothesized cascading paths were significantly different across youths’ gender [χ2 (21) = 41.01, p < .01]. As a result, we investigated which cascading path(s) in the model were different across gender, focusing on paths that were significant (or trending) in at least one gender group. Wald tests for the equality of paths across gender groups revealed one path that was different: W4 alcohol-substance use symptoms → W4 number of sex partners, Wald χ2 (1) = 6.96, p = .008. Multivariate Wald test showed that the rest of the cascading paths in Figure 2 were not significantly different across youths’ gender [χ2 (20) = 19.88, p = .47]. Retaining the invariant paths to be the same while freely estimating this path that was different across youth gender, we found the positive relation between W4 alcohol-substance use symptoms and W4 number of sex partners was stronger for females [B = .17 (.04), p < .001] than for males [B = .04 (.02), p < .05].
Model based on parent-reported internalizing and externalizing
We assessed the extent to which the cascading model based on parent-reported internalizing and externalizing was equivalent across youth gender. Multivariate Wald test showed the hypothesized cascading paths were significantly different across youths’ gender [χ2 (21) = 54.15, p < .001]. As a result, we investigated which cascading path(s) in the model were different across gender, focusing on paths that were significant (or trending) in at least one gender group. Wald tests for the equality of paths across gender groups revealed one path that was different: W2 parent-reported externalizing symptoms → W4 alcohol-substance use symptoms, Wald χ2 (1) = 16.74, p < .001. Multivariate Wald test showed that the rest of the cascading paths were still significantly different across youths’ gender [χ2 (20) =31.87, p = .045]. However, none of the other cascading paths were significantly different across youths’ gender. Retaining the invariant paths to be the same across youths’ gender while freely estimating the path from W2 parent-reported externalizing to W4 alcohol-substance use symptoms in each gender group, we found that there was a positive relation between W2 parent-reported externalizing and W4 alcohol-substance use symptoms for females [B = .19 (.03), p < .001], but not for males.
Moderation of the Cascading Paths by Youth Nativity
Model based on youth-reported internalizing and externalizing
We assessed the extent to which the cascading model based on youth-reported internalizing and externalizing was equivalent across youth nativity. Multivariate Wald test showed that the hypothesized cascading paths were not significantly different across youths’ nativity [χ2 (21) = 28.95, p =.12].
Model based on parent-reported internalizing and externalizing
We assessed the extent to which the cascading model based on parent-reported internalizing and externalizing was equivalent across youth nativity. Multivariate Wald test showed that the hypothesized cascading paths were not significantly different across youths’ nativity [χ2 (21) = 26.99, p = .17].
Moderation Effect of Youth-Reported Mexican American Cultural Values (MACV)
We examined the moderation effects of W2 youth-reported MACV on the relations between W2 youth-reported or parent-reported internalizing and externalizing and downstream variables (W3 deviant peers, W4 alcohol-substance use symptom count, W4 non-problem use of alcohol and substances, and W4 number of sex partners).
Model based on youth-reported internalizing and externalizing
The interaction between W2 MACVS and W2 youth-reported externalizing was a significant predictor of W3 deviant peers [B = .04 (.02), p < .05]. There was a significant positive relation between W2 youth-reported externalizing and W3 deviant peers at a high level (1 SD above the mean) of W2 MACV, but not at a low (1 SD below the mean) or mean level of W2 MACV. None of the other interaction effects between W2 MACV and W2 youth-reported internalizing or externalizing significantly predicted any other downstream outcome.
Model based on parent-reported internalizing and externalizing
The interaction between W2 MACV and W2 parent-reported externalizing was a significant predictor of W4 alcohol-substance use symptom counts among the problematic users [B = .18 (.09), p < .05]. There was a significant positive relation between W2 parent-reported externalizing and W4 alcohol-substance use symptoms at a high level (1 SD above the mean) of W2 MACV, a trending positive relation at the mean of W2 MACV, but no association at a low (1 SD below the mean) level of W2 MACV. None of the other interaction effects between W2 MACV and W2 parent-reported internalizing or externalizing significantly predicted any other downstream outcome.
Moderation Effect of Youth-Reported Mainstream Values (MCV)
We examined the moderation effects of W2 youth-reported MCV on the relations between W2 youth-reported or parent-reported internalizing and externalizing and downstream outcome variables (W3 deviant peers, W4 alcohol-substance use symptom count, W4 non-problem use of alcohol and substances, and W4 number of sex partners).
Model based on youth-reported internalizing and externalizing
None of the interaction effects between W2 MCV and W2 youth-reported internalizing or externalizing was significantly predicting any downstream outcome.
Model based on parent-reported internalizing and externalizing
The interaction between W2 MCV and W2 parent-reported internalizing was a significant predictor of W4 alcohol-substance use symptoms among the problematic users [B = −.10 (.03), p < .001]. The relation between W2 parent-reported internalizing and W4 alcohol-substance use symptoms (among the problematic users) was positive and significant at a low level (1 SD below the mean) of W2 MCV, but trending negative at a high level (1 SD above the mean) of W2 MCV. The interaction between W2 MCV and W2 parent-reported externalizing was a significant predictor of W4 number of sex partners [B = −.10 (.03), p < .01]. The positive relation between W2 parent-reported externalizing and W4 number of sex partners was stronger at lower levels of W2 MCV. None of the other interaction effects between W2 MCV and W2 parent-reported internalizing or externalizing was significantly predicting any other downstream outcome.
Discussion
This study of U.S. Mexican origin youths examined developmental cascades linking hostile and rejecting family and peer contexts in childhood to a sequence of unfolding problems involving externalizing and internalizing symptoms, deviant peers, and risky substance use and sexual behavior in adolescence. Findings supported several hypothesized cascades, confirming that risky family contexts and peer social rejection are significant precursors to compromised psychological functioning in early adolescence, and that externalizing and internalizing problems each play a unique role as pathways to later risk-taking in mid-to-late adolescence. The strength of several findings varied when examined with parent versus youth report of internalizing and externalizing symptoms, yet the pattern of findings replicated in most cases. Several cascades from psychopathology to later risk-taking were moderated by youth gender or cultural orientation (MACV and MCV), but not by youth nativity.
Results supported our hypothesis that risky family and peer contexts in childhood would combine to predict problem behaviors in middle school. The interaction between family risk and peer social rejection was a significant predictor of externalizing symptoms in the model based on youth report of externalizing. Peer social rejection generally had more powerful effects in the prediction of youth- versus parent-reported externalizing, perhaps because parents are less likely to directly observe problem behaviors prompted by difficulties in the peer context. However, while peer social rejection had significant effects on youth-reported externalizing at lower levels of family risk, peer social rejection was unrelated to later externalizing for youth reporting high levels of family risk. This is because youths in risky families (+ 1.S.D) generally reported more externalizing symptoms irrespective of the peer context. In contrast, family risk had more powerful and significant, unique effects on parent-report of youth externalizing, perhaps because youth in hostile and rejecting families are especially likely to display aggressive, oppositional behavior when interacting with parents (Patterson, et al., 1992). Although the family × peer interaction was marginal in the parent-report model, the influence of family risk attenuated and became non-significant at high levels (+1 S.D.) of peer social rejection.
Across both models, risky family contexts showed robust, unique effects to predict increased involvement with deviant peers as adolescents moved from middle to high school, independent of earlier externalizing psychopathology. However, in addition to these significant main effects, the family risk × peer social rejection interaction predicted deviant peer involvement in the parent-report model and marginally predicted deviant peer involvement in the youth-report model. In both models, and similar to effects on externalizing, the negative effects of family risk attenuated at higher levels of peer rejection. Altogether, these findings illustrate the importance of examining family–peer interplay in ecological models of risk. However, the pattern of this interplay was not consistent with a cumulative risk interpretation (i.e., Rutter, 1979). Instead, findings showed family and peer risk were each important, but they did not always work in tandem. Rather, vulnerability for externalizing increased when either or both were elevated.
Results did not support family-peer interplay in the prediction of internalizing symptoms. Instead, peer social rejection uniquely predicted internalizing symptoms in middle school, but only in the model with youth-reported internalizing symptoms Family risk was unrelated to internalizing in both models. These findings are consistent with prior research showing peer rejection is increasingly negative consequences on internalizing symptoms, such as depression, in adolescence (Larson & Ham, 1993; Masten & Cicchetti, 2010; Nolan, et al., 2003; Rudolph & Hammen, 1999; Schwartz et al., 2015). In the current study, perceptions of peer-related conflict and victimization, relational aggression, and ethnic discrimination combined to form a latent construct that predicted youth-reported but not parent-reported internalizing symptoms. Although this finding did not replicate across reporters, evidence has shown that parents and youth have access to different samples of behaviors relevant to youth psychological and behavioral functioning and that each perspective is valid and meaningful (De Los Reyes et al., 2015). Evidence also indicates that self-reports of symptomatology become more important as youth spend more time outside the home, and when reporting on their own internal distress (Achenbach, McConaughy, & Howell, 1987; De Los Reyes, et al., 2015; Meyer et al., 2001).
Externalizing pathways and developmental cascades to risk-taking
Study findings supported several expected linkages between externalizing and subsequent risk-taking. Externalizing was consistently supported as a key pathway to problem alcohol -substance use and to the number of sex partners across both reporters of externalizing. Youth-reported externalizing predicted increased likelihood of being a problem alcohol-and-substance user and greater number of sex partners. Parent-reported externalizing predicted a greater number of sex partners and showed marginal effects to predict decreased likelihood of being a non-problem substance user. Adolescents’ involvement with deviant peers predicted both the likelihood and extent of problem substance use, as well as the number of sex partners. And, as expected, problem substance use and number of sexual partners were positively associated, adding to existing evidence that the presence and quantity of substance use over time, and at the time of sexual activity, increases the likelihood of having sexual intercourse and having more than one sexual partner. For example, in African-American and Latino sample, Bazargan-Hejazi et al. (2012) found alcohol use before sex increases the number of sexual partners, but the magnitude of this effect is significantly increased among alcohol misusers.
Altogether, the multiple cascades found in the current study supported our central hypotheses, based in problem behavior theory, that problems such as deviant behavior, substance use, and risky sex are driven, in part, by common antecedents and developmental processes (Hawkins, et al., 1992; Jessor & Jessor, 1977). However, moderation analyses clarified that these paths were less explanatory for some youths. The prospective link between externalizing symptoms in middle school and number of sex partners in late high school was one of our most robust findings across reporter. Yet, in the parent-report model, the relation of parent-report externalizing with number of sex partners was only significant for females (not males) and was significantly stronger for youth reporting low mainstream values. Parent-reported externalizing predicted problem alcohol-substance use symptoms for youth reporting higher Mexican American values, but not for those low on Mexican American values. Youth-reported externalizing predicted increased deviant peer involvement only at higher levels of Mexican American values, and the link between substance use and number of sexual partners was significantly stronger for females than for males (yet significant for both).
Internalizing pathways and developmental cascades to risk-taking
We found evidence that internalizing also contributes to later risk-taking. In the youth-reported model, internalizing symptoms in middle school predicted problem alcohol and substance use symptom counts in late high school. In tests of moderation, we also found parent-reported internalizing predicted alcohol and substance use symptom counts for adolescents who endorsed low levels of mainstream cultural values (−1 S.D.), but not at higher levels of mainstream values. These patterns conform with the perspective that some youth with elevated internalizing symptoms may turn to drugs and alcohol to cope with their symptoms (Hussong, et al., 2011). Specifically, internalizing predicted increased alcohol-substance use symptom counts among youth with some probability of being a problem user (i.e., users and occasional users); internalizing did not predictive of whether youth were likely to be users or not. This is an important distinction that parallels other studies that have found internalizing may be more relevant in the etiology of alcohol and substance use problems that emerge in late adolescence and early adulthood, and not as a predictor of substance use onset for which externalizing may have greater relevance (Hussong, Curran, & Chassin, 1998; King, et al., 2004), as we also found. That internalizing was only related to alcohol-drug use symptoms, and not directly related to other aspects of risk-taking (i.e., deviant peers) also indicates a more specific mechanisms may be at play in this association, including possible shared genetic risk (Zucker, et al., 2009).
Although these findings provide relatively circumscribed support for internalizing paths to risk-taking, they offer an important contribution to the literature. The role of internalizing on alcohol and substance use has remained unclear among both Caucasian and Latino adolescent populations (see Hussong, et al., 2011). Extant studies have produced equivocal findings, likely due to a host of methodological factors, such as not controlling for prior substance use or co-occurring externalizing behavior. Thus, by using methods that addressed these prior limitations, this study provides strong, longitudinal evidence that internalizing predicted problematic alcohol and substance use for Mexican American adolescents.
Culture-and gender-specific pathways to risk-taking
We extended our test of problem behavior theory and internalizing pathways by examining moderation of theorized paths by gender, nativity and cultural orientation. Two paths were stronger for females than males (externalizing→ number of sex partners, problem alcohol-substance use→ number of sex partners), two were stronger for youth reporting more traditional Mexican American values (externalizing→ deviant peers, externalizing→ alcohol-substance use symptoms), and two were stronger for youth reporting weaker mainstream cultural values (externalizing→ number of sex partners, internalizing→ alcohol-substance use symptoms).
However, the specific moderation effects were not as hypothesized. Because female, less acculturated, and more traditional youths have been shown in prior research to be less vulnerable to risk-taking, we hypothesized developmental cascades would be weaker for these groups. We found the opposite effects, similar to(Vaughan, Gassman, Jun, & Seitz de Martinez, 2015) who found Latina females had greater predicted probabilities than Latino males for alcohol use, binge drinking, and substance use problems across a range of risk and protective factors. (Burnette, et al., 2012) also found early adolescent externalizing predicted rule-breaking behaviors in girls, but not boys, in late adolescence and explained that because rule-breaking is gender atypical for girls it may be more indicative of an underlying problem for girls than for boys. Research also has shown the disinhibiting effects of alcohol may have stronger associations with risky sex for girls because they are less likely than males to have sex with more than one partner; the less normative or sanctioned sexual intercourse is within a group, the stronger these effects are expected to be (Cavanagh, 2004). We found this effects as well. In fact, we only found gender differences in the prediction of sexual risk-taking, possibly because prohibitions about sex are especially pronounced for Latina girls (Deardorff, et al., 2010; Raffaelli & Ontai, 2004).
Similar arguments about differing norms may also apply to the moderation effects shown for youth cultural orientation. It is possible externalizing predicted deviant peers and alcohol-substance use only among traditionally oriented youth because risk-taking is less normative and less compatible with the values of these youth (e.g., respect toward elders, religious values, family obligations), and therefore less likely to occur in the absence of externalizing psychopathology. Likewise, risk-taking behaviors (i.e., deviant peer involvement, drinking) are more normative and prevalent in the lives of acculturated youth (Prado, et al., 2010), potentially explaining why externalizing showed weaker relations with number of sex partners and internalizing was less predictive of alcohol-substance use among youth with stronger ties to mainstream cultural values. While the pattern of these effects lends credence to this explanation, additional cultural explanations may also apply. For example, it is possible that other culturally-linked processes not included in this study but shown to be important for Latinos, such as intergenerational-acculturative family conflicts or loss of protective cultural identity (Schwartz et al., 2012; Unger, 2014), may play a more salient etiological role for these youth.
Limitations, Future Directions, and Implications
Although this study had several notable strengths, including a representative and diverse Mexican origin sample, culturally-informed assessments of contextual risk, longitudinal data with excellent retention, and modern modeling approaches, there were several limitations. Because we used youth report to assess contextual adversity as well as risk-taking, it is possible that some effects are inflated by shared method variance. To reduce such biases, we used both maternal and youth report to assess internalizing and externalizing symptoms and we controlled for stability of youth symptoms and alcohol-substance use when estimating longitudinal effects. Nevertheless, such biases may still be a factor, particularly in the association between perceived peer rejection and internalizing symptoms. The design of the current study did not allow for a test of all possible cross-domain and cross-time reciprocal effects among our study variables (i.e., cross-lag models), as in traditional cascade models (e.g., (Burt, et al., 2008). Rather, we examined a specific sequence of effects (Lynne-Landsman, Bradshaw, & Ialongo, 2010; Martel et al., 2009; Sitnick, et al., 2014) to test externalizing and internalizing as intervening pathways from early adversity to later risk-taking. Nevertheless, we cannot rule out that several variables in our model likely have recursive effects over time that were not tested. We also note that our measure of problem substance use based on the DISC is not equivalent to the more widely-used substance use items typically used for this age group. This should be considered when making comparisons to other studies. Finally, the study was limited to Mexican Americans in the Southwestern United States. Although this subgroup represents a large and growing demographic in the U.S., findings cannot be generalized to other Latinos. Nor can we isolate whether effects are specific to our Mexican American sample. Nevertheless, our ethnic-homogenous design fills an important gap in research on developmental pathways to risk-taking for a population that is now the single largest ethnic group in the U.S. (U.S. Census Bureau, 2012).
Study results highlight that paths to risk-taking are diverse and variable, and that future theory and research with Mexican Americans should account for both externalizing and internalizing paths and for gender and cultural orientation. Future studies also are needed to replicate and advance understanding of the internalizing path to alcohol and substance use among Mexican American and other Latinos, including studies that can tease out the specific dimensions of negative affect that account for these effects, and for which substances. Although our tests of moderation were conceptualized broadly, they offer guidance for future replication and extension. One potential avenue is to examine whether similar gender differences in the prediction of sexual risk-taking are found in other populations or whether they arise from cultural factors specific to Mexican Americans (i.e., traditional gender roles). Our evidence of cultural moderation also merits extension, including more focused test of specific mainstream and ethnic cultural dimensions and processes that alter developmental cascades. As well, future research that examines “bicultural” adaptation is needed, rather than focusing separately on ethnic and mainstream dimensions as distinct processes.
Despite these limitations, our findings have implications for programs and strategies to reduce several high-impact health consequences in adolescence (e.g., unplanned pregnancy, alcohol and drug abuse, STIs, HIV). Specifically, they recommend a focus on the family as a key target to protect youth from problematic risk-taking behaviors in adolescence, including those that stem from prior psychological problems and from more normative risk-taking with peers. Support also has been provided by efficacy trials of prevention programs that intervened to improve family relationships before or during middle school and demonstrated lasting effects to prevent multiple high risk outcomes (Catalano, Hawkins, Berglund, Pollard, & Arthur, 2002), including behavioral problems, substance use, and risky sex among Latino youths (Catalano, et al., 2002; Gonzales et al., 2012; Pantin, Schwartz, Sullivan, Prado, & Szapocznik, 2004). Findings here illustrate how effects from these programs may unfold over time to produce such broad, long-term benefits.
Study findings also highlight gaps in culturally-adapted programs that have yet to address contextual threats outside the family context, such as difficulties in peer relations. Accumulating evidence suggest that peer social rejection and particularly ethnic and racial discrimination are pervasive in the lives and Latinos and have lasting effects on development, even in the context of well-functioning (low-risk) families. Yet few interventions include strategies to specifically address these pervasive threats. Greater sensitivity to gender-specific paths, such as the stronger link between alcohol-drugs and sex for girls, are also important new directions for broadening prevention models. Although Latina females are often considered at low risk for drug and alcohol use, prevalence is increasing due to changing cultural norms (Johnston, O’Malley, Bachman, & Schulenberg, 2011). The prevalence of alcohol and drug use before sex also is increasing among high school students, (CDC, 2010). Thus, strategies focused on health sexual lifestyles, and the risks of combining sex with alcohol and drugs, are important avenues for prevention and health promotion
Acknowledgments
This research was supported by NIMH grant MH68920 (Culture, Context, and Mexican American Mental Health). The authors are thankful for the support of Mark W. Roosa, Marisela Torres, Leticia Gelhard, Jaimee Virgo, our Community Advisory Board and interviewers, and the families who participated in the study.
Footnotes
Accepted for Publications in Development and Psychopathology
By default, the latent factors W1 family risk and W1 social rejection had means equal to zero.
W2 internalizing symptoms and W2 externalizing symptoms, on the other hand, were treated as continuous variables, as their distributions were close to normal (Skewness = .931, Kurtosis = 1.249 and Skewness = 1.436, Kurtosis = 2.335, respectively).
There were 514 counts of zero out of the 567 reports on W4 alcohol-substance use symptoms, including 273 out of the 288 female reports and 241 out of the 279 male reports; and 329 counts of zero out of the 591 reports on T4 number of sex partners, including 181 out of the 305 female reports and 148 out of the 286 male reports.
The form of Poisson regression for the two count outcomes should be the same in these models, given that the only changes were the reporters of the internalizing and externalizing symptoms, which were used as predictors.
References
- Achenbach TM, McConaughy SH, Howell CT. Child/adolescent behavioral and emotional problems: Implications of cross-informant correlations for situational specificity. Psychological bulletin. 1987;101:213–232. doi: 10.1037/0033-2909.101.2.213. [DOI] [PubMed] [Google Scholar]
- Alegría M, Canino G, Shrout P, Woo M, Duan N, Vila D, Meng X-L. Prevalence of mental illness in immigrant and non-immigrant US Latino groups. American Journal of Psychiatry. 2008;165(3):359–369. doi: 10.1176/appi.ajp.2007.07040704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Almeida J, Johnson RM, Matsumoto A, Godette DC. Substance use, generation and time in the United States: The modifying role of gender for immigrant urban adolescents. Social Science & Medicine. 2012;75:2069–2075. doi: 10.1016/j.socscimed.2012.05.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders : DSM-IV. Washington, DC: American Psychiatric Association; 1994. [Google Scholar]
- Bacio GA, Mays VM, Lau AS. Drinking initiation and problematic drinking among Latino adolescents: Explanations of the immigrant paradox. Psychology of Addictive Behaviors. 2013;27(1):14. doi: 10.1037/a0029996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barrera M, Jr, Caples H, Tein JY. The psychological sense of economic hardship: Measurement models, validity, and cross-ethnic equivalence for urban families. American Journal of Community Psychology. 2001;29:493–517. doi: 10.1023/a:1010328115110. [DOI] [PubMed] [Google Scholar]
- Bazargan-Hejazi S, Gains T, Bazargan M, Seddighzadeh B, Ahmadi A. Alcohol misuse and multiple sexual pPartners. Western Journal of Emergency Medicine. 2012;13(2) doi: 10.5811/westjem.2011.6.6676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benson MJ, Buehler C. Family process and peer deviance influences on adolescent aggression: Longitudinal effects across early and middle adolescence. Child development. 2012;83(4):1213–1228. doi: 10.1111/j.1467-8624.2012.01763.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berkel C, Knight GP, Zeiders KH, Tein JY, Roosa MW, Gonzales NA, Saenz D. Discrimination and adjustment for Mexican American adolescents: A prospective examination of the benefits of culturally related values. Journal of Research on Adolescence. 2010;20(4):893–915. doi: 10.1111/j.1532-7795.2010.00668.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berry JW, Trimble JE, Olmedo EL. Assessment of acculturation. In: Lonner WJ, Berry JW, editors. Field methods in cross-cultural research. Thousand Oaks, CA: Sage Publications, Inc; 1986. pp. 291–324. [Google Scholar]
- Blanco C, Morcillo C, Alegría M, Dedios MC, Fernández-Navarro P, Regincos R, Wang S. Acculturation and drug use disorders among Hispanics in the US. Journal of Psychiatric Research. 2013;47:226–232. doi: 10.1016/j.jpsychires.2012.09.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blinn-Pike L, Berger TJ, Hewett J, Oleson J. Sexually Abstinent Adolescents An 18-Month Follow-Up. Journal of Adolescent Research. 2004;19(5):495–511. [Google Scholar]
- Boivin M, Vitaro F, McCord J. The impact of peer relationships on aggression in childhood: Inhibition through coercion or promotion through peer support. Coercion and punishment in long-term perspectives. 1995:183–197. [Google Scholar]
- Bronfenbrenner U. The ecology of human development: Experiments by design and nature. Cambridge, MA: Harvard University Press; 1979. [Google Scholar]
- Brown BB. Adolescents’ relationships with peers. Handbook of adolescent psychology. 2004;2:363–394. [Google Scholar]
- Burnette ML, Oshri A, Lax R, Richards D, Ragbeer SN. Pathways from harsh parenting to adolescent antisocial behavior: A multidomain test of gender moderation. Development and psychopathology. 2012;24(03):857–870. doi: 10.1017/S0954579412000417. [DOI] [PubMed] [Google Scholar]
- Burt KB, Obradović J, Long JD, Masten AS. The interplay of social competence and psychopathology over 20 years: Testing transactional and cascade models. Child development. 2008;79(2):359–374. doi: 10.1111/j.1467-8624.2007.01130.x. [DOI] [PubMed] [Google Scholar]
- Cano MÁ, Schwartz SJ, Castillo LG, Romero AJ, Huang S, Lorenzo-Blanco EI, Szapocznik J. Depressive symptoms and externalizing behaviors among Hispanic immigrant adolescents: Examining longitudinal effects of cultural stress. Journal of Adolescence. 2015;42:31–39. doi: 10.1016/j.adolescence.2015.03.017. doi: http://dx.doi.org/10.1016/j.adolescence.2015.03.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Capaldi DM, Crosby L, Stoolmiller M. Predicting the timing of first sexual intercourse for at-risk adolescent males. Child development. 1996:344–359. [PubMed] [Google Scholar]
- Catalano RF, Hawkins JD, Berglund ML, Pollard JA, Arthur MW. Prevention science and positive youth development: competitive or cooperative frameworks? Journal of Adolescent Health. 2002;31(6):230–239. doi: 10.1016/s1054-139x(02)00496-2. [DOI] [PubMed] [Google Scholar]
- Cavanagh SE. The sexual debut of girls in early adolescence: The intersection of race, pubertal timing, and friendship group characteristics. Journal of Research on Adolescence. 2004;14(3):285–312. [Google Scholar]
- Centers for Disease Control and Prevention. Youth Risk Behavior Surveillance – United States, 2009. Surveillance Summaries. MMRW. 2010;59:SS-5. Available from: http://www.cdc.gov/mmwr/pdf/ss/ss5905.pdf. [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. Sexually transmitted disease surveillance, 2010. Atlanta, GA: US Department of Health and Human Services; 2011. pp. 33–35. [Google Scholar]
- Centers for Disease Control and Prevention. HIV Surveillance Report, 2009 2012 [Google Scholar]
- Centers for Disease Control and Prevention. Mental Health Surveillance among children – United States 2005–2011. MMWR. 2013;62(02):1–35. Available at http://www.cdc.gov/mmwr/preview/mmwrhtml/su6202a6201.htm#Tab6205. [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. Youth Risk Behavior Surveillance—United States, 2015. MMWR. 2016;65(6):1–174. doi: 10.15585/mmwr.ss6506a1. [DOI] [PubMed] [Google Scholar]
- Child Trends. Teen births: Indicators on children and youth. 2015 Available at: http://www.childtrends.org/?indicators=teen-births.
- Cicchetti D, Carlson V. Child maltreatment: Theory and research on the causes and consequences of child abuse and neglect. Cambridge University Press; 1989. [Google Scholar]
- Coie JD, Dodge KA, Kupersmidt JB. 2 Peer group behavior and social status. Peer rejection in childhood. 1990;17 [Google Scholar]
- Conger RD, Lorenz FO, Elder GH, Melby JN, Simons RL, Conger KJ. A process model of family economic pressure and early adolescent alcohol use. The Journal of early adolescence. 1991;11(4):430–449. [Google Scholar]
- Corona M, McCarty C, Cauce AM, Robins RW, Widaman KF, Conger RD. The Relation Between Maternal and Child Depression in Mexican American Families. Hispanic journal of behavioral sciences. 2012;34(4):539–556. doi: 10.1177/0739986312455160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coxe S, West SG, Aiken LS. The analysis of count data: A gentle introduction to Poisson regression and its alternatives. Journal of personality assessment. 2009;91(2):121–136. doi: 10.1080/00223890802634175. [DOI] [PubMed] [Google Scholar]
- Crick NR, Bigbee MA. Relational and overt forms of peer victimization: A multiinformant approach. Journal of consulting and clinical psychology. 1998;66:337–347. doi: 10.1037/0022-006x.66.2.337. [DOI] [PubMed] [Google Scholar]
- Davies PT, Cummings EM. Exploring children’s emotional security as a mediator of the link between marital relations and child adjustment. Child development. 1998;69(1):124–139. [PubMed] [Google Scholar]
- De Los Reyes A. Strategic objectives for improving understanding of informant discrepancies in developmental psychopathology research. Development and psychopathology. 2013;25:669–682. doi: 10.1017/S0954579413000096. [DOI] [PubMed] [Google Scholar]
- De Los Reyes A, Augenstein TM, Wang M, Thomas SA, Drabick DAG, Burgers DE, Rabinowitz J. The validity of the multi-informant approach to assessing child and adolescent mental health. Psychological Bulletin. 2015;141:858–900. doi: 10.1037/a0038498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deardorff J, Tschann JM, Flores E, Ozer EJ. Sexual values and risky sexual behaviors among Latino youths. Perspect Sex Reprod Helath. 2010;42:23–32. doi: 10.1363/4202310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Delgado MY, Updegraff KA, Roosa MW, Umaña-Taylor AJ. Discrimination and Mexican-origin adolescents’ adjustment: The moderating roles of adolescents’, mothers’, and fathers’ cultural orientations and values. Journal of Youth and Adolescence. 2011;40(2):125–139. doi: 10.1007/s10964-009-9467-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dishion TJ, Patterson GR, Stoolmiller M, Skinner ML. Family, school, and behavioral antecedents to early adolescent involvement with antisocial peers. Developmental psychology. 1991;27(1):172. [Google Scholar]
- Dodge KA, Dishion TJ, Lansford JE. Social Policy Report. 1. Vol. 20. Society for Research in Child Development; 2006. Deviant Peer Influences in Intervention and Public Policy for Youth. [Google Scholar]
- Dodge KA, Malone PS, Lansford JE, Miller S, Pettit GS, Bates JE. A dynamic cascade model of the development of substance-use onset. Monogr Soc Res Child Dev. 2009;74(3) doi: 10.1111/j.1540-5834.2009.00528.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Donenberg GR, Emerson E, Mackesy-Amiti ME. Sexual risk among African American girls: Psychopathology and mother–daughter relationships. Journal of consulting and clinical psychology. 2011;79(2):153. doi: 10.1037/a0022837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Enders CK. Applied missing data analysis. Guilford Press; 2010. [Google Scholar]
- Frauenglass S, Routh DK, Pantin HM, Mason CA. Family support decreases influence of deviant peers on Hispanic adolescents’ substance use. Journal of Clinical Child Psychology. 1997;26(1):15–23. doi: 10.1207/s15374424jccp2601_2. [DOI] [PubMed] [Google Scholar]
- Garcia Coll C, Lamberty G, Jenkins R, McAdoo HP, Crnic K, Wasik BH, Vazquez-Garcia J. An integrative model for the study of developmental competencies in minority children. Child Development. 1996;67(5):1891–1914. [PubMed] [Google Scholar]
- Germán M, Gonzales NA, Dumka L. Familism values as a protective factor for Mexican-origin adolescents exposed to deviant peers. The Journal of early adolescence. 2009;29(1):16–42. doi: 10.1177/0272431608324475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibbons FX, Yeh HC, Gerrard M, Cleveland MJ, Cutrona C, Simons RL, Brody GH. Early experience with racial discrimination and conduct disorder as predictors of subsequent drug use: A critical period hypothesis. Drug and Alcohol Dependence. 2007;88(1):S27–S37. doi: 10.1016/j.drugalcdep.2006.12.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glover SH, Pumariega AJ, Holzer CE, Wise BK, Rodriguez M. Anxiety symptomatology in Mexican-American adolescents. Journal of Child and Family Studies. 1999;8(1):47–57. doi: 10.1023/a:1022994510944. [DOI] [Google Scholar]
- Gonzales NA, Deardorff J, Formoso D, Barr A, Barrera M., Jr Family mediators of the relation between acculturation and adolescent mental health. Family Relations. 2006;55(3):318–330. [Google Scholar]
- Gonzales NA, Dumka LE, Millsap RE, Gottschall A, McClain DB, Wong JJ, Kim SY. Randomized trial of a broad preventive intervention for Mexican American adolescents. Journal of Consulting and Clinical Psychology. 2012;80(1):1–16. doi: 10.1037/a0026063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gonzales NA, Germán M, Fabrett FC. U.S. Latino Youth. Handbook of Race and Development in Mental Health 2012 [Google Scholar]
- Gonzales NA, Tein JY, Sandler IN, Friedman RJ. On the limits of coping interaction between stress and coping for inner-city adolescents. Journal of Adolescent Research. 2001a;16(4):372–395. [Google Scholar]
- Gonzales NA, Tein JY, Sandler IN, Friedman RJ. On the limits of coping: Interaction between stress and coping for inner-city adolescents. Journal of Adolescent Research. 2001b;16(4):372–395. doi: 10.1177/0743558401164005. [DOI] [Google Scholar]
- Graham S, Juvonen J. Self-blame and peer victimization in middle school: An attributional analysis. Developmental psychology. 1998;34:587–599. doi: 10.1037/0012-1649.34.3.587. [DOI] [PubMed] [Google Scholar]
- Greene ML, Way N, Pahl K. Trajectories of perceived adult and peer discrimination among Black, Latino, and Asian American adolescents: patterns and psychological correlates. Developmental psychology. 2006;42(2):218. doi: 10.1037/0012-1649.42.2.218. [DOI] [PubMed] [Google Scholar]
- Grigsby TJ, Forster M, Soto DW, Baezconde-Garbanati L, Unger JB. Problematic substance use among Hispanic adolescents and young adults: Implications for prevention efforts. Substance Use & Misuse. 2014;49:1025–1038. doi: 10.3109/10826084.2013.852585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haller M, Handley E, Chassin L, Bountress K. Developmental cascades: Linking adolescent substance use, affiliation with substance use promoting peers, and academic achievement to adult substance use disorders. Development and psychopathology. 2010;22(04):899–916. doi: 10.1017/S0954579410000532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hanish LD, Guerra NG. A longitudinal analysis of patterns of adjustment following peer victimization. Development and psychopathology. 2002;14(01):69–89. doi: 10.1017/s0954579402001049. [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Catalano RF, Miller JY. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: implications for substance abuse prevention. Psychological bulletin. 1992;112(1):64. doi: 10.1037/0033-2909.112.1.64. [DOI] [PubMed] [Google Scholar]
- Hussong AM, Curran PJ, Chassin L. Pathways of risk for accelerated heavy alcohol use among adolescent children of alcoholic parents. Journal of abnormal child psychology. 1998;26:453–466. doi: 10.1023/a:1022699701996. [DOI] [PubMed] [Google Scholar]
- Hussong AM, Jones DJ, Stein GL, Baucom DH, Boeding S. An internalizing pathway to alcohol use and disorder. Psychology of Addictive Behaviors. 2011;25(3):390. doi: 10.1037/a0024519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jensen MR, Wong JJ, Gonzales NA, Dumka LE, Millsap R, Coxe S. Long-term effects of a universal family intervention: Mediation through parent-adolescent conflict. Journal of Clinical Child & Adolescent Psychology. 2014:1–13. doi: 10.1080/15374416.2014.891228. (ahead-of-print) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jessor R, Jessor SL. Problem behavior and psychosocial development: A longitudinal study of youth. New York, NY: Academic Press; 1977. [Google Scholar]
- Jessor R, Turbin MS, Costa FM, Dong Q, Zhang H, Wang C. Adolescent problem behavior in China and the United States: A cross-national study of psychosocial protective factors. Journal of Research on Adolescence. 2003;13:329–360. doi: 10.1111/1532-7795.1303004. [DOI] [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future national survey results on drug use, 1975–2010: Volume I, Secondary school students. Ann Arbor, MI: Institute for Social Research, The University of Michigan; 2011. [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the future national results on adolescent drug use: Overview of key findings, 2011. Ann Arbor, MI: Institute for Social Researh, The University of Michigan; 2012. [Google Scholar]
- Juvonen J, Graham S, Schuster MA. Bullying among young adolescents: The strong, the weak, and the troubled. Pediatrics. 2003;112(6):1231–1237. doi: 10.1542/peds.112.6.1231. [DOI] [PubMed] [Google Scholar]
- Kann L, Kinchen S, Shanklin SL, Flint KH, Kawkins J, Harris WA, Zaza S. Youth risk behavior surveillance—United States, 2013. MMWR. 2014;63(Suppl 4):1–168. [PubMed] [Google Scholar]
- Kelder SH, Murray NG, Orpinas P, Prokhorov A, McReynolds L, Qing Z, Roberts R. Depression and substance use in minority middle-school students. American Journal of Public Health. 2001;91:761–766. doi: 10.2105/ajph.91.5.761. [DOI] [PMC free article] [PubMed] [Google Scholar]
- King SM, Iacono WG, McGue M. Childhood externalizing and internalizing psychopathology in the prediction of early substance use. Addiction. 2004;99:1548–1559. doi: 10.1111/j.1360-0443.2004.00893.x. [DOI] [PubMed] [Google Scholar]
- Knight GP, Gonzales NA, Saenz DS, Bonds DD, German M, Deardorff J, Updegraff KA. The Mexican American Cultural Values Scale for adolescents and adults. Journal of Early Adolescence. 2010;30:444–481. doi: 10.1177/0272431609338178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kochenderfer‐Ladd B, Wardrop JL. Chronicity and instability of children’s peer victimization experiences as predictors of loneliness and social satisfaction trajectories. Child development. 2001;72(1):134–151. doi: 10.1111/1467-8624.00270. [DOI] [PubMed] [Google Scholar]
- Kulis S, Marsiglia FF, Nieri T. Perceived ethnic discrimination versus acculturation stress: Influences on substance use among Latino youth in the Southwest. Journal of health and social behavior. 2009;50(4):443–459. doi: 10.1177/002214650905000405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lansford JE, Criss MM, Pettit GS, Dodge KA, Bates JE. Friendship quality, peer group affiliation, and peer antisocial behavior as moderators of the link between negative parenting and adolescent externalizing behavior. Journal of Research on Adolescence. 2003;13(2):161–184. doi: 10.1111/1532-7795.1302002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Larson R, Ham M. Stress and “storm and stress” in early adolescence: The relationship of negative events with dysphoric affect. Developmental psychology. 1993;29(1):130. [Google Scholar]
- Lev-Wiesel R, Sarid M, Sternberg R. Measuring Social Peer Rejection during Childhood: Development and Validation. Journal of Aggression, Maltreatment & Trauma. 2013;22(5):482–492. [Google Scholar]
- Lopez B, Schwartz SJ, Prado G, Huang S, Rothe EM, Wang W, Pantin H. Correlates of early alcohol and drug use in Hispanic adolescents: Examining the role of ADHD with comorbid conduct disorder, family, school, and peers. Journal of Clinical Child & Adolescent Psychology. 2008;37:820–832. doi: 10.1080/15374410802359676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lorenzo-Blanco EI, Unger JB, Ritt-Olson A, Soto D, Baezconde-Garbanati L. Acculturation, gender, depression, and cigarette smoking among US Hispanic youth: The mediating role of perceived discrimination. Journal of Youth and Adolescence. 2011;40(11):1519–1533. doi: 10.1007/s10964-011-9633-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lynne-Landsman SD, Bradshaw CP, Ialongo NS. Testing a developmental cascade model of adolescent substance use trajectories and young adult adjustment. Development and psychopathology. 2010;22(04):933–948. doi: 10.1017/S0954579410000556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martel MM, Pierce L, Nigg JT, Jester JM, Adams K, Puttler LI, Zucker RA. Temperament pathways to childhood disruptive behavior and adolescent substance abuse: Testing a cascade model. Journal of abnormal child psychology. 2009;37(3):363–373. doi: 10.1007/s10802-008-9269-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Masten AS, Cicchetti D. Developmental cascades. Development and psychopathology. 2010;22(03):491–495. doi: 10.1017/S0954579410000222. [DOI] [PubMed] [Google Scholar]
- McLeod JD, Knight S. The association of socioemotional problems with early sexual initiation. Perspectives on Sexual and Reproductive Health. 2010;42(2):93–101. doi: 10.1363/4209310. [DOI] [PubMed] [Google Scholar]
- Merikangas KR, He JP, Brody D, Fisher PW, Bourdon K, Koretz DS. Prevalence and treatment of mental disorders among US Children in the 2001–2004 NHANES. Pediatrics. 2010;125(1):75–81. doi: 10.1542/peds.2008-2598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer GJ, Finn SE, Eyde LD, Kay GG, Moreland KL, Dies RR, Reed GM. Psychological testing and psychological assessment: A review of evidence and issues. American Psychologist. 2001;56:128–165. doi: 10.1037/0003-066x.56.2.128. [DOI] [PubMed] [Google Scholar]
- Moffitt TE, Caspi A. Childhood predictors differentiate life-course persistent and adolescence-limited antisocial pathways among males and females. Development and psychopathology. 2001;13(02):355–375. doi: 10.1017/s0954579401002097. [DOI] [PubMed] [Google Scholar]
- Monahan KC, Lee JM. Adolescent sexual activity: Links between relational context and depressive symptoms. Journal of Youth and Adolescence. 2008;37(8):917–927. [Google Scholar]
- Muthén L, Muthén B. BO 1998–2012. Mplus user’s guide 1998–2012 [Google Scholar]
- Nair RL, White R, Knight GP, Roosa MW. Cross-language measurement equivalence of parenting measures for use with Mexican American populations. Journal of Family Psychology. 2009;23(5):680. doi: 10.1037/a0016142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Committee on the Prevention of Mental Disorders and Substance Abuse Among Children, Youth, and Young Adults: Research Advances and Promising Interventions. O’Connell Mary Ellen, Boat Thomas, Warner Kenneth E., editors. National Research Council and Institute of Medicine. Preventing mental, emotional, and behavioral disorders among young people: Progress and possibilities. Washington, D.C.: National Academics Press; 2009. Board on Children, Youth, and Families, Division of Behavioral and Social Sciences and Education. [PubMed] [Google Scholar]
- Nolan SA, Flynn C, Garber J. Prospective relations between rejection and depression in young adolescents. Journal of personality and social psychology. 2003;85(4):745. doi: 10.1037/0022-3514.85.4.745. [DOI] [PubMed] [Google Scholar]
- Okamoto J, Ritt-Olson A, Soto D, Baezconde-Garbanati L, Unger JB. Perceived discrimination and substance use among Latino adolescents. American Journal of Health behavior. 2009;33:718–727 710. doi: 10.5993/AJHB.33.6.9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oshri A, Rogosch FA, Burnette ML, Cicchetti D. Developmental pathways to adolescent cannabis abuse and dependence: Child maltreatment, emerging personality, and internalizing versus externalizing psychopathology. Psychology of Addictive Behaviors. 2011;25(4):634. doi: 10.1037/a0023151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pantin H, Schwartz SJ, Sullivan S, Prado G, Szapocznik J. Ecodevelopmental HIV Prevention Programs for Hispanic Adolescents. American Journal of Orthopsychiatry. 2004;74:545–558. doi: 10.1037/0002-9432.74.4.545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pasch LA, Deardorff J, Tschann JM, Flores E, Penilla C, Pantoja P. Acculturation, parent-adolescent conflict, and adolescent adjustment in mexican american families. Family Process. 2006;45(1):75–86. doi: 10.1111/j.1545-5300.2006.00081.x. [DOI] [PubMed] [Google Scholar]
- Patterson GR, Reid JB, Dishion TJ. Antisocial boys. Vol. 4. Castalia Pub Co; 1992. [Google Scholar]
- Pettit GS, Bates JE, Dodge KA, Meece DW. The impact of after‐school peer contact on early adolescent externalizing problems is moderated by parental monitoring, perceived neighborhood safety, and prior adjustment. Child development. 1999;70(3):768–778. doi: 10.1111/1467-8624.00055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Platt B, Kadosh KC, Lau JY. The role of peer rejection in adolescent depression. Depression and anxiety. 2013;30(9):809–821. doi: 10.1002/da.22120. [DOI] [PubMed] [Google Scholar]
- Prado G, Huang Shi, Maldonado-Molina M, Bandiera F, Schwartz SJ, de la Vega P, Pantin H. An empirical test of ecodevelopmental theory in predicting HIV risk behaviors among Hispanic youth. Health Education & behavior. 2010;37(1):97–114. doi: 10.1177/1090198109349218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prado G, Szapocznik J, Maldonado-Molina MM, Schwartz SJ, Pantin H. Drug use/abuse prevalence, etiology, prevention, and treatment in Hispanic adolescents: A cultural perspective. Journal of Drug Issues. 2008;38(1):5–36. doi: 10.1177/002204260803800102. [DOI] [Google Scholar]
- Prinstein MJ, Boergers J, Vernberg EM. Overt and relational aggression in adolescents: Social-psychological adjustment of aggressors and victims. Journal of Clinical Child Psychology. 2001;30(4):479–491. doi: 10.1207/S15374424JCCP3004_05. [DOI] [PubMed] [Google Scholar]
- Prinstein MJ, La Greca AM. Childhood peer rejection and aggression as predictors of adolescent girls’ externalizing and health risk behaviors: a 6-year longitudinal study. Journal of consulting and clinical psychology. 2004;72(1):103. doi: 10.1037/0022-006X.72.1.103. [DOI] [PubMed] [Google Scholar]
- Raffaelli M, Ontai LL. Gender socialization in Latino/a families: Results from two retrospective studies. Sex Roles. 2004;50(5–6):287–299. [Google Scholar]
- Repetti RL, Taylor SE, Seeman TE. Risky families: family social environments and the mental and physical health of offspring. Psychological bulletin. 2002;128(2):330. [PubMed] [Google Scholar]
- Roberts RE, Chen YW. Depressive symptoms and suicidal ideation among Mexican-Origin and Anglo adolescents. Journal of the American Academy of Child & Adolescent Psychiatry. 1995;34(1):81–90. doi: 10.1097/00004583-199501000-00018. [DOI] [PubMed] [Google Scholar]
- Roberts RE, Roberts CR, Chen YR. Ethnocultural differences in prevalence of adolescent depression. American journal of community psychology. 1997;25(1):95–110. doi: 10.1023/a:1024649925737. [DOI] [PubMed] [Google Scholar]
- Rogosch FA, Oshri A, Cicchetti D. From child maltreatment to adolescent cannabis abuse and dependence: A developmental cascade model. Development and psychopathology. 2010;22(04):883–897. doi: 10.1017/S0954579410000520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roosa MW, Liu FF, Torres M, Gonzales NA, Knight GP, Saenz D. Sampling and recruitment in studies of cultural influences on adjustment: a case study with Mexican Americans. Journal of Family Psychology. 2008;22(2):293. doi: 10.1037/0893-3200.22.2.293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rudolph KD, Hammen C. Age and gender as determinants of stress exposure, generation, and reactions in youngsters: A transactional perspective. Child development. 1999;70(3):660–677. doi: 10.1111/1467-8624.00048. [DOI] [PubMed] [Google Scholar]
- Ruiz S, Gonzales N, Formoso D. Multicultural, multidimensional assessment of parent-adolescent conflict; Paper presented at the Poster presented at the Seventh Biennial Meeting of the Society for Research on Adolescence; San Diego, CA. 1998. [Google Scholar]
- Rutter M. Protective factors in children’s responses to stress and disadvantage. Annals of the Academy of Medicine, Singapore. 1979;8(3):324. [PubMed] [Google Scholar]
- Santelli JS, Lindberg LD, Abma J, McNeely CS, Resnick M. Adolescent sexual behavior: Estimates and trends from four nationally representative surveys. Family Planning Perspectives. 2000;32:156–194. doi: 10.2307/2648232. [DOI] [PubMed] [Google Scholar]
- Scalco MD, Colder CR, Hawk LW, Jr, Read JP, Wieczorek WF, Lengua LJ. Internalizing and externalizing problem behavior and early adolescent substance use: A test of a latent variable interaction and conditional indirect effects. Psychology of Addictive Behaviors. 2014;28(3):828. doi: 10.1037/a0035805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schaefer ES. A configurational analysis of children’s reports of parent behavior. Journal of consulting psychology. 1965;29(6):552. doi: 10.1037/h0022702. [DOI] [PubMed] [Google Scholar]
- Schwartz SJ, Des Rosiers S, Zamboana BL, Unger JB, Knight GP, Pantin H, Szapocznik J. Developmental trajectories of acculturation in Hispanic adolescents: Associations with family functioning and adolescent risk behavior. Child Development. 2013;84:1355–1372. doi: 10.1111/cdev.12047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz SJ, Mason CA, Pantin H, Brown CH, Wang W, Campo AE, Szapocznik J. Relationships of social context and identity to problem behavior among high-risk Hispanic adolescents. Youth & Society. 2009;40:541–570. doi: 10.1177/0044118x08327506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz SJ, Unger JB, Baezconde-Garbanati L, Zamboanga BL, Lorenzo-Blanco EI, Des Rosiers SE, Szapocznik J. Trajectories of cultural stressors and effects on mental health and substance use among Hispanic immigrant adolescents. Journal of Adolescent Health. 2015;56:433–439. doi: 10.1016/j.jadohealth.2014.12.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz SJ, Unger JB, Rosiers SED, Huang S, Baezconde-Garbanati L, Lorenzo-Blanco EI, Szapocznik J. Substance use and sexual behavior among recent Hispanic immigrant adolescents: Effects of parent–adolescent differential acculturation and communication. Drug and Alcohol Dependence. 2012;125:S26–S34. doi: 10.1016/j.drugalcdep.2012.05.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz SJ, Unger JB, Zamboanga BL, Szapocznik J. Rethinking the concept of acculturation: Implications for theory and research. American Psychologist. 2010;65(4):237–251. doi: 10.1037/a0019330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaffer D, Fisher P, Lucas CP, Dulcan MK, Schwab-Stone ME. NIMH Diagnostic Interview Schedule for Children Version IV (NIMH DISC-IV): description, differences from previous versions, and reliability of some common diagnoses. Journal of the American Academy of Child & Adolescent Psychiatry. 2000;39(1):28–38. doi: 10.1097/00004583-200001000-00014. [DOI] [PubMed] [Google Scholar]
- Siegel JM, Aneshensel CS, Taub B, Cantwell DP, Driscoll AK. Adolescent depressed mood in a multiethnic sample. Journal of Youth and Adolescence. 1998;27:413–427. doi: 10.1023/a:1022873601030. [DOI] [Google Scholar]
- Siegel RS, La Greca AM, Harrison HM. Peer victimization and social anxiety in adolescents: Prospective and reciprocal relationships. Journal of Youth and Adolescence. 2009;38:1096–1109. doi: 10.1007/s10964-009-9392-1. [DOI] [PubMed] [Google Scholar]
- Sitnick SL, Shaw DS, Hyde LW. Precursors of adolescent substance use from early childhood and early adolescence: testing a developmental cascade model. Dev Psychopathol. 2014;26(1):125–140. doi: 10.1017/S0954579413000539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smokowski PR, Rose R, Bacallao ML. Acculturation and latino family processes: How cultural involvement, biculturalism, and acculturation gaps influence family dynamics. Family Relations. 2008;57(3):295–308. [Google Scholar]
- Stein GL, Gonzalez LM, Cupito AM, Kiang L, Supple AJ. The protective role of familism in the lives of Latino adolescents. Journal of Family Issues. 2015;36:1255–1273. doi: 10.1177/0192513x13502480. [DOI] [Google Scholar]
- Steinberg L, Morris AS. Adolescent development. Journal of Cognitive Education and Psychology. 2001;2(1):55–87. [Google Scholar]
- Szapocznik J, Coatsworth JD. An ecodevelopmental framework for organizing the influences on drug abuse: A developmental model of risk and protection. In: Glantz MD, Hartel CR, editors. Drug abuse: Origins & interventions. Washington, DC: American Psychological Association; 1999. pp. 331–336. [Google Scholar]
- Telzer EH, Gonzales N, Fuligni AJ. Family Obligation Values and Family Assistance Behaviors: Protective and Risk Factors for Mexican–American Adolescents’ Substance Use. Journal of Youth and Adolescence. 2014;43(2):270–283. doi: 10.1007/s10964-013-9941-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thornberry TP, Lizotte AJ, Krohn MD, Farnworth M, Jang SJ. Delinquent Peers, Beliefs, And Delinquent Behavior: A Longitudinal Test Of Interactional Theory*. Criminology. 1994;32(1):47–83. [Google Scholar]
- Tolan PH, Guerra NG, Montaini-Klovdahl LR. Staying out of harm’s way: Coping and the development of inner city children. In: Wolchik SA, Sandler IN, editors. Handbook of children’s coping: Linking theory, research, and interventions. New York: Plenum; 1997. pp. 453–479. [Google Scholar]
- Toro PA, Urberg KA, Heinze HJ. Antisocial behavior and affiliation with deviant peers. Journal of Clinical Child and Adolescent Psychology. 2004;33(2):336–346. doi: 10.1207/s15374424jccp3302_15. [DOI] [PubMed] [Google Scholar]
- U.S. Census Bureau. The Hispanic Population in the United States: 2012 2012 [Google Scholar]
- Umaña-Taylor AJ, Updegraff KA. Latino adolescents’ mental health: Exploring the interrelations among discrimination, ethnic identity, cultural orientation, self-esteem, and depressive symptoms. Journal of Adolescence. 2007;30:549–567. doi: 10.1016/j.adolescence.2006.08.002. [DOI] [PubMed] [Google Scholar]
- Unger JB. Cultural Influences on substance use among Hispanic adolescents and young adults: Findings from Project RED. Child Development Perspectives. 2014;8(1):48–53. doi: 10.1111/cdep.12060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vargas DA, Roosa MW, Knight GP, O’Donnell M. Family and cultural processes linking family instability to Mexican American adolescent adjustment. Journal of Family Psychology. 2013;27(3):387. doi: 10.1037/a0032863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vaughan EL, Gassman RA, Jun MC, Seitz de Martinez BJ. Gender differences in risk and protective factors for alcohol use and substance use problems among Hispanic adolescents. Journal of Child & Adolescent Substance Abuse. 2015;24:243–254. doi: 10.1080/1067828x.2013.826609. [DOI] [Google Scholar]
- Vernberg EM, Jacobs AK, Hershberger SL. Peer victimization and attitudes about violence during early adolescence. Journal of Clinical Child Psychology. 1999;28(3):386–395. doi: 10.1207/S15374424jccp280311. [DOI] [PubMed] [Google Scholar]
- Watt TT, Martinez-Ramos G. The developmental health of Hispanic children: Evidence from the 2003 National Survey of Children’s Health. Sociological Focus. 2009;42(2):87–106. doi: 10.1080/00380237.2009.10571345. [DOI] [Google Scholar]
- Zeiders KH, Doane LD, Roosa MW. Perceived discrimination and diurnal cortisol: Examining relations among Mexican American adolescents. Hormones and behavior. 2012;61(4):541–548. doi: 10.1016/j.yhbeh.2012.01.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zucker RA, Donovan JE, Masten AS, Mattson ME, Moss HB. Developmental processes and mechanisms: ages 0-10. Alcohol Res Health. 2009;32(1):16–29. [PMC free article] [PubMed] [Google Scholar]