

Abstract
Background
Rapid immunochromatographic tests (ICT) for dengue non-structural protein 1 (NS1) have shown good performance for diagnosing acute-phase dengue in serum in laboratory settings, but rarely have been assessed in whole blood and at point of care (POC). This study compare the accuracy and inter- and intra-observer reliability of the NS1 Bioeasy™ ICT in whole blood at POC versus serum in the laboratory, during a DENV-1 epidemic.
Methods
Cross-sectional study involving 144 adults spontaneously demanding care in an emergency department within 4 days of onset of acute febrile illness. Accuracy of NS1 Bioeasy™ ICT was compared in whole blood and serum, both at 15 and 30 min, blinded to the reference RT-PCR or NS1 ELISA. Non-dengue patients were also tested for Zika virus with RT-PCR. Reliability of whole blood and serum readings by the same or different observers was measured by simple kappa (95% CI).
Results
At 15 min, sensitivity (Sn) of NS1 Bioeasy™ ICT in whole blood/POC was 76.7% (95% CI: 68.0–84.1) and specificity (Sp) was 87.0% (95% CI: 66.4–97.2). Sn in serum/laboratory was 82% (95% CI: 74.1–88.6) and Sp 100% (95% CI: 85.8–100). Positive likelihood ratio was 5.9 (95% CI: 2.0–17.0) for whole blood/POC and 19.8 (95% CI: 2.9–135.1) for serum/laboratory. Reliability of matched readings of whole blood/POC and serum/laboratory by the same observer (k = 0.83, 95% CI: 0.74–0.93) or different observers (k = 0.81, 95% CI: 0.72–0.92) was almost perfect, with higher discordant levels in the absence of dengue. Results did not differ statistically at 5%.
Conclusions
NS1 Bioeasy™ ICT in DENV-1 epidemics is a potentially confirmatory test. Invalid results at 15 min should be reread at 30 min. To optimize impact of implementing ICT in the management of false-negatives it should be incorporated into an algorithm according to setting and available specimen.
Trial registration
Keywords: Dengue, Sensitivity and specificity, Diagnosis, Point-of-care systems, NS1, Reproducibility of results
Background
Dengue virus (DENV) is an international public health problem, especially serotype 1 (DENV-1), which shows the highest frequency in the world [1]. The continents with the highest incidence of dengue are America and Asia with 84% of the 390 million cases in the world per year [2]. A systematic analysis on the global burden of dengue suggested that, in 2013, disease costs worldwide may have reached U$ 8.9 billion [3].
Clinical suspicion of dengue is based on the signs and symptoms described in the World Health Organization (WHO) guidelines, i.e., nausea/vomiting, rash, aches and pains, leucopenia, any warning sign (abdominal pain or tenderness, persistent vomiting, clinical fluid accumulation, mucosal bleeding, lethargy/restlessness, liver enlargement, and hemoconcentration concurrent with rapid decrease in platelet count). However, this criterion shows low specificity due to the absence of confirmatory laboratory tests [4].
A study conducted in the United States showed that laboratory diagnostic tests assist health decisions in 60–70% of cases [5]. The World Health Organization (WHO) recommends that ideal laboratory diagnostic tests should be affordable, sensitive, specific, user-friendly, robust, rapid (can be stored at room temperature and interpreted within 30 min), equipment-free, and deliverable to those who need them (ASSURED) [6].
Rapid immunochromatographic tests (ICT) for dengue with the detection of non-structural protein 1 (NS1) meet some of the characteristics of an ASSURED test: high specificity, ranging from 82.8% [7] to 100% [8–12], simple presentations, whether in cassette or strip format, and rapid interpretation of results (15 to 30 min) [13]. However, the sensitivity showed substantial discrepancy, ranging from 55.2% to 94.3% [10, 11].
In addition, the advantages of ICT in cassette format include the possibility of performing the test in whole blood specimens rather than serum and not requiring a specific infrastructure (equipment-free). This allows their deployment in sites with limited resources, for example at point of care (POC) [7, 12–15]. The tests offer rapid results – allowing the implementation of adequate therapy and care in time to avoid possible complications and even unnecessary costs [16]. Meanwhile, ICT in strip test format requires the use of a centrifuge, reagents, storage in a refrigerator, and test tubes to perform the reaction [7–12, 17].
Dengue NS1 ICTs in cassette or strip format have been evaluated in the last decade, mainly for serotypes 1, 2, and 3, with the best performance in the first 5 days of the illness. Still, these studies mostly used serum specimens, whether from biobanks [8, 10, 11] or processed in laboratory settings [8–12]. Lack of the test’s evaluation in whole blood specimens hinders evaluation of ICT performance at POC and the recommendation of its deployment by health systems in epidemic situations [18].
The accuracy and reliability of ICTs for dengue NS1 are essential for guaranteeing quality tests. Still, few published studies on dengue have evaluated agreement between observers with different levels of training [19] or similar levels [14, 20], varying from moderate to almost perfect agreement. No studies were identified that evaluated the reliability of ICTs according to the types of specimens (whole blood versus serum) or settings.
A literature search detected only one study that evaluated duo ICT (NS1/IgM/IgG) and single NS1 using whole blood at POC, with sensitivities of 93.9% (95% CI: 88.8–96.8) and 81.6% (95% CI:74.6–87.1), and specificities of 92% (95% CI: 81.2–96.9) and 98% (95% CI: 89.5–99.7), respectively. Inter-observer reliability proved almost perfect (kappa = 1 95% 95% CI: 0.84–1) [21].
The current study thus aimed to compare the accuracy and reliability of NS1 Bioeasy™ ICT in whole blood at POC and in serum in the laboratory in adults during a DENV-1 epidemic in Rio de Janeiro State, Brazil.
Methods
This was a prospective diagnostic cross-sectional study that evaluated accuracy of the NS1 Bioeasy™ rapid immunochromatographic test and inter- and intra-observer reliability in whole blood specimens at point of care (POC) and serum specimens in the laboratory. The study was conducted according to the Standards for Reporting Studies of Diagnostic Accuracy (STARD) [22].
The study population consisted of patients over 18 years of age with up to 4 days of acute febrile syndrome without an established diagnosis, treated consecutively and by spontaneous demand at an emergency hospital of the Resende Municipal Health Secretariat, Rio de Janeiro State, Brazil, during a dengue epidemic in March 2015.
Data collection
The selected patients answered a questionnaire on clinical signs and symptoms associated with dengue according to WHO 2009 criteria for Dengue diagnosis [4, 23]. All of them signed the free and informed consent form.
Three blood specimens were drawn in vacuum tubes by a nurse and four medical students. Prior asepsis was performed with 70% alcohol, followed by brachial venipuncture with a 25 × 7 mm BD Vacutainer® needle. One tube with EDTA K2 was sent to the hospital laboratory for performing a complete blood count, another with heparin for ICT with whole blood at POC and the third with clotting activator and gel separator for obtaining serum. The latter was transported to the Flavivirus Laboratory, where it remained frozen at −70 °C for subsequent characterization of the specimen and ICT with serum.
The ICTs with whole blood were performed at point of care in the hospital by a nurse, and the ICTs with serum by a biologist and the same nurse (that performed ICT with blood at POC), in the Flavivirus Laboratory of the Oswaldo Cruz Institute, FIOCRUZ, the regional reference laboratory in Rio de Janeiro State. The observers were blinded to the reference test.
Diagnosis
Index test
The index test used was Dengue Eden Test NS1 ICT from the Bioeasy™ company. This is a rectangular cassette with an orifice to add whole blood, serum, or plasma, and which contains an immunochromatographic membrane coated with NS1 antigen on the test line (T) and a window to view the result. When only the control line (C) is visible, the test is considered negative; if lines C and T are visible, the result is positive; and when no line or only the T line is visible, the test result is invalid [13].
The tests were performed according to manufacturer’s instructions and with readings at 15 and 30 min. Tests with invalid results at 15 min were reread at 30 min.
Reference test
All samples were tested using Reverse Transcription Polymerase Chain Reaction (RT-PCR) for dengue and Platelia™ Dengue NS1 Ag-ELISA (Bio-Rad™ Laboratories, France) as reference, performed according to the protocol described by Lanciotti et al. [24] and the manufacturer’s specifications, respectively [25]. Dengue cases were defined by a positive result in at least one of them and non-dengue by negative results in both. Positive specimens according to the reference test were tested by Dengue Serion ELISA classic dengue virus IgM and IgG tests (Virion/Serion, Würzburg, Germany) [26], according to manufacturers’ specifications for characterization of primary and secondary cases, respectively.
Non-dengue patients were also tested for Zika virus with RT-PCR [27] to investigate co-circulation of these viruses.
The reference tests were performed at the Flavivirus Laboratory by two biologists blinded to the index test.
Statistical analysis
The qualitative variables were described by simple frequencies and the quantitative variables by the median with interquartile range (IQR) or minimum and maximum. Shapiro-Wilk test showed rejection of normality for the quantitative variables, indicating the use of a non-parametric test. Verification of association in the dengue and non-dengue groups used the Mann-Whitney non-parametric test and Pearson’s chi-square test for quantitative and qualitative variables, respectively.
To assess the performance of the index test, dengue NS1 ICT, in each setting using whole blood at point of care (POC) and serum in the laboratory in readings at 15′ and 30′, compared to the standard reference, the following measures of accuracy were considered: sensitivity (Sn), specificity (Sp), positive and negative predictive values (PPV, NPV), and positive and negative likelihood ratios (LR+) and (LR-) with the respective 95% confidence intervals (95% CI). Post-test probabilities were calculated for scenarios with prevalence rates of 30%, 50%, and 83.3%, using the Fagan nomogram [28].
The sensitivity and specificity of the index test in different settings were compared for using the χ2 McNemar test [29].
Reliability was assessed by the variability of the ICT results in whole blood/POC and serum/laboratory with readings at 15 min. Inter-observer reliability was analyzed by the readings done by the two professionals (nurse and biologist) and intra-observer reliability by the same professional (nurse), in blinded fashion. The proportions of positive agreement (Ppos) and negative agreement (Pneg) were calculated, as well as simple and prevalence-adjusted bias-adjusted kappa (PABAK) coefficients with respective 95% CI [30]. Kappa values (k) were interpreted according to the classification by Landis & Koch [31]: poor (k < 0.0), slight (0.0 < k < 0.2), fair (0.2 < k < 0.4), moderate (0.4 < k < 0.6), substantial (0.6 < k < 0.8), almost perfect (0.8 < k < 1.00), and perfect agreement (k = 1).
Statistical significance was set at p < 0.05.
The software packages used were R Commander 3.2.1, WinPepi 11.50, and MedCalc 15.8 [32–34].
Results
Of 148 patients recruited, four were excluded due to five or more days of fever (Fig. 1). Of the 144 patients included, 52.8% were women. Patients’ median age was 34.5 years, with higher ages in the dengue group (median: 36.1 years, ranging from 18 to 82.4) than in the non-dengue group (median: 27 years, ranging from 18.8 to 62.9), p = 0.019.
Fig. 1.
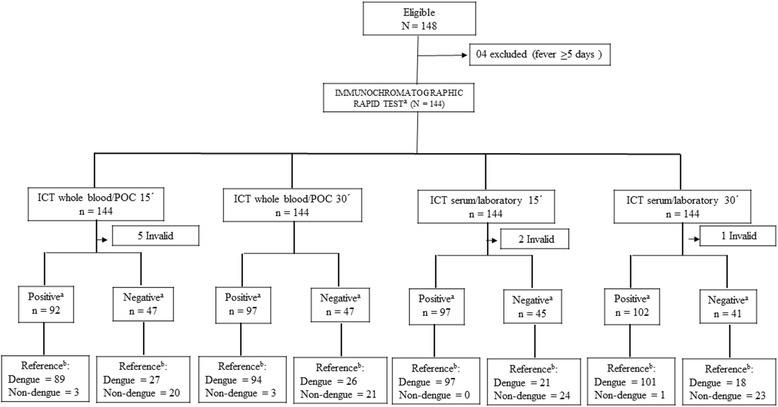
Sample selection and laboratory analysis of 144 suspected dengue cases during a DENV-1 epidemic. a: rapid immunocromatographic test (index test), b: RT-PCR or ELISA NS1 positive (reference test)
Patients presented a median of 1.4 days of fever (95% IQR: 1–2), and the most frequent symptoms were myalgia (91%), headache (89.6%), asthenia (83.3%), and arthralgia (73%). None of the patients evidenced clinical severity signs according to WHO 2009 criteria [4].
Prevalence of the disease was 83.3%. Of the 120 positive cases, 40.3% (n = 58) were primary infections. The dengue virus was characterized by RT-PCR in 105 samples and 15 exclusively by NS1 ELISA. Four samples that were negative for dengue by RT-PCR and NS1 ELISA were positive for Zika virus. One Zika Positive sample tested positive in IgM ELISA.
For all the five invalid cases on readings performed at 15 min in whole blood at POC, readings repeated at 30 min tested positive. For two serum samples at the laboratory showing invalid readings at 15 min, one turned positive at 30 min and the other remained invalid (Fig. 1).
ICT performance was similar in the two settings independently of reading times, both in the point estimate and 95% CI. Sensitivity of ICT with the 15-min reading varied from 76.7% in whole blood at point of care to 82.2% in serum in the laboratory. For the 30-min reading, sensitivity was 78.3% using whole blood at point of care and 84.9% in serum in the laboratory (Table 1). Specificity at 15-was 87% for whole blood at point of care and 100% for serum at the laboratory. For 30-min readings, specificity was 87.5% for whole blood at point of care and 95.8% for serum in the laboratory.
Table 1.
Accuracy of Bioeasy™ rapid immunochromatographic test at point of care and in the laboratory
| Readings at 15’ | Readings at 30’ | |||
|---|---|---|---|---|
| Whole blood/POCa | Serum/Laboratoryb | Whole blood/POCa | Serum/Laboratoryb | |
| Sensitivity | 76.7%c | 82.2%c | 78.3%c | 84.9%c |
| (95%CI) | (68.0–84.1) | (74.1–88.6) | (69.9–85.3) | (77.2–90.8) |
| Specificity | 87.0%d | 100.0%d | 87.5%d | 95.8%d |
| (95% CI) | (66.4–97.2) | (85.8–100.0) | (67.6–97.3) | (78.9–99.9) |
| PPV | 96.7% | 100.0% | 96.9% | 99.0% |
| (95%CI) | (90.8–99.3) | (96.3% - 100.0) | (91.2–99.4) | (95.4–99.8) |
| NPV | 42.6% | 53.3% | 44.7% | 56.1% |
| (95%CI) | (28.3–57.8) | (37.9–68.3) | (30.2–59.9) | (39.8–71.5) |
| LR+ | 5.9 | 19.8e | 6.27 | 20.4 |
| (95%CI) | (2.0–17.0) | (2.9–135.1) | (2.2–18.1) | (3.0–139.0) |
| LR- | 0.27 | 0.18 | 0.25 | 0.16 |
| (95%CI) | (0.19–0.39) | (0.12–0.26) | (0.17–0.36) | (0.10–0.24) |
POC point of care, 95% CI 95% confidence interval, PPV positive predictive value, NPV negative predictive value, LR+ positive likelihood ratio, LR- negative likelihood ratio
aPerformed with whole blood
bPerformed with serum
cP-value <0.01
dP-value >0.05 of χ2 McNemar test
eLR+ calculated using 97.9% specificity
Positive predictive value was high (Table 1) in the prevalence observed in the study (83.3%). In scenarios with prevalence rates of 30% (72.4% CI: 49.3–87.7) or 50% (86%, 95% CI: 69.3–94.3), the PPV remains high. The negative predictive value would increase to 78.9% (95% CI: 72.3–84.3) with a decrease in prevalence in a scenario with 50% prevalence and to 89.7% (95% CI: 85.9–92.6) in a scenario with 30% prevalence.
The reliability between whole blood/POC and serum/laboratory was almost perfect, when evaluated both by the same observer (k = 0.83 CI: 0.74–0.93) and by different observers (k = 0.81 CI: 0.72–0.92), and remained almost perfect even when adjusted by prevalence bias. However, considering the lower limit of Kappa 95% Confidence Interval, reliability interpretation decreased from almost perfect to substantial both for inter-observer (0.73) and for intra-observer 0.75) (Table 2).
Table 2.
Reliability at 15′ of rapid immunochromatographic test comparing whole blood/POC and serum/laboratory
| Kappa | Ppos | Pneg | PABAK | |
|---|---|---|---|---|
| Inter-observera (n = 135) | 0.81 | 94% | 86.7% | 0.83 |
| (95% CI) | (0.73–0.88) | (90.6–97.3) | (79.6–93.8) | |
| Intra-observerb (n = 137) | 0.82 | 94.2% | 87.6% | 0.84 |
| (95% CI) | (0.75–0.89) | (90.9–97.5) | (80.8–94.5) |
Kappa simple kappa, Ppos positive proportion, Pneg negative proportion, PABAK prevalence-adjusted bias-adjusted kappa, 95% CI confidence interval, n absolute number
ainter-observer: nurse (blood/POC) and biologist (serum/laboratory)
bintra-observer: nurse (blood/POC and serum/laboratory)
Discussion
This study assessed the Bioeasy™ rapid immunochromatographic test for DENV-1 NS1 antigen in a high-prevalence setting with adults in Rio de Janeiro State, Brazil, and found similar performance when testing was compared in whole blood/POC and serum/laboratory.
This was the first study to date comparing the performance of NS1 Bioeasy™ ICT in two scenarios, one in a laboratory setting with professionals trained to perform diagnostic tests and the other in a real-world setting (point of care). The evaluation at POC was conducted in the spontaneous treatment flow in an emergency care unit during an epidemic period, with whole blood samples drawn by different professionals. The accuracy of NS1 Bioeasy™ ICT in whole blood/POC showed sensitivity of 76.7% and specificity of 87% at the 15-minuute reading, similar to that found by Gan et al. [21] for Bioline™ ICT SD with whole blood/POC in a predominantly DENV-2 sample, i.e., Sn = 81.6%, 95% CI: 74.6–87.1 and Sp = 98%, 95% CI: 89.5–99.7.
DENV-1 ICT in serum in the laboratory showed a slight increase in accuracy, i.e., Sn = 82.2% and Sp = 100%. The literature reports variability in sensitivity according to serotype, with better performance in serotypes 1, 2, and 3, varying from 69% [7] to 81.8% [8] in DENV-1, from 62% [7] to 81.8% in DENV-2, and from 61.3% to 81.2% [8] in DENV-3, as compared to variation from 44.5% [23] to 84.8% [8] in DENV-4, so that the tests need to be improved in order to perform independently of serotype.
NS1 ICT manufacturers recommend readings at 15 or 20 min [13, 35]. However, in the current study five cases of whole blood specimens at point of care that were invalid at 15 min turned positive at 30 min, and one of the two invalid results at 15 min with serum in the laboratory turned positive at 30 min. Dussart et al. [8] and Osorio et al. [14] used ICT with serum in the laboratory and also reported improved accuracy at the 30-min reading.
The high number of false-negatives suggests that this ICT should not be used to screen for cases, as recommended even by the manufacturer [13] and Andries et al. [15]. The low number of false-positives and the high likelihood of post-testing in this study suggest that the test could be used for diagnostic confirmation. Robustness of this result is strengthened by the use of composite reference test, comprising PCR Dengue [24] and ELISA Dengue NS1 Platelia. The latter has shown very high specificity (100%) in DENV-1 in a previous study [36].
Inter and intra-observer reliability was almost perfect in this study independently of the type of specimen examined (whole blood or serum), the setting (POC or laboratory), and the level of training of the professionals that performed the test. This result corroborates Gan et al. [21].
Evidence for Zika and Dengue cross reactivity has, so far, been identified for IgM ELISA dengue but not for ELISA NS1 dengue tests [27, 37]. In our study, one of four Zika positive samples showed cross-reactivity with IgM Dengue ELISA, but none cross-react with NS1 ELISA Dengue. Increasingly acute febrile syndromes will demand investigation for several flaviviruses.
A possible limitation to the study was the high prevalence of dengue, but the post-test likelihoods were provided for different prevalence scenarios. The evaluation of a single serotype, DENV-1, may have been a limitation, but it resulted from a consecutive patient sample in an epidemic period. The comparison of whole blood/POC and serum/laboratory precludes other comparisons such as serum/POC and whole blood/laboratory, but it represents the possible routine use in emergency care departments without the necessary infrastructure for processing serum specimens during epidemics.
Considering NS1 Bioeasy™ ICT an ASSURED test [6], these recommendations may be particularly useful at sites without laboratory infrastructure or in hyperendemic scenarios, since they would offer faster turnaround of test results, thus favoring diagnosis in emergencies or remote sites [16].
In health services with some laboratory infrastructure, we recommend the use of NS1 ICT with serum in the laboratory, since it is approximately three times more positive in individuals with dengue than without (LR + = 19.8) when compared to whole blood specimens at point of care (LR + = 5.9). However, in services without laboratory infrastructure or during DEN-V 1 epidemics, we recommend screening according to WHO criteria [4] based on clinical signs followed by NS1 Bioeasy™ ICT in whole blood/POC and reading at 15 min and rereading of invalid results at 30 min.
In addition, investment to improve the performance of these tests in whole blood would allow better diagnostic confirmation, potentially optimizing the flow and efficiency of care and treatment. Training strategies for different levels of health professionals involved in performing and reading the NS1 ICT in whole blood at point of care can guarantee the reliability and adequate implementation in the clinical management of suspected cases.
Conclusions
Bioeasy™ NS1 antigen rapid immunochromatographic test showed a good accuracy during the epidemic of DENV-1, particularly for confirmatory diagnosis. It may be useful at the point of care, with no more than a drop of whole blood, since it is rapid and simple to do by minimal trained health personnel. In this context, Bioeasy™ is relevant for the early diagnosis of dengue, particularly at sites without laboratorial infrastructure and in epidemic or hyperendemic scenarios.
Acknowledgements
The authors wish to thank for field work, Rogério Ferrari, Ana Victória Palagi Viganó, Indiara Firmino Brito and Letícia Borges dos Santos.
Funding
This study was supported by the National Council for Scientific and Technological Development (CNPq) [grant numbers 401,366/2013–8] - Brazilian Network for Technological and Health Assessment (REBRATS), Excellence Program in Clinical Research of the Oswaldo Cruz Foundation (PROEP/PCLIN) [grant numbers N° 402,068/2012–2] and the Foundation for Research Support in the State of Rio de Janeiro (FAPERJ) [grant numbers E-25/110.188/2014]. Fellowship grant from CNPq [grant numbers 311,414/2013–3] and UNESA - Productivity Research to [SRLP] and scholarship from FAPERJ [grant numbers 221,354 E_01/2016] to [VEM].
Availability of data and materials
The datasets analyzed during the current study is available from the corresponding author upon request.
Abbreviations
- ASSURED
Affordable, sensitive, specific, user-friendly, robust, rapid, equipment-free, and deliverable to those who need them
- C
Control line
- CI
Confidence interval
- DALYs
Disability-adjusted life years
- DENV
Dengue virus
- DENV-1
Dengue virus serotype 1
- DENV-2
Dengue virus serotype 2
- DENV-3
Dengue virus serotype 3
- DENV-4
Dengue virus serotype 4
- EDTA
Ethylenediaminetetraacetic acid
- ELISA
Enzyme-linked immunosorbent assay
- ICR
Immunochromatographic rapid test
- IgG
Immunoglobulin G
- IgM
Immunoglobulin M
- Kappa
Simple Kappa
- LR−
Negative likelihood ratio
- LR+
Positive likelihood ratio
- NPV
Negative predictive value
- NS1
Nonstructural protein-1
- PABAK
Prevalence and bias adjusted kappa
- POC
Point of care
- PPV
Positive predictive value
- RT-PCR
Reverse-transcription polymerase chain reaction
- S
Sensitivity
- Sp
Specificity
- STARD
Standards for Reporting of Diagnostic Accuracy Study
- T
Test line
- WHO
World Health Organization
Authors’ contributions
VEM conceived of the study, participated in its design, data collection, recording, carried out rapid immunochromatographic test and coordination and helped to draft the manuscript. SRLP conceived of the study, participated in its design and coordination and helped to draft the manuscript. YHMH and MABS participated in the study design, data analysis and interpretation and helped to draft the manuscript. GMB, LVBF and ACFSRM participated in its design, data collection and recording. CDSR and ASS carried out the immunoassays, viral characterization and writing the manuscript. RVCO participated in the design of the study and performed the statistical analysis. All authors read and approved the final manuscript.
Ethics approval and consent to participate
O estudo foi aprovado pelo Conselho de Revisão Institucional do Instituto de Pesquisa Clínica Evandro Chagas (CAAE 0066.0.009.000-11). Todos os pacientes assinaram o formulário de consentimento livre e esclarecido.
Consentimento para publicação
Não aplicável.
Interesses competitivos
Os autores declaram que não têm interesses concorrentes.
Nota do editor
A Springer Nature permanece neutra em relação a reivindicações jurisdicionais em mapas publicados e afiliações institucionais.
Contributor Information
Verónica Elizabeth Mata, Email: veronica.mata@ini.fiocruz.br.
Sonia Regina Lambert Passos, Email: sonia.lambert@ini.fiocruz.br.
Yara Hahr Marques Hökerberg, Email: yarahahr@ini.fiocruz.br.
Guilherme Miguéis Berardinelli, Email: guilherme.berardinelli@ini.fiocruz.br.
Maria Angelica Borges dos Santos, Email: angelicabsantos@ensp.fiocruz.br.
Levy Vilas Boas Fukuoka, Email: levyf@id.uff.br.
Anna Carolina Fontoura Seixas Rangel Maciel, Email: annacarolinafontoura@gmail.com.
Cintia Damasceno dos Santos Rodrigues, Email: cintia_damasceno7@yahoo.com.br.
Aline da Silva Santos, Email: awvgsantos@gmail.com.
Raquel de Vasconcellos Carvalhaes de Oliveira, Email: raquel.vasconcellos@ini.fiocruz.br.
References
- 1.Guzman MG, Halstead SB, Artsob H, Buchy P, Farrar J, Gubler DJ, et al. Dengue: uma ameaça global contínua. Nat Rev Microbiol. 2010;8(12 Suppl):S7–16. doi: 10.1038/nrmicro2460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Constenla D, Armien B, Arredondo J, Carabali M, Carrasquilla G, Castro R, et al. Custeio de casos de febre de dengue e surtos: recomendações de um grupo de trabalho de dengue de custo nas Américas. Valorar questões regionais de saúde. 2015;8C:80–91. [Google Scholar]
- 3.Shepard DS, Undurradga EA, Halasa YA, Stanaway JD. O fardo econômico global da dengue: uma análise sistemática. Lancet Infect Dis. 2016;16(8):935–41. doi: 10.1016/S1473-3099(16)00146-8. [DOI] [PubMed] [Google Scholar]
- 4.Organização Mundial da Saúde. Dengue - diretrizes para diagnóstico, tratamento, prevenção e controle. Genebra: OMS; 2009. p. 11. Disponível em: http://apps.who.int/iris/bitstream/10665/44188/1/9789241547871_eng.pdf. Accessed 9 Apr 2016
- 5.Goodman C, Faulkner E, Gould C, Karnes E, Smith A, Aguiar C, et ai. O valor da inovação, adoção e difusão de diagnósticos nos cuidados de saúde. O grupo Lewin, inc. Adv Med. 2005; Disponível em: https://dx.advamed.org/sites/dx.advamed.org/files/resource/Lewin%20Value%20of%20Diagnostics%20Report.pdf. Acessado em 15 de dezembro de 2016
- 6.Peeling RW, Mabey D. Testes de ponto de atendimento para diagnosticar infecções no mundo em desenvolvimento. Clin Microbiol Infect. 2010;16(8):1062–9. doi: 10.1111/j.1469-0691.2010.03279.x. [DOI] [PubMed] [Google Scholar]
- 7.Fry SR, Meyer M, Semple MG, Simmons CP, Sekaran SD, Huang JX, et al. A sensibilidade diagnóstica dos ensaios de teste rápido de dengue é significativamente aprimorada usando uma abordagem combinada de teste de antígenos e anticorpos. PLoS Negl Trop Dis. 2011;5(6):e1199. doi: 10.1371/journal.pntd.0001199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dussart P, Petit L, Labeau B, Bremand L, Leduc A, Moua D, et al. Avaliação de dois novos testes comerciais para o diagnóstico de infecção aguda do vírus da dengue usando detecção de antígeno NS1 em soro humano. PLoS Negl Trop Dis. 2008;2(8):e280. doi: 10.1371/journal.pntd.0000280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pok KY, Lai YL, Sng J, Ng LC. Avaliação de ensaios de antigénio não estrutural 1 para o diagnóstico e vigilância da dengue em Singapura. Vector Borne Zoonotic Dis. 2010;10(10):1009–16. doi: 10.1089/vbz.2008.0176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Tricou V, Vu HTT, Quynh NVN, Nguyen CW, Tran CT, Farrar J, et al. Comparação de dois testes rápidos NS1 de dengue para sensibilidade, especificidade e relação com a viremia e respostas de anticorpos. BMC Infect Dis. 2010;10:142. doi: 10.1186/1471-2334-10-142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lima MRQ, Nogueira RMR, Schatzmayr HG, Santos FB. Comparação de três ensaios de captura de antígenos NS1 de dengue comercialmente disponíveis para diagnóstico agudo de dengue no Brasil. PLoS Negl Trop Dis. 2010;4(7):e738. doi: 10.1371/journal.pntd.0000738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ferraz FO, Bomfim MRQ, Totola AH, Ávila TV, Cisalpino D, Pessanha JEM, et al. Avaliação de testes laboratoriais para diagnóstico de dengue em espécimes clínicos de pacientes consecutivos com suspeita de dengue em Belo Horizonte, Brasil. J Clin Virol. 2013;58:41–6. doi: 10.1016/j.jcv.2013.06.015. [DOI] [PubMed] [Google Scholar]
- 13.Dengue Eden Test Bioeasy®. Coréia: Bioeasy Diagnóstica Ltda. 2015. Disponível em: http://www.masterdiagnostica.com.br/public/files/produtos/139421463113942146313263116009.pdf. Acessado em 6 de maio de 2017.
- 14.Osorio L, Ramirez M, Bonelo A, Villar LA, Parra B. Comparação da precisão diagnóstica de testes diagnósticos comerciais baseados em NS1 para infecção precoce por dengue. Virol J. 2010;7:361. doi: 10.1186/1743-422X-7-361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Andries AC, Duong V, Ngan C, Ong S, Huy R, Sroin KK, et al. Avaliação de campo e impacto no gerenciamento clínico de um kit de diagnóstico rápido que detecta dengue NS1, IgM e IgG. PLoS Negl Trop Dis. 2012;6(12):e1993. doi: 10.1371/journal.pntd.0001993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Pai NP, Vadnais C, Denkinger C, Engel N, Pai M. Teste de pontos de atendimento para doenças infecciosas: diversidade, complexidade e barreiras nos países de baixa e média renda. PLoS Med. 2012;9(9):e1001306. doi: 10.1371/journal.pmed.1001306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ty Hang V, Minh Nguyet N, The Trung D. Tricou V, Yoksan S, Dung NM, et al. Precisão diagnóstica do NS1 ELISA e testes rápidos de fluxo lateral para sensibilidade à dengue, especificidade e relação com Viremia e respostas de anticorpos. PLoS Negl Trop Dis. 2009;3(1):e360. doi: 10.1371/journal.pntd.0000360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Palamountain KM, Baker J, Cowan LP, Essajee S, Mazzola LT, Metzler M, et al. Perspectivas sobre a introdução e implementação de novos testes diagnósticos de ponto de atendimento. J Infect Dis. 2012;205(Suplemento 2):S181-90. [DOI] [PMC free article] [PubMed]
- 19.Martínez-Veja RA, Diaz-Quijano FA, Coronel-Ruiz C, Gómez SY, Villar-Centeno LA. Avaliação da utilidade da prova rápida de casete por imunocromatografia para diagnóstico de dengue em una região endémica colombiana. Biomedica. 2009;29:616–24. doi: 10.7705/biomedica.v29i4.139. [DOI] [PubMed] [Google Scholar]
- 20.Hunsperger EA, Yoksan S, Buchy P, Nguyem VC, Sekaran SD, Enria DA, et al. Avaliação de testes diagnósticos comercialmente disponíveis para a detecção do anticorpo anti-dengue NS1 do vírus da dengue e anti-IgG anti-dengue. PLoS Negl Trop Dis. 2014;8(10):e3171. doi: 10.1371/journal.pntd.0003171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Gan VC, Tan LK, Lye DC, Pok KY, Mok SQ, Chua RC-R, et al. Diagnóstico da dengue no ponto de atendimento: utilidade de um kit de diagnóstico combinado rápido em Cingapura. PLoS One. 2014;9(3):e90037. doi: 10.1371/journal.pone.0090037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Korevaar DA, Wang J, van Enst WA, Leeflang MM, Hooft L, Smidt N, et al. Relatórios de estudos de precisão diagnóstica: algumas melhorias após 10 anos de STARD. Radiologia. 2015;274:781–9. doi: 10.1148/radiol.14141160. [DOI] [PubMed] [Google Scholar]
- 23.Buonora SN, Passos SRL, do Carmo CN, Quintela FM, DNR d O, dos Santos FB, et al. Precisão de critérios clínicos e teste de tira imunocromatográfica para diagnóstico de dengue em uma epidemia de DENV-4. BMC Infect Dis. 2016;16:37. [DOI] [PMC free article] [PubMed]
- 24.Lanciotti RS, Calisher CH, Gubler DJ, Chang GJ, Vorndam AV. Rápida detecção e digitação de vírus da dengue a partir de amostras clínicas usando a reação em cadeia da polimerase de transcriptase reversa. J Clin Microbiol. 1992;30(3):545-51. [DOI] [PMC free article] [PubMed]
- 25.Platelia ™ Dengue NS1 AG®. França: Bio-Rad Laboratories, Inc .. 2008. Disponível em: http://www.biorad.com/webroot/web/pdf/inserts/CDG/en/72830_881149_EN.pdf. Acessado em 6 de maio de 2017.
- 26.Serion Elisa Classic Dengue Virus IgG / IgM Virion \ Serion®. Alemanha: Institut Virion \ Serion GmbH. 2012. Disponível em: http://www.virion-serion.de/download/flyer/Flyer_ELISA_classic_Dengue_Virus_EN.pdf. Acessado em 6 de maio de 2017.
- 27.Lanciotti RS, Kosoy OL, Laven JJ, Velez JO, Lambert AJ, Johnson AJ, et al. Propriedades genéticas e sorológicas do vírus Zika associado a uma epidemia, estado da Micronesia, 2007. Emerg Infect Dis. 2008;14(8):1232–9. doi: 10.3201/eid1408.080287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Fagan TJ. Nomograma para o teorema de Bayes [carta] N Engl J Med. 1975;293(5):257. doi: 10.1056/NEJM197507312930513. [DOI] [PubMed] [Google Scholar]
- 29.Trajman A, Luiz RR. Teste McNemar χ2 revisitado: comparação da sensibilidade e especificidade dos exames diagnósticos. Scand J Clin Lab Invest. 2007;68(1):77–80. doi: 10.1080/00365510701666031. [DOI] [PubMed] [Google Scholar]
- 30.Byrt T, Bispo J, Carlin JB. Bias, prevalência e kappa. J Clin Epidemiol. 1993;46(5):423–429. doi: 10.1016/0895-4356(93)90018-V. [DOI] [PubMed] [Google Scholar]
- 31.Landis JR, Koch GG. A medida do acordo observador para dados categóricos. Biometria. 1977;33:159–74. doi: 10.2307/2529310. [DOI] [Google Scholar]
- 32.R Core Team . R: um idioma e ambiente para computação estatística. Viena: Fundação R para Computação Estatística; 2015. [Google Scholar]
- 33.Abramson JH. WINPEPI atualizado: programas informáticos para epidemiologistas e seu potencial de ensino. Epidemiol Perspect Innov. 2011;8:1. doi: 10.1186/1742-5573-8-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.MedCalc Statistical Software versão 12.7.8. (MedCalc Software bvba, Ostend; 2014. Disponível em https://www.medcalc.org. Accessed 8 Feb 2017.
- 35.IVB Dengue Ag NS1 OrangeLife®. Brasil: Orangelife comércio e indústria Ltda. 2016. Disponível em: http://www.dmed.com.br/manuais/denguens1orangelife.pdf. Acessado em 7 de janeiro de 2016.
- 36.Pal S, Dauner AL, Mitra I, Forshey BM, Garcia P, Morrison AC, Halsey ES, Kochel TJ, Wu SJ. Avaliação de testes rápidos de antígeno NS1 da dengue e kits Elisa usando amostras clínicas. PLoS One. 2014;9(11):e113411. doi: 10.1371/journal.pone.0113411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Matheus S, Boukhari R, Labeau B, Ernault V, Bremand L, Kazanji M, Rousset D. Especificidade do antígeno NS1 da dengue no diagnóstico diferencial da infecção do vírus da dengue e da Zika. Emer Infect Dis. 2016;22(9):1691–1692. doi: 10.3201/eid2209.160725. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets analyzed during the current study is available from the corresponding author upon request.