

Abstract
Objective:
To determine the definite and potential frequency of seizures and epilepsy as a cause of death (COD) and how often this goes unrecognized.
Methods:
Prospective determination of seizures or epilepsy and final COD for individuals aged 18–90 years with out-of-hospital sudden cardiac deaths (SCDs) from the population-based San Francisco POST SCD Study. We compared prospective seizure or epilepsy diagnosis and final COD as adjudicated by a multidisciplinary committee (pathologists, electrophysiologists, and a vascular neurologist) vs retrospective adjudication by 2 epileptologists with expertise in seizure-related mortality.
Results:
Of 541 SCDs identified during the 37-month study period (mean age 62.8 years, 69% men), 525 (97%) were autopsied; 39/525 (7.4%) had seizures or epilepsy (mean age: 58 years, range: 27–92; 67% men), comprising 17% of 231 nonarrhythmic sudden deaths. The multidisciplinary team identified 15 cases of epilepsy, 6 sudden unexpected deaths in epilepsy (SUDEPs), and no deaths related to acute symptomatic seizures. The epileptologists identified 25 cases of epilepsy and 8 definite SUDEPs, 10 possible SUDEPs, and 5 potential cases of acute symptomatic seizures as a COD.
Conclusions:
Among the 25 patients identified with epilepsy by the epileptologists, they found definite or possible SUDEP in 72% (18/25) vs 24% (6/25) by the multidisciplinary group (6/15 cases they identified with epilepsy). The epileptologists identified acute symptomatic seizures as a potential COD in 5/14 patients with alcohol-related seizures. Epilepsy is underdiagnosed among decedents. Among patients with seizures and epilepsy who die suddenly, seizures and SUDEP often go unrecognized as a potential or definite COD.
Individuals with epilepsy have increased mortality,1 with sudden death rates among young adults 27-fold higher than control populations.2 Seizures and epilepsy can cause or contribute to death from sudden unexpected death in epilepsy (SUDEP), drowning, pneumonia, status epilepticus, accidents, falls, burns, suicide, and consequences of medical and surgical therapies.1–3
The role of seizures and epilepsy in causing death may be underestimated for many reasons, including (1) failure to obtain a history of seizures or epilepsy in the decedent; (2) a lack of seizure stigmata of seizures (e.g., tongue bite) or nonspecific findings (e.g., urinary incontinence and pulmonary edema) at autopsy; (3) failure to recognize seizures as the ultimate cause of death (COD; e.g., seizures causing lethal aspiration pneumonia); (4) failure to recognize seizures as the proximate COD (e.g., seizure is the terminal event in a patient with malignant brain tumor); (5) structural and toxicological findings (e.g., cardiomegaly and serum cocaine metabolite) are given priority over seizures; and (6) potential arrhythmic causes receive higher priority than epilepsy in “autopsy-negative” sudden deaths. We cannot assess the frequency of seizure-related and epilepsy-related sudden deaths because of these biases and the lack of population-based comprehensive investigation.
The POstmortem Systematic InvesTigation of Sudden Cardiac Death (POST SCD) Study4 systematically evaluated nearly every incident out-of-hospital sudden cardiac death (SCD) in a metropolitan area over a 37-month period, including complete autopsies and review of paramedic run sheets and medical records. We examined the records of all POST SCD cases with a history of seizures or epilepsy to independently assess CODs.
METHODS
From February 2011 to March 2014, through active and real-time surveillance of all cases referred to the medical examiner, the POST SCD Study identified all incident SCDs aged 18–90 years within the City and County of San Francisco.4 California law mandates reporting all out-of-hospital deaths to the medical examiner.5 The following sudden deaths were excluded: patients with (1) severe noncardiac chronic and terminal illness, including (a) terminal cancer or (b) end-stage renal disease on dialysis; (2) hospice residents; and (3) an identifiable noncardiac etiology at the time of presentation: (a) signs of drug abuse/overdose (IV needles and empty pill bottles), (b) trauma, (c) violent death, (d) homicide, and (e) suicide. All cases underwent systematic and comprehensive evaluation, including retrieval and review of medical records and full autopsy with detailed heart and cranial vault examination. A multidisciplinary committee of cardiologists and cardiac electrophysiologists, anatomic and forensic pathologists, and a vascular neurologist (in selected cases) adjudicated a single most likely COD for each case by a consensus. For cases with a history of seizures or epilepsy, data were independently reviewed by 2 epileptologists (D.F. and O.D.) with expertise in epilepsy-related mortality. SUDEP was determined using the criteria of Nashef et al.6 Definite SUDEP was a sudden death in benign circumstances (excluding status epilepticus) in a person with epilepsy without an alternative COD on postmortem examination. Definite SUDEP plus was a sudden death in a person with epilepsy and a concomitant condition by history or on autopsy that could have contributed to but was unlikely to be solely responsible for death. Possible SUDEP was a sudden death in a person with epilepsy in which there was a competing cause that may have been solely responsible for death. A case was determined not to be SUDEP if there was a clear alternative COD based on history, postmortem examination, or toxicology. Not all individuals with a history of seizures have epilepsy, defined as ≥2 unprovoked seizures at least 24 hours apart or a single unprovoked seizure with an enduring risk for further seizures. Medical record documentation of seizure history and antiepileptic drug use varied among study participants. We defined epilepsy as definite or probable using the International League Against Epilepsy criteria for epidemiologic and surveillance studies of epilepsy.7
Standard protocol approvals, registrations, and patient consents.
This study was approved by the local institutional review board with a waiver of informed consent.
Statistical analysis.
Statistical analyses were performed with Stata (StataCorp LP, College Park, TX), using the Student t test assuming unequal variance for continuous data, and the Fisher exact test for categorical data, where appropriate. A 2-tailed p < 0.05 was considered statistically significant.
RESULTS
Of 541 consecutive SCDs identified during the 37-month study period, 525 (97%) underwent systematic evaluation and full autopsy (figure). Of these cases, 39 (7.2% of all SCDs and 7.4% of autopsied SCDs) had a history of seizures. The POST SCD team identified epilepsy in 15/39 (38.5%); the epileptologists diagnosed probable or definite epilepsy in 25/39 (64%) cases (table 1 and figure). The major findings that led the epileptologists to diagnose probable or definite epilepsy in these 10 additional cases included clinical history (10) and current or prior use of one or more antiepileptic drugs (7). The POST SCD committee identified 6 definite SUDEP cases. Of the remaining 9 patients, COD was attributed to 7 cardiac causes (2 hypertrophy, 2 cardiomyopathy, 1 chronic coronary artery disease [CAD], 1 acute CAD, and 1 heart failure) and 2 noncardiac causes (1 intracranial hemorrhage and 1 incarcerated hernia) (table 2 and table e-1 at Neurology.org).
Figure. Flow chart of adjudications by the POST SCD team and epileptologists.

SUDEP = sudden unexpected death in epilepsy.
Table 1.
Determination of COD
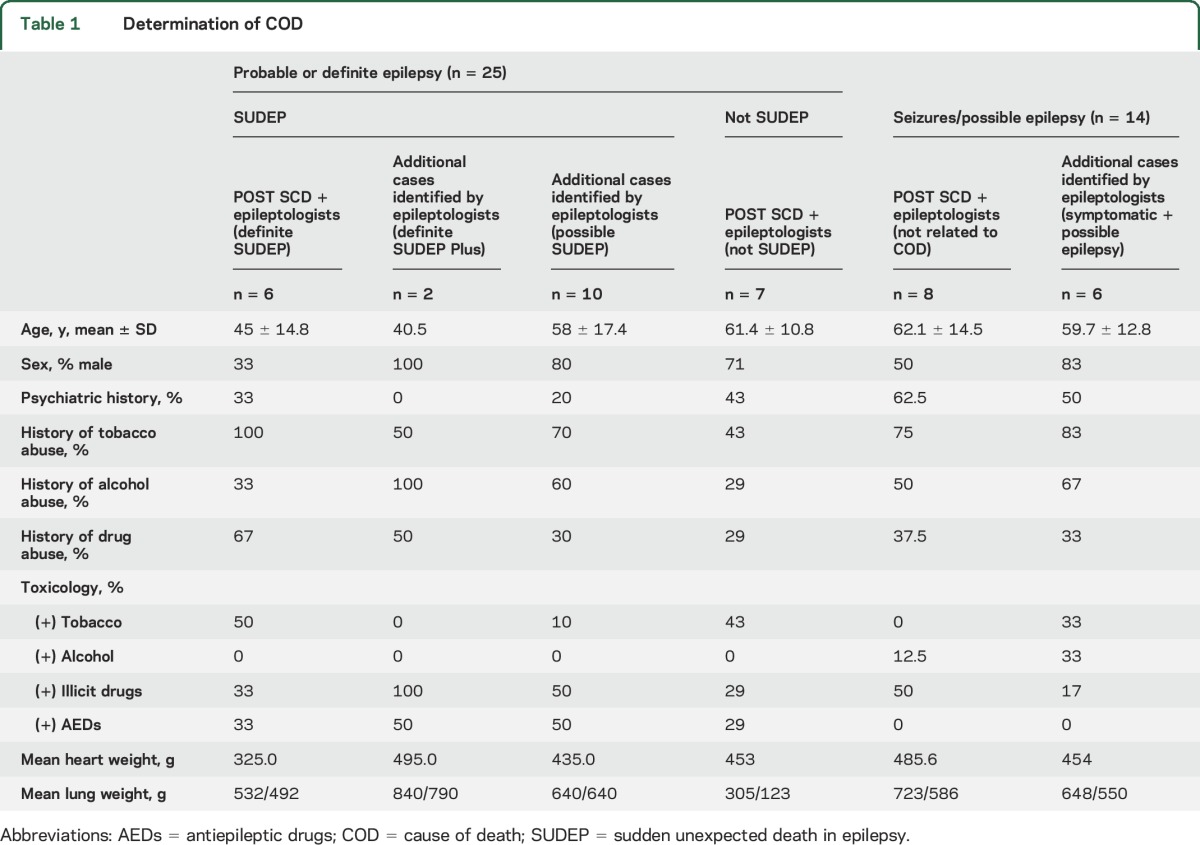
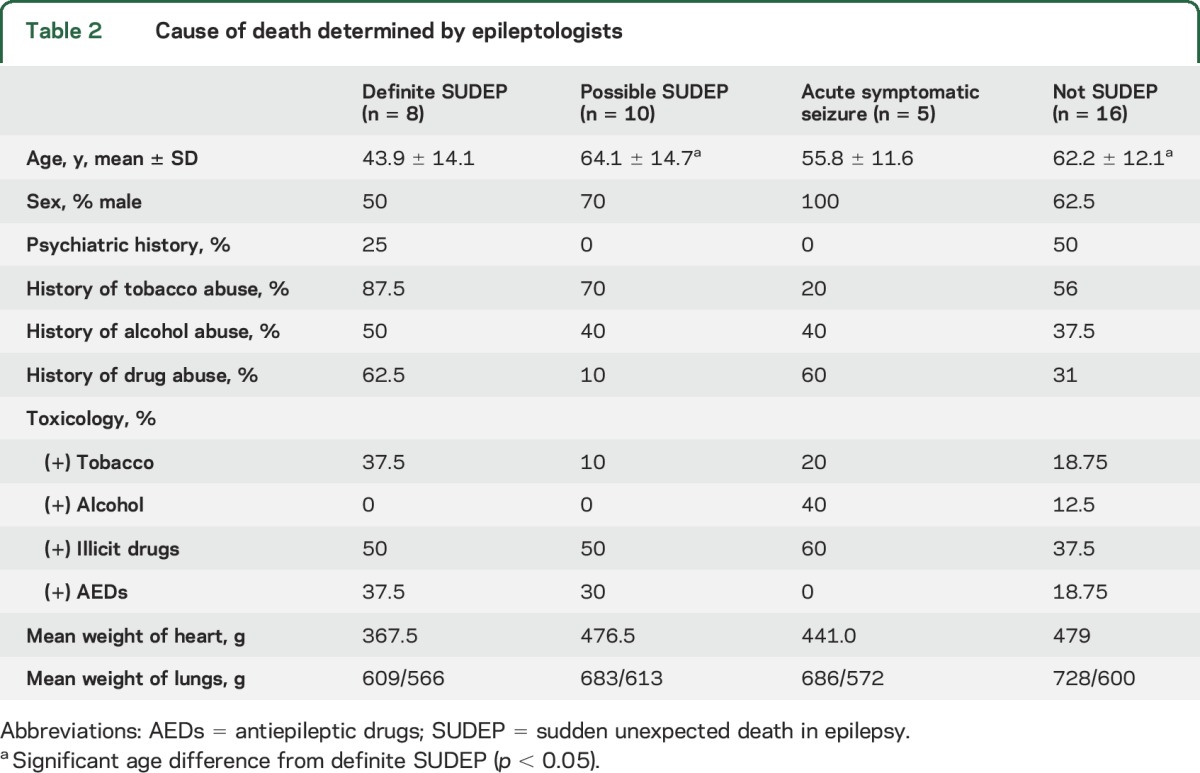
Table 2.
Cause of death determined by epileptologists
Among the 6 SUDEPs identified by the POST SCD team, 3 had nonspecific cardiac findings (minor thickening of septal and posterior left ventricle and interstitial fibrosis). One SUDEP case (17%) was asystolic and apneic when emergency medical services arrived. Two SUDEP cases were young women with juvenile myoclonic epilepsy, including one who recently stopped taking antiseizure medications. SUDEP cases were younger than other SCDs (mean age 45; SD 14.8; range 27–67; p = 0.001).
The epileptologists classified the COD in the 25 epilepsy cases they identified as follows: definite SUDEPs (6; same as POST SCD team), definite SUDEP plus (2), possible SUDEP (10), and not SUDEP (7). For the 2 definite SUDEP plus cases, the POST SCD team determined COD as cardiac hypertensive heart disease and cardiomyopathy. One was a 52-year-old man found prone on a pavement in front of a park bench where he was observed reading, in no distress, 2 hours earlier. This 75-inch, 236 pound man's heart weighed 560 g, and his lungs weighed 1,750 g. He had a history of epilepsy after a motorcycle accident requiring a craniotomy and was on phenytoin (none detected postmortem). His coronary arteries were normal; there was moderate thickening of his mitral valve and subendocardial fibrosis. The second was a 29-year-old man with nocturnal convulsions on carbamazepine (postmortem level 3.7). He had 2 convulsions in the past 6 months. He was found prone in bed and his face in the pillow. This 71-inch, 170-pound man's heart weighed 430 g, and there was subendocardial fibrosis; his lungs weighed 1,510 g (consistent with pulmonary edema). The coronary arteries and cardiac valves were normal. Subendocardial fibrosis and pulmonary edema are common findings in SUDEP8,9 and could have contributed to the mechanism of death. This case could also be considered a definite SUDEP.
For the 10 possible SUDEP cases, the POST SCD team's diagnoses were incarcerated hernia without perforation or sepsis (1), cardiac (7: acute CAD [1], chronic cardiac artery disease [1], cardiomyopathy [3], and hypertensive heart disease [2]), and chemical overdose (2). In these 10 cases, the epileptologists considered the COD as uncertain because SUDEP and the cause listed by the POST SCD team were both possible, and the evidence did not establish a probable cause. For example, a 51-year-old man with acute coronary artery changes (plaque rupture) was witnessed by his wife to have 2 convulsive seizures, 30 minutes apart, out of sleep. He stopped breathing within several minutes of the second convulsion and died, despite resuscitative efforts initiated by emergency medical services 10 minutes later. He had been seizure free for 10 years and was not taking antiseizure medication. The ruptured coronary artery plaque may have resulted from the seizures or potentially triggered cerebral ischemia that provoked the seizures; death may have been primarily due to cardiac ischemia, SUDEP, or a combination of both. In the 2 cases of chemical overdose, one had subtherapeutic valproic acid levels as well as the cocaine metabolite benzoylecgonine (0.17 mg/L) and morphine (0.14 mg/L). However, the average benzoylecgonine levels in cocaine-related sudden deaths are 3.26 mg/L10 and average morphine levels are 0.26 mg/L.11 The other overdose had an oxazepam level of 7 ng/mL, nordiazepam of 344 ng/mL, diazepam of 270 ng/mL, morphine of 0.36 mg/mL, and pseudoephedrine of 760 ng/mL. Low doses (15 mg) of oxazepam produce peak blood levels of 300 ng/mL,12 and living drug users with positive tests have an average level of 1,013 ng/mL.13 Standard pseudoephedrine doses produce peak levels of ∼450 ng/mL.14 Given the individuals' history of drug abuse, they were likely tolerant to opiates or benzodiazepines, and the relationship of the drug use to death is possible but uncertain, similar to SUDEP. A comparison of cases for which there was agreement and disagreement by POST SCD and epileptologist reviewers is summarized in table 1 and table e-1.
Among the other 14 cases with a history of seizures but not epilepsy, acute symptomatic seizures were considered as possible causes or contributing causes of death in 5 patients.
Demographic and historical features in the definite SUDEP, possible SUDEP, and acute symptomatic seizure groups are summarized in table 2. The mean age of the definite SUDEP group was younger than that classified as possible or not SUDEP. The acute symptomatic seizure group was composed entirely of men, whereas the other groups were composed of 50%–70% men.
DISCUSSION
Our study reveals that despite the most rigorous procedures to obtain medical records and perform comprehensive autopsy and adjudicate COD among an entire metropolitan population with epilepsy who die suddenly, the potential role of SUDEP went unrecognized in 12/18 cases (67%). Among 25 epilepsy cases, 6 were diagnosed with SUDEP, whereas 2 definite SUDEP plus and 10 possible SUDEP diagnoses were missed. Thus, there are major limitations in determining the COD among people with seizures and epilepsy. Without the systematic medical record review and comprehensive autopsy and adjudication performed by the POST SCD team, the history of epilepsy and seizures would have been missed in many cases and the underestimation of SUDEP incidence would be even lower. Furthermore, despite attempts by study investigators to obtain medical records, these records may have been limited, suggesting that additional cases of epilepsy and SUDEP may have been missed.
The potential contribution of seizures and epilepsy to sudden death is often overlooked. There were marked differences in the adjudications of the POST SCD multidisciplinary committee (cardiologists, anatomic and forensic pathologists, and a stroke neurologist) and 2 epileptologists with expertise in seizure-related mortality who separately reviewed cases with a history of seizures or epilepsy. The differences likely reflect uncertainties in diagnosing epilepsy with a limited history and determining COD when there is no definite structural or toxicological cause, the decision to choose a single COD, the choice to use positive (i.e., presence of a potentially lethal structural or toxicological cause) over negative (lack of alternative etiology supports SUDEP) findings, as well as the biases of different disciplines and perspectives. Because we have captured the entire population of sudden deaths with seizure history in the metropolitan area, our study may be more generalizable for out-of-hospital sudden death risk than prior studies of selected hospitalized patients with epilepsy.
The underrecognition of SUDEP is widespread among coroner and medical examiner communities. In 1 survey, 83.5% of pathologists acknowledged that SUDEP is a valid diagnosis if autopsy revealed no alternative COD in a person with epilepsy, but only 22.9% of these pathologists diagnosed SUDEP in more than half of the cases that met the criteria.15 Another review of epilepsy cases from a medical examiner office found that nearly all the Definite SUDEP Plus cases went unrecognized, with COD most often attributed to heart disease, alcoholism, or metabolic disorder.16 Seizure or epilepsy was listed as a COD or contributing factor in only 1/12 of these deaths.16 In our study, the role of epilepsy was not identified in either of the 2 definite SUDEP Plus cases. In our series and that by Atherton et al.,16 definite SUDEP plus composed 25%–48% of all definite SUDEP cases. Failure to recognize this category has profound implications on the epidemiology of SUDEP.
Underrecognition of SUDEP often results from the priority given to postmortem findings, the gold standard to determine COD. However, interpretation of postmortem findings varies widely and determining COD often requires judgment and uncertainty. Errors in determining COD can occur from systematic errors (e.g., assuming an antemortem diagnosis without corroborative data),17 limited sampling that biases against certain etiologies,18 greater weight to structural or toxicological than functional causes, or applying population-based probabilities (i.e., cardiovascular disease) in autopsy-negative or nonlethal pathologic findings in specific populations (e.g., epilepsy).
It is challenging to determine the probability that one or more gross or histopathologic abnormalities are the COD or whether they are artifactual. For example, coronary artery atherosclerosis without end-organ damage, mitral valve prolapse, and cardiomegaly are prevalent in the general population,19 and some cardiac abnormalities are more common in obese individuals.20 The comprehensive postmortem methods in POST SCD likely identified abnormalities that would usually be missed (e.g., myocardial fibrosis in a grossly normal heart found on sections of 5 left ventricle areas) and determined a cardiac COD rather than SUDEP, contributing to the underestimation of seizure or epilepsy as a COD.
Postmortem interpretation of toxicology is complex. Drug concentrations are affected by the environment and condition of the body, transport, storage, time to autopsy, collection site, and postmortem redistribution.21 Although reference ranges help to distinguish therapeutic from toxic levels, the aforementioned factors and tolerance in individuals with chronic exposure complicate interpretation.22–24
Biases toward selected diagnoses also affect determination of COD. A common definition of SCD is a sudden and unexpected death within an hour of symptom onset,25,26 but if unwitnessed, individuals should have been observed alive within 24 hours of death.27 This broad definition presumes sudden arrhythmic death syndrome (SADS) with no history, nor macroscopic or microscopic evidence of cardiac disease in individuals who die suddenly.28 In the POST SCD Study, just over half of all SCDs were SADS after postmortem investigation, including the unexpected large contribution of sudden neurologic deaths masquerading as sudden cardiac deaths.29
The need to identify a primary COD forces medical examiners and coroners to make probabilistic determinations. The COD is often uncertain, with multiple competing causes for whom relative probabilities are difficult to determine. When a thorough autopsy and toxicological study fails to reveal a COD in a person with epilepsy, cardiac etiologies are often presumed.15 An autopsy is performed in 8.5% of deaths in the United States; for many without autopsy, the COD on death certificates is unreliable.30 For example, intellectual disability (mental retardation) is often erroneously listed as the COD.31 In many cases, the clinical, pathologic, and toxicologic data do not clearly establish a COD. Identification of clinical risk factors (e.g., hypertension and hypercholesterolemia) and pathologic findings of uncertain significance (e.g., cardiomegaly) often lead to liberal interpretation, exclusion of contributory diagnoses, and biases toward prevalent diseases. Thus, if a person with epilepsy dies suddenly, an alternative COD can be readily supported by circumstantial evidence, although the diagnosis of possible SUDEP specifically allows for a competing COD.
Seizures of any cause, not just epilepsy, increase the risk of sudden death.32 A febrile seizure history is 10-fold more common among toddlers who die suddenly and for whom no COD is found after complete forensic examination than in the general pediatric population.33 Other forms of acute seizures, such as alcohol withdrawal and drug-induced seizures, can cause sudden death.34
There are potential biases of the epileptologists as well, whose expertise is more restricted and who lack training in forensic pathology. They may have selectively reviewed deaths among patients with seizures and epilepsy focusing on potential seizure-related factors. They agreed that the chance of SUDEP must be 10% or higher to be considered a possible SUDEP, although no percent probability is provided in the current criteria. Furthermore, they acknowledge that it is impossible to accurately quantify the probability that death was due to SUDEP or a seizure, especially when competing causes are present.
Our findings confirm that there is often uncertainty in the degree to which seizures contribute to sudden death, especially in older individuals, people with comorbid medical conditions, and those with a history of substance abuse. This uncertainty may influence estimates of epilepsy-related mortality and be substantially but not entirely improved by increasing autopsy rates because forensic science cannot always distinguish between competing COD. Studies of the pathophysiology of SUDEP may reveal genetic and molecular signatures of seizure-related death that can be probed to improve certainty in death certification and may help better define the scope of the problem.
Supplementary Material
GLOSSARY
- CAD
coronary artery disease
- COD
cause of death
- SADS
sudden arrhythmic death syndrome
- SCD
sudden cardiac death
- SUDEP
sudden unexpected death in epilepsy
Footnotes
Supplemental data at Neurology.org
Editorial, page 878
AUTHOR CONTRIBUTIONS
Orrin Devinsky and Daniel Friedman contributed to study conception and design, analysis and interpretation of data, and critical revision of the manuscript. Jocelyn Y. Cheng contributed to analysis of data and critical revision of the manuscript. Anthony Kim contributed to study conception and design, acquisition of data, drafting the manuscript, analysis and interpretation of data, and critical revision of the manuscript. Ellen Moffatt contributed to acquisition of data and critical revision of the manuscript. Zian H. Tseng contributed to acquisition of study funding, study conception and design, acquisition of data, analysis and interpretation of data, and critical revision of the manuscript.
STUDY FUNDING
This study was funded by NIH R01 HL102090 (NHLBI) and UCSF-CTSI UL1 TR000004 (NCATS).
DISCLOSURE
O. Devinsky is the Principal Investigator of the North American SUDEP Registry, during the conduct of the study. D. Friedman is on the executive board of the North American SUDEP Registry; he also receives salary support from the Epilepsy Study Consortium, research support from UCB, Inc., and consulting fees from LivaNova, GW Pharma, and UCB, Inc., outside the submitted work. J.Y. Cheng receives consulting fees from Medscape and LLC, outside the submitted work. E. Moffatt reports no disclosures relevant to the manuscript. A. Kim reports grants from NIH/NCATS during the conduct of the study and research grants from SanBio and Biogen outside the submitted work and receives compensation as a DSMB member for a clinical trial sponsored by Neuravi. Z.H. Tseng reports grants from NIH/NHLBI during the conduct of the study and personal fees from Biotronik, outside the submitted work. Go to Neurology.org for full disclosures.
REFERENCES
- 1.Devinsky O, Hesdorffer DC, Thurman DJ, et al. Sudden unexpected death in epilepsy: epidemiology, mechanisms, and prevention. Lancet Neurol 2016;7:1075–1088. [DOI] [PubMed] [Google Scholar]
- 2.Holst AG, Winkel BG, Risgaard B, et al. Epilepsy and risk of death and sudden unexpected death in the young: a nationwide study. Epilepsia 2013;54:1613–1620. [DOI] [PubMed] [Google Scholar]
- 3.Sheth SG, Krauss G, Krumholz A, Li G. Mortality in epilepsy: driving fatalities vs other causes of death in patients with epilepsy. Neurology 2004;63:1002–1007. [DOI] [PubMed] [Google Scholar]
- 4.Tseng ZH, Hayward RM, Clark NM, et al. Sudden death in patients with cardiac implantable electronic devices. JAMA Intern Med 2015;175:1342–1350. [DOI] [PubMed] [Google Scholar]
- 5.ARTICLE 2. Inquests [27490–27512]. California Legislative Information website. Available at: leginfo.legislature.ca.gov/faces/codes_displaySection.xhtml?lawCode=GOV§ionNum=27491.&highlight=true&keyword=coroner. Accessed September 27, 2016. [Google Scholar]
- 6.Nashef L, So EL, Ryvlin P, Tomson T. Unifying the definitions of sudden unexpected death in epilepsy. Epilepsia 2012;53:227–233. [DOI] [PubMed] [Google Scholar]
- 7.Fisher RS, Acevedo C, Arzimanoglou A, et al. A practical definition of epilepsy. Epilepsia 2014;55:475–482. [DOI] [PubMed] [Google Scholar]
- 8.Stollberger C, Finsterer J. Cardiorespiratory findings in sudden unexplained unexpected death in epilepsy (SUDEP). Epilepsy Res 2004;59:51–60. [DOI] [PubMed] [Google Scholar]
- 9.So EL. What is known about the mechanisms underlying SUDEP? Epilepsia 2008;49(suppl 9):93–98. [DOI] [PubMed] [Google Scholar]
- 10.Pilgrim JL, Woodford N, Drummer OH. Cocaine in sudden and unexpected death: a review of 49 post-mortem cases. Forensic Sci Int 2013;227:52–59. [DOI] [PubMed] [Google Scholar]
- 11.Minett WJ, Moore TL, Juhascik MP, et al. Concentrations of opiates and psychotropic agents in polydrug overdoses: a surprising correlation between morphine and antidepressants. J Forensic Sci 2010;55:1319–1325. [DOI] [PubMed] [Google Scholar]
- 12.Smink BE, Hofman BJ, Dijkhuizen A, et al. The concentration of oxazepam and oxazepam glucuronide in oral fluid, blood and serum after controlled administration of 15 and 30 mg oxazepam. Br J Clin Pharmacol 2008;66:556–560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Burch HJ, Clarke EJ, Hubbard AM, Scott-Ham M. Concentrations of drugs determined in blood samples collected from suspected drugged drivers in England and Wales. J Forensic Leg Med 2013;20:278–289. [DOI] [PubMed] [Google Scholar]
- 14.Mojaverian P, Rosen J, Vadino WA, Liebowitz S, Radwanski E. In-vivo/in-vitro correlation of four extended release formulations of pseudoephedrine sulfate. J Pharm Biomed Anal 1997;15:439–445. [DOI] [PubMed] [Google Scholar]
- 15.Schraeder PL, Delin K, McClelland RL, So EL. Coroner and medical examiner documentation of sudden unexplained deaths in epilepsy. Epilepsy Res 2006;68:137–143. [DOI] [PubMed] [Google Scholar]
- 16.Atherton DS, Devinsky O, Hesdorffer DC, et al. Implications of death certification on sudden death in epilepsy (SUDEP) research. Acad Forensic Pathol 2016;6:96–102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Krishna V, Tan-Figueroa L, Lohiya GS. Errors in autopsy of a patient with ventricular septal defect and tuberous sclerosis. Med Sci Law 2010;50:54. [DOI] [PubMed] [Google Scholar]
- 18.Benbow EW, Roberts ISD. The autopsy: complete or not complete? Histopathology 2003;42:417–423. [DOI] [PubMed] [Google Scholar]
- 19.Papadakis M, Raju H, Behr ER, et al. Sudden cardiac death with autopsy findings of uncertain significance: potential for erroneous interpretation. Circ Arrhythm Electrophysiol 2013;6:588–596. [DOI] [PubMed] [Google Scholar]
- 20.Byard RW. The complex spectrum of forensic issues arising from obesity. Forensic Sci Med Pathol 2012;8:402–413. [DOI] [PubMed] [Google Scholar]
- 21.Gerostamoulos D, Beyer J, Staikos V, et al. The effect of the postmortem interval on the redistribution of drugs: a comparison of mortuary admission and autopsy blood specimens. Forensic Sci Med Pathol 2012;8:373–379. [DOI] [PubMed] [Google Scholar]
- 22.Schulz M, Iwersen-Bergmann S, Andresen H, Schmoldt A. Therapeutic and toxic blood concentrations of nearly 1,000 drugs and other xenobiotics. Crit Care 2012;16:R136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Skopp G. Postmortem toxicology. Forensic Sci Med Pathol 2010;6:314–325. [DOI] [PubMed] [Google Scholar]
- 24.Leikin JB, Watson WA. Post-mortem toxicology: what the dead can and cannot tell us. J Toxicol Clin Toxicol 2003;41:47–56. [DOI] [PubMed] [Google Scholar]
- 25.Report of a Working Group on Ischaemic Heart Disease Registers. Parts I and II. Copenhagen: Regional Office for Europe WHO; 1969. Euro 5010. [Google Scholar]
- 26.Myerburg RJ, Castellanos A. Cardiac arrest and sudden cardiac death. In: Zipes DP, Libby P, Bonow RO, Braunwald E, editors. Braunwald's Heart Disease. A Textbook of Cardiovascular Medicine. Philadelphia: Elsevier Saunders; 2005:865–908. [Google Scholar]
- 27.Chugh SS, Reinier K, Teodorescu C, et al. Epidemiology of sudden cardiac death: clinical and research implications. Prog Cardiovasc Dis 2008;51:213–228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Behr ER, Casey A, Sheppard M, et al. Sudden arrhythmic death syndrome: a national survey of sudden unexplained cardiac death. Heart 2007;93:601–605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kim AS, Moffatt E, Ursell PC, et al. Sudden neurologic death masquerading as out-of-hospital sudden cardiac death. Neurology 2016;87:1–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ravakhah K. Death certificates are not reliable: revivification of the autopsy. South Med J 2006;99:728–734. [DOI] [PubMed] [Google Scholar]
- 31.Landes SD, Peek CW. Death by mental retardation? The influence of ambiguity on death certificate coding error for adults with intellectual disability. J Intell Disabil Res 2013;57:1183–1190. [DOI] [PubMed] [Google Scholar]
- 32.Kirby S, Sadler RM. Injury and death as a result of seizures. Epilepsia 1995;36:25–28. [DOI] [PubMed] [Google Scholar]
- 33.Hesdorffer DC, Crandall LA, Friedman D, Devinsky O. Sudden unexplained death in childhood: a comparison of cases with and without a febrile seizure history. Epilepsia 2015;56:1294–1300. [DOI] [PubMed] [Google Scholar]
- 34.Pieninkeroinen IP, Telakivi TM, Hillborn ME. Outcome in subjects with alcohol-provoked seizures. Alcohol Clin Exp Res 1992;16:955–959. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.