

Abstract
Background: The manual stimulation of acupuncture points has been combined with components of cognitive and exposure therapies into a clinical and self-help approach known as Emotional Freedom Techniques (EFT). More than 40 clinical trials and four meta-analytic reviews of EFT treatments have demonstrated large effect sizes with a range of conditions, including pain, PTSD (in both civilian and military veteran populations), phobias, anxiety, and depression.
Objective: This review describes the approach, with a focus on PTSD in veterans and service members, provides an overview of how EFT is most commonly applied, and outlines obstacles and cautions related to its implementation.
Methods: Peer-reviewed clinical trials and meta-analyses of EFT in the treatment of PTSD are assessed to identify the characteristics of the approach that render it suitable for the treatment of PTSD.
Results: The literature demonstrates that remediation of PTSD and comorbid conditions is typically accomplished within brief time frames, ranging from one session for phobias to between four and ten sessions for PTSD. Clinical EFT has been shown to regulate stress hormones and limbic function and to improve various neurologic markers of general health. The epigenetic effects of EFT include upregulation of immunity genes and downregulation of inflammation genes. Six dismantling studies have indicated that the acupressure component of EFT is an active ingredient and not placebo.
Conclusions: Seven empirically supported strengths of the approach were identified that make it especially suitable for use with veterans and active military: (1) the depth and breadth of treatment effects; (2) the relatively brief timeframes required for successful treatment; (3) the low risk of adverse events; (4) the minimal training time required for the approach to be applied effectively; (5) the simultaneous reduction of physical and psychologic symptoms; (6) the utility and cost-effectiveness of clinical EFT in a large group format; and (7) the method's adaptability to online and telemedicine applications.
Keywords: : acupuncture, PTSD, Emotional Freedom Techniques, anxiety, depression, pain
Introduction
Post-traumatic stress disorder (PTSD) is a mental health condition that can be caused by direct involvement in, witnessing, or indirect exposure to a terrifying event. Symptoms include flashbacks, nightmares, severe anxiety, and uncontrollable thoughts about the event. The condition can interfere with relationships, ability to hold a job, general functioning, and overall health. Accidents, natural disasters, physical or sexual abuse, involvement in a violent crime, civil unrest, or warfare may lead to PTSD, which has reached epidemic proportions, The Veterans Administration <VA> alone is trying to cope with an estimated 500,000 PTSD cases resulting from the Iraq and Afghanistan wars.1
PTSD received official recognition as a clinical condition in 1980 with its inclusion in the third edition of the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders.2 Since then, research into PTSD treatment modalities has ranged from the pharmaceutical to the psychologic to the behavioral. However, this body of research has not resulted in a clear conceptualization of the disorder3 and has failed to provide “a cohesive body of evidence about what works and what does not.”4 Existing studies of PTSD treatments show that psychotherapies as disparate as cognitive behavioral therapy and eye movement desensitization and reprocessing (EMDR) might be equally effective, with other studies finding psychotherapy yielding superior long-term outcomes over psychopharmacology.5 PTSD is often regarded as “a treatment-resistant and refractory condition,”6 and some researchers argue that it is actually an incurable condition that clinicians can, at best, manage.7
The Institute of Medicine (IOM) of the National Academy of Sciences conducted a comprehensive assessment of the existing evidence regarding the outcomes of psychologic and pharmaceutical treatment modalities. In analyzing the most successful studies, the IOM concluded that “psychological exposure” was the only treatment element common to all.4 Based on its assessment, the IOM endorsed two methods for the treatment of PTSD: (1) exposure therapy and (2) cognitive therapy (which frequently utilizes exposure techniques). A 2010 research review conducted for the American Psychiatric Association confirmed the IOM finding that psychologic exposure is singularly effective in the treatment of PTSD.8 Professional practice guidelines now cite exposure therapy as a standard component in the treatment of PTSD.8 Although the techniques utilized in exposure therapy differ, the underlying principle remains the same: exposure to anxiety-producing memories, cues, or other triggers in a controlled setting can alleviate or even eliminate the effects of those triggers in the patient being treated.9
Incorporating Acupoint Stimulation into PTSD Treatment Protocols
Emotional Freedom Techniques (EFT) adds acupoint stimulation to established methods used in exposure and cognitive therapies. Acupuncture itself has been shown to be a potent intervention for PTSD, in particular on the battlefield,10,11 so the acupressure variant was a logical evidence-based adaptation of that approach. While focusing on an emotionally triggering memory, a client stimulates seven or more acupuncture points by tapping on them with his or her fingertips. The degree of emotional arousal is evaluated on an 11-point Likert scale before and after an application of EFT, with 0 indicating no emotional distress and 10 indicating extreme distress. This scale was originally applied in the treatment of trauma by Wolpe as a Subjective Units of Distress (SUD) scale while working with veterans of World War II.12,13 A single application of EFT is sometimes sufficient to reduce the emotional associations of the event to 0 on the SUD scale.14
The evidence-based form of EFT is referred to as “Clinical EFT” to distinguish it from dozens of variants that do not conform to the protocol that is in use for clinical trials of EFT.15 A case report describing the use of EFT in some detail is included in this issue of this journal.16
Therapists began to use EFT with veterans shortly after the first cohort began returning from the Iraq war in 2003, which was followed by its use with Vietnam veterans as well as those who served in other conflicts ranging from WWII to Afghanistan.17 The first pilot study of EFT for veterans presenting with PTSD was conducted at Marshall University Medical School, tracking outcomes after six treatment sessions.18 Highly significant reductions in PTSD symptoms were found, along with concomitant drops in anxiety and depression. Several studies of EFT delivered in a group therapy format also reported reductions in anxiety and depression.19–22 The acupoints used in the “Basic Recipe” protocol of Clinical EFT are shown in Figures 1 and 2.
FIG. 1.
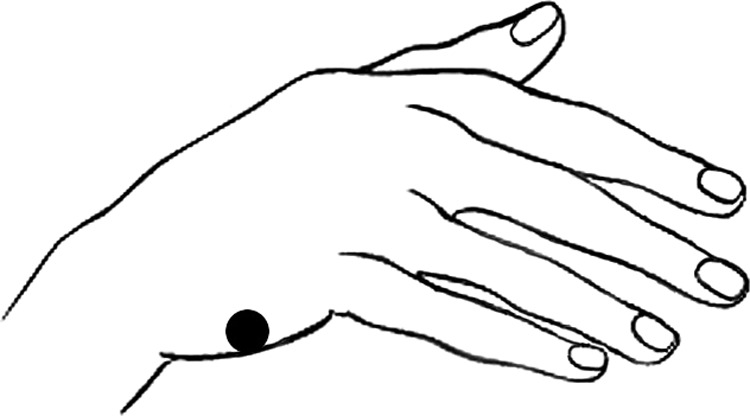
Hand point.
FIG. 2.
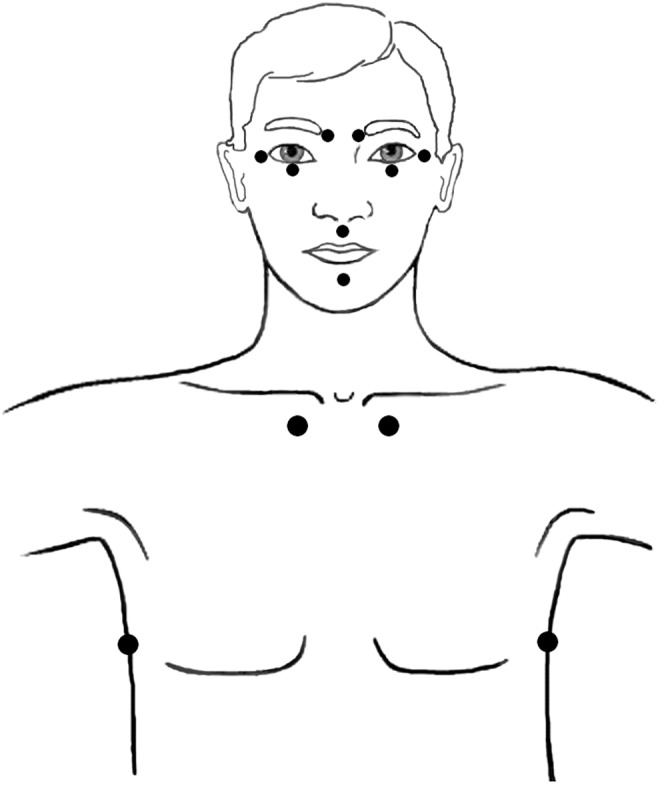
Head and torso points.
EFT with Veterans and Active Military
These early efforts were followed by a randomized controlled trial (RCT) with 49 veterans who initially scored above the PTSD cutoff on the standardized PTSD Checklist–Military Version (PCL-M). After six EFT sessions, 86% scored below the PTSD cutoff, with PTSD symptoms having been reduced by 64% (P < 0.0001). Gains were maintained at 3- and 6-months' follow-ups.23 A replication of this study yielded similar results.24 When the same treatment protocol was applied to veterans at risk of PTSD (heightened PTSD symptom levels but below the diagnostic cutoff), symptom reductions with gains holding at follow-up were also found.17 A meta-analysis of six RCTs of EFT for PTSD found a large effect size across the studies.25
EFT was a core intervention in two large multimodal programs treating PTSD in veterans or active military. Two hundred and eighteen male veterans and their spouses participated in one of six week-long retreats, with 83% of the veterans and 29% of the spouses initially scoring above the PTSD cutoff on a standardized PTSD checklist. Following the retreat, the number of veterans still in the PTSD range had been reduced to 28% and the number of spouses in that range had been reduced to 4%, with gains maintained at follow-up.26 In an ongoing 3-week “Warrior Combat Stress Reset Program” at Fort Hood, with results between 2008 and 2013 reported, 764 active duty service members showed significant reductions in PTSD symptoms (P < 0.001), anxiety (P < 0.001), depression (P < 0.001), and pain (P < 0.001) from pre- to post-treatment.27
While comparisons of a new treatment approach with established therapies do not usually show which patient populations will respond better to which treatment or other between-treatment differences, these comparisons do provide a benchmark for establishing whether or not a new therapy is efficacious. Head-to-head studies comparing EFT to cognitive therapy and EMDR in the treatment of PTSD have been conducted. Congolese women who had been subject to gender-based violence were randomly assigned to EFT treatments or cognitive therapy. The two modalities were equally efficacious.28 A study comparing EFT to EMDR was performed in a hospital in the United Kingdom's National Health Service. The researchers found that both therapies remediated PTSD in an average of four sessions.29 Randomized controlled trials of EFT, showing symptom domains and treatment effect sizes, are presented in Table 1.
Table 1.
Effect Sizes (Cohen's d, with 95% CI) of EFT Treatment, Compared to a Control or Pretreatment Directly After Treatment
| Condition, treatments & scales | Karatzias, et al., 201129 | Church, et al., 201260 | Church, et al., 201323 | Geronilla et al., 201624 | Church, et al., 201640 | Church, et al., 201517 | Nemiro and Papworth, 201528 |
|---|---|---|---|---|---|---|---|
| Control | PreEFT | WL/no treatment | TAU | TAU | TAU | TAU | PreEFT |
| Number of treatments | Up to eight 1-hour sessions | One session | Six 1-hour sessions | Six 1-hour sessions | Ten 1-hour sessions | Six 1-hour sessions | Eight 2½ hour sessions |
| PCL | 1.08 (0.38–1.73)a | 1.93 (1.28–2.58)b | 3.06 (2.30–3.82)b | 2.18 (1.25–2.99) | 6.63 (4.44–8.81)b | NA | |
| Anxiety | 1.11 (0.41–1.77)c | 1.36 (0.77–1.95)d | 1.55 (0.96–2.14)d | 0.78 (0.04–1.47) | 3.64 (2.24–5.04)d | ||
| Depression | 0.69 (0.02–1.32)c | 1.76 (1.13–2.39)d | 1.65 (1.06–2.25)d | 0.89 (0.15–1.60) | 4.32 (2.76–5.89)d | ||
| Intrusive memories | 3.95 (2.26–5.63)e | ||||||
| Avoidance | 6.89 (4.31–9.47)e | ||||||
| IES total | 8.07 (5.11–11.03)e | ||||||
| HSCL | 1.26 (0.61–1.87) | ||||||
| HTQ | 2.29 (1.51–2.99) |
PCL-C.
PCL-M.
HADS.
SA-45.
IES.
CI, confidence interval; EFT, Emotional Freedom Techniques; PCL, Posttraumatic Stress Disorder Checklist (M for Military Version and C for Civilian version); IES, Impact of Events scale; HSCL, Hopkins Symptom Checklist-25; HTQ, Harvard Trauma Questionnaire; WL, wait-list; TAU, treatment as usual; NA, not applicable; SA-45, Symptom Assessment-45; HADS, Hospital Anxiety and Depression Scale.
Mechanisms of Action
Several studies have used functional MRI to investigate the effect of acupuncture on the fear centers of the brain—a region often activated by PTSD. Hui and colleagues reported that needling specific acupuncture points sends deactivating signals to the amygdala, hippocampus, and other brain regions associated with fear and pain.30,31 Fang et al. provided evidence that acupuncture can bring about “extensive deactivation of the limbic–paralimbic–neocortical system.”32 These studies show that brain regions responsible for heightened affect, anxiety, and the fight–flight–freeze response can be regulated by acupuncture. Acupuncture has also been shown to produce endogenous opioids, increase production of serotonin, reduce the stress hormone cortisol, and modulate pain.33–36
Although EFT uses percussion (tapping) rather than needling, there is some evidence that the effect is similar or the same.33,37 For instance, a double-blinded study comparing penetration with nonpenetrating pressure on acupuncture points found equivalent clinical improvements.38 The tapping in EFT protocols seems to result in limbic system downregulation that is similar to that following the needling of specific acupuncture points.
A meta-analysis of six dismantling or partial dismantling studies has demonstrated that the acupuncture component is an essential ingredient, rather than a placebo, in the rapid outcomes shown in EFT clinical trials.* The stimulation of acupuncture points supplements and enhances the effects of the exposure and cognitive components of EFT protocols.
The stress response is activated by the coordinated expression of a specific set of genes at a particular moment in time.39 Rapid changes in gene expression have been shown to be an underlying mechanism in the effects of EFT protocols. Church et al. examined the effect of EFT treatments on gene expression in 16 veterans using a panel of stress-related genes.40 A ten-session treatment program resulted in the downregulation of the interleukin family of genes, which are associated with stress, and the upregulation of several genes associated with immunity. These shifts in gene expression corresponded with reductions in PTSD symptoms and other psychologic complaints, and were not found in the control condition.
A subsequent study investigated whole-genome expression in saliva samples from four nonclinical participants who received first a placebo session and then a 1-hour EFT session.41 The researchers identified differential expression in 72 genes following the EFT session. The functions of the genes affected by the EFT session revealed greater specificity than earlier studies. Among these functions were increased synaptic connectivity between neurons, building white matter in the brain, neural plasticity, metabolic regulation, reducing oxidative stress, strengthening cell membranes, immunity from opportunistic infections, antiviral activity, and synthesis of both red and white blood cells.
The biochemical sequelae of stress-induced changes in gene expression have also been subject to empirical analysis. A triple-blinded randomized controlled trial (RCT) of 83 nonclinical participants examined levels of the stress hormone cortisol in three different groups after a 1-hour session.42 EFT was compared to talk therapy and to rest. Reductions in cortisol were greatest in the EFT group and correlated significantly with drops in the breadth and depth of psychologic distress. A study of the multidimensional physiologic effects of EFT examined participants in a 5-day EFT workshop.† As in other EFT studies, depression, anxiety, PTSD, pain, and other psychologic conditions were reduced significantly. Along with these emotional improvements, resting heart rate went down, blood pressure dropped, and immune function as measured by salivary immunoglobulin A increased. Cortisol dropped by half.
Electroencephalogram studies have tracked changes in electrical activity in the brain following acupoint tapping. Lambrou et al. showed a change in theta waves, as well as reductions in muscular tension, in patients being treated for claustrophobia.43 Swingle et al. found that EFT reduced arousal in the right frontal cortex of victims of motor vehicle accidents being treated for trauma.44
The body of research exploring the physiologic basis of energy psychology (EP; of which EFT is the most widely practiced approach) indicates that EP can potentially modulate physiologic maladaptations, including: “(a) exaggerated limbic system responses to innocuous stimuli, (b) distortions in learning and memory, (c) imbalances between sympathetic and parasympathetic nervous system activity, (d) elevated levels of cortisol and other stress hormones, and (e) impaired immune functioning.”45 The combination of acupoint stimulation and mental activation of a stress-producing cue (the exposure component) counterconditions the cue such that it no longer triggers the maladaptive response.33 In PTSD, with cues triggering traumatic memories, EP reconfigures the memories via memory reconsolidation in such a manner as to eliminate their automatic triggering of limbic hyperarousal.37,46
These stress-reducing effects of EFT are likely relevant to the clinical and research evidence showing that EFT is effective for a broad range of physiologic as well as psychologic disorders. EFT has been used to successfully treat tension headaches,47 fibromyalgia,48 traumatic brain injury,49 frozen shoulder,50 seizure disorders,51 insomnia,52 chemotherapy side-effects,53 and psoriasis.54 In studies of EFT for PTSD, symptoms of anxiety and depression are reduced simultaneously, even though these comorbid conditions are not the primary targets of treatment. A meta-analysis of 20 studies that included a valid and reliable assessment of EFT for depression found a large treatment effect of d = 1.31.55 A meta-analysis of 14 RCTs on anxiety found d = 1.23, also indicating a large effect resulting from EFT treatment.56 The utility of EFT for reducing a wide range of psychologic symptoms has been noted in a number of studies.14,19,20,23,57
EFT in PTSD Treatment: Clinical Implications
Studies of EFT in the treatment of PTSD have consistently pointed to the following clinical strengths, all of which make EFT a favorable treatment option in military populations.
Few EFT Sessions Are Needed to Reduce PTSD
EFT can ameliorate symptoms of PTSD in remarkably few sessions. Studies of single-session EP interventions with individuals who had survived natural disasters, war, or genocide rampages have consistently found statistically significant symptom reductions.58,59 For instance, Church et al. found that a single EFT session brought 8 of 8 abused teenage boys living in a group home in Peru from clinical to nonclinical levels of PTSD on an inventory that tracked intrusive memories and avoidance symptoms. Gains held at a 1-month follow-up, while 8 other abused teenage boys from the group home, randomly selected to be on a wait-list, showed no improvement at 1-month post-testing.60
The number of sessions required to remediate PTSD to nonclinical levels in the studies cited earlier ranged from four29 to ten.40 In the first RCT of EFT in the treatment of PTSD with veterans,23 as well as its replication,24 six 1-hour sessions resulted in significant decreases in traumatic-stress symptoms. These findings have led to guidelines for the application of EFT with veterans presenting with PTSD as well as for at-risk individuals.61
Improvements Are Substantial and Lasting
Studies of the treatment effects following the application of EFT in cases of PTSD typically report highly significant clinical changes, reductions of a range of symptoms, and beneficial outcomes that persist over time. For instance, in the study by Church et al., the 49 veterans in the EFT group all scored above the PTSD cut-off score on the PCL-M before treatment; after six 1-hour sessions, only 7 (14%) of the 49 veterans exceeded that score, meaning that the other 42 no longer met the PCL-M criteria for a PTSD diagnosis.23 Benefits were maintained at a 6-month follow-up.
EFT Is Safe with a Low Risk of Adverse Events
Due to EFT's ability to reduce emotional charge and reaction rapidly, presumably linked to the deactivating signals sent to the limbic system when selected acupuncture points have been stimulated,30–32 practitioner surveys indicate therapist preference for EFT over other methods when dealing with highly emotional memories.14,62 Therapists with EFT training working with adult clients who had been sexually abused as children reported a strong preference for EFT over other methods that were available to them.63 EFT's emotion-stabilizing effect is operational even in the midst of memory recall by extremely traumatized individuals, for whom many memories are so emotionally fraught that they have hitherto avoided accessing them.13,64,65 An examination of the published literature on EFT found no reports of adverse events. Existing evidence indicates that EFT is a safe intervention for PTSD.
Minimal Training Is Needed to Use EFT
As well as being a method that can be integrated into nearly any clinical framework,66 EFT has proven to be effective when applied by paraprofessionals and life coaches following relatively brief training periods. EFT training and certification courses can typically be completed in a few months, with 6 classroom days and 50 supervised cases being sufficient to attain certification in Clinical EFT. One study compared EFT when delivered by life coaches with EFT when delivered by licensed mental health professionals. Veterans with PTSD symptoms received EFT treatments from a practitioner with either background, randomly assigned. Following treatment, 83% of the veterans working with a licensed provider had subclinical symptom levels at a 6-month follow-up, compared with 76% of veterans working with a life coach, a difference that was not statistically significant.67 Even community volunteers have been able to deliver effective EP interventions after brief training programs. Volunteers have, for instance, provided care with strong demonstrated benefits to traumatized orphans following the 2010 Haiti earthquake68 and to genocide survivors in Rwanda.69
The current authors are not advocating or claiming that minimal training is all that practitioners need in order to treat mental health disorders. The results of the studies indicate, however, that EFT could be effective as a front-line mental health intervention administered after relatively brief training of medics, physician's assistants, life coaches, and others with adequate backgrounds and life experience. In addition, licensed medical and mental health professionals can learn the method rapidly. EFT training of the teams responding to natural or human-caused disasters would increase the teams' resources and enable them to offer immediate and rapid psychologic assistance. In mental health agencies, which are often vastly under-resourced, training paraprofessionals, allied life coaches, and allied health care providers would enable the agencies to increase their treatment capacity and outreach to individuals who are in dire need of their services.
EFT Is Effective in Both Individual and Group Sessions
EFT has proven to be effective when used one-on-one or in groups. Several studies have shown EFT to be effective for reducing psychologic symptoms even when administered in large groups.19–22,26,68,70 It could thus be implemented readily with refugees assembled in camps, combat battalions returning from deployment, children in classrooms, caregivers returning from humanitarian missions, and other situations in which widespread one-on-one counseling is not possible due to money, time, staff restraints, or other limitations of the organizations or agencies involved. With teams of practitioners ready to provide trauma or other interventions at disaster sites or other points of service, group treatment is a responsible and efficient method for administering EFT.
EFT Can Remediate Both Psychologic and Physiologic Symptoms
EFT has been shown to resolve or reduce many of the psychologic and physiologic symptoms associated with PTSD. The connection between psychologic trauma and organic disease has been demonstrated persuasively, with trauma often contributing to the development of serious illness.71 If PTSD goes untreated and becomes chronic, it alters brain physiology.72 The results of persistent PTSD symptoms include increases in lifetime hospitalization, disease burdens, and medical costs.73 Untreated PTSD affects not only patients and their families, but also their communities and society at large.74 For the treatment of veterans with PTSD, EFT can ameliorate such associated physical symptoms as traumatic brain injury49 and sleep apnea.75 The epidemic of military suicides is fueled in part by PTSD-related depression, which is also amenable to EFT Treatment.55 EFT is a fast, potent, and cost-effective treatment for addressing physiologic as well as psychologic symptoms.
EFT Can Be Delivered via Electronic Communication Media
The effectiveness of EFT delivered by telephone or via the internet has been studied. A series of six telephone treatment sessions alleviated clinical PTSD symptoms in 67% of participants.76 In another study, 26 women diagnosed with fibromyalgia who participated in an internet-based EFT treatment program had significant improvement in measures of pain, anxiety, depression, vitality, social function, activity level, and performance problems.48
Case histories submitted by EFT practitioners to an EFT website‡ point to increasing utilization of audio and video conferencing services, such as Google Hangouts, Webex, Zoom, and Skype. This use of electronic media enables the application of EFT to a broader patient population than is possible with conventional therapy. This would allow access to treatment for veterans who are reluctant to utilize mental health care in official government settings because of such factors as the stigma of mental illness and the widespread mistrust of bureaucracies. For these reasons, EFT is adaptable to the multiple settings where veterans seek help—on the battlefield, at the home base, within the VA system, in civilian clinics, in drop-in centers, and in inaccessible rural areas.
Controversies Around EFT
Despite evidence of the efficacy of EFT, beginning with clinical reports in the 1980s and culminating with more-recent dismantling studies and meta-analyses, the technique has faced many obstacles to acceptance. The lapse between a new discovery and its implementation in clinical practice has been referred to as the “translational gap.” According to an IOM report, only ∼20% of clinical innovations are successful in crossing the gap, which the IOM report refers to as a “chasm.”77 For those that are successful, the process takes close to 2 decades. In other words, current medical practice is offering patients only 20% of established clinical innovations, and these were available some 20 years before becoming widely utilized.
Beyond these contextual factors facing any clinical innovation, EFT's acceptance has been hampered by (1) the fact that tapping on the skin looks blatantly strange, (2) the ability of tapping to help overcome serious emotional problems is not self-evident nor explained by conventional psychologic theory, (3) EFT borrows heavily from ancient healing methods that are traced to non-Western cultures, and (4) EFT made its first indelible impression on the clinical community with unprecedented claims (e.g., “the 5-minute phobia cure”) that were not backed at the time by research evidence or plausible explanations for the mechanisms of action. Gatekeepers of official bodies and websites often actively block novel treatments and, with EFT's odd appearance, unfamiliar mechanisms of action, and extravagant early claims, it is not surprising that it experienced such resistance.
For instance, in 1999, the American Psychological Association prohibited its sponsoring organizations from offering continuing education credit to psychologists for learning EFT and allied methods.78 While this ban was lifted in 2012, the authoritative Division 12 website¶ listing research-supported psychologic treatments has still not included EFT, despite its having met Division 12's published standards.79 In fact, not one of the more than 100 EFT RCTs, meta-analyses, outcome studies, and case histories published in the past 15 years§ is mentioned or reviewed.
In terms of public perception, Wikipedia is the most popular and widely cited encyclopedia in the world. Its entries, however, often reflect the prejudices of established groups.80 In the early 2000s, a group of professional skeptics81 assumed control of the Wikipedia entries on complementary and alternative medicine (CAM). These skeptics rewrote the entries according to their own agendas, with pertinent facts omitted and biased assessments emphasized. When reputable scholars and subject matter experts attempted to correct misleading statements, the pages were “protected” (locked) from any other editors. This is why the Wikipedia entry on acupuncture, whose principles are at the foundation of EFT, begins with the assertion: “traditional Chinese medicine (TCM)…theory and practice are not based upon scientific knowledge, and acupuncture is a pseudoscience.” The wealth of scientific information contradicting these assertions—found in empirically grounded texts on acupuncture82,83 and in a dozen scholarly acupuncture-related journals in the English language alone—is ignored.
The skeptics regularly “update” the Wikipedia article, adding such statements as: “Many within the scientific community consider attempts to rationalize acupuncture in science to be quackery, pseudoscience and ‘theatrical placebo.’” The top of the article on acupressure reflects a similar bias, informing the reader of Quackwatch's warning that “acupressure is a dubious practice, and its practitioners use irrational methods.” Likewise, Wikipedia's EFT article tells the reader: “EFT has no benefit as a therapy beyond the placebo effect or any known effective psychological techniques that may be provided in addition to the purported ‘energy’ technique. … It is generally characterized as pseudoscience and has not garnered significant support in clinical psychology.” None of the studies cited in this article are listed. Such widely disseminated systematic opposition to unconventional evidence-based therapies extends the translational gap, preventing the timely utilization of efficacious innovations with patients in need of more effective care.
Conclusions
PTSD can be crippling for patients who are affected. It constitutes a growing burden to already overstrained public agencies and medical facilities and exerts an increasing toll on society in violence and economic costs. PTSD's impact on military and veteran populations has been particularly devastating.
Therapeutic interventions that are more effective than conventional PTSD treatments are needed urgently. Research has shown that EFT—a modality that combines the stimulation of acupuncture points with exposure and cognitive techniques—provides such a solution. Among its strengths are its speed and effectiveness for a wide range of psychologic and physiologic conditions, the durability of the clinical outcomes EFT facilitates, its safety, the speed with which EFT can be learned, and its compatibility with group treatment and online platforms that make it possible to treat many patients at once. These factors make EFT a potentially valuable protocol for use by clinicians who treat veterans, whether in military or civilian settings. Institutional and other forces blocking the dissemination of EFT are hindering a significant resource in the remediation of PTSD for both civilians and military personnel.
Author Disclosure Statement
The authors of this article provide services and have published books related to the approach discussed.
CME Quiz Questions
Article learning objectives:
After studying this article, participants should be able to assess peer‐reviewed clinical trials and meta‐analyses of EFT in the treatment of PTSD and identify the characteristics of EFT that support its usefulness in treating PTSD.
Publication date: August 1, 2017
Expiration date: August 31, 2018
Disclosure Information:
Authors have nothing to disclose.
Richard C. Niemtzow, MD, PhD, MPH, Editor-in-Chief, has nothing to disclose.
Questions:
- 1. Identify the incorrect statement:
- a. The Institute of Medicine identifies exposure therapy and cognitive therapy as evidence based therapies for PTSD.
- b. Emotional Freedom Technique adds acupuncture point stimulation to established methods used in exposure and cognitive therapies.
- c. While focusing on an emotionally triggering memory, patients stimulate seven or more acupuncture points by tapping on them with their fingertips.
- d. The evidence-based form of EFT is referred to as “Clinical EFT” to distinguish it from variants that do not conform with the protocol that is used in clinical trials.
- e. EFT uses a set of special, newly identified acupuncture points.
- 2. Identify the incorrect statement:
- a. EFT was a core intervention in two large multi-modal programs treating PTSD in veterans and active military.
- b. These studies showed significant reductions in PTSD symptoms, anxiety, depression, and pain.
- c. A meta-analysis of six RCTs of EFT for PTSD found a large effect size across all of the studies.
- d. Comparison studies for EFT and cognitive therapy for PTSD have not yet been conducted.
- e. Comparative effectiveness trials have demonstrated EFT to be equally effective as cognitive therapy and EMDR.
- 3. Identify the incorrect statement:
- a. fMRI studies on acupuncture demonstrate a regulatory effect on “fear centers” in the brain including the amygdala and hippocampus.
- b. Limbic, paralimbic and neocortex are regions of the brain responsible for heightened affect, anxiety, and fight-flight response.
- c. Acupuncture has been demonstrated to reduce the stress hormone cortisol and increase the production of serotonin and endogenous opioids.
- d. Patients with PTSD show increased cortisol and norepinephrine responses to stress.
- e. PTSD is associated with decreased cortisol response to stress.
- 4. Identify the incorrect statement:
- a. EFT uses percussion (tapping) rather than needling of acupuncture points.
- b. The simultaneous activity of acupoint stimulation and mental activation of a stress-producing cue is not an important part of EFT's action.
- c. Meta-analyses of dismantling studies has demonstrated that the acupuncture point component in EFT is an essential ingredient in the rapid outcomes shown in EFT clinical trials.
- d. EFT combines acupoint stimulation with mental activation of a stress-producing cue (the exposure component).
- e. The observed effect of EFT is that it deconditions the stress producing cue such that it no longer triggers the maladaptive response.
-
5. Identify the incorrect statement:
The research evidence suggests that the clinical strengths of EFT in the treatment of PTSD include:- a. Few EFT sessions are needed to reduce PTSD.
- b. Improvements are substantial and long lasting.
- c. There is a low risk of adverse events.
- d. EFT is effective in both individual and group sessions.
- e. EFT therapy is an opportunity for investors to generate income based on a new, expensive, highly technological medical device.
Continuing Medical Education – Journal Based CME Objectives:
Articles in Medical Acupuncture will focus on acupuncture research through controlled studies (comparative effectiveness or randomized trials); provide systematic reviews and meta-analysis of existing systematic reviews of acupuncture research and provide basic education on how to perform various types and styles of acupuncture. Participants in this journal-based CME activity should be able to demonstrate increased understanding of the material specific to the article featured and be able to apply relevant information to clinical practice.
CME Credit
You may earn CME credit by reading the CME-designated article in this issue of Medical Acupuncture and taking the quiz online. A score of 75% is required to receive CME credit. To complete the CME quiz online, go to http://www.medicalacupuncture.org/cme – AAMA members will need to login to their member account. Non-members have the opportunity to participate for a small fee.
Accreditation: The American Academy of Medical Acupuncture is accredited by the Accreditation Council for Continuing Medical Education (ACCME).
Designation: The AAMA designates this journal-based CME activity for a maximum of 1 AMA PRA Category 1 Credit™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Church D, Feinstein D, Stapleton P, Gallo F, Yang A. Is tapping on acupuncture points an active ingredient in Emotional Freedom Techniques (EFT)? A review and meta-analysis of dismantling studies. Manuscript submitted for publication. 2017.
Bach D, Groesbeck G, Stapleton P, Banton S, Blickheuser K, Church D. Clinical EFT (Emotional Freedom Techniques) improves multiple physiological markers of health. Presented at Omega Institute, October 15, 2016.
Visit www.EFTuniverse.com for more information.
Visit www.div12.org/psychological-treatments/ (retrieved January 8, 2017) for more information.
Visit Research.EFTuniverse.com for the current bibliography.
References
- 1.Veterans Health Administration. Report on VA Facility Specific Operation Enduring Freedom (OEF), Operation Iraqi Freedom (OIF), and Operation New Dawn (OND) Veterans Coded with Potential PTSD. 2014. Online document at: www.publichealth.va.gov/docs/epidemiology/ptsd-report-fy2014-qtr3.pdf Accessed December30, 2016
- 2.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 3rd ed. Washington, DC: American Psychiatric Association; 1980 [Google Scholar]
- 3.Zoellner LA, Eftekhari A, Bedard-Gilligan M. Psychological models of posttraumatic stress disorder and acute stress disorder. In: Antony MM, Stein MB, eds. Oxford Handbook of Anxiety and Related Disorders. Oxford, England: Oxford University Press; 2008:250–261 [Google Scholar]
- 4.Institute of Medicine, Committee on Treatment of Posttraumatic Stress Disorder. Summary. In: Treatment of Posttraumatic Stress Disorder: An Assessment of the Evidence. Washington, DC: National Academy of Sciences; 2008:1–15 [Google Scholar]
- 5.Van der Kolk BA, Spinazzola J, Blaustein ME, et al. A randomized clinical trial of eye movement desensitization and reprocessing (EMDR), fluoxetine, and pill placebo in the treatment of posttraumatic stress disorder: Treatment effects and long-term maintenance. J Clin Psychiatry. 2007;68(1):37–46 [DOI] [PubMed] [Google Scholar]
- 6.Gallo FP. Energy psychology in rehabilitation: Origins, clinical applications, and theory. Energy Psychol. 2009;1(1):57–72 [Google Scholar]
- 7.Johnson DR, Fontana A, Lubin H, Corn B, Rosenheck RA. Long-term course of treatment-seeking Vietnam veterans with posttraumatic stress disorder: Mortality, clinical condition, and life satisfaction. J Nerv Ment Dis. 2004;192(1):35–41 [DOI] [PubMed] [Google Scholar]
- 8.Ursano RJ, Work Group on ASD and PTSD. Practice Guideline for the Treatment of Patients with Acute Stress Disorder and Posttraumatic Stress Disorder. Washington, DC: American Psychiatric Association, 2010. Online document at: https://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/acutestressdisorderptsd.pdf Accessed December14, 2016 [Google Scholar]
- 9.Abramowitz JS, Deacon BJ, Whiteside SPH. Exposure Therapy for Anxiety: Principles and Practice. New York: Guilford; 2012 [Google Scholar]
- 10.Niemtzow RC, Marcucci L, York A, Ives JA, Walter J, Jonas WB. The roles of acupuncture and other components of integrative medicine in cataclysmic natural disasters and military conflicts. Med Acupunct. 2014;26(5):255–263 [Google Scholar]
- 11.Engel CC, Cordova EH, Benedek DM, et al. Randomized effectiveness trial of a brief course of acupuncture for posttraumatic stress disorder. Med Care. 2014;52(12[suppl5]):S57–S64 [DOI] [PubMed] [Google Scholar]
- 12.Wolpe J. The Practice of Behavior Therapy. New York: Pergamon Press; 1969 [Google Scholar]
- 13.Church D. Psychological Trauma: Healing Its Roots in Brain, Body, and Memory, 2nd ed. Santa Rosa, CA: Energy Psychology Press; 2017 [Google Scholar]
- 14.Mollon P. Thought Field Therapy and its derivatives: Rapid relief of mental health problems through tapping on the body. Prim Care Community Psychiatry 2007;12(3–4):123–127 [Google Scholar]
- 15.Church D. The EFT Manual, 3rd ed Santa Rosa, CA: Energy Psychology Press; 2013 [Google Scholar]
- 16.Minewiser L. Six sessions of Emotional Freedom Techniques remediate one veteran's combat-related post-traumatic stress disorder. Med Acupunct. 2017;29(4):249–253 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Church D, Sparks T, Clond M. EFT (Emotional Freedom Techniques) and resiliency in veterans at risk for PTSD: A randomized controlled trial. Explore (NY). 2015;12(5):355–365 [DOI] [PubMed] [Google Scholar]
- 18.Church D, Geronilla L, Dinter I. Psychological symptom change in veterans after six sessions of EFT (Emotional Freedom Techniques): An observational study. Int J Healing Caring. 2009;9(1) [Google Scholar]
- 19.Church D, Brooks AJ. The effect of a brief EFT (Emotional Freedom Techniques) self-intervention on anxiety, depression, pain and cravings in healthcare workers. Integr Med. 2010;9(5):40–44 [Google Scholar]
- 20.Palmer-Hoffman J, Brooks AJ. Psychological symptom change after group application of EFT (Emotional Freedom Techniques). Energy Psychol. 2011;3(1):33–38 [Google Scholar]
- 21.Church D, Brooks AJ. The effect of EFT (Emotional Freedom Techniques) on psychological symptoms in addiction treatment: A pilot study. Int J Sci Res Rep. 2013;2(1):315–323 [Google Scholar]
- 22.Church D, De Asis MA, Brooks AJ. Brief group intervention using EFT (Emotional Freedom Techniques) for depression in college students: A randomized controlled trial. Depress Res Treat. 2012;2012:257172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Church D, Hawk C, Brooks A, et al. Psychological trauma symptom improvement in veterans using Emotional Freedom Techniques: A randomized controlled trial. J Nerv Ment Dis. 2013;201(2):153–160 [DOI] [PubMed] [Google Scholar]
- 24.Geronilla L, Minewiser L, Mollon P, McWilliams M, Clond M. EFT (Emotional Freedom Techniques) remediates PTSD and psychological symptoms in veterans: A randomized controlled replication trial. Energy Psychol. 2016:8(2):13–28 [Google Scholar]
- 25.Sebastian B, Nelms J. Emotional Freedom Techniques (EFT) for posttraumatic stress disorder: A meta-analysis. Explore (NY). 2017:13(1):16–25 [DOI] [PubMed] [Google Scholar]
- 26.Church D, Brooks AJ. CAM and energy psychology techniques remediate PTSD symptoms in veterans and spouses. Explore (NY). 2014;10(1):24–33 [DOI] [PubMed] [Google Scholar]
- 27.Libretto S, Hilton L, Gordon S, Zhang W, Wesch J. Effects of integrative PTSD treatment in a military health setting. Energy Psychol. 2015;7(2):33–44 [Google Scholar]
- 28.Nemiro A, Papworth S. Efficacy of two evidence-based therapies, Emotional Freedom Techniques (EFT) and cognitive behavioral therapy (CBT) for the treatment of gender violence in the Congo: A randomized controlled trial. Energy Psychol. 2015;7(2):13–25 [Google Scholar]
- 29.Karatzias T, Power K, Brown K, et al. A controlled comparison of the effectiveness and efficiency of two psychological therapies for post-traumatic stress disorder: eye movement desensitization and reprocessing vs. Emotional Freedom Techniques. J Nerv Ment Dis. 2011;199(6):372–378 [DOI] [PubMed] [Google Scholar]
- 30.Hui KK, Liu J, Makris N, et al. Acupuncture modulates the limbic system and subcortical gray structures of the human brain: Evidence from fMRI studies in normal subjects. Hum Brain Mapp. 2000;9(1):13–25 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Hui KK, Liu J, Marina O, et al. The integrated response of the human cerebro-cerebellar and limbic systems to acupuncture stimulation at ST 36 as evidenced by fMRI. Neuroimage. 2005;27(3):479–496 [DOI] [PubMed] [Google Scholar]
- 32.Fang J, Jin Z, Wang Y, et al. The salient characteristics of the central effects of acupuncture needling: Limbic–paralimbic–neocortical network modulation. Hum Brain Mapp. 2009;30(4):1196–1206 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Lane J. The neurochemistry of counterconditioning: Acupressure desensitization in psychotherapy. Energy Psychol. 2009;1(1):31–44 [Google Scholar]
- 34.Akimoto T, Nakahori C, Aizawa K, Kimura F, Fukubayashi T, Kono I. Acupuncture and responses of immunologic and endocrine markers during competition. Med Sci Sports Exerc. 2003;35(8):1296–1302 [DOI] [PubMed] [Google Scholar]
- 35.Lee SC, Yin SJ, Lee ML, Tsai WJ, Sim CB. Effects of acupuncture on serum cortisol level and dopamine beta-hydroxylase activity in normal Chinese. Am J Chin Med. 1982;10(1–4):62–69 [DOI] [PubMed] [Google Scholar]
- 36.Ulett G. Beyond Yin and Yang: How Acupuncture Really Works. St. Louis, MO: Warren H. Green; 1992 [Google Scholar]
- 37.Feinstein D. Rapid treatment of PTSD: Why psychological exposure with acupoint tapping may be effective. Psychotherapy (Chic). 2010;47(3):385–402 [DOI] [PubMed] [Google Scholar]
- 38.Takakura N, Yajima H. Analgesic effect of acupuncture needle penetration: A double-blind crossover study. Open Med. 2009;3(2):54–61 [PMC free article] [PubMed] [Google Scholar]
- 39.de Nadal E, Ammerer G, Posas F. Controlling gene expression in response to stress. Nat Rev Genet. 2011;12(2):833–845 [DOI] [PubMed] [Google Scholar]
- 40.Church D, Yount G, Rachlin K, Fox L, Nelms J. Epigenetic effects of PTSD remediation in veterans using clinical EFT (Emotional Freedom Techniques): A randomized controlled pilot study. Am J Health Promot. 2016;August 12:e-pub ahead of print [DOI] [PubMed] [Google Scholar]
- 41.Maharaj ME. Differential gene expression after Emotional Freedom Techniques (EFT) treatment: A novel pilot protocol for salivary mRNA assessment. Energy Psychol. 2016;8(1):17–32 [Google Scholar]
- 42.Church D, Yount G, Brooks A. The effect of Emotional Freedom Techniques (EFT) on stress biochemistry: A randomized controlled trial. J Nerv Ment Dis. 2012;200(10):891–896 [DOI] [PubMed] [Google Scholar]
- 43.Lambrou PT, Pratt GJ, Chevalier G. Physiological and psychological effects of a mind/body therapy on claustrophobia. Subtle Energies Energy Med. 2003;14(3):239–251 [Google Scholar]
- 44.Swingle PG, Pulos L, Swingle MK. Neurophysiological indicators of EFT treatment of posttraumatic stress. Subtle Energies Energy Med. 2004;15(1):75–86 [Google Scholar]
- 45.Feinstein D, Church D. Modulating gene expression through psychotherapy: The contribution of noninvasive somatic interventions. Rev Gen Psychol. 2010;14(4):283–295 [Google Scholar]
- 46.Feinstein D. How energy psychology changes deep emotional learnings. Neuropsychotherapist 2015;January 1:38–49 [Google Scholar]
- 47.Bougea AM, Spandideas N, Alexopoulos EC, Thomaides T, Chrousos GP, Darviri C. Effect of the Emotional Freedom Technique on perceived stress, quality of life, and cortisol salivary levels in tension-type headache sufferers: A randomized controlled trial. Explore (NY). 2013;9(2):91–99 [DOI] [PubMed] [Google Scholar]
- 48.Brattberg G. Self-administered EFT (Emotional Freedom Techniques) in individuals with fibromyalgia: A randomized trial. Integr Med. 2008;7(4):30–35 [Google Scholar]
- 49.Church D, Palmer-Hoffman J. TBI symptoms improve after PTSD remediation with Emotional Freedom Techniques. Traumatology. 2014;20(3):172–181 [Google Scholar]
- 50.Church D, Nelms J. Pain, range of motion, and psychological symptoms in a population with frozen shoulder: A randomized controlled dismantling study of Clinical EFT (Emotional Freedom Techniques). Arch Sci Psychol. 2016;15(1):38–48 [Google Scholar]
- 51.Swingle P. EFT in the neurotherapeutic treatment of seizure disorders. Energy Psychol. 2010;2(1):27–38 [Google Scholar]
- 52.Lee JH, Chung SY, Kim JW. A comparison of Emotional Freedom Techniques–Insomnia (EFT-I) and Sleep Hygiene Education (SHE) for insomnia in a geriatric population: A randomized controlled trial. Energy Psychol. 2015;7(1):22–29 [Google Scholar]
- 53.Baker BS, Hoffman CJ. Emotional Freedom Techniques (EFT) to reduce the side effects associated with tamoxifen and aromatase inhibitor use in women with breast cancer: A service evaluation. Eur J Integr Med. 2014;7(2):136–142 [Google Scholar]
- 54.Hodge PM, Jurgens CY. Psychological and physiological symptoms of psoriasis after brief Emotional Freedom Techniques Treatment: A pilot study. Energy Psychol. 2011;3(2):13–23 [Google Scholar]
- 55.Nelms J, Castel D. A systematic review and meta-analysis of randomized and non-randomized trials of Emotional Freedom Techniques (EFT) for the treatment of depression. Explore (NY). 2016;12(6):416–426 [DOI] [PubMed] [Google Scholar]
- 56.Clond M. Emotional Freedom Techniques for anxiety: A systematic review with meta-analysis. J Nerv Ment Dis. 2016;204(5):388–395 [DOI] [PubMed] [Google Scholar]
- 57.Church D. Pain, depression, and anxiety after PTSD symptom remediation in veterans. Explore (NY). 2014;10(3):162–169 [DOI] [PubMed] [Google Scholar]
- 58.Church D. Clinical EFT (Emotional Freedom Techniques) as single session therapy: Cases, research, indications, and cautions. In: Hoyt M, Talmon M, eds. Capture the Moment: Single Session Therapy and Walk-in Service. Bethel, CT: Crown House; 2013:299–324 [Google Scholar]
- 59.Feinstein D. Energy psychology in disaster relief. Traumatology. 2008;14(1):127–139 [Google Scholar]
- 60.Church D, Piña O, Reategui C, Brooks AJ. Single session reduction of the intensity of traumatic memories in abused adolescents after EFT: A randomized controlled pilot study. Traumatology. 2012;18(3):73–79 [Google Scholar]
- 61.Church D, Stern S, Boath E, Stewart A, Feinstein D, Clond M. Using Emotional Freedom Techniques (EFT) to treat PTSD in veterans: A review of the evidence, survey of practitioners, and proposed clinical guidelines. Permanente J. 2017;21(2), 16–23 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Flint GA, Lammers W, Mitnick DG. Emotional Freedom Techniques: A safe treatment intervention for many trauma based issues. In: Garrick J, Williams MB, eds. Trauma Treatment Techniques: Innovative Trends. New York: Routledge; 2005:125–150 [Google Scholar]
- 63.Schulz P. Integrating energy psychology into treatment for adult survivors of childhood sexual abuse. Energy Psychol. 2009;1(1):15–22 [Google Scholar]
- 64.Church D. The treatment of combat trauma in veterans using EFT (Emotional Freedom Techniques): A pilot protocol. Traumatology 2010;16(1):55–65 [Google Scholar]
- 65.Carbonell JL, Figley C. A systematic clinical demonstration project of promising PTSD treatment approaches. Traumatology. 1999;5(1):6–21 [Google Scholar]
- 66.Feinstein D. A survey of energy psychology practitioners: Who they are, what they do, who they help. Energy Psychol. 2016;8(1):33–39 [Google Scholar]
- 67.Stein PK, Brooks AJ. Efficacy of EFT provided by coaches versus licensed therapists in veterans with PTSD. Energy Psychol. 2011;3(1):11–17 [Google Scholar]
- 68.Gurret JM, Caufour C, Palmer-Hoffman J, Church D. Post-earthquake rehabilitation of clinical PTSD in Haitian seminarians. Energy Psychol. 2012;4(2):26–34 [Google Scholar]
- 69.Connolly S, Sakai C. Brief trauma intervention with Rwandan genocide–survivors using thought field therapy. Int J Emerg Ment Health. 2011;13(3):161–172 [PubMed] [Google Scholar]
- 70.Rowe JE. The effects of EFT on long-term psychological symptoms. Counseling Clin Psychol. 2005;2(3):104–111 [Google Scholar]
- 71.Felliti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. Am J Prev Med. 1998;14(4):245–258 [DOI] [PubMed] [Google Scholar]
- 72.Felmingham K, Kemp A, Williams L, et al. Changes in anterior cingulate and amygdala after cognitive behavior therapy of posttraumatic stress disorder. Psychol Sci. 2007;18(2):127–129 [DOI] [PubMed] [Google Scholar]
- 73.Tanielian T, Jaycox LH, eds. Invisible Wounds of War: Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery. Santa Monica, CA: RAND; 2008 [Google Scholar]
- 74.McFarlane AC, van der Kolk BA. Trauma and its challenge to society. In: Van der Kolk BA, McFarlane AC, Weisaeth L, eds. Traumatic Stress: The Effects of Overwhelming Experience on Mind, Body, and Society. New York: Guilford Press; 2007:24–46 [Google Scholar]
- 75.Drewry D. Central nervous system apnea can be caused by traumatizing events, and it can be resolved. Int J Healing Caring. 2107;17(1) [Google Scholar]
- 76.Hartung J, Stein P. Telephone delivery of EFT (Emotional Freedom Techniques) remediates PTSD symptoms in veterans: A randomized controlled trial. Energy Psychol. 2012;4(1):33–42 [Google Scholar]
- 77.Institute of Medicine, Committee on the Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy of Sciences; 2001 [Google Scholar]
- 78.Murray B. APA no longer approves CE sponsorship for Thought Field Therapy. APA Monitor Psychol. 1999;30(11):9–12 [Google Scholar]
- 79.Church D, Feinstein D, Palmer-Hoffman J, Stein PK, Tranguch A. Empirically supported psychological treatments: The challenge of evaluating clinical innovations. J Nerv Ment Dis. 2014;202(10):699–709 [DOI] [PubMed] [Google Scholar]
- 80.Leskowitz R. Harvard Doc to Wikipedia: “You're Not Playing Fair on Alternative Trauma Therapy.” Common Health, 2014. Online document at: www.wbur.org/commonhealth/2014/11/28/harvard-doc-to-wikipedia-youre-not-playing-fair-on-alternative-trauma-therapy Accessed January7, 2017
- 81.Mollon P. Debunking the pseudoscience debunkers. Clin Psychol Forum. 2007;174:13–16. [Google Scholar]
- 82.Deadman P, Al-Khafaji M, Baker K. A Manual of Acupuncture, 2nd ed East Sussex, England: Journal of Chinese Medicine Publications; 2007 [Google Scholar]
- 83.Keown D. The Spark in the Machine: How the Science of Acupuncture Explains the Mysteries of Western Medicine. Philadelphia: Kingsley; 2014 [Google Scholar]
References
To receive CME credit, you must complete the quiz online at: www.medicalacupuncture.org/cme