

Abstract
Purpose
The phase 2 MONARCH 1 study was designed to evaluate the single-agent activity and adverse event (AE) profile of abemaciclib, a selective inhibitor of CDK4 and CDK6, in women with refractory hormone receptor positive (HR+), HER2− metastatic breast cancer (MBC).
Experimental Design
MONARCH 1 was a phase 2 single arm open-label study. Women with HR+/HER2− MBC who had progressed on or after prior endocrine therapy and had 1 or 2 chemotherapy regimens in the metastatic setting were eligible. Abemaciclib 200 mg was administered orally on a continuous schedule every 12 hours until disease progression or unacceptable toxicity. The primary objective of MONARCH 1 was investigator-assessed objective response rate (ORR). Other endpoints included clinical benefit rate, progression-free survival (PFS) and overall survival (OS).
Results
Patients (n=132) had a median of 3 (range 1–8) lines of prior systemic therapy in the metastatic setting, 90.2% had visceral disease, and 50.8% had ≥3 metastatic sites. At the 12 month final analysis, the primary objective of confirmed objective response rate was 19.7% (95% CI: 13.3, 27.5; 15% not excluded); clinical benefit rate (CR+PR+SD≥6 months) was 42.4%, median progression-free survival was 6.0 months, and median overall survival was 17.7 months. The most common treatment-emergent AEs of any grade were diarrhea, fatigue, and nausea; discontinuations due to AEs were infrequent (7.6%).
Conclusion
In this poor-prognosis, heavily pre-treated population with refractory HR+/HER2- metastatic breast cancer, continuous dosing of single agent abemaciciclib was well tolerated and exhibited promising clinical activity.
Keywords: abemaciclib, metastatic breast cancer, refractory, CDK4, CDK6
Introduction
Patients with hormone receptor positive (HR+) metastatic breast cancer (MBC) represent the largest (>70%) MBC subpopulation and are frequently treated with sequential endocrine therapies.1,2 Although many patients with advanced HR+ breast cancer that initially benefit from hormone therapy will eventually have disease progression, the concept of endocrine resistance is rapidly evolving as many of these tumors continue to be hormone dependent and may respond to additional hormone therapies including new estrogen receptor degraders and the addition of mTOR inhibitors to hormonal therapy.3–5 The possibility of continuing to target hormone dependency is appealing as a large fraction of HR+ tumors do not respond well to chemotherapy. For example, in patients previously exposed to taxanes, response rates to chemotherapy are in the range of 10% to 20%, with median durations of response (DoRs) of 4 to 6 months and median progression-free survival (PFS) ranging from approximately 3 to 4 months.6–11 These chemotherapies may be associated with treatment-limiting toxicity and diminished quality of life.12,13 Therefore, treatments with novel mechanisms of action are needed that are effective, with less toxicity than what has been historically observed with chemotherapy.
One therapeutic approach that has shown promise in the treatment of patients with HR+ breast cancers is to inhibit cell cycle progression at the G1/S checkpoint by targeting cyclin-dependent kinases 4 and 6 (CDK4 and CDK6).14 CDK4 and CDK6, together with D-type cyclins, phosphorylate the Retinoblastoma (Rb) tumor suppressor protein, leading to release of Rb-bound E2F, which enables progression from the G1 to S phase of the cell cycle.15,16 In HR+ breast cancers, estrogen mediated signaling along with other oncogenic pathways can activate CDK4/cyclin D1 to promote proliferation.17–20
Abemaciclib is an inhibitor of CDK4 and CDK6, and in enzymatic assays is 14 times more potent against CDK4/cyclin D1 than CDK6/cyclin D3.21 In a phase 1 study, administration of abemaciclib as a single agent on a continuous schedule was feasible with grade 3 fatigue as the dose-limiting toxicity (DLT).22 In that phase 1 study, abemaciclib as a single agent demonstrated antitumor activity in patients with several cancers with an ORR of 26% in patients with hormone refractory HR+MBC.22
Based on the single agent activity observed in this population, the current phase 2 MONARCH 1 study (NCT02102490) was launched. MONARCH 1 is a multicenter, single-arm, open-label study to evaluate the single-agent activity of abemaciclib and further characterize the adverse event (AE) profile in patients with HR+/HER2- MBC who have received cytotoxic chemotherapy for MBC. This is a population for whom endocrine therapy would no longer be considered suitable.
Methods
Study Design and Objectives
MONARCH 1 was a phase 2 single-arm, open-label study of abemaciclib as a single agent in patients with refractory HR+/HER2− MBC. Patients were enrolled at 35 sites in four countries (Belgium, France, Spain, and the United States). The study protocol was approved by institutional review boards/ethics committees prior to initiation, and conducted in accordance with the Declaration of Helsinki; patients provided written informed consent before entering the study.
The primary objective was to evaluate ORR (complete response [CR] + partial response [PR]) based on investigator-assessed tumor response according to RECIST v1.123, with the primary efficacy analysis at 12 months after the last patient entered. A secondary analysis using independently reviewed tumor response was also planned. Key secondary objectives were safety and tolerability, overall survival (OS), DoR for patients with a confirmed CR or PR (confirmed by a second assessment ≥28 days from first evidence of response), PFS, disease control rate (DCR = CR + PR + stable disease [SD]), and clinical benefit rate (CBR = CR + PR + SD ≥ 6 months).
Patients were followed until death or overall study completion at 18 months after the last patient was enrolled. Patients on study therapy who continued to experience clinical benefit after study completion could continue to receive study therapy until one of the criteria for discontinuation was met.
Patients
Women ≥18 years of age with HR+ (positive for estrogen receptor [ER] and/or progesterone receptor [PgR] by IHC24), HER2 negative (by IHC or in situ-hybridization) MBC were eligible. Additional inclusion criteria included: adequate organ function, measurable disease according to RECIST v1.1, and an ECOG performance status (PS) of 0/1. Patients must have progressed on or after prior endocrine therapy and had prior treatment with at least two chemotherapy regimens, at least one but no more than two of which had been administered in the metastatic setting; one regimen must have included a taxane either in the adjuvant setting or metastatic disease setting.
Key exclusion criteria included prior treatment with CDK4 and CDK6 inhibitors; major surgery within 14 days; treatment with an investigational agent within 14 or 21 days of initial dose of study drug for nonmyelosuppressive or myelosuppressive agents, respectively; evidence or history of central nervous system metastases (screening for brain metastasis was required); and history of any other cancer (except non-melanoma skin cancer or carcinoma in-situ of the cervix), unless in complete remission with no therapy for ≥3 years.
Treatment and Dose Reductions
Abemaciclib 200 mg was administered orally on a continuous schedule every 12 (+/−2) hours (Q12H) on days 1 to 28 of a 28-day cycle, until disease progression and/or unacceptable toxicity. Dose reductions in 50 mg decrements (up to 3 dose reductions allowed) and dose delays for AEs were permitted as per the guidance provided in the Supplemental Methods.
Supportive Management
Hematopoetic growth factors were permitted in accordance with ASCO guidelines.25 Patients were advised to take anti-diarrheal medication (as directed on the medication’s label) at the first onset of diarrhea.
Safety and Efficacy Assessments
AEs were collected at baseline and during the study, and were graded using the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0.26
Tumor assessments were performed according to RECIST v1.1 within 4 weeks before first dose of study drug (baseline), and at every other cycle using computerized tomography or magnetic resonance imaging. Assessment of best response included all tumor assessments from baseline until the earliest of objective progression or start of new anticancer therapy. All tumor measurement images for all enrolled patients were collected to allow for an independent review.
The ORR was estimated as the total number of confirmed CRs and PRs per RECIST v1.1 divided by the total number of patients enrolled. Responses were required to be confirmed at least 4 weeks after the initial observation. The DoR was measured from the date of first evidence (initial assessment) of CR or PR to the date of objective progression or death due to any cause, whichever was earlier. For patients who had experienced a tumor response and were not known to have died or have objective progression as of the data inclusion cutoff date, DoR was censored at the last complete objective progression-free disease assessment date.
PFS was measured from the date of first dose of study drug to the date of objective progression or death due to any cause, whichever was earlier. For patients without complete baseline disease assessments, PFS time was censored at the enrollment date; otherwise, patients were censored as described for DoR. OS was measured from the date of first dose of study drug to the date of death from any cause. OS was censored at the date of last contact prior to the data inclusion cutoff date. Patients were followed for OS for 18 months following the last patient entering treatment.
Statistical Methods
The study was powered assuming a null hypothesis ORR of 15% versus the alternative hypothesis ORR of 25% using a binomial exact test. The null hypothesis of 15% was chosen based on historical data as an ORR representative of what might be expected for approved chemotherapies that may be used in this taxane-refractory setting.6–11 Under this scenario a sample size of 128 provided 82% power at an overall one-sided alpha level of .025. For the primary endpoint, the point estimate, exact p-value for the test of ORR ≤15% versus >15%, and a 95% exact confidence interval were calculated. DoR and PFS were estimated using the Kaplan-Meier method. Point estimates and exact 95% CI for DCR and CBR were calculated. Efficacy and safety were assessed for the enrolled population. Data were analyzed using SAS version 9.2 (SAS Institute Inc., USA).
Results
Patients
A total of 132 patients with HR+ /HER2− MBC were enrolled from June 10, 2014 through April 30, 2015 and treated with abemaciclib (Supplemental Figure 1). All patients had measurable disease at study entry, as required per the protocol (RECIST v1.1). The majority (90.2%) of patients had visceral disease, and 50.8% of patients had 3 or more metastatic sites; the most common sites of metastasis were the liver and bone (Table 1). In the metastatic setting, patients had received a median of 3 (range 1–8) prior lines of systemic therapy including a median of 1 (1–3) lines of chemotherapy and 2 (1–6) lines of endocrine therapy.
Table 1.
Patient and Disease Characteristics
| Treated with abemaciclib (N=132) | |
|---|---|
| Age in years, median (range) | 58 (36–89) |
| ≥65 years, n (%) | 42 (31.8) |
| ECOG PS, n (%) | |
| 0 | 73 (55.3) |
| 1 | 59 (44.7) |
| Disease locations, n (%) | |
| Visceral | 119 (90.2) |
| Liver | 93 (70.5) |
| Lung | 31 (23.5) |
| Bone | 82 (62.1) |
| Bone-only | 3 (2.3) |
| Number of metastatic sites, n (%) | |
| 1 | 19 (14.4) |
| 2 | 46 (34.8) |
| ≥3 | 67 (50.8) |
| Prior endocrine therapy for metastatic disease | |
| Number of regimens | |
| 1 | 48 (36.4) |
| 2 | 25 (18.9) |
| 3 | 24 (18.2) |
| ≥ 4 | 18 (13.6) |
| Fulvestrant | 67 (50.8) |
| Prior chemotherapy for metastatic disease | |
| Number of regimens | |
| 1 | 67 (50.8) |
| 2 | 64 (48.5) |
| 3 | 1 (0.8)a |
| Taxanesb | 91 (68.9) |
| Capecitabine | 73 (55.3) |
| Other therapies for metastatic disease | |
| Everolimus | 37 (28.0) |
| Investigational drug | 16 (12.1) |
Patient first received capecitabine, and then received docetaxel; the patient had a break from docetaxel treatment and then restarted docetaxel without progression in between. The treatment with docetaxel was reported by the site as 2 regimens.
The remainder (31.1%) received prior taxane in the adjuvant setting.
Efficacy
Abemaciclib demonstrated single agent activity with 26/132 patients achieving a confirmed PR for an ORR of 19.7% (95% CI: 13.3, 27.5; 15% not excluded); there were no observed CRs (Table 2, Figure 1A). Of the 26 PRs, 12 (46.2%) patients had received at least 2 prior chemotherapies in the metastatic setting, 24 (92.3%) had visceral disease, and 12 (46.2%) had ≥3 metastatic sites. The median time to response was 3.7 months with a median DoR of 8.6 months (95% CI: 5.8–10.2); the probability of a response lasting at least 6 months was 70.4% and at least 12 months was 28.2% (Figure 1B). There were no patient characteristics, including baseline demographics and prior therapies received, that distinguished patients who rapidly progressed on therapy from those who did not (data not shown). The DCR was 67.4% (63 [47.7%] patients had SD) and the CBR was 42.4% (Table 2). As of April 30, 2016, 97 patients had experienced disease progression, and the median PFS was 6.0 months (95% CI: 4.2–7.5); the median OS was 17.7 months (95% CI: 16.0-NR) with 47 (35.6%) events occurring. Assessments by independent review yielded comparable rates and estimates (Table 2 and data not shown). A final analysis at 18 months of follow-up was conducted; the median OS was 22.3 months (95% CI: 17.7, NR) with 62 (47.0%) events occurring, and the data for the other endpoints were consistent with the 12 month analysis.
Table 2.
Responses according to RECIST v1.1
| Best Overall Response, n (%) | Investigator Determined N=132 |
Independent Review N=132 |
|---|---|---|
| Complete response (CR) | 0 (0.0) | 0 (0.0) |
| Partial response (PR) | 26 (19.7) | 23 (17.4) |
| Stable Disease (SD) | 63 (47.7) | 53 (40.2) |
| SD ≥6 months | 30 (22.7) | 20 (15.2) |
| Non-CR/Non-PD | – | 12 (9.1) |
| Non-CR/Non-PD ≥6 months | – | 7 (5.3) |
| Progressive disease (PD) | 34 (25.8) | 33 (25.0) |
| Not evaluable/not assessed | 9 (6.8) | 11 (8.3) |
| Objective Response Rate (CR + PR) (95% CI) |
26 (19.7) (13.3, 27.5; 15% not excluded) |
23 (17.4) (11.4, 25.0) |
| Disease Control Rate (CR + PR + SD) (95% CI) |
89 (67.4) (58.7, 75.3) |
88 (66.7) (57.9, 74.6) |
| Clinical Benefit Rate (CR + PR + SD ≥6 months) (95% CI) |
56 (42.4) (33.9, 51.3) |
50 (37.9) (29.6–46.7) |
| Survival Estimates | ||
| Median Overall Survival | 17.7 months (95% CI: 16.0–NR) |
N/A |
| Median Progression Free Survival | 6.0 months (95% CI: 4.2–7.5) |
5.9 months (95% CI: 3.7–8.1) |
Figure 1.
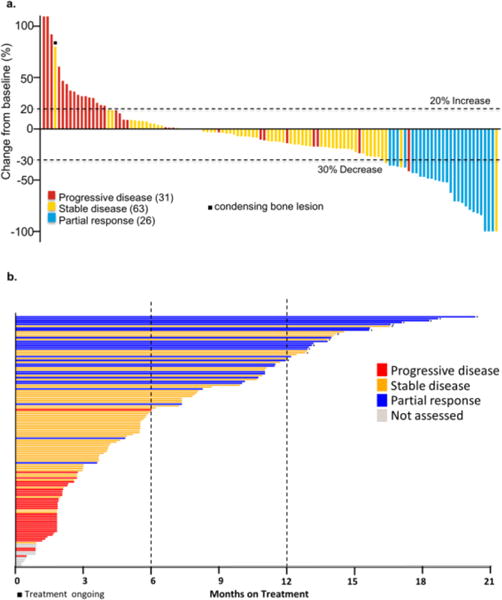
a. The best percent change in tumor size from baseline is plotted for each patient who had an available assessment b. Time on treatment with abemaciclib is plotted for each patient treated in the MONARCH 1 study (N=132). The colors in a and b represent response status per RECIST v1.1 and each bar in a and b represents one patient.
Safety
All patients had at least 1 treatment-emergent AE (TEAE); serious AEs (defined in Supplemental Methods) were reported for 32 patients (24.2%) and 3 grade 5 events occurred (1 grade 5 event of pneumonitis was deemed possibly related to study drug; the subsequent autopsy report showed extensive pulmonary lymphangitic carcinomatosis; the other 2 events were considered not to be treatment related). The most common TEAEs of any grade were diarrhea, fatigue, nausea, and decreased appetite (Table 3).
Table 3.
Treatment-emergent adverse events (TEAEs), regardless of causality (events occurring in ≥20% of patients)
| Investigator Assessed TEAEsa (N = 132) |
Grade 1 % |
Grade 2 % |
Grade 3 % |
Grade 4 % |
All Grades % |
|---|---|---|---|---|---|
| Diarrhea | 41.7 | 28.8 | 19.7 | 0 | 90.2 |
| Fatigue | 21.2 | 31.1 | 12.9 | 0 | 65.2 |
| Nausea | 39.4 | 20.5 | 4.5 | 0 | 64.4 |
| Decreased appetite | 28.0 | 14.4 | 3.0 | 0 | 45.5 |
| Abdominal pain | 22.0 | 14.4 | 2.3 | 0 | 38.6 |
| Vomiting | 22.7 | 10.6 | 1.5 | 0 | 34.8 |
| Headache | 13.6 | 6.8 | 0 | 0 | 20.5 |
| Lab abnormalitiesb | |||||
| Creatinine increased | 46.9 | 50.8 | 0.8 | 0 | 98.5 |
| White blood cell decreased | 18.5 | 44.6 | 27.7 | 0 | 90.8 |
| Neutrophil count decreased | 17.7 | 43.1 | 22.3 | 4.6 | 87.7c |
| Anemia | 30.0 | 38.5 | 0 | 0 | 68.5 |
| Platelet count decreased | 28.9 | 10.2 | 2.3 | 0 | 41.4 |
| Alanine aminotransferase increased | 24.6 | 1.5 | 3.8 | 0 | 30.0 |
| Alkaline phosphatase increased | 16.9 | 7.7 | 1.5 | 0 | 26.2 |
| Hypokalemia | 0 | 20.8 | 5.4 | 0 | 26.2 |
| Hyponatremia | 17.7 | 0 | 3.1 | 0 | 20.8 |
CTCAE Version 4.0
N = 130 for lab abnormalities listed, except platelet count decreased (N=128)
One patient who received cytotoxic chemotherapy within the 30 day follow up window experienced febrile neutropenia
Diarrhea was experienced by 119 (90.2%) patients, typically grade 1 (n=55, 41.7% of patients) or grade 2 (n=38, 28.8%) and less frequently grade 3 (n= 26, 19.7%) (Table 3). Diarrhea tended to occur early after initiation of therapy, with a median time to onset of 7.0 days. Importantly, the duration of diarrhea was generally limited; the median duration of grade 2 diarrhea was 7.5 days and grade 3 was 4.5 days, and there were no grade 4 events (Figure 2). The majority (78.1%) of patients with grade 2 and 3 diarrhea experienced it during the 1st cycle. As indicated in the protocol, many (60.6%) patients received anti-diarrheal medications; of these patients, most (94%) received loperamide. Most patients with an AE of diarrhea (72.3%) did not require a treatment change (dose reduction, omission, discontinuation) due to it, and only one patient (0.8%) discontinued due to diarrhea.
Figure 2.

Analysis of Adverse Event of Diarrhea. Time on treatment (in days) is presented for each patient (N=132). Each bar represents one patient and the length of the bar represents the duration on treatment. The start and end of treatment emergent adverse events of diarrhea while on treatment are color-coded by grade.
Increased blood creatinine was the most common laboratory abnormality reported, and 97.7% of patients assessed had a grade 1/2 event (Table 3). The elevation in serum creatinine was observed during the first cycle, and serum creatinine levels remained elevated and stable throughout the dosing period and decreased at the short term follow up visit (within 30 days of discontinuation of study treatment) (Supplemental Figure 2). Increases in blood urea nitrogen were not observed (Supplemental Figure 3). A post hoc analysis of baseline and Day 15 cystatin C, an alternative marker of renal function independent of serum creatinine used to estimate glomerular filtration rate (GFR)27,28, demonstrated that the rise in serum creatinine was not associated with elevation in cystatin C, and cystatin C-calculated GFR was not reduced; thus, the rise in serum creatinine was not temporally associated with reduced renal function (Supplemental Figure 4 and data not shown).
Decreases in neutrophil counts were observed in 114 (87.7%) patients; the majority of patients had a grade 1 or 2 decrease, with 22.3% of patients with a grade 3 event and 4.6% of patients with a grade 4 event (Table 3). Neutrophil counts typically reached nadir between two and four weeks after the start of treatment, and remained depressed and stable throughout the dosing period (Supplemental Figure 5). Less than 10% of patients received hematopoietic growth factor support (data not shown). One patient experienced febrile neutropenia; this occurred during the study follow-up period (19 days after discontinuation of abemaciclib) and 8 days after the patient began cytotoxic chemotherapy (fluorouracil and vinorelbine). Forty-one patients (31.1%) experienced an infection, the majority of which were low-grade; there did not appear to be a relationship between the occurrence of severe neutropenia and the occurrence of infection.
Dose reductions due to AEs occurred in 65 (49.2%) patients (46 patients had 1 dose reduction, 18 patients had 2, and 1 patient had 3); dose reductions were most often due to diarrhea (n=27, 20.5%), or neutropenia (n=14, 10.6%). Fifty of the 65 patients (76.9%) who required a dose reduction did so within the first 3 cycles. Dose omissions due to AEs occurred in 76 (57.6%) patients, and were most often due to diarrhea (n=32, 24.2%) or neutropenia (n=21, 15.9%). Omissions were typically short; for patients who required a dose omission, the median number of doses missed on treatment was 6.5% of the assigned regimen, resulting in a median relative dose intensity of 89.2% (Q1–Q3: 71.6–98.0). Discontinuations due to AEs were infrequent (n=10, 7.6%). The majority of patients in MONARCH 1 went on to receive further cytotoxic chemotherapy (Supplemental Table 1).
Discussion
The MONARCH 1 study showed that abemaciclib as a single agent had clinical activity in patients with HR+/HER2- MBC who had received prior chemotherapy in the metastatic setting, with an ORR of 19.7% (95% CI: 13.3, 27.5; 15% not excluded), a CBR of 42.4% and a median PFS of 6.0 months. The median DoR was 8.6 months and the median time to response was 3.7 months. Although the lower bound of the 95% CI for the ORR did not exclude 15%, when evaluated alongside historical data, the ORR observed in MONARCH 1 was consistent with the approximate ORR range of 10–20% observed with approved cytotoxic chemotherapy treatments in taxane-pretreated patients with MBC.6–11
The safety profile of abemaciclib as a single agent was consistent with previous phase 1 observations.22 The most frequent TEAE reported was diarrhea, which generally occurred in the first treatment cycle. Although dose reductions and omissions were most commonly due to diarrhea, most patients with an AE of diarrhea did not require a dose modification due to it; many patients received antidiarrheal medications as indicated in the protocol. This, along with the generally limited duration of diarrhea, suggests that in many cases, diarrhea was manageable. Abemaciclib administration was not associated with a high incidence of grade 4 neutropenia even though patients in MONARCH 1 had received prior treatment with multiple lines of cytotoxic chemotherapy. Severe neutropenia was not temporally associated with an increased risk of infection.
When considering other CDK4 and CDK6 inhibitors, palbociclib and ribociclib are administered for 21 consecutive days followed by a 7 day break, with neutropenia as a DLT, while abemaciclib is administered on a continuous schedule with a DLT of grade 3 fatigue.22,29–31 The ORR for single agent palbociclib in a phase 2 trial was 6% in patients with HR+ MBC.32 In a phase 1 study evaluating the single agent activity of ribociclib, one PR was observed in a patient with ER+ breast cancer in a cohort of 18 patients with MBC.31 Taken together, these studies suggest that abemaciclib may have a different clinical activity profile characterized by a different DLT, and single agent activity.
In enzymatic assays, abemaciclib is 14 times more potent against CDK4/Cyclin D1 than CDK6/Cyclin D3.21 The relative contribution of CDK4 and CDK6 to cell cycle entry and progression differs in a context dependent manner and CDK4 and Cyclin D1 are particularly important for breast tumorigenesis, while CDK6 and Cyclin D3 have critical roles in hematopoietic stem cell differentiation.15,20,33–36 Thus, the differential potency of abemaciclib for CDK4 vs CDK6 could help explain why abemaciclib is not associated with a DLT of myelosuppression and therefore can be dosed on a continuous schedule. Moreover, in vivo and in vitro studies have shown that sustained inhibition of CDK4 and CDK6 and consequent cell cycle arrest leads to shrinkage of HR+ breast cancers in xenograft models, while shorter term inhibition of CDK4 and CDK6 leads to temporary cell cycle arrest with a rebound induction of DNA synthesis on withdrawal.37,38 Thus, the ability to dose abemaciclib on a continuous schedule may have clinical implications. Understanding the potential relationship between sustained target inhibition and clinical activity warrants further exploration, including investigation of potential biomarkers to predict or characterize responses to treatment.39
In current practice, patients who have endocrine refractory or symptomatic visceral HR+ MBC are typically treated with cytotoxic chemotherapy that provides ORRs from 10 to 20% with median DoRs between 4 and 6 months.1,2,6–11,40,41 Chemotherapy can be associated with toxicity impacting quality of life, including alopecia, hand-foot syndrome, nausea/vomiting, grade 3–4 neutropenia, thrombocytopenia, anemia, febrile neutropenia, and peripheral neuropathy.13 Although a direct comparison with chemotherapy in this setting has not been done, the ORR of 19.7% (95% CI: 13.3, 27.5; 15% not excluded) observed with single agent abemaciclib in MONARCH 1 is consistent with the approximate ORR range historically observed in approved chemotherapy treatments for patients who have previously received a taxane, with a safety profile consistent with previous phase 1 observations.22
In conclusion, the MONARCH 1 study has demonstrated that abemaciclib as a single agent dosed on a continuous schedule has antitumor activity and manageable toxicities in patients with HR+ HER2− MBC who had previously progressed on or after endocrine therapy and received 1–2 lines of chemotherapy in the metastatic setting. The future role of abemaciclib in the therapy of HR+ MBC will be delineated by a number of clinical trials, and two ongoing phase 3 trials are investigating abemaciclib in combination with endocrine therapy in the first- and second-line settings (NCT02246621 and NCT02107703).
Supplementary Material
Translational Relevance.
This trial is the first phase 2 study to report single agent activity of abemaciclib, a selective inhibitor of CDK4 and CDK6, in patients with HR+/HER2− MBC who have progressed on or after prior endocrine therapy and received chemotherapy in the metastatic setting. The safety profile allows for dosing on a continuous schedule. The demonstration of single agent activity of abemaciclib is novel in this patient population, whose treatment options are typically limited to chemotherapy. Although these patients have tumors that are initially responsive to endocrine therapy, HR+/HER2- MBC eventually develops disease progression requiring the need for cytotoxic therapy. Single agent activity with a CDK 4 and 6 inhibitor represents a major advance in therapy of treatment-refractory HR+/HER2− MBC, and targeted agents such as abemaciclib may be the next generation of agents for this otherwise poor prognosis patient population.
Acknowledgments
We thank the patients and their caregivers for participating in this trial. We also thank the investigators and their support staff who generously participated in this work. Karen T. Smith and Susan P. Whitman, employees of Eli Lilly and Company, provided medical writing support.
Footnotes
Financial support: This study was funded by Eli Lilly and Company. MND has funding from the National Cancer Institute (P30 CA008748).
References
- 1.National Comprehensive Cancer Network N. Invasive Breast Cancer. 2016. (NCCN Guidelines Version 1). [Google Scholar]
- 2.Rugo HS, Rumble RB, Macrae E, Barton DL, Connolly HK, Dickler MN, et al. Endocrine Therapy for Hormone Receptor-Positive Metastatic Breast Cancer: American Society of Clinical Oncology Guideline. J Clin Oncol. 2016;34:3069–3103. doi: 10.1200/JCO.2016.67.1487. [DOI] [PubMed] [Google Scholar]
- 3.Piccart M, Hortobagyi GN, Campone M, Pritcard KI, Lebrun F, Ito Y, et al. Everolimus plus exemestane for hormone-receptor-positive, human epidermal growth factor receptor-2-negative advanced breast cancer: overall survival results from BOLERO-2dagger. Ann Oncol. 2014;25:2357–2362. doi: 10.1093/annonc/mdu456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Yardley DA, Noguchi S, Pritchard KI, Burris HA, 3rd, Baselga J, Gnant M, et al. Everolimus plus exemestane in postmenopausal patients with HR(+) breast cancer: BOLERO-2 final progression-free survival analysis. Adv Ther. 2013;30:870–884. doi: 10.1007/s12325-013-0060-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dickler MBA, Mayer I, Winer E, Rix P, Hager J, Chen M, Chan I, Chow-Maneval E, Arteaga C, Baselga J. A first-in-human phase I study to evaluate the oral selective estrogen receptor degrader GDC-0810 (ARN-810) in postmenopausal women with estrogen receptor+ HER2−, advanced/metastatic breast cancer; Proceedings of the 106th Annual Meeting of the American Association for Cancer Research; Philadelphia, PA: Cancer Research; 2015. p. CT231. [Google Scholar]
- 6.Cortes J, O’Shaughnessy J, Loesch D, Blum JL, Vahdat LT, Petrakova K, et al. Eribulin monotherapy versus treatment of physician’s choice in patients with metastatic breast cancer (EMBRACE): a phase 3 open-label randomised study. Lancet. 2011;377:914–923. doi: 10.1016/S0140-6736(11)60070-6. [DOI] [PubMed] [Google Scholar]
- 7.HALAVEN® [package insert] Eisai Inc; WL, NJ: Accessed May 17, 2016. [Google Scholar]
- 8.IXEMPRA® [package insert] Bristol-Myers Squibb Company P; NJ: Accessed May 17, 2016. [Google Scholar]
- 9.Perez EA, Lerzo G, Pivot X, Thomas E, Vahdat L, Bosserman L, et al. Efficacy and safety of ixabepilone (BMS-247550) in a phase II study of patients with advanced breast cancer resistant to an anthracycline, a taxane, and capecitabine. J Clin Oncol. 2007;25:3407–3414. doi: 10.1200/JCO.2006.09.3849. [DOI] [PubMed] [Google Scholar]
- 10.XELODA® [package insert] Genentech USA Inc; SSF, CA: Accessed May 17, 2016. [Google Scholar]
- 11.Kaufman PA, Awada A, Twelves C, Yelle L, Perez EA, Velikova G, et al. Phase III open-label randomized study of eribulin mesylate versus capecitabine in patients with locally advanced or metastatic breast cancer previously treated with an anthracycline and a taxane. J Clin Oncol. 2015;33:594–601. doi: 10.1200/JCO.2013.52.4892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gupta S, Zhang J, Jerusalem G. The association of chemotherapy versus hormonal therapy and health outcomes among patients with hormone receptor-positive, HER2-negative metastatic breast cancer: experience from the patient perspective. Expert Rev Pharmacoecon Outcomes Res. 2014;14:929–940. doi: 10.1586/14737167.2014.949243. [DOI] [PubMed] [Google Scholar]
- 13.Twelves C, Jove M, Gombos A, Awada A. Cytotoxic chemotherapy: Still the mainstay of clinical practice for all subtypes metastatic breast cancer. Crit Rev Oncol Hematol. 2016;100:74–87. doi: 10.1016/j.critrevonc.2016.01.021. [DOI] [PubMed] [Google Scholar]
- 14.Vidula N, Rugo HS. Cyclin-Dependent Kinase 4/6 Inhibitors for the Treatment of Breast Cancer: A Review of Preclinical and Clinical Data. Clin Breast Cancer. 2016;16:8–17. doi: 10.1016/j.clbc.2015.07.005. [DOI] [PubMed] [Google Scholar]
- 15.Malumbres M, Barbacid M. Cell cycle, CDKs and cancer: a changing paradigm. Nat Rev Cancer. 2009;9:153–166. doi: 10.1038/nrc2602. [DOI] [PubMed] [Google Scholar]
- 16.Musgrove EA, Caldon CE, Barraclough J, Stone A, Sutherland RL. Cyclin D as a therapeutic target in cancer. Nat Rev Cancer. 2011;11:558–572. doi: 10.1038/nrc3090. [DOI] [PubMed] [Google Scholar]
- 17.Johnston SR. Enhancing Endocrine Therapy for Hormone Receptor-Positive Advanced Breast Cancer: Cotargeting Signaling Pathways. J Natl Cancer Inst. 2015;107:djv212. doi: 10.1093/jnci/djv212. [DOI] [PubMed] [Google Scholar]
- 18.Altucci L, Addeo R, Cicatiello L, Dauvois S, Parker MG, Truss M, et al. 17beta-Estradiol induces cyclin D1 gene transcription, p36D1-p34cdk4 complex activation and p105Rb phosphorylation during mitogenic stimulation of G(1)-arrested human breast cancer cells. Oncogene. 1996;12:2315–2324. [PubMed] [Google Scholar]
- 19.Prall OW, Sarcevic B, Musgrove EA, Watts CK, Sutherland RL. Estrogen-induced activation of Cdk4 and Cdk2 during G1-S phase progression is accompanied by increased cyclin D1 expression and decreased cyclin-dependent kinase inhibitor association with cyclin E-Cdk2. J Biol Chem. 1997;272:10882–10894. doi: 10.1074/jbc.272.16.10882. [DOI] [PubMed] [Google Scholar]
- 20.Miller TW, Balko JM, Fox EM, Ghazoui Z, Dunbier A, Anderson H, et al. ERalpha-dependent E2F transcription can mediate resistance to estrogen deprivation in human breast cancer. Cancer Discov. 2011;1:338–351. doi: 10.1158/2159-8290.CD-11-0101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lallena MJ, Boehnke K, Torres R, Hermoso A, Amat J, Calsina B, De Dios A, Buchanan S, Du J, Beckmann RP, Gong X, Mcnulty A. In-vitro characterization of Abemaciclib pharmacology in ER+ breast cancer cell lines; Proceedings of the 106th Annual Meeting of the American Association for Cancer Research; 2015. p. 3101. [Google Scholar]
- 22.Patnaik ARL, Tolaney SM, Tolcher AW, Goldman JW, Gandhi L, Papadopoulos KP, et al. Efficacy and Safety of Abemaciclib, an Inhibitor of CDK4 and CDK6, for Patients with Breast Cancer, Non–Small Cell Lung Cancer, and Other Solid Tumors. Cancer Discov. 2016;6:740–753. doi: 10.1158/2159-8290.CD-16-0095. [DOI] [PubMed] [Google Scholar]
- 23.Eisenhauer EA, Therasse P, Bogaerts J, Scwartz LH, Sarget D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 11) Eur J Cancer. 2009;45:228–247. doi: 10.1016/j.ejca.2008.10.026. [DOI] [PubMed] [Google Scholar]
- 24.Hammond MEM, Hayes DF, Dowsett M, Allred DC, Hagerty KL, Badve S, et al. American Society of Clinical Oncology/College of American Pathologists Guideline Recommendations for Immunohistochemical Testing of Estrogen and Progesterone Receptors in Breast Cancer. J Clin Oncol. 2010;28:2784–2795. doi: 10.1200/JCO.2009.25.6529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Smith TJ, Bohlke K, Lyman GH, Carson KR, Crawford J, Cross SJ, et al. Recommendations for the Use of WBC Growth Factors: American Society of Clinical Oncology Clinical Practice Guideline Update. J Clin Oncol. 2015;33:3199–3212. doi: 10.1200/JCO.2015.62.3488. [DOI] [PubMed] [Google Scholar]
- 26.NCI. Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0. http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdf.
- 27.Onopiuk A, Tokarzewicz A, Gorodkiewicz E. Cystatin C: a kidney function biomarker. Adv Clin Chem. 2015;68:57–69. doi: 10.1016/bs.acc.2014.11.007. [DOI] [PubMed] [Google Scholar]
- 28.Inker LA, Schmid CH, Tighiouart H, Eckfeldt JH, Feldman HI, Greene T, et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med. 2012;367:20–29. doi: 10.1056/NEJMoa1114248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Flaherty KT, Lorusso PM, Demichele A, Abramson VG, Courtney R, Randolph SS, et al. Phase I, dose-escalation trial of the oral cyclin-dependent kinase 4/6 inhibitor PD 0332991, administered using a 21-day schedule in patients with advanced cancer. Clin Cancer Res. 2012;18:568–576. doi: 10.1158/1078-0432.CCR-11-0509. [DOI] [PubMed] [Google Scholar]
- 30.IBRANCE® [package insert] Pfizer INY; NY: Feb, 2016. Accessed June 2, 2016. [Google Scholar]
- 31.Infante SG, JR, Witteveen P, Gerecitano JF, Ribrag V, Chugh R, Issa I, Chakraborty A, Matano A, Zhao X, Parasuraman S, Cassier P. A phase I study of the single-agent CDK4/6 inhibitor LEE011 in pts with advanced solid tumors and lymphomas. J Clin Oncol. 2014;(suppl 32) 5s abstr 2528. [Google Scholar]
- 32.DeMichele A, Clark AS, Tan KS, Heitjan DF, Gramlich K, Gallagher M, et al. CDK 4/6 inhibitor palbociclib (PD0332991) in Rb+ advanced breast cancer: phase II activity, safety, and predictive biomarker assessment. Clin Cancer Res. 2015;21:995–1001. doi: 10.1158/1078-0432.CCR-14-2258. [DOI] [PubMed] [Google Scholar]
- 33.Yu Q, Geng Y, Sicinski P. Specific protection against breast cancers by cyclin D1 ablation. Nature. 2001;411:1017–1021. doi: 10.1038/35082500. [DOI] [PubMed] [Google Scholar]
- 34.Yu Q, Sicinska E, Geng Y, AhnstrÖm M, Zagozdzon A, Kong Y, et al. Requirement for CDK4 kinase function in breast cancer. Cancer Cell. 2006;9:23–32. doi: 10.1016/j.ccr.2005.12.012. [DOI] [PubMed] [Google Scholar]
- 35.Laurenti E, Frelin C, Xie S, Ferrari R, Dunant CF, Zandi S, et al. CDK6 levels regulate quiescence exit in human hematopoietic stem cells. Cell Stem Cell. 2015;16:302–313. doi: 10.1016/j.stem.2015.01.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Scheicher R, Hoelbl-Kovacic A, Bellutti F, Tigan AS, Prchal-Murphy M, Heller G, et al. CDK6 as a key regulator of hematopoietic and leukemic stem cell activation. Blood. 2015;125:90–101. doi: 10.1182/blood-2014-06-584417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.O’Brien NACD, Luo T, Kalous O, Euw EV, Hurvitz SA, Beckmann RP, Mockbee C, Slamon DJ. Preclinical activity of abemaciclib as a single agent or in combination with anti-mitotic or targeted therapies for breast cancer; Proceedings of the 107th Annual Meeting of the American Association for Cancer Research; New Orleans, LA, USA. 2016. p. 2828. [Google Scholar]
- 38.Gelbert LM, Cai S, Lin X, Sanchez-Martinez C, Del Prado M, Lallena MJ, et al. Preclinical characterization of the CDK4/6 inhibitor LY2835219: in-vivo cell cycle-dependent/independent anti-tumor activities alone/in combination with gemcitabine. Invest New Drugs. 2014;32:825–837. doi: 10.1007/s10637-014-0120-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Tolaney SMCJ, Dickler MN, Zamora E, Caldwell CW, Nguyen TS, Nanda S, Koustenis A, Rugo HS. Exploratory biomarkers in MONARCH 1, a phase II study of abemaciclib monotherapy in hormone-receptor positive (HR+) HER2− metastatic breast cancer (MBC), European Society for Medical Oncology Congress, Copenhagen, Denmark. 2016;27:1–36. [Google Scholar]
- 40.Johnston SR. The role of chemotherapy and targeted agents in patients with metastatic breast cancer. Eur J Cancer. 2011;47(Suppl 3):S38–47. doi: 10.1016/S0959-8049(11)70145-9. [DOI] [PubMed] [Google Scholar]
- 41.Swallow E, Zhang J, Thomason D, Tan RD, Kageleiry A, Signorovitch J. Real-world patterns of endocrine therapy for metastatic hormone-receptor-positive (HR+)/human epidermal growth factor receptor-2-negative (HER2−) breast cancer patients in the United States: 2002–2012. Curr Med Res Opin. 2014;30:1537–1545. doi: 10.1185/03007995.2014.908829. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.