

Over the past several decades, the surgical approach to primary hyperparathyroidism (PHPT) has shifted to minimally invasive parathyroidectomy (MIP) in lieu of the traditional four-gland bilateral neck exploration. However, the success of MIP hinges on the ability to localize the adenomatous gland via imaging before the operation. Four-dimensional computed tomography (4D-CT) has increasingly been used for preoperative localization of adenomatous parathyroid glands in patients with PHPT.1 This technique combines standard multiplanar CT scanning with a fourth dimension consisting of changes in contrast attenuation over time. As a result, 4D-CT scanning provides both functional and anatomic information about the abnormal gland, while also permitting unbiased detection of ectopic glands or multiglandular disease that may be missed by other imaging modalities.1,2
The available literature has not yet reached a consensus on the optimal 4D-CT scanning protocol for parathyroid imaging; however, many authors describe a three- or four-phase imaging protocol consisting of precontrast, arterial (25 to 30 seconds after contrast injection), early-delayed (45 seconds after contrast injection), and late-delayed (80 to 90 seconds after contrast injection) phases (figure 1, A–C).1–3
Figure 1.
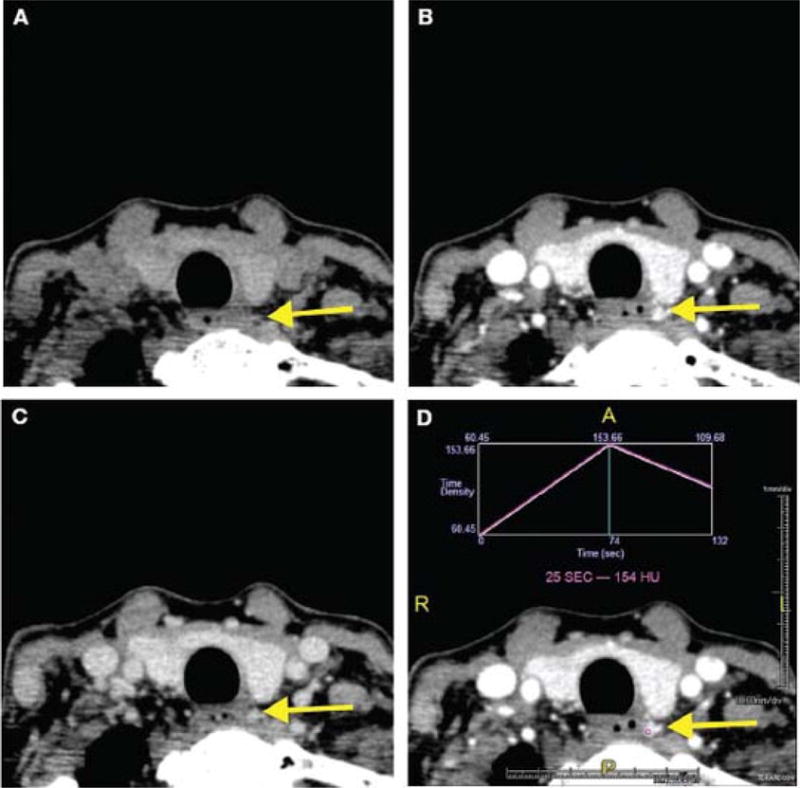
Single axial, 1-mm 4D-CT images show the precontrast phase (A), arterial phase (B), and delayed phase (C). Panel (D) shows a time-attenuation curve demonstrating rapid contrast enhancement and washout from the adenomatous gland.
Adenomatous glands characteristically have low attenuation on the precontrast phase, maximal contrast enhancement during the arterial phase, and rapid washout during the delayed phases (figure 1, D). By contrast, normal parathyroid glands typically exhibit less contrast enhancement than the adenomatous gland during the arterial phase.2 Additionally, 4D-CT scanning may identify a polar feeding vessel, termed the “polar vessel sign,” in up to 63% of adenomas.4 The presence of this sign significantly increases the likelihood that the identified gland is an adenoma.4
Based on these characteristic findings, 4D-CT scanning has a reported sensitivity of 60 to 87% in localizing an adenoma to a quadrant when used as a first-line imaging study.3 By comparison, the most commonly used first-line imaging modalities, Tc99m-sestamibi scanning and ultrasound, have reported sensitivities ranging from 68 to 95% and 72 to 89%, respectively.5 However, despite sound radiographic technique, a subset of parathyroid adenomas cannot be localized by ultrasound or sestamibi scanning.6
Brown et al reported that among instances in which an abnormal gland was not identified by sestamibi scanning, 4D-CT correctly identified the abnormal gland in 80% of cases (figure 2).7 Similarly, in patients undergoing reoperation, 4D-CT scanning correctly identified the abnormal gland in 91% of cases, compared to 45% for sestamibi scanning.7
Figure 2.
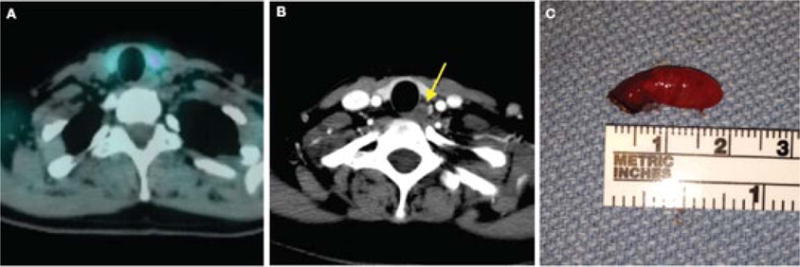
Images from a Tc99m-sestamibi single positron-emission CT (SPECT) scan (A) and a 4D-CT scan (B) for the same patient with primary hyperparathyroidism are shown. SPECT fails to localize the parathyroid gland, but the gland is readily apparent on 4D-CT scanning (arrow). The parathyroid adenoma has been excised by MIP (C).
Using cost estimates based on Medicare national reimbursement data from 2011 and sensitivity data of different imaging modalities based on a review of the literature, Lubitz et al demonstrated that the most cost-effective strategy for localizing parathyroid adenomas was to combine ultrasound with 4D-CT.8 Interestingly, ultrasound alone or 4D-CT alone was more expensive than using both modalities in combination.8 A retrospective economic analysis among patients who all underwent ultrasound and sestamibi scan demonstrated that those who also underwent 4D-CT had a shorter length of stay and were less likely to undergo bilateral neck exploration.9 Therefore, the use of 4D-CT scanning may reduce costs and morbidity associated with parathyroidectomy.
Despite the utility of 4D-CT in localizing parathyroid adenomas, concerns over the increased radiation dosage associated with the technique have limited its widespread use. When compared to sestamibi scanning, 4D-CT results in significantly higher radiation doses to the head and neck, which may be associated with an increased lifetime risk of thyroid cancer based on modeling from the Biological Effects of Ionizing Radiation Committee VII report, particularly among young women.10,11
To decrease the risk of iatrogenic cancers associated with 4D-CT, several groups have used one- or two-phase imaging protocols to identify parathyroid adenomas. These protocols consist of an arterial phase alone, an unenhanced and an arterial phase, or an arterial and a venous phase. The modified protocols have localization accuracies similar to those of traditional three- and four-phase imaging protocols while imparting significantly lower radiation dosages. 12,13 Accordingly, eliminating the unenhanced phase of imaging in certain patients may reduce the risk of iatrogenic cancer without compromising the ability of CT scanning to identify parathyroid adenomas.
In conclusion, 4D-CT scanning is a highly accurate method to identify parathyroid adenomas, and modifications to previously published protocols may reduce the radiation risk associated with multiphase CT scanning to levels similar to those of other parathyroid imaging modalities. Additionally, the use of 4D-CT scanning may be both cost-effective and associated with shorter hospital stays.
Acknowledgments
We gratefully acknowledge NCI grant F30 CA 165774 for providing funding to Dr. Bann.
References
- 1.Rodgers SE, Hunter GJ, Hamberg LM, et al. Improved preoperative planning for directed parathyroidectomy with 4-dimensional computed tomography. Surgery. 2006;140(6):932–40. doi: 10.1016/j.surg.2006.07.028. [DOI] [PubMed] [Google Scholar]
- 2.Chazen JL, Gupta A, Dunning A, Phillips CD. Diagnostic accuracy of 4D-CT for parathyroid adenomas and hyperplasia. AJNR Am J Neuroradiol. 2012;33(3):429–33. doi: 10.3174/ajnr.A2805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hoang JK, Sung WK, Bahl M, Phillips CD. How to perform parathyroid 4D CT: Tips and traps for technique and interpretation. Radiology. 2014;270(1):15–24. doi: 10.1148/radiol.13122661. [DOI] [PubMed] [Google Scholar]
- 4.Bahl M, Muzaffar M, Vij G, et al. Prevalence of the polar vessel sign in parathyroid adenomas on the arterial phase of 4D CT. AJNR Am J Neuroradiol. 2014;35(3):578–81. doi: 10.3174/ajnr.A3715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Johnson NA, Carty SE, Tublin ME. Parathyroid imaging. Radiol Clin North Am. 2011;49(3):489–509. vi. doi: 10.1016/j.rcl.2011.02.009. [DOI] [PubMed] [Google Scholar]
- 6.Payne SJ, Smucker JE, Bruno MA, et al. Radiographic evaluation of non-localizing parathyroid adenomas. Am J Otolaryngol. 2015;36(2):217–22. doi: 10.1016/j.amjoto.2014.10.036. [DOI] [PubMed] [Google Scholar]
- 7.Brown SJ, Lee JC, Christie J, et al. Four-dimensional computed tomography for parathyroid localization: A new imaging modality. ANZ J Surg. 2014 Mar 27; doi: 10.1111/ans.12571. doi:10.1111.ans.12571. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 8.Lubitz CC, Stephen AE, Hodin RA, Pandharipande P. Preoperative localization strategies for primary hyperparathyroidism: An economic analysis. Ann Surg Oncol. 2012;19(13):4202–9. doi: 10.1245/s10434-012-2512-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Abbott DE, Cantor SB, Grubbs EG, et al. Outcomes and economic analysis of routine preoperative 4-dimensional CT for surgical intervention in de novo primary hyperparathyroidism: Does clinical benefit justify the cost? J Am Coll Surg. 2012;214(4):629–37. doi: 10.1016/j.jamcollsurg.2011.12.022. [DOI] [PubMed] [Google Scholar]
- 10.National Research Council (U.S.). Committee to Assess Health Risks from Exposure to Low Levels of Ionizing Radiation. Health risks from exposure to low levels of ionizing radiation: BEIR VII Phase 2. Washington, D.C.: National Academies Press; 2006. www.nap.edu/catalog/11340/health-risks-from-exposure-to-low-levels-of-ionizing-radiation/( http://www.nap.edu/catalog/11340/health-risks-from-exposure-to-low-levels-of-ionizing-radiation/). Accessed February 24, 2015. [PubMed] [Google Scholar]
- 11.Mahajan A, Starker LF, Ghita M, et al. Parathyroid four-dimensional computed tomography: Evaluation of radiation dose exposure during preoperative localization of parathyroid tumors in primary hyperparathyroidism. World J Surg. 2012;36(6):1335–9. doi: 10.1007/s00268-011-1365-3. [DOI] [PubMed] [Google Scholar]
- 12.Gafton AR, Glastonbury CM, Eastwood JD, Hoang JK. Parathyroid lesions: Characterization with dual-phase arterial and venous enhanced CT of the neck. AJNR Am J Neuroradiol. 2012;33(5):949–52. doi: 10.3174/ajnr.A2885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Raghavan P, Durst CR, Ornan DA, et al. Dynamic CT for parathyroid disease: Are multiple phases necessary? AJNR Am J Neuroradiol. 2014;35(10):1959–64. doi: 10.3174/ajnr.A3978. [DOI] [PMC free article] [PubMed] [Google Scholar]