

Abstract
Objective:
Placental transmogrification of the lung (PTL) is rare cystic lesion. Thus, we summarized the characteristics of PTL to explore the strategy of diagnosis and treatment.
Methods:
Two patients pathologically confirmed PTL were treated in our hospital. Retrospectively analysis was performed on such 2 cases and 34 cases of PTL reported in abroad. The basic information and clinical characteristics from each patient were gathered and analyzed.
Results:
The imaging findings of 2 patients were the pulmonary solid mass with peripheral multiple pulmonary bullae. After the improvement of preoperative examination and the multidisciplinary discussion of thoracic surgery, respiration, imaging, and anesthesia, the possibility of benign pulmonary lesions was improved in all cases. Thoracoscopic lobectomy was carried out under general anesthesia, and the intraoperative frozen pathology showed bullae of lung. Ultimately, PTL was confirmed by paraffin pathological diagnosis. Both 2 PTL patients had satisfied recovery without obvious complications or imaging abnormalities. In addition, the literature review of 34 PTL cases from PubMed database was summarized between 1995 and 2015. A total of 36 patients were retrospectively analyzed in our study. The age of 34 cases ranged from 24 to 72 years (an average age of 45.6 ± 13.5 years). Among these, 8 cases were no obvious symptoms. In addition, the other 25 cases had respiratory symptoms such as chest tightness, cough, and chest pain. Moreover, the mean size of pulmonary bulla was 6.5 ± 5.5 cm. The size of the solid lesions in 23 cases was 3.3 ± 3.4 cm (ranging from 0.5 to 15). The follow-up period was 2 to 96 months (average 27.3 ± 29.8 months).
Conclusion:
Early diagnosis and surgical operation of PTL should be performed as soon as possible. These lesions are best treated by minimally invasive surgery, so as to preserve more normal lung tissue and avoid the pneumonectomy.
Keywords: bullous emphysema, image feature, operation, pathology feature, placental transmogrification of the lung
1. Introduction
Placental transmogrification of the lung (PTL) is a rare cystic lesion of the lung, which is first described in 1979 by McChesney.[1] Although it does not bear any biological and biochemical properties of a placenta, it is so named because morphologically it resembles immature placental structures. Moreover, it is also considered as a histologic variant of unilateral bullous emphysema.[2,3] However, the pathogenesis of the lesion has not been intensively studied.
Relevant keywords were retrieved in the PubMed database, covering all the papers published until February 1, 2017, and a total of 34 studies about the cases of PTL were detected.[2–18] Nevertheless, no relevant reports were found in China yet. After searching a large number of medical records, we found the clinical pathology and follow-up data of 2 patients with PTL confirmed by pathology in our hospital, to provide a reference for clinicians in the treatment of PTL.
In recent years, the number of studies relevant to PTL was relatively small, resulting in limited sample size for statistical analysis to clarify the clinical characteristics of this disease. Hence, the statistical analysis of these data could be more accurate and objective to provide more evidence, which is very important for clinicians. Therefore, we performed a systematic review, in order to describe the clinical characteristics of PTL, and sum up the best diagnosis and treatment strategies.
2. Methods and results
2.1. Ethic approval
This study was approved by The Institutional Review Board of Ethics Committee of Peking Union Medical College Hospital. All participants received written and oral information before giving written consent, and the study was performed in accordance with the Helsinki II declaration.
2.2. Clinical findings
2.2.1. Case report 1
A 59-year-old man presented chest tightness for a month. He was a 40-pack-year smoker without other neoplastic diseases. Computed tomography (CT) of the chest was performed, and revealed the soft tissue mass of the right lower lung, measuring 3.8 cm × 2.33 cm; CT value: −31Hu to 58Hu. Besides, the edge of the tumor was clear, and the shallow lobe with multiple peripheral pulmonary bullae was found. In addition, tumor marker: carcinoembryonic antigen (5.22 ng/mL), neuron specific enolase (19.9 ng/mL), and tissue polypeptide specific antigen (89.02 U/L) were slightly elevated. However, blood biochemical examination and sputum culture were normal. Physical examination indicated normal lung function. Therefore, we considered the possibility of benign lesions, bronchiectasis, lung cyst, or emphysematous bullae.
The patient underwent a thoracoscopic right lower lobectomy on January 12, 2016. In the operation, the lower right lung mass was found on the surface of the lung, without adhesion, pleural shrinkage, or giant pulmonary bulla. The frozen pathology showed that the diagnosis was consistent with pulmonary bulla. However, it is necessary to obtain the result of paraffin pathology, because of the limitation of the frozen material. Because the mass profile was similar to that of a clustered cluster of mucus like vesicles, it is impossible to exclude the mucinous adenocarcinoma. So the patient underwent systemic lymph node dissection. Besides, the surgery time was 120 minutes and blood loss was 100 mL. Paraffin pathology showed that the right lower lung tumor was consistent with PTL. No special abnormality was found in the bronchial stump, and chronic inflammation of the lymph nodes (0/19). Immunohistochemistry results were as follows: CD10 (+), CD117 (scattered+), AE1/AE3 (alveolar epithelial+), CD1 (+), CD31 (+), CD34 (partial+). D2–40 (+), desmin (−), ER (−), HMB45 (−), Ki-67 (index-2%), P40 (−), PAX-8 (−), PR (partial+), S-100 (−), SMA (partial+), TTF-1 (+), CD9 (+), TFE3 (−).
2.2.2. Case report 2
A high-density shadow of the right lower lung was found in a 30-year-old woman for 2 months. Enhanced CT scan revealed the soft tissue mass in the right lower segment of the lung with a size of 2.7 cm × 2.5 cm. The edge of the tumor was clear, uneven, and mild, and multiple peripheral pulmonary bullae were found. In addition, the blood biochemical examination and sputum culture were normal, and physical examination revealed normal lung function. The patient complained no obvious discomfort, and had no family history of cancer or history of smoking or drinking. Thus, we considered that the patient had the possibility of benign lesions, hypoplasia of the right lower lung, emphysematous bullae, or sclerosing hemangioma.
The patient underwent the uniportal video assisted thoracoscopic surgery (VATS) thoracoscopic right lower lobectomy with right ventral position on April 5, 2016. The right lower lung tumor with peripheral membrane adhesion and no pleural collapse was found on the surface of the lung in the operation. The frozen pathology showed that the diagnosis was consistent with pulmonary bull, and lymphocytic infiltration was found in lung tissue. Paraffin pathology showed that the right lower lung tumor was consistent with PTL. Besides, the surgery time was 105 minutes and blood loss was 80 mL. There was no special abnormality in the bronchial stump, and chronic inflammation of the lymph nodes (0/8). Immunohistochemistry results were as follows: keratin (+), vimentin (+), CD10 (+), AE1/AE3 (+), CD34 (partial+), D2–40 (+), TTF-1 (+), desmin (−), HMB45 (−), S-100 (−), SMA (−), Ki-67 (index-1%).
All the 2 patients were followed up until now without any obvious discomfort. Moreover, no radiographic abnormalities were found. All studied patients fulfilled the diagnostic criteria of the International Study Group for PTL. Gross and microscopic features of PTL are shown in Fig. 1.
Figure 1.
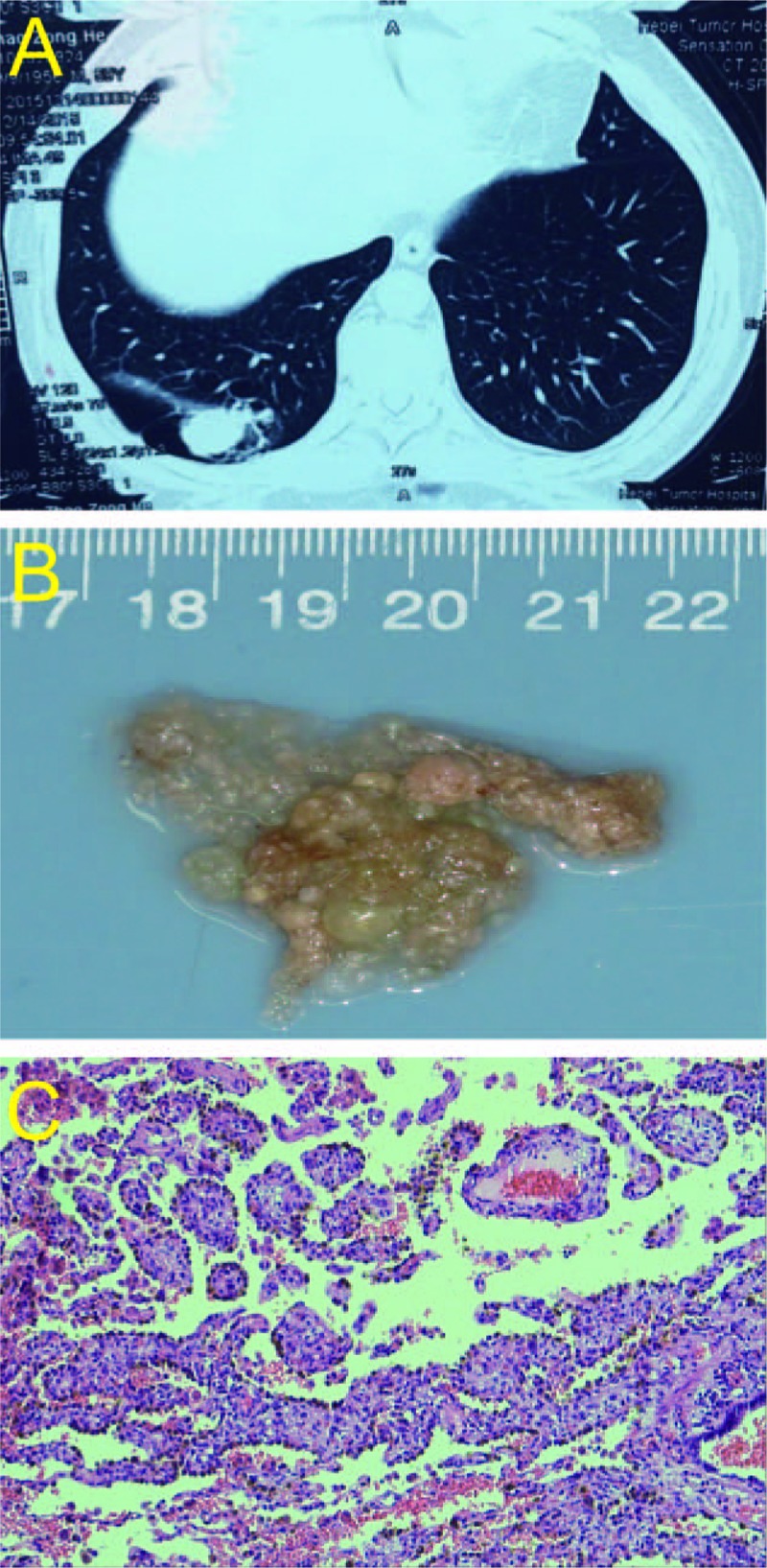
Gross and microscopic features of PTL. (A) CT scan of PTL, the soft tissue mass of the right lower lung, measuring 3.8 cm × 2.33 cm. The edge of the tumor was clear, and the shallow lobe with multiple peripheral pulmonary bullae was found. (B) Gross pathology: well-circumscribed mass with papillary projections, resembling a placenta. (C) Photomicrograph with hematoxylin and eosin staining shows the cystic lesions of the lung containing multiple villous papillary structures similar to placental villi.
2.3. Systematic analysis
As PTL is a rare disease, no randomized controlled studies were retrieved. Demographic and clinical characteristics of patients are shown in Tables 1 and 2. A total of 36 patients were retrospectively analyzed in our study (26 men, and 10 women).[2–18] Two patients were admitted into our hospital. The other 34 cases with complete data were searched from PubMed between 1995 and 2015. The age of 34 cases ranged from 24 to 72 years (an average age of 45.6 ± 13.5 years). Forty-eight percent of patients had a history of smoking. Among these, 8 cases were no obvious symptoms. In addition, 25 cases had respiratory symptoms such as chest tightness, cough, and chest pain. There were pneumothorax (5 cases), bilateral pulmonary emphysema (2 cases), and pulmonary hamartoma (6 cases). Moreover, the mean size of pulmonary bulla was 6.5 ± 5.5 cm. Among them, 12 cases had the relevant data; the available data were not obtained in 17 patients; the pulmonary bullae in other 7 patients were occupied with 50% to 90% of the unilateral pleural. In addition, the size of the solid lesions in 23 cases was 3.3 ± 3.4 cm (ranging from 0.5 to 15). The corresponding distribution of the position of the disease and the choice of operation in 33 patients is listed in Table 3. Among them, 8 cases was unknown surgical procedure; 8 cases underwent VATS; 20 cases were open thoracotomy; only 1 case was converted to thoracotomy, because VATS could not determine the scope of the implementation of lesions. None of the cases who were completely resected the lesion in the literature reappeared. In addition, 3 cases of postoperative residual lesions were found in CT, and the patients with incomplete resection of pulmonary bullae reappeared, only 2 patients were observed follow-up. Moreover, Table 4 shows the choice of operation and prognosis of 28 patients. The follow-up period was 2 to 96 months (average 27.3 ± 29.8 months).
Table 1.
Patient demographic characteristics.
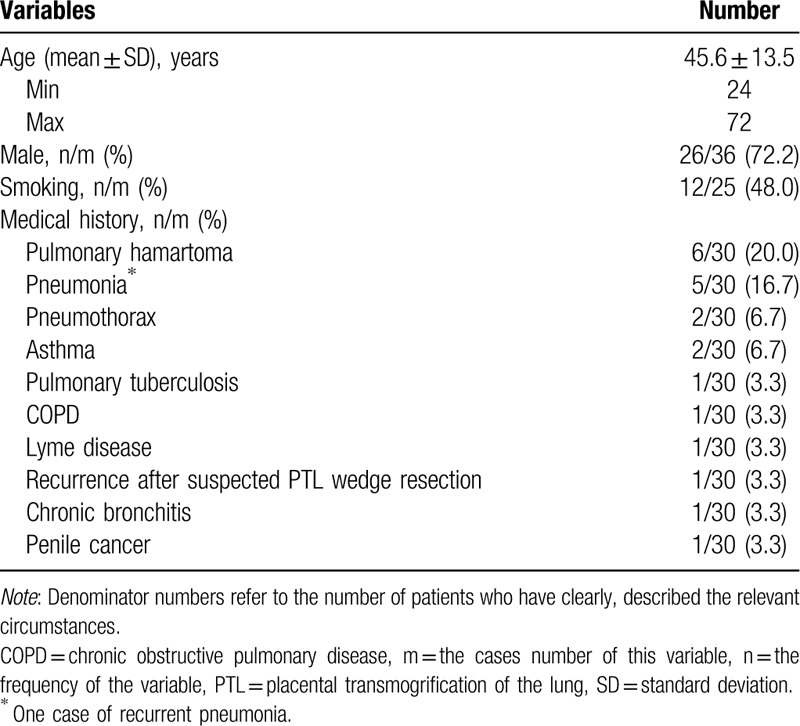
Table 2.
Clinical characteristics of patients.
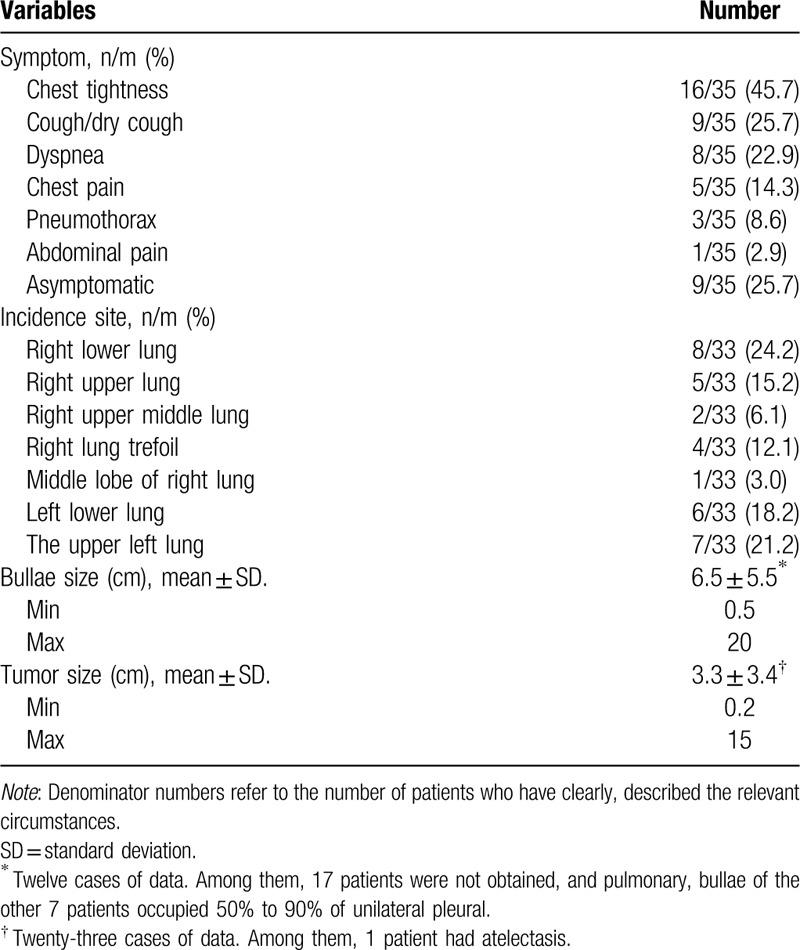
Table 3.
The corresponding distribution of the position of the disease and the choice of operation in 33 patients.
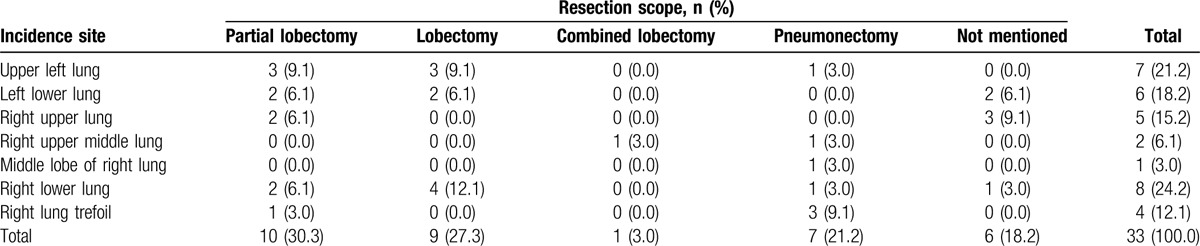
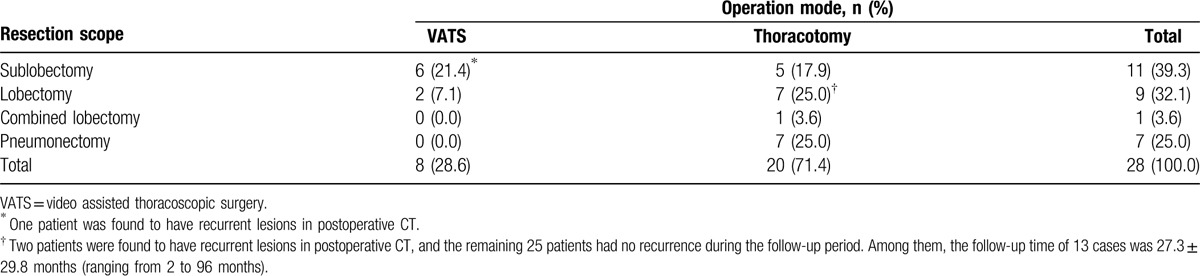
Table 4.
The choice of operation and prognosis of 28 patients.
3. Discussion
PTL is a very rare lesion, and acts as a histologic subtype of bullous emphysema, which radiographically has unilateral giant bullous emphysema with or without an associated nodule in the ipsilateral hemithorax.[1] Till now, only 34 reports of PTL have been published to our knowledge.[2–18] Clinically, placental transmogrification usually occurs in men between 20 and 50 years old.[19,20] In addition, placental transmogrification is associated with both cystic or emphysematous lung lesion and pulmonary fibrochondromatous hamartomas, pulmonary lipomatosis. Thus, the radiologic presentation showed bullous change or pulmonary lung nodules.[18] Patients might be asymptomatic or perhaps present with dyspnea, chest pain, chronic obstructive lung disease, or pneumothorax, or a combination of these.[21] The lesions are occasionally incidental masses seen by radiography.[22,23] Although lung and placenta seem to have nothing in common, they are both gas exchanging organs. However, hypotheses for the etiology and pathogenesis remain unclear. They included congenital hamartomatous malformation and lymphatic or vascular proliferation in emphysematous lung parenchyma.[24,25] Moreover, Cavazza et al[4] suggested that PTL might not be just a variant of focal emphysema, but rather a benign proliferation of immature interstitial clear cells with secondary cystic change.
Grossly, the PTL resembles a placenta or cystic lesions. These areas are replaced or filled by gelatinous tissues described as bubbly, vesicular, grape-like, or sponge like. Differential diagnosis of PTL includes intralobar pulmonary sequestration, congenital cystic adenomatoid malformation, bronchogenic cyst, and cystic lung tumors.[21,24] CT or magnetic resonance imaging could help distinguish these entities from PTL, but final diagnosis requires excisional resection.[25]
According to the analysis of the above literature and our 2 cases, although it is a rare disease, the clinical manifestation of PTL is a circumscribed mass lesion, which is the unilateral localized emphysematous bulla with soft tissue and fat composition. Familiar with its clinical characteristics, it is convenient for surgeon to differentiate malignant tumor and the diseases associated with similar manifestations of imaging, to improve the diagnosis and treatment of patients with PTL, and avoid excessive preoperative examination and the invalid treatment of emphysema.[16,22]
Based on the corresponding distribution of the position of the disease and the choice of operation in 33 patients, 10 PTL cases underwent pulmonary lobectomy, 9 cases underwent lobectomy, and the other 1 case was composite pulmonary lobectomy. Besides, it is worth noting that 7 cases underwent pneumonectomy. The reason is that the lesions, especially the bullae of lung, are involved in the lateral thoracic cavity, which severely damages the normal lung tissue, and makes the mediastinal to lateral displacement. Amongst them, the lesions in 4 cases involved multiple lobes; the other 3 cases originated from a single lobe, but the pulmonary bulla invaded the whole thoracic cavity. It is difficult to make statistical analysis results, because of the limited data of relevant studies without uniform standard. However, based on the current data, we can draw the following conclusions. When the lesions of PTL and the extent of pulmonary bullae are small, the sublobectomy or lobectomy is often selected. In addition, when the lesion of PTL is large, involving a wide range (e.g., involving 2 lobe of the lung in the ipsilateral chest, even 3 lung lobes), especially giant bullae of lung, which severely compressed normal lung tissue, the patients often underwent multiple lobectomy or pneumonectomy. Therefore, surgical resection is the treatment of choice, which is usually curative and successful in improving symptoms and quality of life.[22,23] Meanwhile, it is necessary to cooperate with the anesthesiologist to ensure the normal lung ventilation, thus to accurately determine the normal lung tissue to be preserved and avoid the whole lung resection during the operation. As showed in our report, PTL can result in severe pulmonary symptoms, if left untreated. In addition, It is unfortunately to provide the exact diagnosis in only histologic and immunohistochemical findings. Even if the patients have severe lung involvement and symptoms, we can make an excellent outcome by complete surgical resection. Therefore, we should abandon unnecessary surgical procedures such as lymph node dissection, and guarantee PTL patients the most reasonable surgical strategy and rapid recovery.
Overall, we used the sufficient statistical evidence with the large sample size to estimate such association. However, several limitations were involved in our study. First, in this review, the studies mainly conducted on Caucasians and only a little studies were Asian populations. Besides, no reports were found on the other population available. Hence, more researches should be paid attention to the influence of ethnicity factors in the subsequent studies. Second, there were only 17 studies, thus to weak the reliability of our study. Thus, we should conduct more well-designed studies with large cases to validate the characteristics of PTL and explore the strategy of diagnosis and treatment. In addition, based on unadjusted estimates, so the effect of multiple confounders such as life-style, age, environmental factors, and so on should be taken into consideration. Accordingly, to improve reliability of the study, more researches should need to explore the strategy of diagnosis and treatment of PTL in the future.
4. Conclusion
PTL is a rare benign lesion, characterized by cystic lesions of the lung. Grossly and microscopically, the lesion resembles placental tissue, with formation of placental villus-like papillary structures covered by epithelial cells. The most common imaging manifestation of PTL is a bullous emphysema pattern with a mixed pattern of thin-walled cystic lesions and nodules. Early diagnosis and surgical operation should be performed as soon as possible, these lesions are best treated by minimal resection, to preserve more normal lung tissue and avoid the pneumonectomy as soon as possible. Surgical resection is usually curative and leads to successful improvement of symptoms and quality of life.
Footnotes
Abbreviation: PTL = placental transmogrification of the lung.
The authors have no conflicts of interest to disclose.
References
- [1].McChesney T. Placental transmogrification of the lung: a unique case with remarkable histopathologic feature. Lab Invest 1979;40:245–6. [Google Scholar]
- [2].Fidler ME, Koomen M, Sebek B, et al. Placental transmogrification of the lung, a histologic variant of giant bullous emphysema. Clinicopathological study of three further cases. Am J Surg Pathol 1995;19:563–70. [DOI] [PubMed] [Google Scholar]
- [3].Horsley WS, Gal AA, Mansour KA. Unilateral giant bullous emphysema with placental transmogrification of the lung. Ann Thorac Surg 1997;64:226–8. [DOI] [PubMed] [Google Scholar]
- [4].Cavazza A, Lantuejoul S, Sartori G, et al. Placental transmogrification of the lung: clinicopathologic, immunohistochemical and molecular study of two cases, with particular emphasis on the interstitial clear cells. Hum Pathol 2004;35:517–21. [DOI] [PubMed] [Google Scholar]
- [5].Theile A, Wex P, Müller KM. Placentoid malformation of the lung as differential diagnosis of localized emphysema. Pneumologie 1997;51:550–4. [PubMed] [Google Scholar]
- [6].Dunning K, Chen S, Aksade A, et al. Placental transmogrification of the lung presenting as tension pneumothorax: case report with review of literature. J Thorac Cardiovasc Surg 2008;136:778–80. [DOI] [PubMed] [Google Scholar]
- [7].Shapiro M, Vidal C, Lipskar AM, et al. Placental transmogrification of the lung presenting as emphysema and a lung mass. Ann Thorac Surg 2009;87:615–6. [DOI] [PubMed] [Google Scholar]
- [8].Santana AN, Canzian M, Stelmach R, et al. Placental transmogrification of the lung presenting as giant bullae with soft-fatty components. Eur J Cardiothorac Surg 2008;33:124–6. [DOI] [PubMed] [Google Scholar]
- [9].Kim JW, Park IH, Kwon W, et al. Placental transmogrification of the lung. Korean J Radiol 2013;14:977–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Saito Y, Ikeya T, Hoshi E, et al. Placental transmogrification of the lung presenting as a small solitary nodule. Ann Thorac Surg 2009;87:950–2. [DOI] [PubMed] [Google Scholar]
- [11].Buch A, Kini U. A case report of pulmonary placental transmogrification with review of literature. Indian J Chest Dis Allied Sci 2006;48:147–50. [PubMed] [Google Scholar]
- [12].Ferretti GR, Kocier M, Moro-Sibilot D, et al. Placental transmogrication of the lung: CT-pathologic correlation of a rare pulmonary nodule. AJR Am J Roentgenol 2004;183:99–101. [DOI] [PubMed] [Google Scholar]
- [13].Mohning MP, Schwarz MI, McKinley SJ. Placental transmogrification of the lung: a rare cause of unilateral bullous disease. Am J Respir Crit Care Med 2014;190:e1. [DOI] [PubMed] [Google Scholar]
- [14].Hochhegger B, Camargo S, Camargo J, et al. Placental transmogrification of the lung. Lung 2015;193:855–7. [DOI] [PubMed] [Google Scholar]
- [15].Marchevsky AM, Guintu R, Koss M, et al. Swyer-James (MacLeod) syndrome with placental transmogrification of the lung: a case report and review of the literature. Arch Pathol Lab Med 2005;129:686–9. [DOI] [PubMed] [Google Scholar]
- [16].Kronz JD, Palmer C, Askin FB. Images in pathology. Placental transmogrification of the lung. Arch Pathol Lab Med 1999;123:856. [DOI] [PubMed] [Google Scholar]
- [17].Hochholzer L, Moran CA, Koss MN. Pulmonary lipomatosis: a variant of placental transmogrification. Mod Pathol 1997;10:846–9. [PubMed] [Google Scholar]
- [18].Xu R, Murray M, Jagirdar J, et al. Placental transmogrification of the lung is a histologic pattern frequently associated with pulmonary fibrochondromatous hamartoma. Arch Pathol Lab Med 2002;126:562–6. [DOI] [PubMed] [Google Scholar]
- [19].Mark EJ, Muller KM, McChesney T, et al. Placentoid bullous lesion of the lung. Hum Pathol 1995;26:74–9. [DOI] [PubMed] [Google Scholar]
- [20].Vogel-Claussen J, Kulesza P, Macura KJ. Placental transmogrification of the lung. J Thorac Imaging 2005;20:233–5. [DOI] [PubMed] [Google Scholar]
- [21].Santana AN, Canzian M, Stelmach R, et al. Placental transmogrification of the lung presenting as giant bullae with soft-fatty components. Eur J Cardiothorac Surg 2008;33:124–6. [DOI] [PubMed] [Google Scholar]
- [22].Brevetti GR, Clary-Macy C, Jablons DM. Pulmonary placental transmogrification: diagnosis and treatment. J Thorac Cardiovasc Surg 1999;118:966–7. [DOI] [PubMed] [Google Scholar]
- [23].Brüstle K, Lema S, Komminoth P, et al. Placental transmogrification of the lung presenting as progressive symptomatic bullous emphysema. Thorax 2016;72:284–5. [DOI] [PubMed] [Google Scholar]
- [24].Jenkins JM, Attia RQ, Green A, et al. A case of pulmonary placental transmogrification. Asian Cardiovasc Thorac Ann 2016;24:811–3. [DOI] [PubMed] [Google Scholar]
- [25].Ventura L, Gnetti L, Silini EM, et al. Placental transmogrification of the lung presenting as a giant bulla associated with a pulmonary hamartoma. Ann Thorac Surg 2016;102:e61. [DOI] [PubMed] [Google Scholar]