

Abstract
Background:
This study aimed to determine the efficacy and safety of extracorporeal shock-wave therapy (ESWT) for treating patients with chronic rotator cuff tendonitis (CRCT).
Methods:
In this study, 84 patients with CRCT were randomly divided into intervention and control groups in a ratio of 1:1. Patients in the intervention group received ESWT, whereas those in the control group received placebo. The primary outcome was measured by Numeric Rating Scale (NRS). The secondary outcomes were measured by the Constant-Murley score (CMS), simple shoulder test (SST) score, and adverse events.
Results:
Compared with placebo, ESWT showed greater efficacy in shoulder pain relief with regard to NRS score and shoulder function as measured by using CMS and SST score at 4 weeks (P < .05) and 8 weeks (P < .01) after treatment. However, no adverse events occurred in both groups.
Conclusion:
ESWT was efficacious and safe for treating patients with CRCT.
Keywords: chronic rotator cuff tendonitis, clinical trial, efficacy, extracorporeal shock-wave therapy, safety
1. Introduction
Chronic rotator cuff tendonitis (CRCT) is a common condition in people who often play sports that require extending the arm over the head frequently. It occurs when the tendons and muscles that help to move the shoulder joint are inflamed or irritated. The most common symptoms of CRCT are shoulder pain related to movement, muscular weakness, and mobility reduction.[1] Thus, the shoulder pain results from the inflammation and degenerative changes in rotator cuff tendonitis and the adjacent structures of the shoulder.[1]
The symptoms of CRCT, especially shoulder pain, can be relieved by analgesics, nonsteroidal antiinflammatory drugs (NSAIDs), corticosteroid injection in the local area, physical therapy, and even surgical treatment.[2–7] Unfortunately, limited evidence exists on the efficacy and safety of these therapies in the treatment of CRCT. Thus, an alternative therapy that leads to a few or no adverse events (AEs) is necessary for the management of CRCT.
Extracorporeal shock-wave therapy (ESWT) has been proposed for pain relief in various conditions [8–11] such as tendinitis of the shoulder, lateral epicondylitis of the elbow, and plantar fasciitis.[12–14] CRCT is one of the most common conditions treated with ESWT, although its mechanism remains unclear. ESWT has been reported to be effective for promoting tissue healing through improvement of neovascularization and reduction of local inflammation.[15–18] In addition, although its clinical effects were reported in previous studies, the results remain controversial.[16,19–20]
In this study, we aimed to investigate the efficacy and safety of ESWT for treating patients with CRCT in Chinese population. We hypothesized that for treatment of CRCT, the effect of ESWT would be superior to the effect of placebo.
2. Methods and materials
2.1. Study design
This randomized, double-blinded placebo-controlled trial was approved by the ethics committee of the First Hospital of Harbin City and was conducted at this hospital from February 2015 to January 2017. Eighty-four eligible patients were randomly divided into an intervention group or a control group, each group 42 patients. Patients in the intervention group received ESWT, whereas subjects in the control group received placebo.
2.2. Patients
Patients were included if they met the following criteria: (1) diagnosis of CRCT without calcification by physical examination, ultrasonographic examination, a painful arc, and positive empty can test result; (2) age between 18 and 65 years; (3) a history of clinical signs of chronic tendinitis for more than 6 months; (4) no alternative therapy, including ESWT, within 1 month before enrollment in the study; and (5) informed consent before enrollment in this study. However, patients were excluded if they were pregnant or breastfeeding; blood coagulation disorders, history of surgery, and history or presence of tumors, pacemaker, frozen shoulder, systematic diseases. In addition, those with skin disease, cancer, or severe mental disorders were excluded.
2.3. Randomization and blinding
Randomization schedule was operated by a computerized number generated using SAS package (Version 8.3; SAS Institute Inc., Cary, NC). All patients were randomized to receive ESWT (intervention group) or placebo (control group) at a 1:1 ratio. All information of assignments and allocation were concealed in sequentially numbered, opaque, and sealed envelopes. The patients and practitioners were not informed whether a subject was assigned to the intervention or control group. The outcome assessors and data analysts were also blinded in this study.
2.4. Intervention
Patients in the intervention group received ESWT with 3000 pulses of 0.11 mJ/mm2 at a frequency of 15 Hz using the Pain Treatment System of Radial Shockwave Device (Sonothera, Hanil Tm Co. Ltd, Korea). Pressure was set at 3 bar. The participants in the control group received placebo by using an identical-looking placebo probe. This probe could emit the same sounds as the ESWT probe. Patients in both groups were treated for 5 sessions with an interval of 3 days.
2.5. Outcome measurements
The primary outcome of the intensity of shoulder pain was measured by Numeric Rating Scale (NRS). The secondary outcome measurements included Constant–Murley score (CMS) [21] and the simple shoulder test (SST) score.[22] NRS score, CMS, and SST score were measured and evaluated at 4 and 8 weeks after the treatment. In addition, any AEs were recorded to assess the safety of ESWT.
2.6. Statistical analysis
All outcome data were analyzed using the Statistical Package for the Social Sciences software v.17.0 (SPSS Inc., Chicago, IL). Sample size was calculated based on the 50% difference in NRS score with α = 0.5, β = 0.8, and assuming a 20% drop-out rate. Therefore, the required sample size of the present study was estimated to be 84 patients, with 42 assigned to each group. All outcome measurements were evaluated by using the mean change from baseline [with a 95% confidence interval (CI)] and the difference (with a 95% CI) between the 2 groups. In the study, t test or Mann–Whitney rank sum test was used to analyze the data of NRS, CMS, and SST scores between baseline, 4 and 8 weeks after treatment. Pearson χ2 test or Fisher exact test was used to analyze the categorical data at baseline. All data were analyzed by intention-to-treat (ITT). Two side P < .05 were regarded as the statistical significant.
3. Results
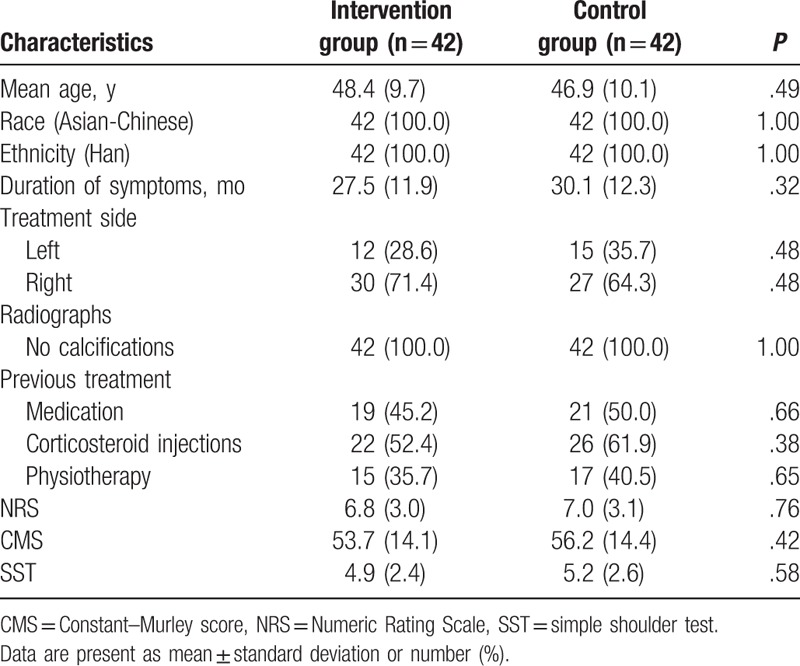
A total of 125 patients were eligible for inclusion in this study (Fig. 1). Of these 125 patients, 41 were excluded because of failure to meet the inclusion criteria (n = 20), meeting exclusion criteria (n = 10), and rejection to participate the study (n = 11). Therefore, 84 patients were allocated to an intervention group or a control group in a ratio of 1:1. All outcome data were analyzed using ITT approach. Fifteen patients withdrew from the study, because of the consent withdrawal (n = 3) and lost to follow up (n = 12) (Fig. 1). The patients’ characteristics are shown in Table 1. No significant differences of characteristic values were found between 2 groups at baseline (Table 1).
Figure 1.
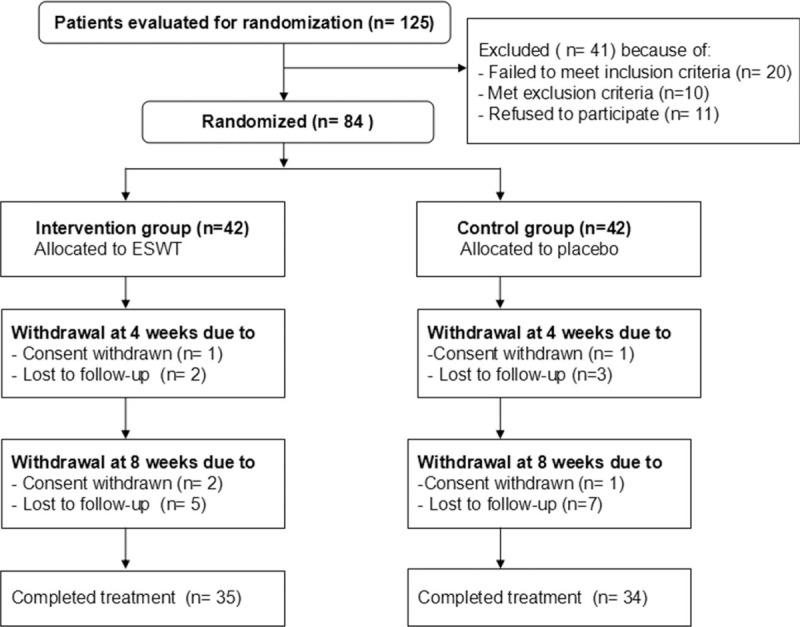
Flow diagram of patients through the study.
Table 1.
Characteristics of study population at baseline.
The results of all outcome measurements are summarized in Table 2. ESWT significantly decreased the intensity of shoulder pain associated with CRCT, as measured by using the NRS score and shoulder function as measured by using CMS and SST score at both 4 (P < .05) and 8 weeks (P < .01) after the treatment. In addition, no AEs were reported in any of the groups during the study period.
Table 2.
Outcome measurements at the 4 and 8 weeks after treatment (change from baseline).

4. Discussion
The results of this study confirmed the hypothesis that ESWT showed encouraging effect for treating patients with CRCT, compared with the placebo. To our best knowledge, this study is the first blind, randomized placebo-controlled trial of using ESWT for treating patients with CRCT in Chinese population. The findings demonstrated the promising effect of ESWT for treatment of patients with CRCT.
Previous studies also reported ESWT treatment for patients with CRCT, albeit with inconsistent results.[18,23] One prospective study assessed the efficacy of ESWT at either high- or low-energy for treating patients with rotator cuff. It found that ESWT with high-energy is efficacious for the symptoms improvement in patients with calcifying tendinitis of the rotator cuff after 3-month follow up.[18] The other study explored the effect of radial ESWT (rESWT) for the treatment of patients with the rotator cuff.[23] Its results demonstrated that low-dose rESWT neither reduced pain nor improved function for patients.[23] The result of the current study is consistent with that of the previous study [18] and revealed that ESWT is an effective therapy for patients with CRCT in a Chinese population.
In this study, the pain associated with CRCT as measured by using the NRS score was significantly reduced in the intervention group, in comparison with that in the control group. In addition, the CMSs and SST scores were also significantly greater for the participants in the intervention group than for those in the control group. These results indicate the promising efficacy of ESWT for shoulder pain relief in participants with CRCT and encouraging improvement in shoulder function as measured by using CMS and SST score. Furthermore, no AEs were reported in both groups in this study.
Although the promising effect of ESWT was achieved, this study still had several limitations. First, the sample size was small, which affected the results of the study. Second, this study was only conducted at a single center and included only Chinese Han ethnicity, which might have affected its generalization to other hospitals and other ethnicities in China.
5. Conclusion
This study found that ESWT can reduce the intensity of shoulder pain associated with CRCT and improve the shoulder function of patients with CRCT. However, further studies with larger sample sizes are warranted to confirm our results.
Footnotes
Abbreviations: AEs = adverse events, CI = confidence interval, CMS = Constant–Murley score, CRCT = chronic rotator cuff tendonitis, ESWT = extracorporeal shock-wave therapy, ITT = intention-to-treat, NRS = Numeric Rating Scale, NSAIDs = nonsteroidal antiinflammatory drugs, SST = simple shoulder test.
WL and S-XZ contributed equally to this work.
This study was funded by grants from the Science and Technology Talents Program of Harbin (2014RFXGJ041, 2014RFQGJ094), Harbin first hospital postdoctoral fellowship program (HRBSDYYYBSH-1); Postdoctoral Fund (160780); Harbin high level talent fund (HRBGCCRCJJ-6, 2013SYYRCYJ01–1); China Postdoctoral Science Foundation, Heilongjiang Natural Science Foundation (QC2016102, H2016002).
The authors declare no conflicts of interest.
References
- [1].Razavi M, Jansen GB. Effects of acupuncture and placebo TENS in addition to exercise in treatment of rotator cuff tendonitis. Clin Rehabil 2004;18:872–8. [DOI] [PubMed] [Google Scholar]
- [2].Andres BM, Murrell GA. Treatment of tendinopathy: what works, what does not, and what is on the horizon. Clin Orthop Relat Res 2008;466:1539–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Buchbinder R, Green S, Youd JM. Corticosteroid injections for shoulder pain. Cochrane Database Syst Rev 2003;1:CD004016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Green S, Buchbinder R, Hetrick SE. Physiotherapy interventions for shoulder pain. Cochrane Database Syst Rev 2003;2:CD004258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Karthikeyan S, Kwong HT, Upadhyay PK, et al. A double-blind randomised controlled study comparing subacromial injection of tenoxicam or methylprednisolone in patients with subacromial impingement. J Bone Joint Surg Br 2010;92-B:77–82. [DOI] [PubMed] [Google Scholar]
- [6].Robinson PM, Wilson J, Dalal S, et al. Rotator cuff repair in patients over 70 years of age: early outcomes and risk factors associated with re-tear. Bone Joint J 2013;95-B:199–205. [DOI] [PubMed] [Google Scholar]
- [7].Rees JL. The pathogenesis and surgical treatment of tears of the rotator cuff. J Bone Joint Surg Br 2008;90-B:827–32. [DOI] [PubMed] [Google Scholar]
- [8].Sun J, Gao F, Wang Y, et al. Extracorporeal shock wave therapy is effective in treating chronic plantar fasciitis: a meta-analysis of RCTs. Medicine (Baltimore) 2017;96:e6621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Al Edwan GM, Muheilan MM, Atta ON. Long term efficacy of extracorporeal shock wave therapy [ESWT] for treatment of refractory chronic abacterial prostatitis. Ann Med Surg (Lond) 2017;14:12–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Lee JH, Lee S, Choi S, et al. The effects of extracorporeal shock wave therapy on the pain and function of patients with degenerative knee arthritis. J Phys Ther Sci 2017;29:536–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Cho YS, Joo SY, Cui H, et al. Effect of extracorporeal shock wave therapy on scar pain in burn patients: a prospective, randomized, single-blind, placebo-controlled study. Medicine (Baltimore) 2016;95:e4575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Notarnicola A, Moretti L, Maccagnano G, et al. Tendonitis of the rotator cuff treated with extracorporeal shock wave therapy: radiographic monitoring to identify prognostic factors for disintegration. J Biol Regul Homeost Agents 2016;30:1195–202. [PubMed] [Google Scholar]
- [13].Arirachakaran A, Boonard M, Yamaphai S, et al. Extracorporeal shock wave therapy, ultrasound-guided percutaneous lavage, corticosteroid injection and combined treatment for the treatment of rotator cuff calcific tendinopathy: a network meta-analysis of RCTs. Eur J Orthop Surg Traumatol 2017;27:381–90. [DOI] [PubMed] [Google Scholar]
- [14].Bannuru RR, Flavin NE, Vaysbrot E, et al. High-energy extracorporeal shock-wave therapy for treating chronic calcific tendinitis of the shoulder: a systematic review. Ann Intern Med 2014;160:542–9. [DOI] [PubMed] [Google Scholar]
- [15].Buchbinder R, Green S, Youd JM, et al. Shock wave therapy for lateral elbow pain. Cochrane Database Syst Rev 2005;4:CD003524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Harniman E, Carette S, Kennedy C, et al. Extracorporeal shock wave therapy for calcific and noncalcific tendonitis of the rotator cuff: a systematic review. J Hand Ther 2004;17:132–51. [DOI] [PubMed] [Google Scholar]
- [17].Ogden JA, Alvarez RG, Marlow M. Shockwave therapy for chronic proximal plantar fasciitis: a meta-analysis. Foot Ankle Int 2002;23:301–8. [DOI] [PubMed] [Google Scholar]
- [18].Albert JD, Meadeb J, Guggenbuhl P, et al. High-energy extracorporeal shockwave therapy for calcifying tendinitis of the rotator cuff: a randomised trial. J Bone Joint Surg Br 2007;89-B:335–41. [DOI] [PubMed] [Google Scholar]
- [19].Schmitt J, Haake M, Tosch A, et al. Low-energy extracorporeal shock-wave treatment (ESWT) for tendinitis of the supraspinatus. J Bone Joint Surg Br 2001;83- B:873–6. [DOI] [PubMed] [Google Scholar]
- [20].Speed CA, Richards C, Nichols D, et al. Extracorporeal shock-wave therapy for tendonitis of the rotator cuff: a double-blind, randomised, controlled trial. J Bone Joint Surg Br 2002;84-B:509–12. [DOI] [PubMed] [Google Scholar]
- [21].Constant CR, Murley AH. A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res 1987;214:160–4. [PubMed] [Google Scholar]
- [22].Van Kampen DA, van Beers LW, Scholtes VA, et al. Validation of the Dutch version of the Simple Shoulder Test. J Shoulder Elbow Surg 2012;21:808–14. [DOI] [PubMed] [Google Scholar]
- [23].Kolk A, Yang KG, Tamminga R, et al. Radial extracorporeal shock-wave therapy in patients with chronic rotator cuff tendinitis: a prospective randomised double-blind placebo-controlled multicentre trial. Bone Joint J 2013;95-B:1521–6. [DOI] [PubMed] [Google Scholar]