

Abstract
Objectives:
Writer's cramp is a focal dystonia producing abnormal postures during selective motor activities. Thalamotomy or globus pallidus internus deep brain stimulation (GPi DBS) has been used as a surgical treatment in patients not responding to medical treatment.
Materials and Methods:
Eight patients (all men, age 16–47 years) with refractory focal hand dystonia underwent either ventrooralis (Vo) thalamotomy (seven patients) or GPi DBS (one patient) using stereotactic techniques. Preoperative video recordings, Writing movment score for dystonic posture and latency of dystonia (WMS), and symptom severity scores (SSSs) were evaluated at baseline and latest follow-up ranging from 1 to 4 years.
Results:
All patients had difficulty in performing their most common tasks. The duration of symptoms ranged from 6 months to 12 years. All patients obtained immediate postoperative relief from the dystonic symptoms, and the effect was sustained during the follow-up period. The WMS (range 0–28) improved from a mean of 14.5 before surgery to 2, whereas the SSS (maximum 43 and minimum 10) improved from a mean of 15.3 before surgery to 2 at the last follow-up. There were no surgical complications, morbidity, or mortality.
Conclusion:
Vo thalamotomy or GPi DBS offers successful symptom relief in patients with task-specific dystonia.
Keywords: Focal dystonia, globus pallidus internus deep brain stimulation, thalamotomy, Writer's cramp
INTRODUCTION
Writer's cramp, also known as task-specific dystonia (TSD), is a type of focal dystonia which often involves highly skilled, repetitive movements. It occurs due to dysfunction of the pallido-thalamocortical pathway. Symptom of dystonia can be improved by interrupting this loop at a certain anatomical point.[1] Recent studies have revealed a variety of sensory deficits in the hands of patients with TSD. For example, patients showed impaired performance in spatial and temporal discrimination tasks,[2] changes in single and paired somatosensory-evoked potentials (SEPs),[3] and alterations in the spatial distribution of SEPs or functional imaging maps, suggestive of changes in the underlying somatosensory maps of the hand.[4] Others have emphasized that the important feature of focal hand dystonia (FHD) is an abnormal link between sensory input and motor output.[5] A volumetric magnetic resonance imaging study found that characteristic gray matter volume changes in the TSD involve the brain regions responsible for sensorimotor control during writing and speaking such as primary somatosensory cortex, middle frontal gyrus, superior/inferior temporal gyrus, middle/posterior cingulate cortex, and occipital cortex as well as the striatum and cerebellum (lobules VI–VIIa).[6]
Although clinical manifestations in FHD are typically unilateral in the beginning, the disorder is considered as a bilateral dysfunction of the basal ganglia.[7] This is demonstrated by the fact that up to 25% of patients develop bilateral FHD if they switch to the previously unaffected hand.[8,9] The prevalence of Writer's cramp has been reported as being between 16.3 and 68.9 per million.[10] Nonsurgical treatments such as botulinum toxin have been tried, but the therapeutic effects are not so remarkable.[11] We present a series of eight patients with TSD, seven of whom underwent ventrooralis (Vo) thalamotomy and one underwent globus pallidus internus deep brain stimulation (GPi DBS) with marked improvement in the symptoms postoperatively.
MATERIALS AND METHODS
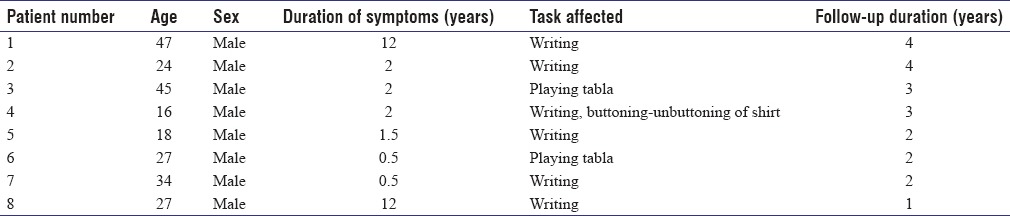
Between August 2012 and September 2015, eight patients (all men; age 16–47 years) with medically refractory FHD underwent either Vo nucleus thalamotomy (seven patients) or GPi DBS (one patient) at our institute. All the patients were carefully diagnosed as having FHD by history taking and clinical examination. Preoperative video recordings, for dystonic posture and latency of dystonia (WMS), and symptom severity score (SSS) were evaluated. Patients were explained about the procedure in detail. Informed consent for the surgery was obtained from the patient and the relatives [Table 1].
Table 1.
Clinical detail of patients with task-specific dystonias
All the surgeries were performed under local anesthesia using CRW stereotactic system. Vo nucleus of thalamus was targeted on computerized tomography (CT) scan based on the coordinates published by Taira and Hori.[1] The target was selected at the junction of Vo anterior and posterior nuclei. This was 13.5 mm lateral, 2 mm posterior to the mid-anterior commissure-posterior commissure (AC-PC) point and at the level of AC-PC plane. Intraoperative stimulation was performed using 1 mm diameter and 2 mm exposed tip electrode. Stimulation of the target would elicit improvement in dystonia and facilitate the action such as writing or playing drums. The acceptable limit for eliciting any capsular response was 2 V at 5 Hz and 100 μs. The improvement in the symptoms was recorded using stimulation at 100 Hz and 100 μs. This was followed by a test lesion at 45°C for 60 s. If there were no side effects, we would proceed with the lesioning at 70°C for 60 s. The electrode was withdrawn, and another lesion was made using a similar protocol. A total of two or three lesions were performed based on the electrical stimulation response and clinical improvement. No lesion extended below the AC-PC plane. A check CT scan was performed to evaluate the lesion and look for any hemorrhage. GPi DBS was performed using microelectrode guidance and test stimulation as per standard technique of targeting GPi.
RESULTS
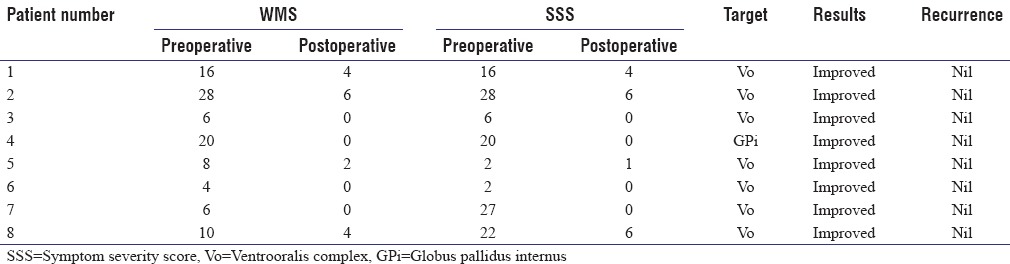
All the patients had difficulty in performing their most common tasks (e.g., writing, playing tabla/drums, etc.). The duration of symptoms ranged from 6 months to 12 years. One patient who was a professional drummer had severe dystonia involving right second and third finger beginning as soon as he started playing. The patient who underwent GPi DBS had symptoms predominantly pointing toward Writer's dystonia, but the fact that they were present with other tasks (buttoning and unbuttoning of shirt and grasping of objects with right hand) lead us to think in terms of focal upper limb dystonia. In view of this, we proceeded with GPi DBS in this patient. The intraoperative course was uneventful. All the patients obtained immediate postoperative relief from the dystonic symptoms, and the effect was sustained during the follow-up period. The patient undergoing Gpi DBS was stimulated with contact 1 as a cathode and contact 2 as an anode with a pulse width of 240 μs and frequency of 100 Hz with a voltage of 1.6 V. On the postoperative scan, contact 0 was found to be at the bottom of the pallidum. The minimum follow-up was for 1 year and the maximum follow-up was for 4 years. The WMS (range 0–28) improved from a mean of 14.5 before surgery to 2, whereas the SSS (maximum 43 and minimum 10) improved from a mean of 15.3 before surgery to 2 at the last follow-up [Table 2]. There were no surgical complications, morbidity, or mortality.
Table 2.
Results of ventrooralis complex thalamotomy and globus pallidus internus deep brain stimulation
DISCUSSION
Writer's cramp and laryngeal dystonias are the most common forms of TSDs though less common then dystonias of neck and eyelids. Remissions are uncommon, and symptoms can progress to the other hand.[11] Symptoms appear at a mean age of 38 years and may be painless or accompanied by painful hand and forearm cramping. In our study, the mean age of presentation was 33 years and the mean duration of symptoms was 4.5 years [Table 1]. Five out of eight patients experienced pain in fingers, wrist, and arm while performing the task of writing.
The exact pathophysiology of Writer's cramp is not known though several mechanisms have been suggested. Byl et al. suggested that it occurs as a result of maladaptive response of the brain to repetitive stereotyped tasks.[12] Kaji et al. suggested that a disorder of a motor subroutine might exist in the motor cortex-basal ganglia thalamus-cortex loop in patients with dystonia. Improvement in dystonia after ablation or stimulation in the motor thalamus and GPi may occur as a result of a disruption or normalization of altered pallidal or thalamic output.[13]
The main symptom is difficulty in writing, which is slow, and change of handwriting to a less legible form. Usually, distal muscles of the dominant hand are the first affected. Tight grip of the pen is typical, and hand–wrist flexors are more commonly involved than extensors even though hyperextension of the distal phalanges or even the fingers has been seen. Six out of our eight patients had dystonia in right hand beginning within seconds of starting to write and resulted in tight grip of pen and gradual abduction of arm and forearm as they continued writing. Two patients were a professional drummer and had dystonia in right second and third finger as soon as they started playing drums.
Excessive muscle spasms may progress to more proximal muscles around the elbow and shoulder, producing abduction of the arm. Later, the task specificity is lost, and patients may develop difficulty in other tasks also.[14] In our study, one patient had difficulty in other tasks (buttoning-unbuttoning of shirt and eating) with his right upper limb apart from dystonia while writing. In this patient, we chose GPi as the target for DBS as we felt that his dystonia may progress over the period of time and the GPi stimulation will be able to control the same.
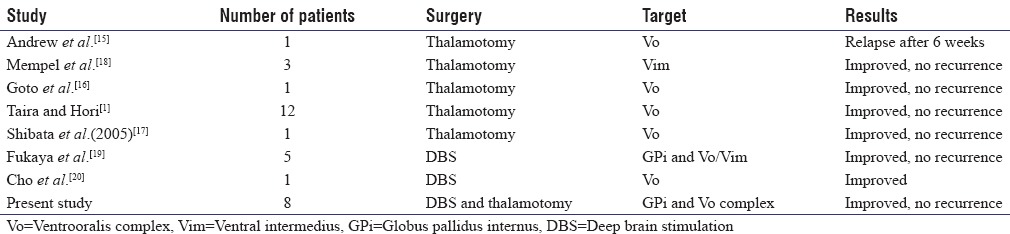
Various management modalities consist of oral medications, botulinum toxin injection, sensorimotor retuning, and neurosurgical procedures, with latter giving more consistent and long-term relief. There have been very limited number of reports on the surgical treatment of TSD, most of them being case reports. Different targets in thalamus and GPi have been chosen for the surgical treatment. Andrew et al.,[15] Goto et al.,[16] Taira and Hori,[1] and Shibata et al.[17] performed thalamotomy and used Vo complex as their target. Mempel et al.[18] reported thalamotomy using ventralis intermedius (Vim) as their target, whereas Fukaya et al. and Cho et al. performed DBS, targeting Gpi, and Vo/Vim [Table 3].[19,20] However, the Vo is the most common target. Vo thalamotomy has also been offered for musician's and hairdresser dystonia, again another form of TSD.[21,22] Asahi et al. reported improvement in a patient with table tennis dystonia following Vo thalamotomy.[23] All these reports underscore the role of Vo thalamus as a gateway that can be manipulated to improve any TSD. We present a series of eight patients with Writer's cramp, seven of whom underwent Vo thalamotomy and one underwent GPi DBS with marked improvement in the symptoms postoperatively. This is one of the largest series reported outside Japan [Table 3].
Table 3.
Comparison of various studies with current case series
Based on the literature and our experience, thalamotomy or DBS could be effective in relieving the symptoms. Thalamotomy is a one-time procedure without any risks associated with hardware complications of DBS. However, thalamotomy has a higher rate of complications such as dysarthria and motor deficits.[24] This can be reduced by intraoperative test lesions and adequate expertise in performing surgery. The recurrence rate of patients with Writer's cramp who underwent lesioning surgery has been reported to be 15%, presumably because of inadequate lesioning. In our study, there were no recurrences at the last follow-up, but one patient (Case 8) reported that he was not fully satisfied with the outcome, as though his writing speed had improved; it had not been near-normal. All the patients had significant to complete relief from their symptoms, and this was correlated by WMS and SSS at follow-up [Table 2].
The patient with GPi DBS though did not progress in the involvement of any other body parts but continued to require an increasing amount of stimulation over time. Initially, his symptoms were controlled with 90 μs, 130 Hz, and 1.0 V which were changed to 240 μs, 100 Hz, and 1.6 V.
The present study confirms the usefulness of thalamotomy and GPi DBS for Writer's cramp.
CONCLUSION
Writer's dystonia is a rare TSD. Vo thalamotomy or GPi DBS offers successful symptom relief in patients with TSD.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Taira T, Hori T. Stereotactic ventrooralis thalamotomy for task-specific focal hand dystonia (writer's cramp) Stereotact Funct Neurosurg. 2004;80:88–91. doi: 10.1159/000075165. [DOI] [PubMed] [Google Scholar]
- 2.Bara-Jimenez W, Shelton P, Hallett M. Spatial discrimination is abnormal in focal hand dystonia. Neurology. 2000;55:1869–73. doi: 10.1212/wnl.55.12.1869. [DOI] [PubMed] [Google Scholar]
- 3.Tinazzi M, Priori A, Bertolasi L, Frasson E, Mauguière F, Fiaschi A. Abnormal central integration of a dual somatosensory input in dystonia. Evidence for sensory overflow. Brain. 2000;123(Pt 1):42–50. doi: 10.1093/brain/123.1.42. [DOI] [PubMed] [Google Scholar]
- 4.Butterworth S, Francis S, Kelly E, McGlone F, Bowtell R, Sawle GV. Abnormal cortical sensory activation in dystonia: An fMRI study. Mov Disord. 2003;18:673–82. doi: 10.1002/mds.10416. [DOI] [PubMed] [Google Scholar]
- 5.Tamburin S, Manganotti P, Marzi CA, Fiaschi A, Zanette G. Abnormal somatotopic arrangement of sensorimotor interactions in dystonic patients. Brain. 2002;125(Pt 12):2719–30. doi: 10.1093/brain/awf279. [DOI] [PubMed] [Google Scholar]
- 6.Ramdhani RA, Kumar V, Velickovic M, Frucht SJ, Tagliati M, Simonyan K. What's special about task in dystonia? A voxel-based morphometry and diffusion weighted imaging study. Mov Disord. 2014;29:1141–50. doi: 10.1002/mds.25934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hallett M. Neurophysiology of dystonia: The role of inhibition. Neurobiol Dis. 2011;42:177–84. doi: 10.1016/j.nbd.2010.08.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sheehy MP, Marsden CD. Writers’ cramp-a focal dystonia. Brain. 1982;105(Pt 3):461–80. doi: 10.1093/brain/105.3.461. [DOI] [PubMed] [Google Scholar]
- 9.Zeuner KE, Molloy FM. Abnormal reorganization in focal hand dystonia – Sensory and motor training programs to retrain cortical function. NeuroRehabilitation. 2008;23:43–53. [PubMed] [Google Scholar]
- 10.Nutt JG, Muenter MD, Aronson A, Kurland LT, Melton LJ., 3rd Epidemiology of focal and generalized dystonia in Rochester, Minnesota. Mov Disord. 1988;3:188–94. doi: 10.1002/mds.870030302. [DOI] [PubMed] [Google Scholar]
- 11.Rivest J, Lees AJ, Marsden CD. Writer's cramp: Treatment with botulinum toxin injections. Mov Disord. 1991;6:55–9. doi: 10.1002/mds.870060110. [DOI] [PubMed] [Google Scholar]
- 12.Byl NN, Merzenich MM, Jenkins WM. A primate genesis model of focal dystonia and repetitive strain injury: I. Learning-induced dedifferentiation of the representation of the hand in the primary somatosensory cortex in adult monkeys. Neurology. 1996;47:508–20. doi: 10.1212/wnl.47.2.508. [DOI] [PubMed] [Google Scholar]
- 13.Kaji R, Shibasaki H, Kimura J. Writer's cramp: A disorder of motor subroutine? Ann Neurol. 1995;38:837–8. doi: 10.1002/ana.410380603. [DOI] [PubMed] [Google Scholar]
- 14.Torres-Russotto D, Perlmutter JS. Task-specific dystonias: A review. Ann N Y Acad Sci. 2008;1142:179–99. doi: 10.1196/annals.1444.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Andrew J, Fowler CJ, Harrison MJ. Stereotaxic thalamotomy in 55 cases of dystonia. Brain. 1983;106(Pt 4):981–1000. doi: 10.1093/brain/106.4.981. [DOI] [PubMed] [Google Scholar]
- 16.Goto S, Tsuiki H, Soyama N, Okamura A, Yamada K, Yoshikawa M, et al. Stereotactic selective Vo-complex thalamotomy in a patient with dystonic writer's cramp. Neurology. 1997;49:1173–4. doi: 10.1212/wnl.49.4.1173. [DOI] [PubMed] [Google Scholar]
- 17.Shibata T, Hirashima Y, Ikeda H, Asahi T, Hayashi N, Endo S. Stereotactic Voa-Vop complex thalamotomy for writer's cramp. Eur Neurol. 2005;53:38–9. doi: 10.1159/000084262. [DOI] [PubMed] [Google Scholar]
- 18.Mempel E, Kucinski L, Witkiewicz B. Writer's cramp syndrome treated successfully by thalamotomy. Neurol Neurochir Pol. 1986;20:475–80. [PubMed] [Google Scholar]
- 19.Fukaya C, Katayama Y, Kano T, Nagaoka T, Kobayashi K, Oshima H, et al. Thalamic deep brain stimulation for Writer's cramp. J Neurosurg. 2007;107:977–82. doi: 10.3171/JNS-07/11/0977. [DOI] [PubMed] [Google Scholar]
- 20.Cho CB, Park HK, Lee KJ, Rha HK. Thalamic deep brain stimulation for Writer's cramp. J Korean Neurosurg Soc. 2009;46:52–5. doi: 10.3340/jkns.2009.46.1.52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Horisawa S, Goto S, Nakajima T, Kawamata T, Taira T. Bilateral stereotactic thalamotomy for bilateral musician's hand dystonia. World Neurosurg. 2016;92:585.e21–5. doi: 10.1016/j.wneu.2016.05.017. [DOI] [PubMed] [Google Scholar]
- 22.Horisawa S, Goto S, Nakajima T, Ochiai T, Kawamata T, Taira T. Stereotactic thalamotomy for hairdresser's dystonia: A case series. Stereotact Funct Neurosurg. 2016;94:201–6. doi: 10.1159/000446612. [DOI] [PubMed] [Google Scholar]
- 23.Asahi T, Taira T, Ikeda K, Yamamoto J, Sato S. Improvement of table tennis dystonia by stereotactic ventro-oral thalamotomy: A case report. World Neurosurg. 2017;99:810.e1–4. doi: 10.1016/j.wneu.2016.12.117. [DOI] [PubMed] [Google Scholar]
- 24.Horisawa S, Taira T, Goto S, Ochiai T, Nakajima T. Long-term improvement of musician's dystonia after stereotactic ventro-oral thalamotomy. Ann Neurol. 2013;74:648–54. doi: 10.1002/ana.23877. [DOI] [PubMed] [Google Scholar]