

Abstract
Two experiments that studied the effects of hypnotic suggestions on tactile sensitivity are reported. Experiment 1 found that suggestions for anesthesia, as measured by both traditional psychophysical methods and signal detection procedures, were linearly related to hypnotizability. Experiment 2 employed the same methodologies in an application of the real-simulator paradigm to examine the effects of suggestions for both anesthesia and hyperesthesia. Significant effects of hypnotic suggestion on both sensitivity and bias were found in the anesthesia condition but not for the hyperesthesia condition. A new bias parameter, C′, indicated that much of the bias found in the initial analyses was artifactual, a function of changes in sensitivity across conditions. There were no behavioral differences between reals and simulators in any of the conditions, though analyses of postexperimental interviews suggested the 2 groups had very different phenomenal experiences.
Alterations in sensory and perceptual functioning are among the hallmarks of hypnosis. In hypnotic blindness, deafness, and agnosia, hypnotized subjects cannot see, hear, smell, or taste stimuli that are presented in the sensory field at above threshold levels. In negative hallucinations, the impairment occurs with respect to specific objects, leaving acuity in the rest of the sensory field unchanged. In positive hallucinations, subjects respond to stimuli that are not actually present in the stimulus field. It has also been claimed that hypnotic suggestions can improve sensory acuity.
Among these sensory-perceptual phenomena is hypnotic tactile anesthesia, in which the subject receives suggestions for a loss or diminution in tactile sensitivity—an effect somewhat analogous to the pain reduction observed in hypnotic analgesia (Hilgard & Hilgard, 1975), though targeting sensations of touch rather than pain. Suggestions for anesthesia play a role in the “circle-touch” test proposed by Janet (1907) for distinguishing organic from functional anesthesia, and by Orne (1959) for distinguishing truly hypnotized individuals from simulators (Eiblmayr, 1987; McConkey, Bryant, Bibb, Kihlstrom, & Tataryn, 1990; Wilton, Barnier, & McConkey, 1997). Wallace and his colleagues have reported that suggestions for tactile anesthesia reduce or eliminate the perceptual-kinesthetic adaptation normally acquired by subjects asked to point at a target while gazing through a prism (e.g., Wallace & Garrett, 1973; but see Spanos, Dubreuil, Saad, & Gorassini, 1983).
Aside from very early studies that did not employ modern psychophysical methods (e.g., Young, 1925, 1926), the effects of hypnotic tactile anesthesia have not been explored systematically. However, investigations of this sort have been carried out in a number of other sensory-perceptual domains, and these form the background for the studies reported here. In a classic study of hypnotic analgesia, Hilgard (1967) employed the method of magnitude estimation during the cold-pressor test, in which subjects’ arms are submerged in circulating ice water. Perceived pain was measured by the technique of magnitude estimation, employing a 0-to-10 scale. Plotting pain ratings as a function of time on log-log paper, Hilgard found that subjects of low, medium, and high hypnotizability had identical linear slopes and intercept values in the absence of hypnosis and the analgesia suggestion. In the hypnotic analgesia condition, however, there were significant group differences in the intercept values representing the levels of reported pain. The overall correlation between hypnotizability and pain reduction experienced by each subject was .46.
Crawford, Macdonald, and Hilgard (1979) extended Hilgard’s basic paradigm to examine the relationship between hypnotizability and hypnotic deafness. As with the analgesia study, overall decrements in hearing were strongly related to hypnotizability. In the normal hearing condition, the slopes and intercepts were close to identical across groups. Suggestions for hypnotic deafness resulted in a change in intercept but not slope: there were equal decrements in hearing across the range of stimuli, the magnitude of which was related to group membership.
Although the effects documented in the magnitude-estimation studies of analgesia and deafness are clear, they are not unambiguous. As Jones and Spanos (1982) noted, experiments employing classic psychophysical techniques are not able to discriminate between genuine changes in sensitivity on the one hand and alterations in response criterion for another. For example, in the magnitude-estimation studies, an apparent effect of analgesia or deafness suggestions can be produced simply by subtracting a constant from the felt intensity: reporting a value of 2 on a 0-to-10 scale, for example, when the actual intensity is 4, and a value of 6 when the actual intensity is 8. Alternatively, in studies employing threshold-determination procedures, apparent analgesia or deafness can be produced simply by denying sensation on trials where sensation actually occurs: reporting that the stimulus is not felt, or heard, when in fact it was. A similar strategy can produce reports of increased hearing (or, in the case of pain, hyperalgesia).
It was to take account of just this sort of problem, which first arose in nonhypnotic studies of classic psychophysics, that signal detection theory (SDT) and its associated procedures were developed (Green & Swets, 1966; Macmillan & Creelman, 1991; Pastore & Scheirer, 1974; Swets, Tanner, & Birdsall, 1961). Signal detection theory explicitly recognizes that an observer’s response is a function of both underlying sensitivity, the actual ability to discriminate a stimulus, and the response criterion the observer used to decide that a stimulus had occurred, and provides a methodology by which to separate them. In their study, Jones and Spanos found no significant effect of suggestion on perceptual sensitivity, in either direction – diminished or enhanced hearing. In fact, highly hypnotizable subjects showed increased sensitivity, relative to baseline, when given either set of instructions to change sensitivity. There was a significant three-way interaction for bias: For the hypnotic induction condition only, highs became more liberal in their response criteria while the lows became more conservative. Jones and Spanos also reported that, across all conditions, subjects classified as lows were consistently more sensitive to acoustical stimuli than the highs.
The purpose of the present research was to evaluate quantitatively the effect of hypnotic suggestions for tactile anesthesia and hyperesthesia as well, employing methods from both classic psychophysical and signal-detection theory.
Experiment 1
Experiment 1 focused on hypnotically induced tactile anesthesia and generally followed the protocol set by Hilgard (1967, 1969) in his classic psychophysical analyses of hypnotic analgesia. However, the experiment also employed SDT methods, in order to isolate the effects of any changes in both sensitivity and response criteria.
Method
Subjects
A total of 40 undergraduate males and females were recruited on the basis of their scores on the Harvard Group Scale of Hypnotic Susceptibility, Form A. (HGSHS:A; Shor & Orne, 1962) and the Stanford Hypnotic Susceptibility Scale: Form C (SHSS:C; Weitzenhoffer & Hilgard, 1962). Subjects received either a monetary payment of $10.00, credit toward the research participation requirement of their introductory psychology course, or a combination of the two as reimbursement for their participation. The subjects were divided into four groups of 10: Lows (SHSS:C range: 1 to 4, M = 1.8, SD = 1.14), Mediums (range: 5 to 7, M = 6.2, SD = .79), Highs (range: 8 to 10, M = 8.8, SD = .63), and Virtuosos (all had scores of 11).
Apparatus
A plastic template (1.375” diameter) and red erasable ink were used to draw a circle on the palm of the subject’s right hand. Stoelting pressure aesthesiometers, similar to Von Frey filaments, served as tactile stimuli. The aesthesiometers are marked in log force units that yield a linear interval scale suitable for statistical comparisons. A personal computer signaled the beginning of each trial with three consecutive beeps, specified to the experimenter the appropriate stimulation for each trial, and collected both subject responses and reaction times via a computer mouse.
Procedure
During the introductory overview of the session, the subject was told that the experiment dealt with tactile sensitivity and establishing what levels of stimulation they could feel most of the time, but not necessarily all of the time. They were not informed that the experiment would involve suggestions for altered sensitivity. The subjects were seated in a large, comfortable chair and shown the array of aesthesiometers. They were told that the filaments were of different thicknesses, and used to determine what people can feel on the surface of the skin. A circle was drawn and traced over several times so the subject could “get a good sense of where it was located,” as their eyes would be closed during the test itself.
The subjects then took part in both threshold measurement and signal-detection procedures, both before and after receiving a hypnotic induction and suggestions for tactile anesthesia. The subjects were told that for the first series of trials they would hear a series of three beeps from the computer. Sometime between the second and third beeps they would be touched inside the circle on their palm. After each trial, they were to respond “Yes” if they felt the touch, and “No” if they did not. If they had not felt anything by the end of the third beep, they should respond “No.” The subjects were informed that their reaction times would be recorded but that it was much more important to be accurate than to be fast. If they made a mistake, they were instructed to tell the experimenter, so the response could be changed. Subjects were instructed to close their eyes during the testing procedures.
Threshold estimation
Thresholds for each subject were determined using the double random interleaved staircase (DRIS) method of limits (Cornsweet, 1962; Herrick, 1973; Jesteadt, 1980). The DRIS procedure was developed within classic psychophysics because different sensory thresholds are often obtained for descending (starting above threshold and going “down”) and ascending (starting below threshold and going “up”) methods. The DRIS method randomly intersperses both methods in the same session, thus eliminating any biases inherent in either of them. Two initial stimuli are chosen, one well above, and the other well below, the average threshold for most observers. If the observer responds positively to the stimulus, the value in the corresponding series (ascending or descending) is decreased one unit, if the response is negative, then a stronger stimulus is used. Over trials, in a staircase-like manner, the two series will converge on one or two stimulus intensities and oscillate at that level. This is considered to be the observer’s threshold or limen for that sensory domain. The DRIS has two attractive features. As mentioned earlier, it eliminates the bias associated with using either the ascending or descending method alone. Second, nonveridical or random responding on the observer’s part shows up quite clearly, if the two staircases never converge.
Signal detection
After the first DRIS trials, the weakest stimulus for which at least half the subject’s responses were positive was selected as a stimulus for the signal detection (SD) phase. The subject was told that he or she would be touched on about half the trials and was instructed to respond “Yes, if you think you were touched, and No, if you think you were not.” Confidence ratings were obtained after each decision on a 3-point scale, in which 3 meant very confident, 2 meant fairly confident, but not completely sure, and 1 meaning not confident at all in the decision. Confidence judgments were entered into the computer by the experimenter. Reaction times for confidence rating were not recorded. A total of 30 SD trials were given.
Hypnosis
The subjects were then hypnotized using the SHSS:C script as a standard induction technique. Each subject was then given a hand lowering suggestion (Item 1 of SHSS:C), and asked to rate his or her hypnotic depth on a 1-to-10 scale (O’Connell, 1964; Tart, 1972). Suggestions for anesthesia within the area of the circle were given and both the DRIS and signal detection procedures were repeated, in that order. At the end of the testing procedure, the subject again rated hypnotic depth, the suggestion for anesthesia was cancelled, and hypnosis was terminated. The total session time was approximately 1.5 hours.
Results
Thresholds
The average trial on which convergence occurred for the baseline and anesthesia conditions was 11.55 (SD = 2.60) and 12.48 (SD = 2.94) respectively. Only 5 subjects needed more than 30 trials to establish a stable threshold. The threshold was operationally defined for each subject as the arithmetic mean stimulus value on all trials after the ascending and descending staircases converged. As can be seen in Table 1, the suggestion for hypnotic anesthesia did induce a threshold change, the magnitude of which was lawfully related to hypnotizability. Lows and mediums showed little change, while highs and virtuosos showed fairly large increases in threshold. The main effect of hypnotizability was significant, F(3,36) = 6.98, MSe = .248, p < .0008; the main effect of condition (baseline vs. anesthesia) was also significant, F(1,36) = 28.82, MSe = .165, p < .0001, as was the hypnotizability-by-state interaction, F(3,36) = 5.57, MSe = .165, p < .003.
Table 1.
Mean Threshold Aesthesiometer Values, Experiment 1
| Condition | Hypnotizability | |||
|---|---|---|---|---|
| Low | Medium | High | Virtuoso | |
| Baseline | 2.85 | 3.24 | 3.15 | 3.15 |
| (.17) | (.28) | (.42) | (.23) | |
| Anesthesia | 3.10 | 3.31 | 3.74 | 4.20 |
| (.41) | (.58) | (.26) | (.85) | |
Note: Standard deviations in parentheses
Tests for simple main effects showed that within the baseline condition, there was a small effect of hypnotizability, F(3,36) = 3.31, MSe = .087, p <.03. Newman-Keuls post hoc tests (p < .05) showed that lows had a slightly lower tactile threshold than mediums, highs or virtuosos. Within the hypnotic anesthesia condition, there was a larger effect of hypnotizability, F(3,36) = 7.25, MSe = .326, p < .0006. Newman-Keuls post hoc tests showed that virtuosos and highs had higher thresholds than the lows, and that virtuosos had higher thresholds than mediums. Simple main effects were also obtained in each of the hypnotic groups, testing for difference between baseline and anesthesia conditions. The F-ratios for lows, F(1,36) = 1.89, MSe = 0.165, p > .05, mediums, F(1,36) = 0.148, MSe = .165, p > .05, highs, F(1,36) = 10.17, MSe = .165, p < .005, and virtuosos, F(1,36) = 33.35, MSe = .165, p < .001, revealed that only highs and virtuosos had significantly different thresholds from baseline to anesthesia conditions, both being significantly higher under anesthesia. The effect was larger for virtuosos than for highs.
Prior to calculating each subject’s average reaction time per condition, outlying data points, defined as laying four or more standard deviations above each subject’s respective mean for that condition, were eliminated. Truncation with reference to an individual’s distribution, as opposed to the group distribution, eliminated the influence of abnormal reaction times without affecting the intrinsic individual differences found among subjects on this variable. Based on this criterion, a total of four trials were eliminated from the analyses, one from each of the medium and virtuoso groups, and two from the high group.
Table 2 shows the mean reaction times as a function of hypnotizability and condition. A repeated measures ANOVA showed only a main effect of condition, F(1,36) = 5.25, MSe = .119, p < .028), reaction times being slightly slower under hypnosis, regardless of hypnotizability (baseline M = .87 sec, SD = .55; hypnosis M = 1.05 sec, SD = .56). This effect seemed to be driven by the changes in the reaction times for highs and virtuosos, though the interaction was not significant, F(3,36) = 1.89, MSe = .224, p < .15).
Table 2.
DRIS Reaction Times, Experiment 1
| Condition | Hypnotizability | |||
|---|---|---|---|---|
| Low | Medium | High | Virtuoso | |
| Baseline | 0.76 | 0.94 | 1.04 | 0.77 |
| (.43) | (.74) | (.59) | (.47) | |
| Anesthesia | 0.78 | 0.93 | 1.32 | 1.20 |
| (.39) | (.59) | (.58) | (.72) | |
Note: Standard deviations in parentheses
Rating scale usage
A critical assumption in the use of a rating scale in a signal-detection paradigm is that the observer has the capacity to define and maintain the appropriate number of internal criteria by which to evaluate a trial interval and make a decision as to the stimulus presence or absence. This assumption is considered justified if the subject demonstrates a monotonic increasing function between the criterion judgments and the proportion of trials the stimulus is actually present (Swets et al., 1961). For the purposes of the signal-detection analysis, the three-point confidence ratings associated with the subjects’ yes/no responses were transformed into a 1-to-6 criterion scale, with 1 meaning that the subject was very confident that he or she had not been touched, and 6 meaning that the subject was very confident that he or she had been touched. Analysis of the proportion of signal trials associated with each criterion level revealed that the monotonicity requirement was met for both baseline and anesthesia suggestion conditions. For example, baseline condition ratings of 1 were associated with signal trials only 20% of the time, while ratings of 6 were associated with signal trials about 95% of the time. Thus, the subjects used the yes/no decision and confidence scale sequence in the manner required by the assumptions of signal-detection theory.
Choosing measures of signal-detection
SDT developed as a framework in which sensitivity could be conceptualized and estimated independently of the influences of response bias, or the general willingness of an observer to say that a signal occurred. The fraction of trials that the observer responds “signal present” when a signal had actually been presented is called the observer’s hit rate (HR); the fraction of the trials the observer responds “signal present” when no signal had been presented is the observer’s false alarm rate (FAR). Varying the criterion changes both the HR and FAR. Plotting these two values against each other generates a curve known as the receiver operating characteristic (ROC), from which a variety of measures of sensitivity and bias can be constructed. The traditional measure of sensitivity, called d′, is measured in units of standardized distance between the means of the distributions of signal and noise on the ROC curve. The bias parameter which usually accompanies d′ is β (beta), the ratio of the likelihood of the observer responding “signal” over “noise.”
While d′ and β have been the parameters of choice in signal detection experiments since its origin, some researchers have proposed that alternative parameters are superior, both in terms of the plausibility of their assumptions and f their statistical robustness (Macmillan & Creelman, 1990). For instance, Snodgrass and Corwin (1988) have demonstrated β to be inferior to a newer bias measure, C. Schulman and Greenburg (1970) and Egan and Clark (1966) have demonstrated that the parameter d′s is superior to d′ when estimating sensitivity for a ROC curve. There are also nonparametric measures, such as the P(A) measure of sensitivity (Hodos, 1970; Pollack, Norman, & Galanter, 1964), though even these calculations make distributional assumptions and, hence, are actually parametric. The sensitivity measure, P(A), for example, is simply the total area under the ROC curve.
For this study, P(A) was chosen over d′ and d′s as a measure of sensitivity for several reasons. One is P(A)’s relative independence from assumptions. Both d′ and d′s assume normal distributions for the both the noise and signal-plus-noise distributions, and d′ also assumes that both distributions have equal variances. There is a great deal of research indicating that these conditions are not always met (Markowitz & Swets, 1967; Schulman & Greenberg, 1970; Treisman, 1977; Treisman & Faulkner, 1984). Also both parameters, being based on estimated regression lines, are best calculated with very stable HR and FAR points. This would require a great many trials per subject, which is not feasible where groups of subjects are being compared. In contrast, P(A) makes very few assumptions about the data, is fairly robust with regard to outlier points, and is intuitively understood (Pollack et al., 1964). With regard to bias, C was chosen over β, even though it does make some distributional assumptions, because the literature has clearly demonstrated its superiority (Macmillan & Creelman, 1990; Snodgrass & Corwin, 1988).
Hit and false alarm rates
A 1–4 confidence rating scale yields three possible criteria for signal detection: a liberal or loose criterion of 2, a more moderate criterion of 3, or a very conservative or strict criterion of 4. The confidence rating of 4 was used, as this is the point on the scale at which a verbal “Yes” response first occurs (i.e., a subjective judgment by the observer that the stimulus was, in fact, present). Note that, in general, any changes in hit rates have corresponding changes in the false alarm rates. The signal detection analysis extracts indices of sensitivity that are independent of any changes in response criteria. Table 3 shows the means and standard deviations for the hit and false alarm rates.
Table 3.
Hit and False Alarm Rates at Confidence Level 4, Experiment 1
| Condition | Hypnotizability | |||
|---|---|---|---|---|
| Low | Medium | High | Virtuoso | |
| Hit Rate | ||||
| Baseline | 0.76 | 0.72 | 0.59 | 0.74 |
| (.20) | (.12) | (.20) | (.15) | |
| Anesthesia | 0.78 | 0.66 | 0.43 | 0.27 |
| (.22) | (.19) | (.25) | (.16) | |
| False Alarm Rate | ||||
| Baseline | 0.13 | 0.19 | 0.07 | 0.11 |
| (.08) | (.13) | (.07) | (.11) | |
| Anesthesia | 0.08 | 0.08 | 0.07 | 0.05 |
| (.06) | (.06) | (.06) | (.04) | |
Note: Standard deviations in parentheses
Signal-detection analysis
Table 4 shows the corresponding values for the sensitivity measure P(A), derived by calculating the area beneath the ROC curve (Green & Swets, 1966). A 4 × 2 mixed-design analysis of variance with one between-groups factor (level of hypnotizability) and one within-subjects factor (condition) revealed significant main effects of both groups, F(3,36) = 4.94, MSe = .015, p < .01, and condition F(1,36) = 16.01, MSe = .004, p < .001; these effects were qualified by a significant interaction, F(3,36) = 8.61, MSe = .004, p < .001). There were no significant group differences in baseline sensitivity, F(3,36) = 1.29, MSe = .01, n.s. During anesthesia, however, the two groups of hypnotizable subjects showed substantially less sensitivity than insusceptible subjects, F(3,36) = 8.75, MSe = .01, p < .001. The variances of the sensitivity parameter P(A) suggested no pattern of differences amongst the four susceptibility groups.
Table 4.
Sensitivity Parameter P(A) and Bias Parameters C and C′, Experiment 1
| Condition | Hypnotizability | |||
|---|---|---|---|---|
| Low | Medium | High | Virtuoso | |
| Sensitivity Parameter P(A) | ||||
| Baseline | 0.87 | 0.84 | 0.79 | 0.84 |
| (.07) | (.07) | (.10) | (.10) | |
| Anesthesia | 0.89 | 0.83 | 0.70 | 0.68 |
| (.10) | (.06) | (.13) | (.11) | |
| Bias Parameter C | ||||
| Baseline | 0.23 | 0.21 | 0.66 | 0.34 |
| (.36) | (.42) | (.43) | (.37) | |
| Anesthesia | 0.30 | 0.51 | 0.86 | 1.22 |
| (.45) | (.43) | (.55) | (.42) | |
| Bias Parameter C′ | ||||
| Baseline | 0.23 | 0.21 | 0.66 | 0.34 |
| (.36) | (.42) | (.43) | (.37) | |
| Anesthesia | 0.48 | 0.67 | 0.64 | 0.62 |
| (.40) | (.44) | (.48) | (.56) | |
Note: Standard deviations in parentheses.
Table 4 also presents the cell means for the bias measure C, also at the confidence scale rating of 4. ANOVA revealed significant main effects of both group, F(3,36) = 4.83, MSe = .296, p < .001, and condition, F(1,36) = 33.99, MSe = .078, p < .0001; again, these effects were qualified by a significant two-way interaction, F(3,36) = 8.14, MSe = .078, p < .001. The within-group comparisons of waking to anesthesia condition were as follows. lows: F(1,9) = .73, MSe = .037, n.s.; mediums: F(1,9) = 8.15, MSe = .054, p < .05; highs: F(1,9) = 3.3, MSe = .064, n.s.; virtuosos: F(1,9) = 24.67, MSe = .158, p < .001. All groups became more conservative during hypnotic anesthesia: this tendency was significant for the mediums, and quite pronounced for the virtuoso subjects.
Alternative bias parameter C′
Traditional psychophysical methods showed a significant reduction in sensory acuity when highly hypnotizable subjects receive hypnotic suggestions for tactile anesthesia. However, the initial signal-detection analysis did not produce a clear choice between an actual change in sensitivity on the one hand, and a mere change in response criterion on the other. The fact that both the sensitivity and criterion changed should not be interpreted as indicating that subjects deliberately and strategically changed their criterion for judging the presence of the stimulus in response to the suggestion for anesthesia – i.e., saying “No” (indicating stimulus absence) where they formerly would have said “Yes” (indicating stimulus presence). Subjects do say “No” more frequently during anesthesia, but a little reflection indicates that this must be so.
Consider a subject who, on baseline trials (without anesthesia), judged the presence and absence of the stimulus with 100% accuracy, saying “Yes” on the 50% of trials where the stimulus was present and “No” on the 50% of the trials where the stimulus was absent. Consider, further, the performance of the same subject under conditions of hypnotic anesthesia – i.e., a subject who can no longer feel stimuli that formerly were palpable. This subject will say “No” to the 50% of trials in which the stimulus is absent, as before; but he or she will also say “No” to some portion of the 50% of trials in which the stimulus is present. This will result in an increase in “No” responses, but not because of bias or any adjustment of a criterion for responding “Yes.” The increase in “No” responses occurs because the stimulus is not felt, and thus is judged to be absent.
Thus, signal-detection theory presents the investigator with a paradox. While the parameters estimating sensitivity are independent of those estimating bias, the reverse is not true: the parameters estimating bias depend intimately on those estimating sensitivity. The essence of this paradox was recognized by Collyer (1981), who has shown that the bias estimate β and the sensitivity measure d′ are algebraically related to each other, and hence, are not independent. While this one-way dependency between sensitivity and bias is not problematic within a single observational session, it is problematic when comparisons are made across sessions in which experimental or other manipulations have changed the observer’s sensitivity. Under these circumstances, changes in sensitivity contaminate any indices of bias, possibly causing significant artifactual changes to appear, when in fact the observer had not changed his or her criterion for response. Conversely, a change in sensitivity across sessions can mask a genuine change in the subject’s criterion across the sessions, provided that the second response criterion is the same relative distance from the new intersection of the two signal and signal-plus-noise distributions.
An accurate comparison of response criteria can be made across experimental sessions, even in the presence of a change in sensitivity, by assuming that the noise-alone distribution does not change from one condition to the next. Thus, its mean can serve as an anchor point by which the two sets of signal and signal-plus-noise distributions can be examined relative to each other. Under these constraints, a new bias measure, in this case C′, can be derived as the distance between the subject’s response criterion and optimal responding (the intersection point).
Table 4 also shows the results for this new bias measure, C′. A repeated measures ANOVA for the confidence criterion of 4 revealed a condition effect, F(1,36) = 10.15, MSe = .120, p < .01. However, unlike the analyses of C, the main effect of group was not significant, F(3,36) = 1.15, MSe = .264, n.s., nor was there a significant interaction between group and condition, F(3,36) = 1.59, MSe = .120, n.s. Thus, while the initial analysis of response bias using C indicated that the Highs had become significantly more conservative than the other groups in setting their response criterion (relative to the waking condition), the analyses of C′ showed this to be artifactual, a function of this group’s greater decrement in sensitivity. Table 6 show the means and standard deviations of C′.
Table 6.
Signal-Detection Parameters, Experiment 2A
| Group | N | Condition | ||
|---|---|---|---|---|
| Baseline | Anesthesia | Hyperesthesia | ||
| Sensitivity Parameter P(A) | ||||
| Simulators | 9 | 0.81 | 0.67 | 0.76 |
| (.08) | (.10) | (.13) | ||
| Reals | 10 | 0.78 | 0.64 | 0.75 |
| (.09) | (.09) | (.12) | ||
| Bias Parameter C | ||||
| Simulators | 9 | 0.48 | 1.67 | 0.30 |
| (.37) | (.50) | (.61) | ||
| Reals | 10 | 0.25 | 1.51 | −0.05 |
| (.33) | (.76) | (.51) | ||
| Bias Parameter C′ | ||||
| Simulators | 9 | 0.48 | 1.03 | 0.17 |
| (.37) | (.31) | (.70) | ||
| Reals | 10 | 0.25 | 1.23 | −0.13 |
| (.33) | (.69) | (.76) | ||
Note: Standard deviations in parentheses.
Discussion
Assessment of tactile sensitivity via classic psychophysical methods indicated a significant interaction between hypnotic suggestions for anesthesia and hypnotizability. Lows and mediums showed no changes, whereas highs and virtuosos showed respectively greater increments in threshold. Initial analyses of tactile sensitivity with traditional signal detection parameters P(A) and C suggested that these changes were mediated by changes in both sensitivity and response criterion, and that Highs were significantly more conservative in responding, relative to baseline, than the other groups. Subsequent analyses using the revised bias parameter C′, however, showed that the apparent interaction between group and condition in response criterion changes was artifactual, a result of the virtuosos experiencing larger changes in sensitivity than the other groups, and signal detection theory’s inability to accurately access changes in bias in the presence of such changes. In other words, highly hypnotizable subjects showed genuine changes in tactile sensitivity.
Experiment 2
Experiment 1 established that suggestions for hypnotic anesthesia do lead to actual decrements in tactile sensitivity, the magnitude of which is related to hypnotizability. However, there are still other factors to be examined. First, can tactile sensitivity be enhanced as well as diminished? Experiment 2 replicated the basic findings of Experiment 1 and, in light of the provocative findings obtained by Graham and Liebowitz (1972; see also Sheehan, Smith, & Forrest, 1982), added suggestions for hyperesthesia, i.e., increased tactile sensitivity, as well (for a critique of these experiments, see (Raz, Marinoff, Zephrani, Schweizer, & Posner, 2004).
In addition, Experiment 2 was designed evaluate the demand characteristics of the initial experiment and take account of potential baseline and carryover effects. As Orne (1962, 1969, 1979) and many others have noted, subjects in psychological experiments are sentient beings who are motivated to discover what the experimental hypotheses are. Demand characteristics cannot be controlled in such a manner, because they can arise from sources that are outside the experimenter’s control. For this purpose, Orne advocated use of a quasi-control group of simulators who are insusceptible to hypnosis but instructed to simulate the behavior of their highly hypnotizable counterparts.
In addition to demand characteristics, which are a problem for any experiment, there are special problems inherent in any experiment in which subjects receive suggestions for enhanced performance (Evans & Orne, 1965; Sheehan & Perry, 1976). In particular, a subject’s knowledge that he or she is participating in a hypnotic experiment will often change baseline performance. For example, a subject, knowing that in the next condition he or she will be asked to increase sensitivity, may intentionally or unintentionally lower performance during baseline assessment in order to demonstrate a subsequent gain. In this study, by having each subject participate in the anesthesia and hyperesthesia as well as the baseline conditions, there is little a subject can do to strategically influence the baseline sensitivity. In addition, the order of conditions was counter-balanced within each group, so that effects that might have occurred as a result of encountering a given condition first, will be cancelled out. Simple between-subjects comparison of baseline levels of performance with experiment one will determine if this strategy is being employed.
Related to these baseline effects, work by Watson and Clopton (1969) has shown that subjects in signal-detection experiments vary as to when they reach stable asymptotic performance. If baseline assessment is terminated before the subject’s performance has reached asymptote, the changes attributed to an experimental manipulation may simply be part of the subject’s continued movement towards asymptotic responding. Accordingly, each condition in Experiment 2 was partitioned into five blocks of 30 trials each, in order to permit an empirical determination of any effects of nonasymptotic performance.
Method
Subjects
A total of 22 undergraduates were selected on the basis of their scores on the SHSS:C. One subject was used as a pilot subject and procedural difficulties resulted in the loss of 2 subsequent subjects, leaving 19 subjects for the final analyses: 10 subjects who scored between 9 and 12 constituted the “real” group in Orne’s real-simulating paradigm; the remaining 9 subjects, who scored between 1 and 4 on SHSS:C, constituted the simulator group. Subjects received experimental participation credits, a monetary payment of $10.00, or a combination of the two as reimbursement for their participation.
Apparatus
The apparatus used was the same as that utilized in Experiment 1, except for two changes. Subjects’ responses were collected via a specially constructed, six-button response box, rather than the earlier two-step process employing a computer mouse. Moreover, while all assessments of sensitivity in Experiment 1 were obtained while the subject had his or her eyes closed, a box-blind was employed in Experiment 2 to isolate subjects from visual cues.
Procedure
The basic procedure was identical to that of Experiment 1, with the following exceptions. At the beginning of the session, each subject was met by a second experimenter (Martha Glisky), who administered either “real” or “simulating” instructions to each subject and carried out the postexperimental interviews, strictly following the procedures outlined by Orne. Upon entering the experimental room, each subject was familiarized with the response box until they could reliably push the button that corresponded to each response judgment. The response judgment criteria were explained to each subject while they were being shown a card with the following definitions.
1 = Very confident a touch did not occur
2 = Fairly confident a touch did not occur
3 = Just guessing a touch did not occur
4 = Just guessing a touch did occur
5 = Fairly confident a touch did occur
6 = Very confident a touch did occur
For purposes of exposition, the presentation of Experiment 2 is divided into two sections. Experiment 2A is, essentially, a replication of Experiment 1 comparing reals and simulators and anesthesia and hyperesthesia suggestions. Experiment 2B focused solely on anesthesia and expressly manipulated subjects’ response strategies.
Experiment 2A
The DRIS threshold determination procedure was performed only once, during the baseline condition, for the sole purpose of selecting the threshold stimulus to be used for the signal detection conditions in the experiment. Signal detection assessments of baseline sensitivity and of the two main perceptual alteration conditions utilized five blocks of 30 trials each.
The order of the suggestions for anesthesia and hyperesthesia was counterbalanced for both reals and simulators. The main experimenter was blind to the real/simulating status of the subject. The experimenter recorded his judgment of the real/simulating status of each subject after completion of the hypnotic induction. Judgments were done on a 0 to 1 probability scale, with 1 representing high confidence the subject was a real, 0 representing high confidence the subject was a simulator, and .5 denoting an inability to decide either way.
At the end of each suggestion condition the subject rated hypnotic depth and the suggestion for altered sensitivity was cancelled. Ratings of hypnotic depth were also taken after each block of trials within each condition. A brief rest period was given between each condition, during which suggestions for increasing hypnotic depth were given. Subjects were asked to move their hands after the third block of trials in each suggestion condition, in order to alleviate the effects of any physical fatigue on tactile sensitivity.
Experiment 2B
After completion of these three conditions and a brief rest period, two more conditions manipulating the subject’s strategy for responding were conducted. Subjects whose immediately prior suggestion was for hyperesthesia had this suggestion cancelled and received new suggestions for anesthesia. Subjects whose final suggestion was for anesthesia simply continued to the next conditions. In the “Sure” condition the subject was instructed to respond only if he or she was “absolutely sure” a touch had occurred. To further emphasise this strategy, the subject was instructed to use only buttons 1 and 6 (the two “very confident” response buttons). In the “Guess” condition, the subject was told to respond using buttons 3 and 4, the two “guessing” buttons; pressing button 4 if he or she had “any kind of a leaning or intuition” that a touch had occurred. One block of 30 trials was run for each condition. The order of occurrence for these two conditions was randomly counterbalanced across subjects. The hypnosis session was terminated after all five conditions had been run. Total session time for each subject was approximately 2 hours. After the experiment proper had terminated, each subject was given two postexperimental interviews, one by the main experimenter, and one by the second experimenter who had administered the real or simulating instructions. The second interview was conducted after the simulators were finished “simulating.” Thus, this second interview is generally taken to be an accurate reflection of the subjective experience of simulators during the time of the hypnosis session.
Results
During the DRIS procedure, all subjects converged on a stable threshold within the allotted 30 trials. The average trial on which convergence occurred was 10.30 (SD = 2.00) and 11.22 (SD = 1.99) for the reals and simulators respectively. This difference is not significant, F(1,17) = 1.01, MSe = 3.97, n.s. The average baseline tactile threshold was identical for both reals and simulators, falling between the 2nd and 3rd aesthesiometers of the series; approximately 51.28 milligrams of force. The average reaction time (with outliers removed) for all trials after convergence was 1.50 seconds (SD = .54) for reals, and 1.75 seconds (SD = .39) for simulators. This difference was not significant, F(1,17) = 1.28, MSe = .226, p > .05. As in Experiment 1, both groups readily satisfied the criterion for rating-scale usage.
Signal-detection analysis
Table 5 displays the means and standard deviations of the hit and false alarm rates at confidence level 4, for the two groups of subjects in each of the three conditions. Table 6 displays the corresponding figures for the various signal-detection parameters.
Table 5.
Hit and False Alarm Rates at Confidence Level 4, Experiment 2A
| Group | N | Condition | ||
|---|---|---|---|---|
| Baseline | Anesthesia | Hyperesthesia | ||
| Hit Rate | ||||
| Simulators | 9 | 0.68 | 0.17 | 0.70 |
| (.24) | (.15) | (.16) | ||
| Reals | 10 | 0.76 | 0.24 | 0.70 |
| (.12) | (.24) | (.14) | ||
| False Alarm Rate | ||||
| Simulators | 9 | 0.07 | 0.03 | 0.15 |
| (.03) | (.02) | (.13) | ||
| Reals | 10 | 0.17 | 0.05 | 0.31 |
| (.13) | (.07) | (.25) | ||
Note: Standard deviations in parentheses.
The mixed-design ANOVA on the sensitivity parameter P(A) showed a significant effect of condition, F(2,34) = 34.01, MSe = 0.487, p < .0001). Newman-Keuls post-hoc analyses revealed the mean sensitivity for the anesthesia condition (0.66, SD = .12) was significantly lower than the means of both the baseline (0.80, SD = .10) and the hyperesthesia (0.76, SD = .13) conditions, but that the latter two means were not significantly different from each other. Reals and simulators did not differ from each other, nor was the two-way interaction significant.
The ANOVA on the index of bias, C, gave similar results: only the condition factor was significant, F(2,34) = 65.18, MSe = .178, p < .0001. Both reals and simulators became more conservative in the anesthesia condition, and more liberal in the hyperaesthesia condition. As in Experiment 1, however, this apparent change in response criterion may have been an artifact of the change in sensitivity experienced by the subjects in the anesthesia condition. Accordingly, as before, analysis of C′ was performed. The ANOVA for C′ also revealed a significant effect only for condition, F(2,34) = 26.79, MSe = .229, p < .0001. The changes in response criterion were much smaller than those indicated by the analyses of C: the average difference between the baseline and anesthesia condition was approximately 1–1/4 standardized units, approximately half a standard deviation greater than the difference in C′. The differences between the hyperesthesia and baseline sensitivity for the two criterion measures were quite similar, which is expected given the insignificant change in sensitivity.
Effects of response strategy on sensitivity and bias
In Experiments 1 and 2A, the subjects were free to set their own criterion for responding in the signal-detection procedure. For Experiment 2B, however, response criteria were explicitly imposed on them: either a very strict “Sure” criterion in which only certainty that the stimulus was present counted, or a “Guessing” criterion, in which any uncertainly that the stimulus was absent counted as a “Yes.” The results are shown in Table 7.
Table 7.
Signal-Detection Parameters as a Function of Response Strategy, Experiment 2B
| Group | N | Strategy | |
|---|---|---|---|
| Guess | Sure | ||
| Sensitivity Parameter P(A) | |||
| Simulators | 9 | 0.64 | 0.57 |
| (0.06) | (0.07) | ||
| Reals | 10 | 0.62 | 0.57 |
| (0.12) | (0.12) | ||
| Bias Parameter C | |||
| Simulators | 9 | 0.96 | 1.46 |
| (0.30) | (0.39) | ||
| Reals | 10 | 1.07 | 1.38 |
| (0.50) | (0.60) | ||
| Bias Parameter C′ | |||
| Simulators | 9 | 1.23 | 1.46 |
| (0.40) | (0.39) | ||
| Reals | 10 | 1.23 | 1.38 |
| (0.58) | (0.60) | ||
The repeated-measures ANOVA of P(A), contrasting the effects of the “Sure” and “Guessing” conditions, as a function of real/simulator status, revealed only a significant effect of condition, F(1,17) = 14.18, MSe = .002, p < .01. The difference between the two conditions, collapsed across groups, represents an 85% increase in above-chance responding as the subjects changed their strategy for responding from “very confident” to “just guessing” that a touch occurred. While earlier analyses did not find a significant block effect, the fact that the sensitivity estimate for both Groups in this condition was lower than the prior estimates of sensitivity in the anesthesia condition, suggests that fatigue was effecting the subjects’ performances.
The ANOVA of the bias parameter C showed only a significant effect of condition, F(1,17) = 22.67, MSe = .068, p < .002. This effect was in the expected direction, with the “Sure” condition invoking a more conservative response set in both groups. Table 7 shows the means and standard deviations as a function of group by condition.
As with the other analyses of Experiments 1 and 2A, the bias index C′ was calculated to obtain an index of response bias uncontaminated by the change in sensitivity which occurred between the Sure and the Guess conditions. The repeated measures ANOVA produced a significant effect of condition, F(1,17) = 5.86, MSe = .055, p < .05, and no effect of group nor interaction. Note that as with the other comparisons between C and C′, this analysis indicates a much smaller change in response criterion between the two conditions. Interestingly, even though subjects have been instructed to guess, the response criterion is still quite conservative in comparison to either the baseline or hyperesthesia conditions. None of the subjects are saying “Yes” to everything.
Analyses of experimenter judgments and expectancies
A cross-tabulation of actual subject status (real/simulator) by the experimenter’s rating of subject status yielded a hit rate of.67 and the false alarm rate of.50. A X2 analysis based on the 2×2 contingency table showed that the experimenter was no more accurate in detecting reals and simulators than would be expected by chance (X2(1) = .88, n.s.).
In order to examine the possible influence of the experimenter’s perception of the real/simulating status of a subject on the subject’s response to the hypnotic suggestions, sensitivity and bias parameters were recalculated using perceived status in place of actual group status. Neither the main effect of Perceived Status nor the interaction of Perceived Status and Condition approached significance for any of the signal-detection parameters, P(A), C, or C′. In the absence of any experimenter expectancy effects on these conditions, no further analyses were conducted.
Postexperimental interviews
During the postexperimental interview with the main experimenter, all subjects (i.e., regardless of their actual real/simulating status), claimed to experience genuine alterations in tactile sensitivity for each of the two hypnotic suggestions (anesthesia and hyperesthesia). This was not true during the second interview with the experimenter who had set the subjects up for their roles. On an open-ended question, designed to elicit spontaneous descriptions of their experience, 8 of the 10 reals reported experiencing a genuine decrement in sensitivity, usually described as the hand becoming numb or tingly or, in 1 case, cold. Only 1 simulator described a similar experience. When asked whether they had actually lost sensitivity or just changed what they considered a touch, 5 reals maintained that they had simply lost tactile sensitivity in the area of the circle, 3 said that they had changed their definition of a touch, and 1 said both had happened; 7 simulators changed their definition of a touch.
In response to the general question about their experience of hyperesthesia, 4 reals and 4 simulators reported experiencing an increase in tactile sensitivity, while 8 reals and 7 simulators claimed a better ability to tell when they had or had not been touched, 8 reals and 7 simulators responded positively – despite the fact that subjects did not, in fact, display any objective increase in sensitivity.
General Discussion
Both experiments showed apparent threshold changes during hypnotic tactile anesthesia, as measured by traditional psychophysical methods. These changes in sensitivity, as measured by P(A), were confirmed by the signal detection analyses. Signal-detection analyses also indicated changes in response bias (as measured by C) in both experiments, with suggestions for anesthesia inducing a large conservative response criterion shift, especially so for the virtuosos in Experiment 1. However, analyses of C′ showed that much of this change was an artifact of changes in sensitivity across the conditions. In fact, once the changes in sensitivity were accounted for, the virtuosos showed no greater change in response criterion than the other groups. This finding was confirmed in Experiment 2A. In contrast to suggestions for anesthesia, suggestions for hypnotic hyperesthesia had no effects on sensitivity. Experimentally manipulating the subject’s response strategy to encourage guessing increased sensitivity in the anesthesia condition.
Insusceptible subjects instructed to simulate hypnosis showed a pattern of performance in the anesthesia and hyperesthesia conditions that closely mimicked that of the real hypnotic subjects. The postexperimental interviews however, indicated that the reals and simulators had very different subjective experiences during the different hypnotic suggestions. The experimenter to be unable to differentiate reals from simulators; and in any event his impressions did not influence the subjects’ responses to the experimental manipulations.
While suggestion-induced differences in thresholds, as estimated by traditional psychophysical methods, may be readily dismissed as being a function of suggestion-induced changes in response biases, this cannot be said for changes in acuity that are manifested in signal-detection paradigm. Hypnotic suggestions for anesthesia produce real changes in tactile sensitivity. These changes vary linearly with hypnotizability, with virtuosos showing the greatest effects, and lows showing none. While several virtuosos in Experiment 1 showed a complete loss of tactile sensitivity, the average decrement in this group, as measured by the change in above-chance responding, was 47%. These outcomes are likely not an artifact of baseline or carryover affects, as subjects at all levels of hypnotizability had nearly identical baseline sensitivity. This result, in conjunction with the fact that lows do not show any effect of anesthesia suggestions, indicates that the baseline assessments of sensitivity are uncontaminated by strategic responding on the part of the more hypnotizable subjects.
Looking across Experiments 1 and 2, we find a small but insignificant decrease in baseline responding for the virtuosos (t18 = .99, n.s.) and lows/simulators (t17 = 1.26, n.s.). Even if the changes had be significant, the fact that they were both negative, suggests that such an alleged strategy would be for subsequently exhibiting hypersensitivity. However, this hypothesis is made untenable by the fact that there was only a significant effect of suggestions for anesthesia in Experiment 2 and a small insignificant decrease in the hyperesthesia condition (likely an effect of fatigue). Finally, assessment of experimenter effects indicated only chance classification of subjects into real and simulators, and no relationship between perceived status and experimental outcome. The final conclusion is that suggestions for anesthesia produce genuine decrements in tactile sensitivity.
There was no significant effect of suggestions for hyperesthesia in this experiment. This contrasts with the significant, rather large effects on visual acuity obtained by Graham and Liebowitz (1972) and Sheehan et al. (1982). There are several possible reasons for this. One is that this present study used near-liminal stimuli and tried to increase sensitivity beyond this, while the visual enhancement studies used myopic individuals, who suffer from chronic below-optimal sensory functioning. The nature of the tasks in the two studies are also quite different: threshold detection has to do with the raw ability to detect a stimulus, while sensory acuity has to do with the ability to discriminate stimuli once detection has occurred. Additionally, the visual acuity studies gave rather indirect suggestions for increased visual functioning (“relax the muscles of the eye”), while the present experiment used direct, explicit suggestions to enhance performance, mirroring the suggestions for tactile anesthesia.
Experiment 2 found no behavioral differences between reals and simulators in any of the conditions—baseline, anesthesia, or hyperesthesia. Apparently, the demand characteristics in the experimental setting were sufficient to guide a simulator to behave similarly to a genuinely hypnotized person. This in no way, however, impeaches the accomplishment of the latter nor informs as to the actual mechanism by which the reals achieved their decrements in tactile sensitivity. Further inquiry into these mechanisms is accomplished through critical examinations of the postexperimental inquiries.
As expected, both groups responded similarly to the postexperimental interview when it was administered by the main experimenter—the reals were describing their phenomenal experiences during the course of the experiment, and the simulators continued to generate the responses they thought appropriate to a highly hypnotizable subject. However, during the second postexperimental interview, when the demands of the experimental context had been withdrawn, it became clear that while the behaviors of the two groups had been identical, they were accompanied by very different experiences. The majority of the reals continued to report the phenomenal experience of losing tactile sensation during the anesthesia condition, while only 1 simulator expressed a similar claim. The simulators described either changing their definition of what they would call a touch or of other strategies, such as concentrating less during that condition. This same pattern holds for the testimonies regarding phenomenal experience during suggestions for hypersensitivity. Here, even though an equal number of reals and simulators felt they had experienced genuine hyperesthesia, over half of the simulators again reported using intentional strategies to do so (e.g., increasing concentration). The reals did not. This general result, in which reals and simulators behave similarly but via different mechanisms or with different subjective experiences, is consistent with other literature in the area (McConkey, Bryant, Bibb, & Kihlstrom, 1991; Miller & Bowers, 1986).
Both the psychophysical and signal-detection methods of analysis found decreased sensitivity in the anesthesia condition and no effects of suggestions for hyperesthesia. These results are consistent with Hilgard’s (1973, 1977) neodissociation theory of divided consciousness. According to Hilgard, normal mental functioning reflects an integration between executive control functions and the various subsystems of control needed to execute given tasks. Under certain circumstances however, this integrated functioning is sometimes disrupted—for example, by erection of an amnesia-like dissociative barrier between the executive control functions and the cognitive subsystems that have been responsible for the cognitive processes and actions during the disrupted state. Hilgard employs this model to explain many of the core phenomena of hypnosis, such as hypnotic analgesia, posthypnotic amnesia, and the experience of involuntariness in responding to suggestions. In the same manner, hypnotic tactile anesthesia could reflect the dissociation of the subsystem responsible for tactile sensation from executive monitoring, effectively blocking or diminishing the phenomenal experience of being touched. The ineffectiveness of suggestions for hyperaesthesia, as found in Experiment 2, is also predicted by this model: executive control can be dissociated from a subsystem’s output, but there is no mechanism by which the output of a subsystem can be augmented.
While Experiments 1 and 2A showed clearly that tactile anesthesia experienced displayed by highly hypnotizable subjects was not an artifact of shifts in response criterion, Experiment 2B presented a seeming paradox: a shift in criterion—from “sure” to “guess” resulted in a significant increase in sensitivity. The apparent paradox is that a shift in response criterion produced a change in sensitivity as measured by a statistic that is supposedly bias-free—that is, independent of the criterion employed for responding. This result is not completely anomalous however, as analogous findings have been reported in the domain of memory.
It is now commonplace to distinguish between two expressions of memory (for reviews, see Kihlstrom, Dorfman, & Park, 2015; Schacter, 1987). Explicit memory refers to conscious recollection, such as reflected in standard tests of recall and recognition; implicit memory refers to any change in experience, thought, or action that is attributable to memory, such as perceptual and semantic priming effects. Explicit and implicit memory can be dissociated, as when amnesic patients (and normal subjects) show priming in the absence of, or independent of, recall or recognition. Nevertheless, Mandler’s (1980) dual-process theory of memory retrieval holds that recognition can be mediated not just by the retrieval of trace information, but also by a priming-based feeling of familiarity (see also Jacoby, 1991; Jacoby & Kelley, 1991; Yonelinas & Jacoby, 2012). For this reason, even amnesic patients, who lack conscious recollection, can strategically rely on this feeling of familiarity to perform at above-chance levels on tests of recognition (e.g., Dorfman, Kihlstrom, Cork, & Misiaszek, 1995; Hirst et al., 1986; Hirst, Johnson, Phelps, & Volpe, 1988; Mieke Verfaellie & Cermak, 1999; M. Verfaellie, Giovanello, & Keane, 2001).
Perhaps something similar occurs in sensation and perception. Following Schacter’s distinction between explicit and implicit memory, we can draw a distinction between two expressions of perception (Kihlstrom, 1996, 2012; Kihlstrom, Barnhardt, & Tataryn, 1992): explicit perception refers to conscious sensation and perception, as exemplified by the conscious detection of a stimulus or the recognition of an object; implicit perception refers to any change in experience, thought, or action which is attributable to a stimulus, in the absence of, or independent of, conscious awareness of that stimulus. As with memory, explicit and implicit perception can be dissociated: examples include “blindsight” (Jackson, 2000; Weiskrantz, 1986) and “subliminal” or masked priming (e.g., Marcel, 1983; Merikle & Reingold, 1990). But just as priming can contribute to performance on recognition tasks, it is possible that priming can contribute to performance on stimulus-detection tasks. That is, subjects may achieve above-chance levels of stimulus-detection by strategically relying on the feeling of familiarity and accompanies priming. Subjects may be more likely to employ this strategy when they are encouraged to guess about the presence of the signal, as opposed to cautioned to say “Yes” only when they are certain, i.e., when they shift criterion from certainty to guessing. As with guessing on multiple-choice tests, this increase in hits will be accompanied by an increase in false alarms. But so long as the stimulus is present on at least some trials, and a priming-like process gives rise to a feeling of familiarity, hits will exceed false alarms, resulting in an increase in even bias-free measures of sensitivity.
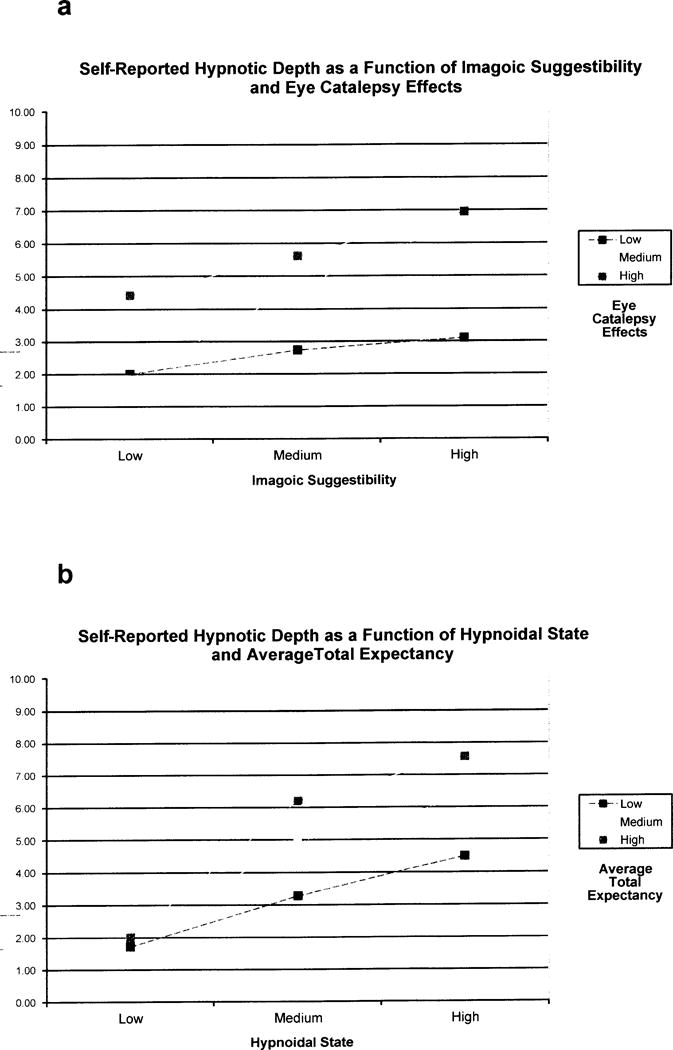
Figure 1.
Acknowledgments
This paper is based on a doctoral dissertation completed at the University of Arizona by DJT, supported in part by Grant #MH-35856 from the National Institute of Mental Health and in part by a dissertation grant from the American Psychological Association (Tataryn, 1992). Thanks to the other members of the dissertation committee: Richard Bootzin, Lynn Nadel, Mary Peterson, and Varda Shoham; A.J. Figueredo for statistical advice; and Martha Glisky for preparing and debriefing the reals and simulators in Experiment 2.
References
- Collyer CE. The algebra and geometry of β. Bulletin of the Psychonomic Society. 1981;17:61–62. [Google Scholar]
- Cornsweet TN. The staircase method in psychophysics. American Journal of Psychology. 1962;75:485–491. doi: http://dx.doi.org/10.2307/1419876. [PubMed] [Google Scholar]
- Crawford JH, Macdonald H, Hilgard ER. Hypnotic deafness–psychophysical study of responses to tone intensity as modified by hypnosis. American Journal of Psychology. 1979;92:193–214. doi: http://dx.doi.org/10.2307/1421920. [PubMed] [Google Scholar]
- Dorfman J, Kihlstrom JF, Cork RC, Misiaszek J. Priming and recognition in ECT-induced amnesia. Psychonomic Bulletin & Review. 1995;2(2):244–248. doi: 10.3758/BF03210964. doi: http://dx.doi.org/10.3758/BF03210964. [DOI] [PubMed] [Google Scholar]
- Egan JP, Clarke FR. Psychophysics and signal detection. In: Sidowsky JB, editor. Experimental Methods and Instrumentation in Psychology. New York, NY: McGraw-Hill; 1966. pp. 211–246. [Google Scholar]
- Eiblmayr K. Trance logic and the circle-touch test. Australian Journal of Clinical and Experimental Hypnosis. 1987;15:113–145. [Google Scholar]
- Evans FJ, Orne MT. Motivation, performance, and hypnosis. International Journal of Clinical and Experimental Hypnosis. 1965;13:103–116. doi: 10.1080/00207146508412932. [DOI] [PubMed] [Google Scholar]
- Graham C, Leibowitz HW. The effect of suggestion on visual acuity. International Journal of Clinical and Experimental Hypnosis. 1972;20:169–186. doi: 10.1080/00207147208409288. doi: http://dx.doi.org/10.1080/00207147208409288. [DOI] [PubMed] [Google Scholar]
- Green DM, Swets JA. Signal detection theory and psychophysics. New York, NY: Wiley; 1966. [Google Scholar]
- Herrick RM. Psychophysical methodology: VI. Random method of limits. Perception & Psychophysics. 1973;13:548–554. doi: http://dx.doi.org/10.3758/BF03205818. [Google Scholar]
- Hilgard ER. A quantitative study of pain and its reduction through hypnotic suggestion. Proceedings of the National Academy of Sciences. 1967;57:1581–1586. doi: 10.1073/pnas.57.6.1581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hilgard ER. Pain as a puzzle for psychology and physiology. American Psychologist. 1969;24:103–113. doi: 10.1037/h0027146. doi: http://dx.doi.org/10.1037/h0027146. [DOI] [PubMed] [Google Scholar]
- Hilgard ER. A neodissociation interpretation of pain reduction in hypnosis. Psychological Review. 1973;80:396–411. doi: 10.1037/h0020073. doi: http://dx.doi.org/10.1037/h0020073. [DOI] [PubMed] [Google Scholar]
- Hilgard ER. Divided consciousness: Multiple controls in human thought and action. New York, NY: Wiley-Interscience; 1977. [Google Scholar]
- Hilgard ER, Hilgard JR. Hypnosis in the relief of pain. Los Altos, Ca.: Kaufman; 1975. [Google Scholar]
- Hirst W, Johnson MK, Kim JK, Phelps EA, Risse G, Volpe BT. Recognition and recall in amnesics. Journal of Experimental Psychology: Learning, Memory, & Cognition. 1986;12:445–451. doi: http://dx.doi.org/10.1037/0278-7393.12.3.445. [PubMed] [Google Scholar]
- Hirst W, Johnson MK, Phelps EA, Volpe BT. More on recognition and recall with amnesia. Journal of Experimental Psychology: Learning, Memory, & Cognition. 1988;14:758–762. doi: 10.1037//0278-7393.14.4.758. doi: http://dx.doi.org/10.1037/0278-7393.14.4.758. [DOI] [PubMed] [Google Scholar]
- Hodos W. Nonparametric index of response bias for use in detection and recognition experiments. Psychological Bulletin. 1970;74:351–354. doi: http://dx.doi.org/10.1037/h0029933. [Google Scholar]
- Jackson SR. Beyond dissociation: Interaction between dissociated implicit and explicit processing. Amsterdam, Netherlands: John Benjamins Publishing Company; 2000. Perception, awareness and action: Insights from blindsight; pp. 73–98. [Google Scholar]
- Jacoby LL. A process dissociation framework: Separating automatic from intentional uses of memory. Journal of Memory & Language. 1991;13:513–541. doi: http://dx.doi.org/10.1016/0749-596X(91)90025-F. [Google Scholar]
- Jacoby LL, Kelley C. Unconscious influences of memory: Dissociations and automaticity. In: Milner D, Rugg M, editors. The neuropsychology of consciousness. San Diego: Academic; 1991. pp. 201–203. [Google Scholar]
- Janet P. The major symptoms of hysteria. New York, NY: Macmillan; 1907. [Google Scholar]
- Jesteadt W. An adaptive procedure for subjective judgments. Perception & Psychophysics. 1980;28:85–88. doi: 10.3758/bf03204321. doi: http://dx.doi.org/10.3758/BF03204321. [DOI] [PubMed] [Google Scholar]
- Jones B, Spanos NP. Suggestions for altered auditory sensitivity, the negative subject effect, and hypnotic susceptibility: A signal-detection analysis. Journal of Personality and Social Psychology. 1982;43:637–647. doi: 10.1037//0022-3514.43.3.637. doi: http://dx.doi.org/10.1037/0022-3514.43.3.637. [DOI] [PubMed] [Google Scholar]
- Kihlstrom JF. Perception without awareness of what is perceived, learning without awareness of what is learned. In: Velmans M, editor. The science of consciousness: Psychological, neuropsychological and clinical reviews. London, England UK: Routledge; 1996. pp. 23–46. [Google Scholar]
- Kihlstrom JF. Unconscious processes. In: Reisberg D, editor. Oxford Handbook of Cognitive Psychology. Oxford: Oxford University Press; 2012. pp. 176–186. [Google Scholar]
- Kihlstrom JF, Barnhardt TM, Tataryn DJ. Implicit perception. In: Bornstein RF, Pittman TS, editors. Perception without awareness: Cognitive, clinical, and social perspectives. New York, NY, USA: The Guilford Press; 1992. pp. 17–54. [Google Scholar]
- Kihlstrom JF, Dorfman J, Park L. Conscious and unconscious memory. In: Schneider S, Velmans M, editors. Blackwell companion to consciousness. 2nd. Oxford: Wiley; 2015. in press. [Google Scholar]
- Macmillan NA, Creelman CD. Response bias: Characteristics of detection theory, threshold theory, and nonparametric indexes. Psychological Bulletin. 1990;107:401–413. doi: http://dx.doi.org/10.1037/0033-2909.107.3.401. [Google Scholar]
- Macmillan NA, Creelman CD. Detection theory: a user’s guide. New York, NY: Cambridge University Press; 1991. [Google Scholar]
- Mandler G. Recognizing: The judgment of previous occurrence. Psychological Review. 1980;87(3):252–271. doi: http://dx.doi.org/10.1037/0033-295X.87.3.252. [Google Scholar]
- Marcel AJ. Conscious and unconscious perception: Experiments on visual masking and word recognition. Cognitive Psychology. 1983;15:197–237. doi: 10.1016/0010-0285(83)90009-9. doi: http://dx.doi.org/10.1016/0010-0285(83)90009-9. [DOI] [PubMed] [Google Scholar]
- Markowitz J, Swets JA. Factors affecting the slope of empirical ROC curves: Comparison of binary and rating responses. Perception & Psychophysics. 1967;2:91–100. doi: http://dx.doi.org/10.3758/BF03210301. [Google Scholar]
- McConkey KM, Bryant RA, Bibb BC, Kihlstrom JF. Trance logic in hypnosis and imagination. Journal of Abnormal Psychology. 1991;100(4):464–472. doi: 10.1037//0021-843x.100.4.464. doi: http://dx.doi.org/10.1037/0021-843X.100.4.464. [DOI] [PubMed] [Google Scholar]
- McConkey KM, Bryant RA, Bibb BC, Kihlstrom JF, Tataryn DJ. Hypnotically suggested anaesthesia and the circle-touch test: A real-simulating comparison. British Journal of Experimental & Clinical Hypnosis. 1990;7(3):153–157. [Google Scholar]
- Merikle PM, Reingold EM. Recognition and lexical decision without detection: Unconscious perception? Journal of Experimental Psychology: Human Perception & Performance. 1990;16:574–583. doi: 10.1037//0096-1523.16.3.574. doi: http://dx.doi.org/10.1037/0096-1523.16.3.574. [DOI] [PubMed] [Google Scholar]
- Miller ME, Bowers KS. Hypnotic analgesia and stress inoculation in the reduction of pain. Journal of Abnormal Psychology. 1986;95:6–14. doi: 10.1037//0021-843x.95.1.6. doi: http://dx.doi.org/10.1037/0021-843X.95.1.6. [DOI] [PubMed] [Google Scholar]
- O’Connell DM. An experimental comparison of hypnotic depth measured by self-ratings and by an objective scale. International Journal of Clinical and Experimental Hypnosis. 1964;12:34–36. doi: 10.1080/00207146408409256. [DOI] [PubMed] [Google Scholar]
- Orne MT. The nature of hypnosis: Artifact and essence. Journal of Abnormal and Social Psychology. 1959;58:277–299. doi: 10.1037/h0046128. doi: http://dx.doi.org/10.1037/h0046128. [DOI] [PubMed] [Google Scholar]
- Orne MT. On the social psychology of the psychological experiment: With particular reference to demand characteristics and their implications. American Psychologist. 1962;17:776–783. doi: http://dx.doi.org/10.1037/h0043424. [Google Scholar]
- Orne MT. Demand characteristics and the concept of quasi-controls. In: Rosenthal R, Rosnow R, editors. Artifact in Behavioral Research. Academic Press; 1969. pp. 143–179. [Google Scholar]
- Orne MT. On the simulating subject as a quasi-control group in hypnosis research: What, why, and how. In: Fromm E, Shor RE, editors. Hypnosis: Developments in research and new perspectives. New York, NY: Aldine; 1979. pp. 519–565. [Google Scholar]
- Pastore RE, Scheirer CJ. Signal detection theory: Considerations for general application. Psychological Bulletin. 1974;81:945–958. doi: http://dx.doi.org/10.1037/h0037357. [Google Scholar]
- Pollack I, Norman DA, Galanter E. An efficient non-parametric analysis of recognition memory. Psychonomic Science. 1964;1:327–328. [Google Scholar]
- Raz A, Marinoff GP, Zephrani ZR, Schweizer HR, Posner MI. See Clearly: Suggestion, Hypnosis, Attention, and Visual Acuity. International Journal of Clinical and Experimental Hypnosis. 2004;52:159–187. doi: 10.1076/iceh.52.2.159.28097. doi: http://dx.doi.org/10.1076/iceh.52.2.159.28097. [DOI] [PubMed] [Google Scholar]
- Schacter DL. Implicit memory: History and current status. Journal of Experimental Psychology: Learning, Memory, and Cognition. 1987;13:501–518. doi: 10.1037//0278-7393.11.3.501. doi: http://dx.doi.org/10.1037/0278-7393.13.3.501. [DOI] [PubMed] [Google Scholar]
- Schulman AI, Greenberg GZ. Operating characteristics and a priori probability of the signal. Perception & Psychophysics. 1970;8:317–320. doi: http://dx.doi.org/10.3758/BF03212600. [Google Scholar]
- Sheehan EP, Smith HV, Forrest DW. A signal-detection study of the effects of suggested improvement on the monocular visual acuity of myopes. International Journal of Clinical and Experimental Hypnosis. 1982;30:138–146. doi: 10.1080/00207148208407379. doi: http://dx.doi.org/10.1080/00207148208407379. [DOI] [PubMed] [Google Scholar]
- Sheehan PW, Perry C. Methodologies of hypnosis: A critical appraisal of contemporary paradigms of hypnosis. Hillsdale, N.J.: Erlbaum; 1976. [Google Scholar]
- Shor RE, Orne EC. Harvard Group Scale of Hypnotic Susceptibility, Form A. Palo Alto, CA: Consulting Psychologists Press; 1962. [Google Scholar]
- Snodgrass JG, Corwin J. Pragmatics of measuring recognition memory: Applications to dementia and amnesia. Journal of Experimental Psychology: General. 1988;117:34–50. doi: 10.1037//0096-3445.117.1.34. doi: http://dx.doi.org/10.1037/0096-3445.117.1.34. [DOI] [PubMed] [Google Scholar]
- Spanos NP, Dubreuil DL, Saad CL, Gorassini D. Hypnotic elimination of prism-induced aftereffects: Perceptual effect or responses to experimental demands. Journal of Abnormal Psychology. 1983;92:216–222. doi: 10.1037//0021-843x.92.2.216. doi: http://dx.doi.org/10.1037/0021-843X.92.2.216. [DOI] [PubMed] [Google Scholar]
- Swets JA, Tanner WP, Birdsall TG. Decision processes in perception. Psychological Review. 1961;68:301–340. doi: http://dx.doi.org/10.1037/h0040547. [PubMed] [Google Scholar]
- Tart CT. Measuring depth of an altered state of consciousness with particular reference to self-report scales of hypnotic depth. In: Fromm E, Shor RE, editors. Hypnosis: Research developments and perspectives. Chicago: Aldine-Atherton; 1972. [Google Scholar]
- Tataryn DJ. Psychophysical and signal detection analyses of hypnotic anesthesia (Order No 9229841) 1992 doi: 10.1080/00207144.2017.1276358. Available from ProQuest Dissertations & Theses A&I; ProQuest Dissertations & Theses Global. (304002023). Retrieved from http://search.proquest.com/docview/304002023?accountid=14496. [DOI] [PMC free article] [PubMed]
- Treisman M. On the stability of ds. Psychological Bulletin. 1977;84:235–243. doi: http://dx.doi.org/10.1037/0033-2909.84.2.235. [Google Scholar]
- Treisman M, Faulkner A. The effect of signal probability on the slope of the receiver operating characteristic given by the rating procedure. British Journal of Mathematical & Statistical Psychology. 1984;37:199–215. doi: http://dx.doi.org/10.1111/j.2044-8317.1984.tb00800.x. [Google Scholar]
- Verfaellie M, Cermak LS. Perceptual fluency as a cue for recognition judgments in amnesia. Neuropsychology. 1999;13(2):198–205. doi: 10.1037//0894-4105.13.2.198. doi: http://dx.doi.org/10.1037/0894-4105.13.2.198. [DOI] [PubMed] [Google Scholar]
- Verfaellie M, Giovanello KS, Keane MM. Recognition memory in amnesia: Effects of relaxing rsponse criteria. Cognitive, Affective, & Behavioral Neuroscience. 2001;1(1):3–9. doi: 10.3758/cabn.1.1.3. doi: http://dx.doi.org/10.3758/CABN.1.1.3. [DOI] [PubMed] [Google Scholar]
- Wallace B, Garrett JB. Reduced felt arm sensation effects on visual adaptation. Perception and Psychophysics. 1973;14:597–600. [Google Scholar]
- Watson CS, Clopton DM. Motivated changes of auditory sensitivity in a simple detection task. Perception & Psychophysics. 1969;5:281–287. doi: http://dx.doi.org/10.3758/BF03209563. [Google Scholar]
- Weiskrantz L. Blindsight: A case study and implications. Oxford, UK: Oxford University Press; 1986. [Google Scholar]
- Weitzenhoffer AM, Hilgard ER. Stanford Hypnotic Susceptibility Scale, Form C. Palo Alto, CA: Consulting Psychologists Press; 1962. [Google Scholar]
- Wilton HJ, Barnier AJ, McConkey KM. Hypnotic anaesthesia and the circle-touch test: Investigating the components of the instructions. Contemporary Hypnosis. 1997;14(1):9–15. doi: http://dx.doi.org/10.1002/ch.79. [Google Scholar]
- Yonelinas AP, Jacoby LL. The process-dissociation approach two decades later: Convergence, boundary conditions, and new directions. Memory & Cognition. 2012;40:663–680. doi: 10.3758/s13421-012-0205-5. doi: http://dx.doi.org/10.3758/s13421-012-0205-5. [DOI] [PubMed] [Google Scholar]
- Young PC. An experimental study of mental and physical functions in the normal and hypnotic states. American Journal of Psychology. 1925;36:214–232. doi: http://dx.doi.org/10.2307/1413859. [Google Scholar]
- Young PC. An experimental study of mental and physical functions in the normal and hypnotic states: additional results. American Journal of Psychology. 1926;37:345–356. doi: http://dx.doi.org/10.2307/1413621. [Google Scholar]