

Abstract
Signet ring adenocarcinoma of the breast with synchronous metastasis to the gastrointestinal (GI) tract is a rare occurrence, typically presenting with abdominal pain, dyspepsia, or GI bleed. We report a case of metastatic breast cancer presenting with a complaint of anemia. A further diagnostic evaluation revealed generalized lymphadenopathy, nodular thickening of the urinary bladder wall, bone lesions, and enlarged pancreas. Biopsies from the lymph nodes, pancreatic biopsy, and bladder nodule all revealed a signet cell carcinoma. An upper and lower GI endoscopy revealed multiple ulcerated gastric mucosal nodules and polypoid folds in the cecum and proximal ascending colon; the biopsies from these lesions were also positive for signet ring cell adenocarcinoma.
Keywords: breast cancer, metastasis, case reports, gastrointestinal bleed, anemia
Introduction
Breast cancer is the most documented malignancy in women and an important factor leading towards the morbidity and mortality in women aged 20-59 years [1]. It accounts for more than 25% of all newly diagnosed cancers in females and is responsible for 15% of the cancer-related deaths in women [1]. The metastatic disease usually develops in 75% of breast cancer patients with or without treatment of the primary malignancy. This metastatic behavior of breast cancer, once it penetrates through the gastrointestinal (GI) tract, usually involves the upper GI tract such as the stomach, small bowel, and pancreaticobiliary regions. This is a very rare form of metastasis [2]. Signet ring adenocarcinoma of the breast with synchronous metastasis to the GI tract is a rare finding presenting with abdominal pain, dyspepsia, or GI bleed. We report an occult breast cancer presenting with severe anemia and synchronous metastasis to the GI tract.
Case presentation
A 56-year-old woman, with a history of hypertension and hypothyroidism, presented with progressive weakness and was found to be severely anemic with a hemoglobin of 5.2 gm/dl, low mean corpuscular volume (MCV), and low iron saturation. A subsequent workup revealed generalized lymphadenopathy, bone lesions, enlarged pancreas, and nodular thickening of the urinary bladder wall. Biopsies from the lymph nodes, pancreatic biopsy, and bladder nodule all revealed a signet cell carcinoma. An upper and lower GI endoscopy revealed multiple ulcerated gastric mucosal nodules and polypoid folds in the cecum and proximal ascending colon; the biopsies from these lesions were also positive for signet ring cell adenocarcinoma (Figures 1-2). Deoxyribonucleic acid (DNA) microarray testing of the lymph node biopsy showed that the primary tissue of origin was consistent with the breast. The patient was started on chemotherapy, yet her condition deteriorated, and she died. An autopsy revealed a right breast cancer with extensive widespread metastases including the stomach, small intestine, and colon.
Figure 1. Esophagogastroduodenoscopy (EGD).
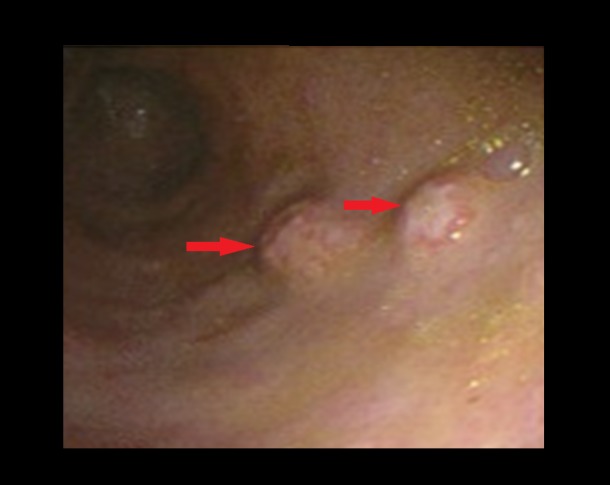
EGD showing ulcerated nodular lesions (red arrows).
Figure 2. Colonoscopy.

Colonoscopy showing ulcerated polypoid nodules (red arrows).
Discussion
Breast cancer is the most common cancer among women, but it is only second to melanoma as the most frequent primary with metastases to the GI tract. Such metastases occur only in 4%-18% of patients, especially in lobular carcinoma [1]. The most commonly involved part is the stomach. When breast carcinoma metastasizes to the stomach, it is important to differentiate it from a primary gastric carcinoma as the treatment plan for these two malignancies are different. This can be done on the basis of clinical, endoscopic, radiological, and histopathological features [2].
Patients with GI metastasis can present with abdominal pain, nausea, vomiting, dysphagia, early satiety, weight loss, tenesmus, or gross bleed. Presentation with severe symptomatic iron deficiency anemia is very unusual and to our knowledge, has rarely been reported. The signet ring cell feature is characteristic of not only gastric but also of other GI adenocarcinoma, and this feature can add to the diagnostic dilemma in such cases [3]. The availability of DNA microarray has facilitated a distinction. The degree of anemia signals advanced disease and a long history of GI involvement.
Invasive ductal carcinoma (IDC) typically metastasizes to the lung, liver, or bone whereas Invasive lobular carcinoma (ILC) more commonly metastasizes to the GI tract and sometimes to the peritoneum and retroperitoneum [3]. This behavior has been explained by various studies, most of which state that this is due to the small size and shape of ILC cells, with E-cadherin overexpression favoring dis-cohesiveness between the cells to migrate to areas of microanatomy that are more conducive to stopping these cells [4]. The difference in metastatic behavior of ILC can be explained by the survival and growth factors provided by the ovaries and peritoneum [5]. Gastric metastasis alone, colon metastasis alone, and metastases in both locations from the breast cancer have been described, but, to our knowledge, there haven’t been too many cases with simultaneous spread to the stomach and colon presenting with severe anemia as the first manifestation of the disease [6-8].
One such case was reported by Villa Guzman, et al. where the patient presented with severe dyspeptic symptoms like nausea and epigastric pain. She underwent an esophagogastroscopy that showed signs of malignancy; biopsies were taken from the suspicious gastric and colonic areas which revealed metastases from lobular carcinoma of the breast [9].
Although IDC and ILC are the more common types of breast carcinoma, there has been a case of phyllodes tumor that was reported recently. The presentation was quite similar to our case. This was a 44-year-old patient who presented with similar symptoms of anemia (hemoglobin levels of 6.7 g/dL) and subsequently, an esophagogastroduodenoscopic (EGD) evaluation was performed, which identified a large gastric mass (approximately 7 cm in diameter) with active bleeding and other related masses. In addition to that, the same study points out the importance of considering GI metastasis as the cause when any patient with breast carcinoma presents with severe anemia, followed by proper workup in order to rule out any bleeding foci. This is also important when considering chemotherapy or targeted therapy as some of these can increase the risk of bleeding [10].
Conclusions
Signet ring adenocarcinoma of the breast with metastasis to the GI tract is a rare entity. Occult breast cancer with synchronous metastases to the stomach and intestine and severe microcytic anemia is an unusual presentation and can delay the diagnosis. Therefore, an in-time diagnosis could have led to an early treatment that would have increased the rate of survival.
The content published in Cureus is the result of clinical experience and/or research by independent individuals or organizations. Cureus is not responsible for the scientific accuracy or reliability of data or conclusions published herein. All content published within Cureus is intended only for educational, research and reference purposes. Additionally, articles published within Cureus should not be deemed a suitable substitute for the advice of a qualified health care professional. Do not disregard or avoid professional medical advice due to content published within Cureus.
The authors have declared that no competing interests exist.
Human Ethics
Consent was obtained by all participants in this study
References
- 1.Gastric metastases originating from occult breast lobular carcinoma: diagnostic and therapeutic problems. Ciulla A, Castronovo G, Tomasello G, Maiorana AM, Russo L, Daniele E, Genova G. World J Surg Oncol. 2008;6:78. doi: 10.1186/1477-7819-6-78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Breast cancer metastasis to the stomach may mimic primary gastric cancer: report of two cases and review of literature. Jones GE, Strauss DC, Forshaw MJ, Deere H, Mahedeva U, Mason RC. World J Surg Oncol. 2007;5:75. doi: 10.1186/1477-7819-5-75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Shakoor MT, Ayub S, Mohindra R, Ayub Z, Ahad A. Int J Biomed Sci. Vol. 10. Dec: 2014. Unique presentations of invasive lobular breast cancer: a case series; pp. 287–293. [PMC free article] [PubMed] [Google Scholar]
- 4.Cytokeratin 8 immunostaining pattern and e-cadherin expression distinguish lobular from ductal breast carcinoma. Lehr HA, Folpe A, Yaziji H, Kommoss F, Gown AM. Am J Clin Pathol. 2015;114:190–196. doi: 10.1309/CPUX-KWEH-7B26-YE19. [DOI] [PubMed] [Google Scholar]
- 5.Infiltrating lobular carcinoma of the breast: tumor characteristics and clinical outcome. Arpino G, Bardou VJ, Clark GM, Elledge RM. Breast Cancer Res. 2004;6:149–156. doi: 10.1186/bcr767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gastric metastases originating from breast cancer: report of 8 cases and review of the literature. Pectasides D, Psyrri A, Pliarchopoulou K, et al. https://www.ncbi.nlm.nih.gov/pubmed/20032432. Anticancer Res. 2009;29:4759–4763. [PubMed] [Google Scholar]
- 7.Single colon metastasis from breast cancer: a clinical case report. Signorelli C, Pomponi-Formiconi D, Nelli F, Pollera CF. https://www.ncbi.nlm.nih.gov/pubmed/16459641. Tumori. 2005;91:424–427. doi: 10.1177/030089160509100509. [DOI] [PubMed] [Google Scholar]
- 8.A rare case of breast cancer metastasis presenting as linitis plastica of the stomach and colon. Malhotra A, Guturu P, Basim MS, Raju GS. Gastrointest Endosc. 2009;70:552–553. doi: 10.1016/j.gie.2009.04.029. [DOI] [PubMed] [Google Scholar]
- 9.Gastric and colon metastasis from breast cancer: case report, review of the literature, and possible underlying mechanisms. Villa Guzmán JC, Espinosa J, Cervera R, Delgado M, Patón R, Cordero García JM. Breast Cancer (Dove Med Press) 2016;9:1–7. doi: 10.2147/BCTT.S79506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.A rare rase of phyllodes tumor metastasis to the stomach presenting as anemia. [Sep;2017 ];Choi DII, Chi HS, Lee SH, et al. Cancer Res Treat. 2016 9:188. doi: 10.4143/crt.2016.188. [DOI] [PMC free article] [PubMed] [Google Scholar]