

Abstract
Pulmonary benign metastasizing leiomyoma (PBML) is a rare disease entity that usually occurs in females of reproductive age with a previous history of uterine myoma. It is typically characterized by multiple pulmonary tumors consisting of benign leiomyoma cells. In the present study, two cases of PBML are discussed. The patient in each case underwent 2-deoxy-2-(fluorine-18)-fluoro-D-glucose positron emission tomography/computed tomography (18-FDG-PET/CT) scans. One patient demonstrated a lack of 18-FDG uptake and a quiescent clinical course. However, the second patient exhibited a markedly high uptake of 18-FDG and aggressive cell proliferation. The two tumors revealed significant differences in metabolic behavior and in clinical course; however, they were similar with regard to cellular appearance. A review of previous studies concerning the findings of 18-FDG-PET/CT in published cases of PBML was also conducted and is presented here.
Keywords: benign metastasizing leiomyoma, 2-deoxy-2-(fluorine-18)-fluoro-D-glucose positron emission tomography/computed tomography
Introduction
Pulmonary benign metastasizing leiomyoma (PBML) is a rare disease entity that usually occurs in females of reproductive age with a prior history of uterine myoma. PBML was first described by Steiner in 1939 (1). PBML is typically characterized by multiple pulmonary tumors containing benign leiomyoma cells (2). Patients are usually asymptomatic and the tumors grow gradually (3). In the present study, two cases of PBML are presented, each of which include the results of 2-deoxy-2-(fluorine-18)-fluoro-D-glucose positron emission tomography/computed tomography (18-FDG-PET/CT) scans. The first patient demonstrated an absence of 18-FDG uptake and a quiescent clinical course. However, the second patient exhibited a markedly high uptake of 18-FDG and the aggressive proliferation of tumor cells was detected. The two tumors revealed significant differences in metabolic behavior and clinical course, yet were alike in regard to cellular appearance. A literature review on the findings of 18-FDG-PET/CT scans in previous published cases of PBML was also conducted and is discussed here.
Case
Case 1
A 38-year-old female was diagnosed with papillary adenocarcinoma of the thyroid gland following a fine-needle aspiration biopsy in Kansai Medical University Takii Hospital in July 2009. However, a CT scan of the chest revealed the presence of multiple nodules of varying sizes in each of the lungs (Fig. 1A). Consequently, an 18-FDG-PET/CT scan was performed. A lesion with high 18-FDG uptake [maximum standard uptake value (SUVmax), >4.9] was observed in the left lobe of the thyroid gland (Fig. 1B and C). However, the results revealed that none of the pulmonary nodules demonstrated 18-FDG uptake (SUVmax, <1.6; Fig. 1C and D). To elucidate whether the pulmonary nodules were metastatic, a CT-guided needle biopsy of the lungs was performed.
Figure 1.

Radiological findings for case 1. (A) CT scan of the pulmonary nodule. (B) A lesion exhibiting high 18-FDG uptake (SUVmax, >4.9) was detected in the tumor of the left lobe of the thyroid gland (arrow). (C) The fusion image of 18-FDG-PET/CT in the coronal plane. Only one lesion in the thyroid gland exhibited a positive accumulation of 18-FDG (arrow). (D) The fusion image of 18-FDG-PET/CT in the horizontal plane. The pulmonary nodule demonstrated no significant 18-FDG uptake (SUVmax, <1.6). CT, computed tomography; 18-FDG-PET/CT, 2-deoxy-2-(fluorine-18)-fluoro-D-glucose positron emission tomography/CT; SUVmax, maximum standard uptake value.
Histological examination was performed as part of routine clinical practice. Briefly, the 7-µm thick sections obtained from formalin-fixed and paraffin-embedded tissues were used for further examination. Resected tissue was fixed in 10% formalin neutral buffer solution (Muto Pure Chemicals Co., Ltd., Tokyo, Japan) at room temperature overnight. Hematoxylin and eosin (H&E) staining was used according to standard clinical histological examination. Light microscopy (BM43/DP27, original magnification, ×400; Olympus Corporation, Tokyo, Japan) was used for observation. H&E staining was performed with Tissue-Tek DRS Slide Stainer (Sakura Fine Tek Europe B.V., Flemingweg, Netherlands) according to manufacturer's protocol. Immunohistochemical staining for αSMA and Ki-67 was performed with Histofine Histostainer 36A (Nichirei Biosciences Inc., Tokyo, Japan) using primary antibodies against αSMA and Ki-67 according to manufacturer's protocol.
The 4 µm thick sections obtained from formalin-fixed and paraffin-embedded tissues were deparaffinized in xylene and rehydrated in a graded series of alcohol to water. Antigen retrieval was performed using 10 mM citrate buffer (pH 6.0) at 121°C for 15 min. Sections were washed in TBS. Antigen retrieval was not performed when examining the expression of αSMA. Sections were blocked with 3% H2O2 at room temperature for 10 min and then incubated for 1 h at room temperature with the antibodies against αSMA (catalog no. 712021; clone no. 1A4; pre-diluted working solution for Histostainer) or Ki-67 (catalog no. 718017; clone no. SP6; pre-diluted working solution for Histostainer) (both from Nichirei Biosciences Inc., Tokyo, Japan).
The sections were subsequently incubated with the Histofine Simple Stain MAX PO (Nichirei Biosciences Inc.) for 30 min at room temperature according to the manufacturer's protocol. Staining was visualized by adding 3,3′diaminobenzidine (K5007; Dako; Agilent Technologies, Inc., Santa Clara, CA, USA) for 10 min at room temperature. Sections were counterstained with haematoxylin for 1 min and then dehydrated with a series of alcohols and xylene.
The lung biopsy tissue specimen revealed a disordered arrangement of spindle-shaped tumor cells (Fig. 2A), and immunohistochemical examination indicated that the cells stained positive for α-smooth muscle actin (α-SMA). The Ki-67 ratio was <1% (Fig. 2B and C). These findings were consistent with the phenotypic characteristics of benign leiomyoma (1). At the age of 37, the patient had experienced extensive genital bleeding due to a uterine myoma, and an emergency total hysterectomy with a right oophorectomy was performed. Histological examination of the preexisting uterine myoma tissue specimens, which were obtained during a previous surgical resection (Japan Community Health Care Organization Hoshigaoka Medical Center, Osaka, Japan), was performed as aforementioned. The results of the histological examination revealed the presence of intravascular leiomyomatosis, which is associated with the pathogenesis of PBML (4). Thus, a definitive diagnosis of PBML was established.
Figure 2.

Histological findings of the biopsy tissue specimen. (A-C) The histological findings of the biopsy specimen from case 1. (D-F) The histological findings of the biopsy specimen from case 2. (A and D) Results of H&E staining. The tissue samples exhibited a similar appearance consisting of interlaced bundles of spindle shaped tumor cells. (B and E) Immunohistochemical staining for α-SMA. The tumor cells each stained positive for α-SMA. (C and F) Immunohistochemical staining for Ki-67 antigen. Staining for Ki-67 revealed positive expression in <1% of the two tumors. Original magnification, ×400. H&E, hematoxylin and eosin. α-SMA α-smooth muscle actin.
As the pulmonary lesions were not attributable to metastases of thyroid cancer, the patient underwent a subtotal thyroidectomy with a curative intention. The tumor-node-metastasis classification pathological stage of the tumor was identified to be pT1aN1aM0 (5). With regard to PBML, observation without the use of aggressive therapy is recommended when the tumor is clinically quiescent (3).
Case 2
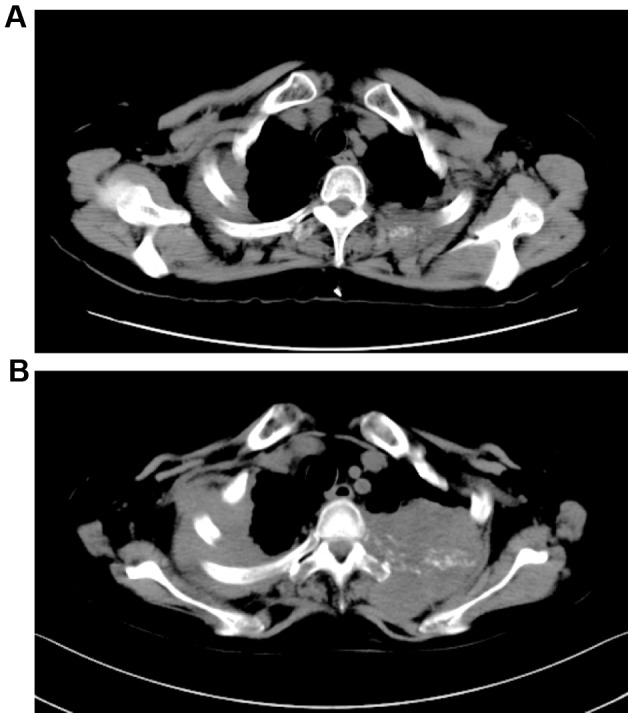
A 62-year-old post-menopausal female was referred to Kansai Medical University Takii Hospital for an investigation due to the presence of numerous pulmonary nodules detected in a routine chest radiography in August 2013. The patient had experienced bilateral upper back pain for two weeks prior to the first appointment at this hospital. The patient had no history of uterine myoma. A chest CT revealed the presence of a tumor in the right upper lung that was 60 mm in diameter and numerous nodular lesions of varying sizes in each of the lungs, in addition to a soft tissue mass that was 70 mm in diameter in the left second rib (Fig. 3A). The parameters assessed included complete blood count and standard clinical laboratory examinations, and the expression levels of specific tumor markers were within normal limits, including carcinoembryonic antigen, serum cytokeratin-19 fragments and Pro-gastrin-releasing pepetide. Contrast-enhanced magnetic resonance imaging of the head revealed a tumor in the left parietal lobe that was 20 mm in diameter, with an edema. As the patient was suspected to have a lung cancer with pulmonary, bone and brain metastases, an 18-FDG-PET/CT scan was performed. The results indicated abnormally high 18-FDG uptake in the right upper lung tumor, the left third rib tumor, atlas vertebra, fourth thoracic vertebra, bilateral ilia and multiple bilateral pulmonary nodules in the lungs (Fig. 3B-D; SUVmax, 20.1). Subsequently, a CT-guided needle biopsy of the right upper lung tumor was performed. Histological examination of the lung biopsy tissue specimen revealed a disordered arrangement of spindle-shaped tumor cells with mild atypia (Fig. 2D). Immunohistochemical examination revealed that the cells stained positive for α-SMA (Fig. 2E). By contrast, CD34, S-100, estrogen receptor (ER) and progesterone receptor (PgR) expression was not detected in these cells. The Ki-67 ratio was <1% (Fig. 2F). These findings are consistent with the phenotypic characteristics of benign leiomyoma. In order to confirm the pathological diagnosis, an additional CT-guided needle biopsy of the tumor of the left rib was performed. The results of the second biopsy tissue specimen from the tumor of the left rib corroborated the findings from the first biopsy specimen obtained from the tumor in the right lung. Consequently, a definitive diagnosis of PBML was established. The patient received whole brain irradiation followed by palliative irradiation for the pulmonary nodules in the right upper lung and left second rib. However, no treatment response was observed and the tumors were identified to be growing (Fig. 4). After three months, the patient was re-admitted to hospital due to a consciousness disorder. Corticosteroids and glycerin were administered, and the neurological symptoms were temporarily improved. However, the patient succumbed to septicemia with Clostridium perfringens.
Figure 3.

Radiological findings for case 2. (A) The image of CT for pulmonary nodule. (B) The fusion image of 18-FDG-PET/CT in horizontal plane. The left pulmonary nodule exhibited a notably high 18-FDG uptake (SUVmax, >20.1). The right pleural thickening also demonstrated marked 18-FDG uptake (SUVmax, >10.1). (C) A lesion exhibiting high 18-FDG uptake (SUVmax, >12.1) was detected in the right side of the atlas vertebra. (D) The fusion image of 18-FDG-PET/CT in the coronal plane. Numerous lesions had a positive accumulation of 18-FDG (arrows). CT, computed tomography; 18-FDG-PET/CT, 2-deoxy-2-(fluorine-18)-fluoro-D-glucose positron emission tomography/CT; SUVmax, maximum standard uptake value.
Figure 4.
Time-dependent change in the radiological findings for Case 2. (A) The CT scan image of pleural thickening at the initial appointment. (B) The CT scan of pleural thickening at the time of readmission. CT, computed tomography.
Discussion
To date, the metabolic behavior of PBML in 18-FDG-PET/CT has attracted a high degree of interest. A number of previous reports have demonstrated that there is a lack of 18-FDG uptake in PBML. However, to the best of our knowledge, there has not yet been a systematic review with respect to the 18-FDG-PET/CT findings for PBML. Therefore, a literature review of prior case reports concerning patients with PBML and 18-FDG-PET/CT findings was conducted. In total, 34 cases were identified in 29 reports (3,6–33). In addition to these 34 cases, the present two cases were added and a total of 36 cases of PBML were reviewed. The results are summarized in Table I. The median age of the patients included was 47 years (range, 34–69 years). A total of 5 patients were pre-menopausal, 2 were post-menopausal and 19 patients had previously received a hysterectomy. The conditions of the reproductive systems of the remaining 10 patients were unconfirmed. All of the total 36 cases were of benign leiomyoma. However, only one patient exhibited malignant transformation (16). With regard to the 18-FDG-PET/CT findings, the accumulation of 18-FDG varied significantly. According to the discretion of the researchers, the patients were assigned into the following three groups: No (minimal) uptake, low (moderate) uptake and high (positive) uptake. A total of 25 patients (69.4%) were assigned to the no uptake group, 8 patients (22.2%) were assigned to the low uptake group and 3 patients (8.3%) were assigned to the high uptake group. However, only one patient out of those 3 had a tumor that demonstrated aggressive behavior. The SUVmax values were identified in 13/36 cases and the median value was determined to be 2.2 (range, 1.4–20.1). The Ki-67 proliferation index ranged from 0–5% in those 13 cases and a total of 7/13 cases had a Ki-67 index <1%. Consequently, there was no significant correlation observed between the uptake of 18-FDG in the tumors and the Ki-67 index. The expression of ER and PgR within the tumors was also assessed. In total, 21/23 patient tissue samples exhibited positive staining for ER (91.3%) and 20/21 had positive staining for PgR (95.2%). However, the patient in case 2 was determined to be double negative for ER and PgR.
Table I.
Characteristics of patients with PBML with 18-FDG-PET/CT findings.
| Author, year | Age | Status | FDG uptake (SUVmax) | Ki-67 index | ER | PgR | (Refs.) |
|---|---|---|---|---|---|---|---|
| Chan et al, 2005 | (6) | ||||||
| Case 1 | 49 | Pre | No uptake (ca. 1.4) | NE | + | + | |
| Case 2 | 45 | HRT | no uptake (ca. 2.0) | NE | NE | NE | |
| Moon et al, 2009 | 52 | Post | No uptake (NE) | NE | + | + | (7) |
| di Scioscio et al, 2009 | 64 | HRT | no uptake (NE) | <1% | + | + | (8) |
| Lee, 2007 | 51 | NE | No uptake (NE) | NE | NE | NE | (9) |
| Londero et al, 2008 | 52 | HRT | low uptake (NE) | NE | + | + | (10) |
| Kasai et al, 2009 | 53 | HRT | No uptake (NE) | NE | − | + | (11) |
| Lin et al, 2010 | (12) | ||||||
| Case 1 | 38 | NE | low uptake (0.2–2.2) | NE | NE | NE | |
| Case 2 | 37 | HRT | Non avid (0.7–2.9) | NE | NE | NE | |
| Clément-Duchêne et al, 2010 | 55 | HRT | no uptake (NE) | NE | NE | NE | (13) |
| Lin and Bradshaw, 2010 | 44 | Pre | No uptake (NE) | NE | + | + | (14) |
| Caminati et al, 2011 | 69 | NE | no uptake (NE) | NE | + | + | (15) |
| Ogawa et al, 2011 | 65 | NE | Low uptake (ca. 3.8) | NE | NE | NE | (16) |
| Yoon et al, 2011 | 34 | Pre | faint uptake (NE) | NE | NE | NE | (17) |
| Ni et al, 2012 | 46 | NE | Non avid (ca. 3.1) | NE | NE | NE | (18) |
| Nakajo et al, 2012 | 50 | HRT | no uptake (ca. 1.5) | <1% | + | + | (19) |
| Fu et al, 2012 | 46 | HRT | No uptake (NE) | <5% | NE | + | (20) |
| Alraiyes et al, 2013 | 40 | HRT | no uptake (NE) | NE | + | + | (21) |
| Okabe et al, 2013 | 47 | Pre | No uptake (NE) | NE | + | NE | (22) |
| Tsunooka et al, 2013 | (23) | ||||||
| Case 1 | 51 | NE | no uptake (NE) | <1% | + | + | |
| Case 2 | 58 | HRT | No uptake (NE) | <1% | + | + | |
| Mogi et al, 2013 | 35 | NE | no uptake (NE) | NE | + | + | (24) |
| Chen et al, 2013 | (25) | ||||||
| Case 1 | 47 | NE | No uptake (NE) | NE | + | + | |
| Case 2 | 47 | HRT | moderately (NE) | <3% | + | + | |
| Case 3 | 53 | NE | Moderately (NE) | <5% | + | + | |
| Ağaçkiran et al, 2013 | 44 | HRT | increased (1.92–4.60) | <3% | + | + | (26) |
| Loukeri et al, 2014 | 47 | Pre | Low uptake (ca. 2.2) | <3% | + | NE | (27) |
| Jeon et al, 2013 | 57 | HRT | low uptake (NE) | NE | + | + | (28) |
| Okita et al, 2013 | 44 | HRT | No uptake (NE) | NE | NE | NE | (29) |
| Jin et al, 2013 | 43 | HRT | minimal (0.9–1.8) | <1% | + | + | (30) |
| Taftaf et al, 2014 | 52 | HRT | Positive uptake (NE) | NE | + | NE | (31) |
| Ma and Cao, 2015 | 45 | HRT | no uptake (NE) | <1% | + | + | (32) |
| Wei et al, 2015 | 47 | HRT | No uptake (NE) | <5% | NE | NE | (3) |
| Wang et al, 2016 | 48 | NE | low uptake (0.5–2.1) | NE | NE | NE | (33) |
| Present case-1 | 38 | HRT | No uptake (<1.6) | <1% | NE | NE | |
| Present case-2 | 62 | Post | high uptake (20.1) | <1% | − | − |
ER, estrogen receptor; PgR, progesterone receptor; HRT, hysterectomy; Pre, premenopausal; Post, postmenopausal; NE, not evaluated; ca, circa; 18-FDG-PET/CT, 2-deoxy-2-(fluorine-18)-fluoro-D-glucose positron emission tomography/computed tomography; SUVmax, maximum standard uptake value.
It has previously been reported that 18-FDG-PET/CT is useful for distinguishing malignant leiomyosarcoma from benign leiomyoma (34,35). In general, SUV values for leiomyosarcoma were observed to be significantly greater than those for leiomyoma. However, numerous reports for 18-FDG-avid leiomyoma were also identified (36–38). Furthermore, a series of comprehensive analyses for those patients who underwent 18-FDG-PET/CT revealed that small proportion of benign uterine leiomyomas exhibited positive 18-FDG uptake. In the present study, a case of 18-FDG-avid PBML is detailed. Summarizing previous studies indicated that 33 PBML cases involved 18-FDG non-avid tumors, and only 3 were 18-FDG-avid tumors. No particular phenotype was identified to be associated with 18-FDG-avid PBML. Further investigations are required in order to improve present understanding of the biological characteristics of PBML, thus leading to its optimal management.
References
- 1.Steiner PE. Metastasizing fibroleiomyoma of the uterus: Report of a case and review of the literature. Am J Pathol. 1939;15:89–110. 7. [PMC free article] [PubMed] [Google Scholar]
- 2.Ki EY, Hwang SJ, Lee KH, Park JS, Hur SY. Benign metastasizing leiomyoma of the lung. World J Surg Oncol. 2013;11:279. doi: 10.1186/1477-7819-11-279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wei WT, Chen PC. Benign metastasizing leiomyoma of the lung: A case report and literature review. Oncol Lett. 2015;10:307–312. doi: 10.3892/ol.2015.3224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mahmoud MS, Desai K, Nezhat FR. Leiomyomas beyond the uterus; benign metastasizing leiomyomatosis with paraaortic metastasizing endometriosis and intravenous leiomyomatosis: A case series and review of the literature. Arch Gynecol Obstet. 2015;291:223–230. doi: 10.1007/s00404-014-3356-8. [DOI] [PubMed] [Google Scholar]
- 5.Wada N, Nakayama H, Suganuma N, Masudo Y, Rino Y, Masuda M, Imada T. Prognostic value of the sixth edition AJCC/UICC TNM classification for differentiated thyroid carcinoma with extrathyroid extension. J Clin Endocrinol Metab. 2007;92:215–218. doi: 10.1210/jc.2006-1443. [DOI] [PubMed] [Google Scholar]
- 6.Chan JW, Law WL, Cheung SO, Lee MP, Ng CK, Lee S, Ko KM, Ma CC, Liu JY, Chan TM, Mok TY. Benign metastasising leiomyoma: A rare but possible cause of bilateral pulmonary nodules in Chinese patients. Hong Kong Med J. 2005;11:303–306. [PubMed] [Google Scholar]
- 7.Moon H, Park SJ, Lee HB, Kim SR, Choe YH, Chung MJ, Jin GY, Lee YC. Pulmonary benign metastasizing leiomyoma in a postmenopausal woman. Am J Med Sci. 2009;338:72–74. doi: 10.1097/MAJ.0b013e31819c7160. [DOI] [PubMed] [Google Scholar]
- 8.di Scioscio V, Feraco P, Miglio L, Toni F, Malvi D, Pacilli AM, Fasano L, Fabbri M, Zompatori M. Benign metastasizing leiomyoma of the lung: PET findings. J Thorac Imaging. 2009;24:41–44. doi: 10.1097/RTI.0b013e31818a0840. [DOI] [PubMed] [Google Scholar]
- 9.Lee SM. Incidental multiple pulmonary nodules: Benign metastasizing leiomyoma and 18F-FDG PET/CT. Nucl Med Mol Imaging. 2007;41:258–259. [Google Scholar]
- 10.Londero AP, Perego P, Mangioni C, Lellé RJ, Londero F, Marchesoni D. Locally relapsed and metastatic uterine leiomyoma: A case report. J Med Case Rep. 2008;2:308. doi: 10.1186/1752-1947-2-308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kasai Y, Masuya D, Matsuoka H, Yoshimatsu H, Suzuki Y. Value of FDG-PET in a case of benign metastasizing leiomyoma. The J Jpn Assoc Chest Surg. 2009;23:871–874. doi: 10.2995/jacsurg.23.871. [DOI] [Google Scholar]
- 12.Lin X, Fan W, Lang P, Hu Y, Zhang X, Sun X. Benign metastasizing leiomyoma identified using 18F-FDG PET/CT. Int J Gynaecol Obstet. 2010;110:154–156. doi: 10.1016/j.ijgo.2010.03.017. [DOI] [PubMed] [Google Scholar]
- 13.Clément-Duchêne C, Vignaud JM, Régent D, Martinet Y. Benign metastasizing leiomyoma with lung cystic lesions and pneumothoraces: A case report. Resp Med CME. 2010;3:183–185. doi: 10.1016/j.rmedc.2009.07.003. [DOI] [Google Scholar]
- 14.Lin TK, Bradshaw DA. Benign metastasizing leiomyoma in a patient without gynecologic symptoms. Chest. 2010;138:89A. doi: 10.1378/chest.10903. [DOI] [Google Scholar]
- 15.Caminati A, Cavazza A, Mirenda MR, Harari S. A 69-year-old female with multiple, bilateral pulmonary nodules. Eur Respir Rev. 2011;20:56–59. doi: 10.1183/09059180.00005010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ogawa M, Hara M, Ozawa Y, Moriyama S, Yano M, Shimizu S, Shibamoto Y. Benign metastasizing leiomyoma of the lung with malignant transformation mimicking mediastinal tumor. Clin Imaging. 2011;35:401–404. doi: 10.1016/j.clinimag.2010.11.003. [DOI] [PubMed] [Google Scholar]
- 17.Yoon G, Kim TJ, Sung CO, Choi CH, Lee JW, Lee JH, Bae DS, Kim BG. Benign metastasizing leiomyoma with multiple lymph node metastasis: A case report. Cancer Res Treat. 2011;43:131–133. doi: 10.4143/crt.2011.43.2.131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ni Y, Shi G, Wan H, Shen J, Jiang X, Yuan F. Pulmonary benign metastasizing leiomyoma: Case report and review of the literature. Clin Exp Obstet Gynecol. 2012;39:249–251. [PubMed] [Google Scholar]
- 19.Nakajo M, Nakayama H, Sato M, Fukukura Y, Nakajo M, Kajiya Y, Yanagi M, Tabata K, Higashi M. FDG-PET/CT finding of benign metastasizing leiomyoma of the lung. Acta Radiol Short Rep. 2012;1 doi: 10.1258/arsr.2012.120012. pii: arsr.2012.120012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fu Y, Li H, Tian B, Hu B. Pulmonary benign metastasizing leiomyoma: A case report and review of the literature. World J Surg Oncol. 2012;10:268. doi: 10.1186/1477-7819-10-268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Alraiyes AH, Kheir F, Hirsh S, Salerno D, Bernal-Green L, Daroca P. A 40-year-old woman with multiple lung nodules. Chest. 2013;143:1826–1829. doi: 10.1378/chest.12-1795. [DOI] [PubMed] [Google Scholar]
- 22.Okabe R, Shoji T, Huang CL. Benign metastasizing leiomyoma of the lung with spontaneous pneumothorax. Thorac Cardiovasc Surg Rep. 2013;2:26–28. doi: 10.1055/s-0033-1345266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Tsunooka N, Hirayama K, Inazawa K. Benign lung metastasizing leiomyoma: A report of 2 cases. Nihon Rinsho Geka Gakkai Zasshi (Journal of Japan Surgical Association) 2013;74:2428–2433. doi: 10.3919/jjsa.74.2428. [DOI] [Google Scholar]
- 24.Mogi A, Hirato J, Kosaka T, Yamaki E, Kuwano H. Benign metastasizing leiomyoma of the lung: Report of a case. Gen Thorac Cardiovasc Surg. 2013;61:719–722. doi: 10.1007/s11748-012-0174-4. [DOI] [PubMed] [Google Scholar]
- 25.Chen S, Zhang Y, Zhang J, Hu H, Cheng Y, Zhou J, Shen L, Chen H. Pulmonary benign metastasizing leiomyoma from uterine leiomyoma. World J Surg Oncol. 2013;11:163. doi: 10.1186/1477-7819-11-163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ağaçkiran Y, Findik G, Ustün LN, Aydoğdu K, Kaya S. Pulmonary benign metastasizing leiomyoma: An extremely rare case. Turk Patoloji Derg. 2014 Apr 9; doi: 10.5146/tjpath.2013.01217. (Epub ahead of print) [DOI] [PubMed] [Google Scholar]
- 27.Loukeri AA, Pantazopoulos IN, Tringidou R, Giampoudakis P, Valaskatzi A, Loukeri PA, Kampolis CF. Benign metastasizing leiomyoma presenting as cavitating lung nodules. Respir Care. 2014;59:e94–e97. doi: 10.4187/respcare.02775. [DOI] [PubMed] [Google Scholar]
- 28.Jeon HW, Choi SH, Sung SW, Park JK. Pulmonary benign metastasizing leiomyoma: Report of three cases. World J Surg Oncol. 2013;11:281. doi: 10.1186/1477-7819-11-281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Okita R, Yasuda K, Nojima Y, Maeda A, Yukawa T, Saisho S, Shimizu K, Akiyama T, Miyagi Y, Oda T, Nakata M. CT, MRI and 18F-FDG PET-CT findings of pulmonary benign metastasizing leiomyoma: A case report. Open J Thoracic Surg. 2013;3:127–129. doi: 10.4236/ojts.2013.34026. [DOI] [Google Scholar]
- 30.Jin X, Meng Y, Zhu Z, Jing H, Li F. Elevated 99mTc 3PRGD2 activity in benign metastasizing leiomyoma. Clin Nucl Med. 2013;38:117–119. doi: 10.1097/RLU.0b013e318279f14d. [DOI] [PubMed] [Google Scholar]
- 31.Taftaf R, Starnes S, Wang J, Shipley R, Namad T, Khaled R, Abdel Karim N. Benign metastasizing leiomyoma: A rare type of lung metastases-two case reports and review of the literature. Case Rep Oncol Med. 2014;2014:842801. doi: 10.1155/2014/842801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ma H, Cao J. Benign pulmonary metastasizing leiomyoma of the uterus: A case report. Oncol Lett. 2015;9:1347–1350. doi: 10.3892/ol.2015.2878. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Wang HC, Wang YB, Chen XH, Cui LL. Uterine intravenous leiomyomatosis with intracardiac extension and pulmonary benign metastases on FDG PET/CT: A case report. Korean J Radiol. 2016;17:289–294. doi: 10.3348/kjr.2016.17.2.289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Schwarzbach MH, Dimitrakopoulou-Strauss A, Willeke F, Hinz U, Strauss LG, Zhang YM, Mechtersheimer G, Attigah N, Lehnert T, Herfarth C. Clinical value of [18-F] fluorodeoxyglucose positron emission tomography imaging in soft tissue sarcomas. Ann Surg. 2000;231:380–386. doi: 10.1097/00000658-200003000-00011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Nagamatsu A, Umesaki N, Li L, Tanaka T. Use of 18F-fluorodeoxyglucose positron emission tomography for diagnosis of uterine sarcomas. Oncol Rep. 2010;23:1069–1076. doi: 10.3892/or_00000734. [DOI] [PubMed] [Google Scholar]
- 36.Ak I, Ozalp S, Yalcin OT, Zor E, Vardareli E. Uptake of 2-[18F]fluoro-2-deoxy-D-glucose in uterine leiomyoma: Imaging of four patients by coincidence positron emission tomography. Nucl Med Commun. 2004;25:941–945. doi: 10.1097/00006231-200409000-00012. [DOI] [PubMed] [Google Scholar]
- 37.Shida M, Murakami M, Tsukada H, Ishiguro Y, Kikuchi K, Yamashita E, Kajiwara H, Yasuda M, Ide M. F-18 fluorodeoxyglucose uptake in leiomyomatous uterus. Int J Gynecol Cancer. 2007;17:285–290. doi: 10.1111/j.1525-1438.2006.00778.x. [DOI] [PubMed] [Google Scholar]
- 38.Vriens D, de Geus-Oei LF, Flucke UE, van der Kogel AJ, Oyen WJ, Vierhout ME, van der Meer JW. Benign uterine uptake of FDG: A case report and review of literature. Neth J Med. 2010;68:379–380. [PubMed] [Google Scholar]