

Abstract
Dysautonomia, dysfunction of the autonomic nervous system, presents with heterogeneous clinical features from an imbalanced regulation of the sympathetic and parasympathetic nervous systems. Low Vitamin D levels can explain the heterogeneous clinical features of migraine headaches, cardiac and gastrointestinal dysfunction, and oxidative stress evident in dysautonomia patients. The role of Vitamin D in modulating pain sensitivity has been recently established. However, there is a lack of research and understanding regarding the association between Vitamin D deficiency and autonomic dysfunction. Vitamin D is a neuroactive hormone that modulates autonomic balance, regulating the sympathetic and parasympathetic nervous systems, and has multisystem benefits. The following review explores the literature and addresses the relationship between Vitamin D deficiency and autonomic dysfunction. Overall, this literature review implicates Vitamin D deficiency in autonomic dysfunction and elucidates the potential therapeutic role of Vitamin D in autonomic disorders. PubMed search was performed for English articles from 1996 to 2016. Following keywords: Vitamin D, autonomic dysfunction and orthostatic hypotension, Vitamin D receptor, migraine and traumatic brain injury, Vitamin D, cardiac and gastrointestinal disease, Vitamin D, glutathione, oxidative stress, and serotonin were included. Only articles reporting primary data relevant to the above question were included in the study.
KEYWORDS: Autonomic dysfunction and orthostatic hypotension, cardiac and gastrointestinal disease, glutathione and oxidative stress, migraine and traumatic brain injury, serotonin, Vitamin D, Vitamin D receptor
INTRODUCTION
Dysautonomia, dysfunction of the autonomic nervous system, impairs the differentiating neural crest that gives rise to neurons of the sympathetic and the parasympathetic nervous system affecting cardiac, enteric, osteocytes, and connective tissue. It presents with multiple symptoms including headaches, lightheadedness with orthostatic intolerance, palpitations, gastrointestinal dysfunction, generalized muscular pains, and exercise intolerance. Oxidative stress with increased pro-inflammatory markers and low levels of cerebrospinal fluid serotonin and dopamine metabolites- 5HIAA, and HVA are evident in a subset of patients with juvenile neurocardiogenic syncope with dysautonomia based on abnormal tilt table test.[1,2]
Autonomic dysfunction has also been associated with increased pain sensitivity as in reflex sympathetic dystrophy with pain out of proportion to the cause.[3] Often increased pain sensitivity and nonspecific muscular aches can be a sign of Vitamin D deficiency. Headaches in dysautonomia patients may be explained by Vitamin D deficiency. A case series of three premenarchal girls with chronic tension-type headaches and generalized body pain were evaluated with Vitamin D deficiency. Symptoms improved with Vitamin D therapy suggesting a single symptom complex with Vitamin D deficiency as an etiology.[4] This literature review illustrates Vitamin D deficiency in autonomic dysfunction by demonstrating the role of Vitamin D in autonomic regulation, pain modulation and muscle function, gastrointestinal functioning, and as an antioxidative agent and thereby implicates Vitamin D deficiency in autonomic dysfunction. Figure 1 illustrates the role of Vitamin D deficiency in autonomic dysfunction.
Figure 1.
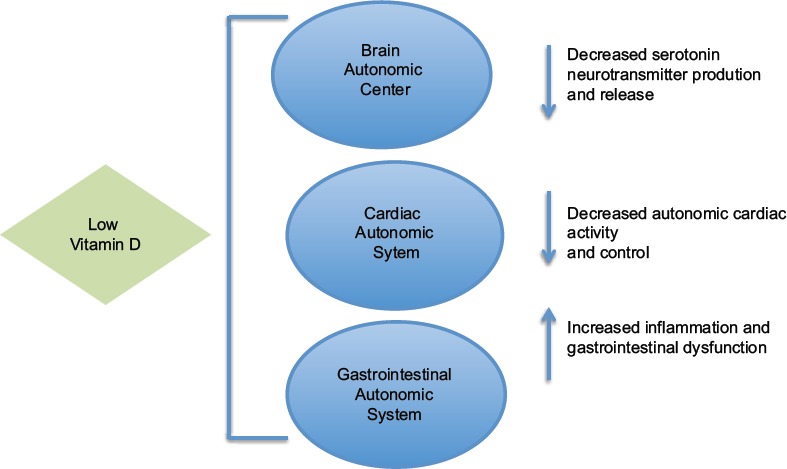
Vitamin D deficiency and autonomic dysfunction - Vitamin D stimulates release of serotonin and acts as an antioxidant, influencing the autonomic activities of the brain, cardiac, and gastrointestinal systems
METHODOLOGY OF REVIEW
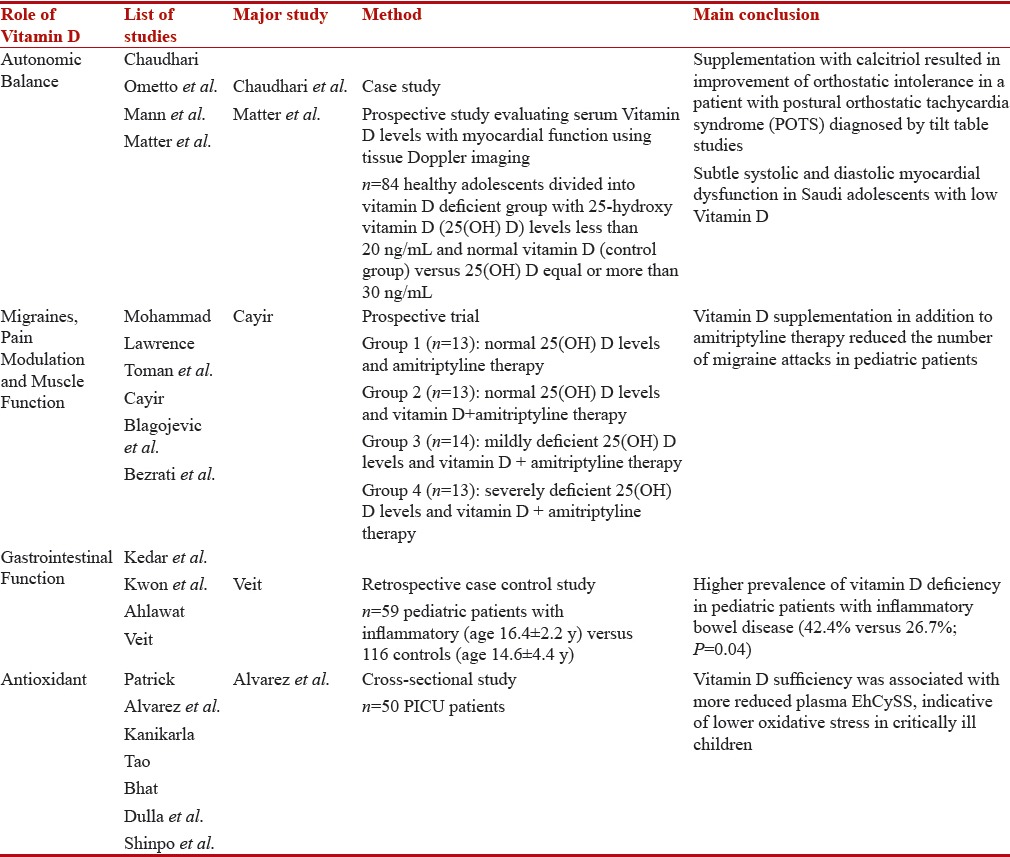
Studies published between 1996 and 2016 were reviewed through PubMed. The search was restricted to English. Following keywords were included: Vitamin D, autonomic dysfunction, orthostatic hypotension, Vitamin D receptor (VDR), migraine, traumatic brain injury (TBI), Vitamin D, cardiac and gastrointestinal disease, serotonin, glutathione, and oxidative stress. Only articles reporting primary data relevant to the association between Vitamin D deficiency and autonomic dysfunction were included in the study. Articles irrelevant to the role of Vitamin D and autonomic dysfunction were excluded with the rationale that these articles would lead to digression from this specific study. Table 1 summarizes the major studies reviewed.
Table 1.
The role of Vitamin D deficiency in autonomic dysfunction
VITAMIN D FOR AUTONOMIC BALANCE
Vitamin D plays a crucial role in autonomic balance and may act as a central neuroactive substance. In a case report of a patient diagnosed with postural orthostatic tachycardia syndrome by tilt table studies, 1,25-dihydroxyvitamin D 125(OH) 2D] 125(OH) D3, calcitriol] – the main biologically active form of Vitamin D was found to be below normal. Supplementation with calcitriol resulted in improvement of orthostatic intolerance and palpitations. This suggests the potential therapeutic role of Vitamin D in autonomic dysfunction.[5]
Low Vitamin D status is associated with an increased risk of orthostatic hypotension. The association of hypovitaminosis D with orthostatic hypotension was confirmed in a meta-analysis of five cross-sectional studies including 3646 participants (1270 with hypovitaminosis D and 2376 without). The participants with hypovitaminosis D had a higher prevalence of orthostatic hypotension (odds ratio = 1.88; 95% confidence interval [CI]: 1.25–2.84; I = 68%) that was not affected by adjusting for a median of five potential confounders. People with orthostatic hypotension had significantly reduced serum Vitamin D concentrations (standardized mean difference = −0.42; 95% CI: −0.72–−0.12).[6]
Low 1,25(OH) D3 levels are associated with unfavorable cardiac autonomic activity with suppression of resting cardiac autonomic activity.[7] A study of 84 healthy adolescents evaluating serum Vitamin D levels with myocardial function using tissue Doppler imaging showed subtle systolic and diastolic myocardial dysfunction in Saudi adolescents with low Vitamin D.[8] These studies suggest the crucial role of Vitamin D in the maintenance of cardiac autonomic balance.
VITAMIN D FOR PAIN MODULATION, MIGRAINES, AND MUSCLE FUNCTION
The association of Vitamin D deficiency with increased pain sensation, migraine headaches, and poor muscle function are evident in several studies. Vitamin D receptors are found in the hypothalamus, a region of migraine pain sensation. There has been an association between migraines without aura and two VDR polymorphisms (Taq1 and FokI) in Iranian patients. Furthermore, headache severity was found to be worse in FokI heterozygote patients than homozygote patients.[9] Vitamin D binding to the VDR may be important in pain modulation. Vitamin D deficiency could lead to increased excitability and sensitization.
Vitamin D supplementation has been shown to reduce the frequency of migraine attacks. In the study by Cayir, Vitamin D supplementation in addition to antimigraine treatment reduced the number of migraine attacks in pediatric patients.[10] Vitamin D is known to have a neuroprotective role in patients with TBI.[11] There is a correlation between serum Vitamin D levels and severity of TBI. In a prospective observational study, Vitamin D was significantly lower in patients with severe TBI compared to patients with mild TBI (n = 95, P = 0.03, CI 95% −23.60–−1.21, mean effect size 12.40 nmol/L).[12]
Vitamin D reduces pain severity and improves mobility and daily functioning. In a prospective pilot study of 35 children (18 males; age 10.48 ± 3.87 years) with different musculoskeletal/orthopedic conditions and Vitamin D deficiency, Vitamin D therapy for 6 months resulted in decreased pain intensity (P ≤ 0.03) as well as decreased functioning problems related to pain (P ≤ 0.01).[13] In a cross-sectional study of 125 healthy children who practiced football as a leisure activity, low plasma 25(OH)D levels were associated with decreased muscle strength and decreased exercise performance.[14] Vitamin D status may be a key factor in muscle function and pain intensity in patients with autonomic dysfunction.
VITAMIN D FOR GASTROINTESTINAL FUNCTION
Vitamin D deficiency is associated with gastrointestinal dysfunction. Vitamin D is important for health of the enteric nervous system and influences gastric emptying. Patients with gastric dysmotility have low serum Vitamin D levels.[15] Low serum 25(OH)D levels are associated with delayed gastric emptying time (GET) assessed by scintigraphy in Parkinson's disease patients that were divided into a delayed-GET group and a normal-GET group.[16]
Vitamin D deficiency is common in pediatric patients with gastrointestinal symptoms. The anti-inflammatory role of Vitamin D plays a protective role in gastrointestinal function. There is evidence to suggest an inverse relationship between Vitamin D status and inflammatory bowel disease (IBD).[17] In a retrospective case–control study of 59 pediatric patients with IBD (age 16.4 ± 2.2 years) versus 116 controls (age 14.6 ± 4.4 years) demonstrated that patients with IBD had a higher prevalence of Vitamin D deficiency (42.4% vs. 26.7%; P = 0.04) with inflammation being the key determinant of Vitamin D status in IBD.[18]
VITAMIN D AS AN ANTIOXIDANT
Interestingly, Vitamin D has been shown to have antioxidant properties along with its role in the production of serotonin, an antioxidant. The active form of Vitamin D, calcitriol activates the synthesis of serotonin-synthesizing gene tryptophan hydroxylase 2 in the brain at a Vitamin D response element.[19] Vitamin D sufficiency is associated with lower oxidative stress in critically ill children suggesting the crucial role of Vitamin D in maintaining redox status and in protecting against oxidative stress.[20]
Vitamin D inhibits oxidative stress and has anti-inflammatory properties.[21] In a study evaluating the association of cord blood levels of 25(OH)D with an inflammatory marker, C-reactive protein (CRP) in 1491 neonates in Heifei China, it was shown that the CRP decreased by 1.42 mg/L (95% CI: 0.90, 1.95) per 10 nmol/L increase in 25(OH)D among neonates with 25(OH)D <25.0 nmol/L, and CRP decreased by 0.49 mg/L (95% CI: 0.17, 0.80) among neonates with 25(OH)D between 25.0 nmol/L and 49.9 nmol/L.[22] The antioxidant potential of Vitamin D was evident in a rat model where treatment with Vitamin D caused a reversal of oxidative stress in the muscle tissue.[23] Vitamin D has been shown to inhibit production of several pro-inflammatory molecules including nitric oxide, interleukin (IL)-1β, and IL-6 from microglia.[24] The biologically active form of Vitamin D, 1,25(OH)2D3, has been reported to enhance intracellular glutathione concentration in the central nervous system.[25] Vitamin D as an antioxidative agent may serve to protect against autonomic dysfunction.
CONCLUSION
Dysautonomia, dysfunction of the autonomic nervous system, affects the expression of genes involved in calcium metabolism before and after differentiation of the neural cells that gives rise to neurons of the sympathetic and the parasympathetic nervous system. Vitamin D is crucial for the effective functioning of the sympathetic and parasympathetic nervous systems. Low Vitamin D levels can explain the symptom complex of migraine headaches, cardiac and gastrointestinal dysfunction, and oxidative stress as evident in dysautonomia patients. This literature review elucidates the potential therapeutic role of Vitamin D for autonomic dysfunction. More research is needed to investigate the role of Vitamin D in autonomic disorders.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Butler IJ, Lankford JE, Hashmi SS, Numan MT. Biogenic amine metabolism in juvenile neurocardiogenic syncope with dysautonomia. Ann Clin Transl Neurol. 2014;1:251–7. doi: 10.1002/acn3.49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wadhwania R, Butler I, Hashmi S, Numan M, Lankford J. Dysautonomia: Retrospective study of amino acids, cytokines and neurotransmitter metabolites. Ann Neurol. 2016;80:S299. [Google Scholar]
- 3.Gordon N. Reflex sympathetic dystrophy. Brain Dev. 1996;18:257–62. doi: 10.1016/0387-7604(96)00037-x. [DOI] [PubMed] [Google Scholar]
- 4.Prakash S, Makwana P, Rathore C. Vitamin D deficiency mimicking chronic tension-type headache in children. BMJ Case Rep 2016. 2016:pii: Bcr2015213833. doi: 10.1136/bcr-2015-213833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chaudhari SA, Sacerdote A, Bahtiyar G. 1-a hydroxylation defect in postural orthostatic tachycardia syndrome: Remission with calcitriol supplementation. BMJ Case Rep 2012. 2012:pii: Bcr0220125730. doi: 10.1136/bcr.02.2012.5730. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ometto F, Stubbs B, Annweiler C, Duval GT, Jang W, Kim HT, et al. Hypovitaminosis D and orthostatic hypotension: A systematic review and meta-analysis. J Hypertens. 2016;34:1036–43. doi: 10.1097/HJH.0000000000000907. [DOI] [PubMed] [Google Scholar]
- 7.Mann MC, Exner DV, Hemmelgarn BR, Sola DY, Turin TC, Ellis L, et al. Vitamin D levels are associated with cardiac autonomic activity in healthy humans. Nutrients. 2013;5:2114–27. doi: 10.3390/nu5062114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Matter M, El-Sherbiny E, Elmougy A, Abass M, Aldossary S, Ali WA. Myocardial function in Saudi adolescents with Vitamin D deficiency: Tissue Doppler imaging study. J Saudi Heart Assoc. 2016;28:22–30. doi: 10.1016/j.jsha.2015.06.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Motaghi M, Haghjooy Javanmard S, Haghdoost F, Tajadini M, Saadatnia M, Rafiee L, et al. Relationship between Vitamin D receptor gene polymorphisms and migraine without aura in an Iranian population. Biomed Res Int. 2013;2013:351942. doi: 10.1155/2013/351942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cayir A, Turan MI, Tan H. Effect of Vitamin D therapy in addition to amitriptyline on migraine attacks in pediatric patients. Braz J Med Biol Res. 2014;47:349–54. doi: 10.1590/1414-431X20143606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lawrence DW, Sharma B. A review of the neuroprotective role of Vitamin D in traumatic brain injury with implications for supplementation post-concussion. Brain Inj. 2016;30:960–8. doi: 10.3109/02699052.2016.1147081. [DOI] [PubMed] [Google Scholar]
- 12.Toman E, Bishop JR, Davies DJ, Su Z, Criseno S, Mason A, et al. Vitamin D deficiency in traumatic brain injury and its relationship with severity of injury and quality of life: A prospective, observational study. J Neurotrauma. 2017;34:1448–56. doi: 10.1089/neu.2016.4494. [DOI] [PubMed] [Google Scholar]
- 13.Blagojevic Z, Nikolic V, Kisic-Tepavcevic D, Terzic Supic Z, Kovacevic R, Zivkovic Z, et al. Musculoskeletal pain and Vitamin D deficiency in children: A pilot follow-up study of Vitamin D therapy in musculoskeletal/orthopedic conditions. Acta Chir Orthop Traumatol Cech. 2016;83:21–6. [PubMed] [Google Scholar]
- 14.Bezrati I, Hammami R, Ben Fradj MK, Martone D, Padulo J, Feki M, et al. Association of plasma 25-hydroxyvitamin D with physical performance in physically active children. Appl Physiol Nutr Metab. 2016;41:1124–8. doi: 10.1139/apnm-2016-0097. [DOI] [PubMed] [Google Scholar]
- 15.Kedar A, Nikitina Y, Henry OR, Abell KB, Vedanarayanan V, Griswold ME, et al. Gastric dysmotility and low serum Vitamin D levels in patients with gastroparesis. Horm Metab Res. 2013;45:47–53. doi: 10.1055/s-0032-1323689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kwon KY, Jo KD, Lee MK, Oh M, Kim EN, Park J, et al. Low serum Vitamin D levels may contribute to gastric dysmotility in de novo Parkinson's disease. Neurodegener Dis. 2016;16:199–205. doi: 10.1159/000441917. [DOI] [PubMed] [Google Scholar]
- 17.Ahlawat R, Weinstein T, Pettei MJ. Vitamin D in pediatric gastrointestinal disease. Curr Opin Pediatr. 2016;29:122–7. doi: 10.1097/MOP.0000000000000451. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 18.Veit LE, Maranda L, Nwosu BU. The nondietary determinants of Vitamin D status in pediatric inflammatory bowel disease. Nutrition. 2015;31:994–9. doi: 10.1016/j.nut.2015.03.010. [DOI] [PubMed] [Google Scholar]
- 19.Patrick RP, Ames BN. Vitamin D hormone regulates serotonin synthesis. Part 1: Relevance for autism. FASEB J. 2014;28:2398–413. doi: 10.1096/fj.13-246546. [DOI] [PubMed] [Google Scholar]
- 20.Alvarez JA, Grunwell JR, Gillespie SE, Tangpricha V, Hebbar KB. Vitamin D deficiency is associated with an oxidized plasma cysteine redox potential in critically Ill children. J Steroid Biochem Mol Biol. 2016:pii: S0960-076030249-7. doi: 10.1016/j.jsbmb.2016.09.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kanikarla-Marie P, Jain SK. 1,25(OH) 2D3 inhibits oxidative stress and monocyte adhesion by mediating the upregulation of GCLC and GSH in endothelial cells treated with acetoacetate (ketosis) J Steroid Biochem Mol Biol. 2016;159:94–101. doi: 10.1016/j.jsbmb.2016.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Tao RX, Zhou QF, Xu ZW, Hao JH, Huang K, Mou Z, et al. Inverse correlation between Vitamin D and C-reactive protein in newborns. Nutrients. 2015;7:9218–28. doi: 10.3390/nu7115468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Bhat M, Ismail A. Vitamin D treatment protects against and reverses oxidative stress induced muscle proteolysis. J Steroid Biochem Mol Biol. 2015;152:171–9. doi: 10.1016/j.jsbmb.2015.05.012. [DOI] [PubMed] [Google Scholar]
- 24.Dulla YA, Kurauchi Y, Hisatsune A, Seki T, Shudo K, Katsuki H, et al. Regulatory mechanisms of Vitamin D3 on production of nitric oxide and pro-inflammatory cytokines in microglial BV-2 cells. Neurochem Res. 2016;41:2848–58. doi: 10.1007/s11064-016-2000-3. [DOI] [PubMed] [Google Scholar]
- 25.Shinpo K, Kikuchi S, Sasaki H, Moriwaka F, Tashiro K. Effect of 1,25-dihydroxyvitamin D(3) on cultured mesencephalic dopaminergic neurons to the combined toxicity caused by L-buthionine sulfoximine and 1-methyl-4-phenylpyridine. J Neurosci Res. 2000;62:374–82. doi: 10.1002/1097-4547(20001101)62:3<374::AID-JNR7>3.0.CO;2-7. [DOI] [PubMed] [Google Scholar]