

Abstract
Background
The Transdisciplinary Research Consortium for Gulf Resilience on Women’s Health (GROWH) addresses reproductive health disparities in the Gulf Coast by linking communities and scientists through community-engaged research. Funded by the National Institutes of Environmental Health Sciences, GROWH’s Community Outreach and Dissemination Core (CODC) seeks to utilize community-based participatory research (CBPR) and other community-centered outreach strategies to strengthen resilience in vulnerable Gulf Coast populations. The CODC is an academic-community partnership comprised of Tulane University, Mary Queen of Vietnam Community Development Corporation, Bayou Interfaith Shared Community Organizing, and the Louisiana Public Health Institute (LPHI).
Methods
Alongside its CODC partners, LPHI collaboratively developed, piloted and evaluated an innovative CBPR curriculum. In addition to helping with curriculum design, the CODC’s community and academic partners participated in the pilot. The curriculum was designed to impart applied, practical knowledge to community-based organizations and academic researchers on the successful formulation, execution and sustaining of CBPR projects and partnerships within the context of environmental health research.
Results
The curriculum resulted in increased knowledge about CBPR methods among both community and academic partners as well as improved relationships within the GROWH CODC partnership.
Conclusion
The efforts of the GROWH partnership and curriculum were successful. This curriculum may serve as an anchor for future GROWH efforts including: competency development, translation of the curriculum into education and training products, community development of a CBPR curriculum for academic partners, community practice of CBPR, and future environmental health work.
Keywords: Community-Based Participatory Research, Research Curriculum, Evaluation, Environmental Health
Introduction
Community-Engaged and Community-Based Participatory Research in the Environmental Health Context
Community-engaged and participatory research methods are increasingly used to ensure that research results support positive changes in community health. These methods work in tandem, facilitating partnerships between community members and academic researchers to collaboratively define research questions, develop and implement research agendas, and translate findings into meaningful changes within communities. Importantly, community-engaged and participatory approaches allow for the development and translation of research questions and results that are informed by community needs as well as the interests and expertise of academic researchers[1, 2].
Community-based participatory research (CBPR) holds significant potential for improving outcomes in public health, environmental health and social sciences research by engaging community members, organizational representatives, and researchers at every stage and aspect of the research process. All CBPR partners contribute their unique expertise to the partnership and share decision-making as well as ownership of the research project. A primary goal of this approach is to generate research findings that address community concerns and interests and seek to improve community health while aiding in the development of mutually beneficial academic-community partnerships that foster long-term collaboration [1,3,4–6].
Whereas other community-based and participatory models of research emphasize the importance of individual and community organization perspectives, CBPR is uniquely premised on the idea that community perspectives should not only inform or advise the research process, but must serve as a guiding voice in the development and execution of a research agenda co-created with academic partners [1,2]. Importantly, CBPR partnerships are not monolithic and vary depending on the context in which they emerge as well as their research agenda. Stakeholders within CBPR partnerships bring together individuals and organizations with different needs, skills, and abilities in order to engage in various aspects of the research process, and challenges may arise by uniting diverse actors within a singular partnership. In order to formalize CBPR methodological approaches and in response to these challenges, Israel et al. (1998) developed a set of commonly accepted principles for CBPR:
Recognizes community as a unit of identity;
Builds on strengths and resources within the community;
Facilitates collaborative, equitable involvement of all partners in all phases of the research;
Integrates knowledge and action for the mutual benefit of all partners;
Promotes a co-learning and empowering process that attends to social inequalities;
Involves a cyclical and iterative process;
Addresses health from both positive and ecological perspectives;
Disseminates findings and knowledge gained to all partners; and
Involves a long-term commitment by all partners.
Effective CBPR methodology requires that all partners develop and maintain a common understanding of the research process as well as community needs and perspectives. In order to strengthen the research capacity of community partners and ensure common understanding of the research process, the Transdisciplinary Research Consortium for Gulf Resilience on Women’s Health (GROWH) partnership collaboratively developed and piloted a CBPR curriculum over twelve months during 2014 and 2015. This manuscript describes the experience of developing and implementing a CBPR curriculum with GROWH’s community and academic partners and presents evaluation findings from this pilot implementation.
Introduction to the Transdisciplinary Research Consortium for Gulf Resilience on Women’s Health
GROWH, initiated in 2011 with funding from the National Institutes of Environmental Health Sciences, is part of a research consortium of community-university partnerships that explore the potential adverse effects of the 2010 Deepwater Horizon oil spill on community health. GROWH is a five-year program led by the Tulane University School of Public Health and Tropical Medicine. Its multi-disciplinary academic research team conducts population and laboratory research on the health effects of the oil spill on vulnerable communities living in the disaster-prone, low-lying coastal Gulf region of Southeast Louisiana. The GROWH consortium was deliberately designed to answer three prevalent community concerns in the after math of the 2010 oil spill: Is the seafood safe to eat? Is the air safe to breathe? What will happen to our babies? GROWH’s study design reflects the need for a transdisciplinary approach that links public health, ecosystems and psychosocial health [7]. Its Community Outreach and Dissemination Core (CODC), tasked with the dissemination and translation of research findings, was comprised of Mary Queen of Vietnam Community Development Corporation (MQVN CDC) and Bayou Interfaith Shared Community Organizing (BISCO). MQVN CDC and BISCO are both well-established community organizations serving large and diverse populations in Southeast Louisiana. LPHI served as convener and facilitator for the CODC (see Figure 1 for additional information on the partners). In addition to participating in the dissemination and translation of research findings, GROWH’s community partners helped with data collection and analysis. For example, community and academic partners from MQVN CDC and Tulane went on joint fishing trips to analyze the environmental contaminants in shrimp caught and consumed daily by Vietnamese-American communities in the region [8]. Similarly, the BISCO team was instrumental in placing and retrieving air assessment devices at area homes selected for both outdoor and indoor air analyses.
Figure 1.
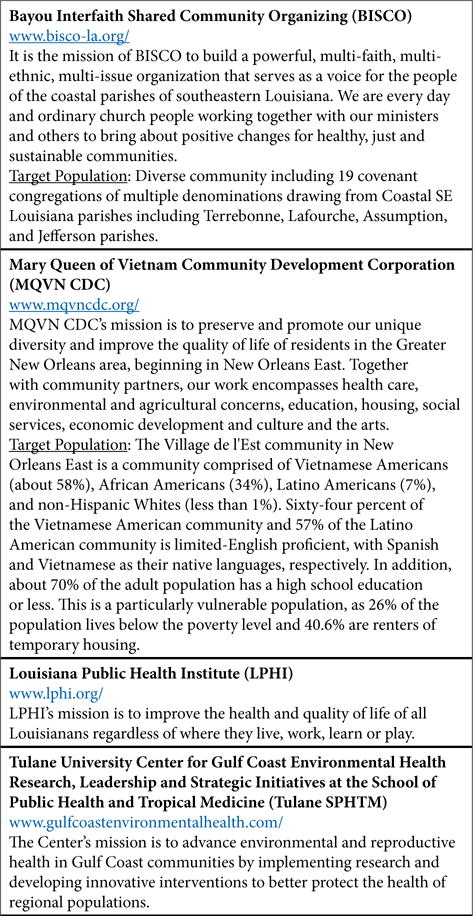
List of GROWH CODC Members.
In the third year of the GROWH program, when preliminary research findings were becoming available, the CODC recognized that despite a track record of successful collaboration, the traditional CBPR principles were not fully realized within their partnership given the project’s post-disaster context and the urgency of proposal submission after the oil spill occurred. CODC members agreed that receiving formal education on the principles and methods of CBPR would help them not only in the dissemination phase of the project but also in strengthening their partnership and improving productivity. In May 2014, the community and academic partners decided to create and participate in a formal training program in CBPR methods.
From May 2014 to April 2015, GROWH’s CODC members collaboratively developed and served as pilot test subjects for a curriculum designed to impart applied, practical knowledge to community-based organizations and academic researchers on how to successfully form, execute, and sustain CBPR partnerships and projects. Development of the curriculum incorporated partners’ past experiences in community-engaged research as well as exemplary CBPR projects from across the United States. The LPHI team led efforts to create the curriculum and served as primary facilitators for the training program. Key goals for the GROWH partnership were to provide in-depth insight into the operationalization of CBPR principles and to develop a formalized partnership framework. Given GROWH’s environmental health focus, the curriculum also addressed translation and dissemination of research findings specific to the discipline of environmental health.
Materials & Methods
The LPHI curriculum development team consisted of four staff members with Master’s degrees in public health and education and PhDs in epidemiology and public and community health, as well as two student interns. LPHI team members led the initial development of the curriculum, beginning with a systematic review of literature, trainings, and curricula on CBPR and community-engaged research. Both peer-reviewed and gray literature published by academic researchers and community organizations were consulted. Drawing from the existing sources, LPHI developed CBPR curricular content adapted to GROWH CODC members’ needs and interests. These adaptations took into account group members’ preference for in-person and interactive training sessions, members’ prior familiarity with CBPR, and the stage of each of the GROWH research projects. The curriculum deployed adult learning strategies and emphasized hands-on skill development through interactive learning. Real-world case studies of environmental health disparities and examples from the Gulf South region were incorporated when possible. LPHI developed PowerPoint presentations, presentation scripts, and activity materials in advance of each training session.
The CBPR curriculum consisted of seven day-long modules led by the LPHI staff members who developed the curriculum. Each module focused on a different aspect of CBPR and featured a combination of pedagogical activities including facilitated discussions and case studies. Training modules were implemented between September 2014 and April 2015. Each module was attended by a minimum of four people, with at least one representative from each of the four CODC partners, resulting in an average of eight participants at each session. Attendees were compensated for their time participating in the training. The training session titles, which reflect each session’s respective topic area, as well as the total number of attendees at each session, are provided in Figure 2.
Figure 2.
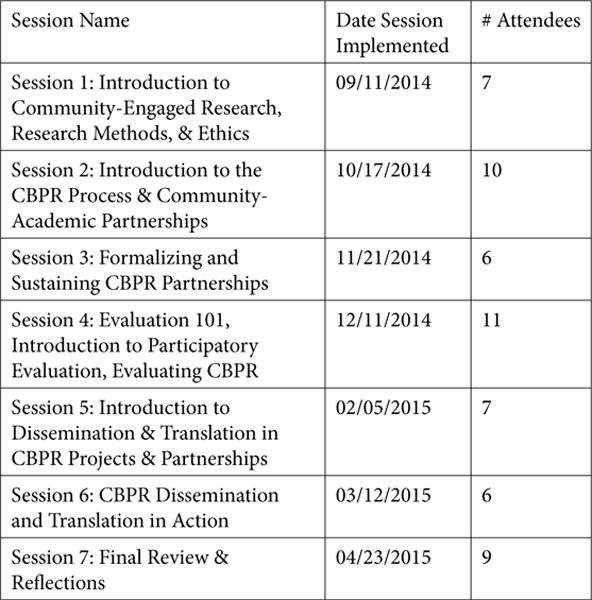
CBPR Curriculum Sessions, Dates, Attendees.
An overall process evaluation plan was developed by the LPHI team prior to implementation of the first training session. Evaluation tools included qualitative field notes taken by an LPHI staff member during each session, participant survey assessments, and follow-up interviews with participants conducted within two weeks of the conclusion of the last session. These evaluation tools are described in greater detail below:
Field notes (n=7): A designated LPHI team member took comprehensive field notes during each session. These notes detailed participant presence and engagement during sessions as well as the duration of time for each lecture and activity. In order to ensure consistency, the same LPHI team member recorded field notes for all seven sessions. Within 24 hours of each session, two to three members of the LPHI development team who had attended or led the session reviewed the notes to ensure their reliability. Next, the LPHI team met to discuss the notes as a group, with the aim of improving future sessions as well as the final curriculum product. For example, the team compared actual activity durations with the original curriculum script and then adjusted the final curriculum accordingly. Participant engagement was assessed through verbal exchanges, body language, and tone of voice and facial expressions, all noted in the field notes.
- Survey assessments (n=25): Following implementation of each session, participants completed open-ended survey assessments designed by the LPHI development team. Surveys measured participants’ comprehension of the session content and captured participant feedback on which activities they felt were successful or unsuccessful as well as the reasons why. Examples of survey questions are:
- “Prior to this training, what knowledge did you have about the research process?”
- “Were there any topics or ideas covered in this training that were unclear? If so, which topics or ideas?”
- “Do you have any recommendations for the trainers on improving training sessions going forward?”
3. Follow-up interviews (n=8): After completion of the seventh and final curriculum session, brief semi-structured interviews were conducted with eight GROWH CODC participants. In order to ensure that both community and academic participants were comfortable discussing strengths and weaknesses related to the curriculum, an LPHI employee who had not worked on curriculum development conducted the interviews. Interviews were organized around the following key themes: pre and post comprehension of CBPR, most and least preferred training sessions and curriculum elements, perceptions of impact of the training on the CODC partnership, and perception of change within the CODC partnership over time.
Both field notes and post-session assessments, deployed during each training session, were designed to assess participants’ knowledge of CBPR as well as perceptions of the curriculum as an effective learning and training tool. This evaluation approach allowed for iterative curriculum development. While preliminary development of all seven modules was completed prior to pilot testing of the first module, LPHI modified the overall curriculum and future sessions as necessary, based on analysis of field notes and participant assessments following each training session. For example, when a particular activity was successful in engaging the group and/or imparting specific knowledge about CBPR, similar activities were incorporated into subsequent modules.
This iterative approach to evaluation and curriculum development ensured that each subsequent module took into account feedback from prior modules and that the final curriculum product captured both successes and limitations of the pilot. In addition to written feedback via assessments, participants were encouraged by the LPHI facilitators to communicate their perceptions of the training session’s materials and activities. This feedback was also incorporated into planning for future sessions.
Evaluation Findings
Following pilot testing of each module, evaluation materials were reviewed and analyzed by LPHI’s curriculum development team using qualitative thematic analysis. Next, the curricular materials for each module were revised according to formal evaluation data as well as verbal feedback from participants. Evaluation findings are summarized below along the following themes: 1) Comprehension of CBPR principles and practices; 2) Changes in the GROWH CODC partnership; and 3) Implications of the CBPR training for other research partnerships.
Comprehension of CBPR Principles and Practice
Survey responses as well as post-training in-depth interviews indicated that participants had increased knowledge regarding central components and tenets of CBPR. In addition to an increase in understanding of CBPR, all participants expressed that they were more confident in their own ability to engage in CBPR projects and partnerships. Two themes emerged from post-curriculum interviews. First, a number of community participants noted that while they had not engaged in a formal CBPR training or project prior to participating in the curriculum, they believed that their organizations had “been doing this work” previously. Secondly, both academic and community participants valued engaging in a formal learning process about CBPR. They indicated that by providing the GROWH partners with a common CBPR language and knowledge base, the curriculum helped with communication between partners.
Changes in the GROWH CODC Partnership
Evaluation findings also revealed that participants saw an improvement in the GROWH CODC’s inter-organizational relationships. In particular, community and academic participants reported more effective and honest communication, an increase in trust, and better appreciation of one another’s limitations and strengths after participation in the pilot training. Participants reported that barriers to transparency between partners diminished as they participated in the curriculum, and that this allowed relationships to evolve, and in the words of one participant, “become more real”. According to participants, the pilot training increased clarity around the roles and competencies of individual GROWH partners and created opportunities for each partner to demonstrate their credibility to the rest of the partnership.
Several participants mentioned that a particular activity, the collaborative development of a logic model for the CBPR curriculum, was especially helpful in recognizing the improvement in relationships between GROWH partners. Prior to the activity, LPHI created an initial logic model for the curriculum informed by the goals set by GROWH partners prior to engaging in the training (see Figure 3a). During the activity, GROWH’s community and academic partners collaboratively developed a logic model that included inputs, outputs, outcomes and impacts for the CBPR curriculum (see Figure 3b). This collaborative logic model demonstrates one of the most important outcomes of the curriculum, one identified by the partners themselves: improved relationships between community and academic partners.
Figure 3a.
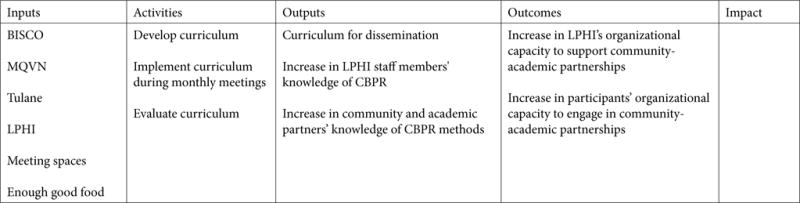
Preliminary Curriculum Logic Model Developed by LPHI.
Figure 3b.
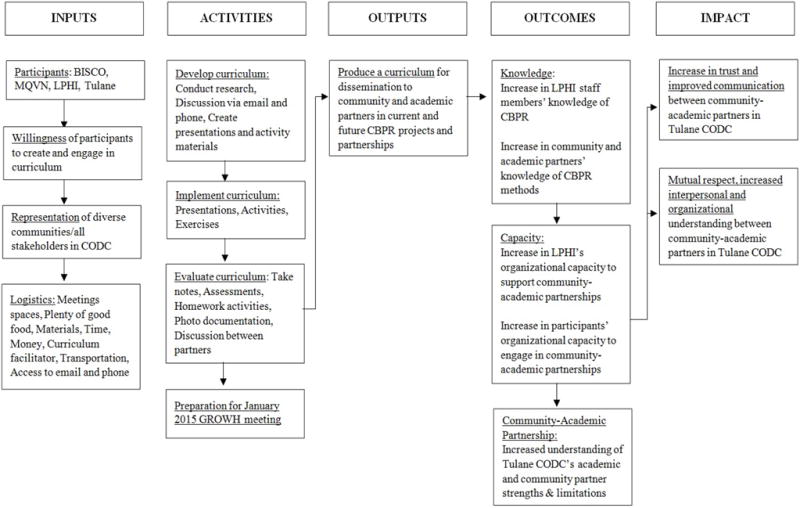
Collaborative Curriculum Logic Model Developed by GROWH CODC Partners.
Implications of the CBPR Training for other Partnerships
Both field notes and written session evaluations revealed that, in keeping with adult learning theory, participants preferred activities and exercises that were interactive and dynamic. For example, activities that encouraged participants to stand up and move around the room were especially popular as well as activities that involved group or one-on-one discussions [8]. Thus, efforts were made to ensure that lectures included as many interactive and physically engaging components as possible, such as guided discussions and short physical and verbal activities punctuated throughout longer lectures. Almost all participants expressed a clear desire for content that was relatable to their context and geographic location. Participants from all partner organizations expressed that more case studies of “CBPR partnerships in action”, particularly in their local context (in this case the Gulf South), would have further enhanced their understanding and future application of CBPR.
There was consensus among almost all participants that CBPR trainings should be held at the beginning of a CBPR partnership and project. Some participants cited the fact that the training was conducted in the middle of the partnership as a drawback when considering whether there had been a positive change in the GROWH partnership. On the whole, participants expressed that the existing GROWH partnership was improved by the pilot training, but that results could have been optimized if the training had been held earlier. In addition, several community and academic participants wished for more opportunities for community partners to educate academic partners on community needs and preferences. Evaluation findings also indicated that participation by researchers throughout all sessions would have been preferred by a majority of the participants. However, the curriculum provided a space for academic researchers working on the GROWH projects to share their progress-to-date and present preliminary findings. Sessions in which academic researchers participated in the curriculum were especially helpful in integrating the curriculum with the actual GROWH project.
Summary of Evaluation Findings
Both formative and summative evaluation approaches were critical to the success of this pilot CBPR curriculum. The process evaluation techniques of field notes and post-session survey assessments were invaluable in facilitating the iterative development of subsequent modules in a way that took into account both the successes and shortcomings of previous modules. These evaluation approaches, in addition to the post-curriculum key informant interviews, proved important in gauging the larger impact of the curriculum on the GROWH CODC’s community-academic partnership. While the curriculum was successful in deepening the existing collaborative relationships between GROWH CODC partners, participants felt that implementing such a training in the formative stages of the project would have better prepared both academic and community partners for the demands and challenges inherent to CBPR such as trust building, shared expectations, competing priorities and resource allocation, as well as its unique processes and benefits. Reduced knowledge gain was cited in several post-training interviews; this was likely due to the fact that modules were implemented monthly. A more condensed schedule, such as presenting modules on back-to-back days or each week, may produce higher retention of the information presented. It is important to note that many of the evaluation findings were not gleaned from written survey assessments. This highlights the importance of field notes, post-curriculum interviews, and informal conversations with participants to assessing the impacts of the curriculum on relationships among participants.
Future Applications of the CBPR Curriculum
Five future developments for which this CBPR curriculum can serve as an anchor are: competency development, translation of the curriculum into education and training products, community development of a CBPR curriculum for academic partners, community practice of CBPR, and future environmental health work. These future developments are described in greater detail below.
Competency development
The mapping of an existing curriculum to competencies is possible [10], and the GROWH partnership plans to do so in the future in order to provide learning benchmarks for the curriculum. While competency development typically precedes curriculum development, the creation of competencies for the CBPR curriculum was not an explicit task assigned to the CODC and was not feasible in the allotted time frame.
Translation of the curriculum into education and training products
The existing CBPR curriculum may be augmented by a compendium portfolio of “field-ready” training products designed to accelerate learning about the applications of CBPR research in general, as well as within the context of environmental health specifically. Examples include module-specific case studies and interactive exercises.
Community development of a CBPR curriculum for academic partners
Trainings associated with community-academic partnerships have traditionally targeted community members. The GROWH CODC experience made clear that there is an important opportunity for a “flipped classroom” strategy where community members would teach research scientists how to bolster community and faculty engagement, research translation, and dissemination.
Community practice of CBPR
The development and piloting of the CBPR curriculum could create opportunities to leverage funding and support for GROWH CODC partners. A community of practice in the Gulf Coast could create a space for community leaders, thought partners and experts on CBPR to bolster resilience and advance health equity. It could also screen community-engaged research studies and proposals to determine the researchers’ proposed level of community engagement and work with them to adhere to the principles of CBPR or community-engaged research prior to beginning the study [10, 11].
Application in future environmental health work
The CBPR curriculum could be utilized by the aforementioned community of practice to train future researchers and community partners. Because the Gulf Coast region faces unique challenges in environmental health, the curriculum is tailored to needs specific to this region. GROWH CODC partners can assist other research projects in the region to better understand and adopt the principles of CBPR and community-engaged research.
Limitations
Creation of the curriculum was not intended as a formal research project and therefore did not seek to answer a specific research question. Instead, the intent was to address a gap in the knowledge and skills of the GROWH community-academic partnership. As such, our project collected data from ten participants and may not be generalizable to other partnerships or communities. Surveys of participant knowledge and participation took place immediately following each session and therefore we are unable to infer long-term knowledge gains from the curriculum. Key informant interviews were conducted within 2 weeks of the last session, thus the curriculum’s impact on the GROWH partnership is limited to that time period.
Staff representing the GROWH CODC’s community and academic partners participated in all seven sessions. The study’s principal investigators were consulted throughout the process regarding progress on the research studies and attended two sessions. Attendance throughout by principal investigators could have further strengthened cohesion and learning, and may have further advanced the community-academic partnership. Because the training was designed to have sessions build on the content and conversations of previous sessions, those who attended every session could more actively and meaningfully participate by drawing on past experiences. Participants reported that the shared experience of going through the training together strengthened relationships among partners. Both the formal group activities and informal time and space for getting to know each other better were critical to strengthening relationships. Those unable to participate in all sessions reported less of a shared experience and had fewer opportunities to cultivate inter-partner relationships.
Acknowledgments
The following individuals played important roles in the development and implementation of curriculum: Laila Fox, Patricia Davis, and Hannah Covert of Tulane School of Public Health and Tropical Medicine; Maggie Gustafson, Katie Sacca, and Amy Pruim of LPHI; Maryal Mewherter, Patty Whitney, and Sharon Foret of BISCO. We would also like to thank the project Principal Investigators Drs. Emily Harville and Jeffrey Wickliffe and all other members of GROWH, BISCO and MQVN CDC for their support.
Funding
This work was supported by the National Institute of Environmental Health Sciences under award number 5U19ES020677. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Competing Interests
None of the authors have any conflicts of interest to disclose
Authors Contributions
Canfield, Angove, and Boselovic led the development, implementation and evaluation of the CBPR curriculumas well as the writing of the manuscript. Brown reviewed all curriculum materials, led some sessions and contributed to the writing of the manuscript. S. Gauthe, Bui, D. Gauthe, Bogue, Denham, and Nguyen participated in the curriculum pilot, informed its implementation and evaluation, and contributed to the manuscript. As the GROWH Principal Investigator, Lichtveld provided overall leadership, reviewed all curriculum materials, led a session on research methods, and contributed to the writing of the manuscript.
References
- 1.Israel BA, Eng E, Schultz AJ, Parker EA, editors. Methods in Community-Based Participatory Research for Health. San Francisco, CA: Jossey-Bass Publishers, USA; 2013. [Google Scholar]
- 2.Minkler M, Wallerstein N, editors. Community-Based Participatory Research for Health: From Process to Outcomes. Jossey-Bass Publishers, USA; 2008. [Google Scholar]
- 3.Israel BA, Schultz AJ, Parker EA, Becker AB. Review of Community Based Research: Assessing Partnership Approaches to Improve Public Health. Annu Rev Public Health. 1998;19:173–202. doi: 10.1146/annurev.publhealth.19.1.173. [DOI] [PubMed] [Google Scholar]
- 4.Lantz PA, Viruell-Fuentes E, Israel BA, Softley D, Guzman R. Can Communities and Academia Work Together on Public Health Research? Evaluation Results from a CBPR Participatory Research Partnership in Detroit. J Urban Health. 2001;78:495–507. doi: 10.1093/jurban/78.3.495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Access Alliance Multicultural Health and Community Services. Community-Based Research Toolkit: Resource for Doing Research with Community for Social Change. Toronto, ON: Access Alliance Multicultural Health and Community Services; 2011. [Google Scholar]
- 6.Cashman SB, Adeky S, Allen AJ, Corburn J, Israel BA, et al. The power and the promise: Working with communities to analyze data, interpret findings, and get to outcomes. American Journal of Public Health. 2008;98:1407–1417. doi: 10.2105/AJPH.2007.113571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Goldstein BD, Osofsky HJ, Lichtveld MY. The Gulf Oil Spill. New England Journal of Medicine. 2011;364:1334–48. doi: 10.1056/NEJMra1007197. [DOI] [PubMed] [Google Scholar]
- 8.Wilson M, Frickel S, Nguyen D, Bui T, Echsner S, et al. A Targeted Health Risk Assessment Following the Deep Water Horizon Oil Spill: Polycyclic Aromatic Hydrocarbon Exposure in Vietnamese-American Shrimp Consumers. Environ Health Perspect. 2015;123:152–159. doi: 10.1289/ehp.1408684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Knowles MS, Holton EF, III, Swanson RA. The Adult Learner. Routledge; 2012. [Google Scholar]
- 10.Neiworth LL, Allan S, D’Ambrosio L, Coplen-Abrahamson M. Charting a Course to Competency: An Approach to Mapping Public Health Core Competencies to Existing Trainings. Health Promot Pract. 2014;15:33S–38S. doi: 10.1177/1524839913509274. [DOI] [PubMed] [Google Scholar]
- 11.Abramson DM, Grattan LM, Mayer B, Colten CE, Arosemena FA, et al. The Resilience Activation Framework: A conceptual model of how access to social resources promotes adaptation and rapid recovery in post-disaster settings. J Behav Health Serv Res. 2015;42:42–57. doi: 10.1007/s11414-014-9410-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Connor KM, Davidson JR. Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC) Depression and Anxiety. 2003;18:76–82. doi: 10.1002/da.10113. [DOI] [PubMed] [Google Scholar]