

Abstract
Objective
To compare the clinical utilities of the platelet count and platelet-lymphocyte ratio (PLR) for predicting survival in patients with cervical cancer.
Results
Multivariate analyses demonstrated that thrombocytosis and elevated PLR were found to be independent prognostic factors for progression-free survival (PFS, P = 0.0077, P = 0.044) and overall survival (OS, P = 0.025, P = 0.019) in separate Multivariate analyses. In the ROC analysis, the platelet count showed a significantly greater area under the ROC curve (AUC) value than that of PLR for predicting patient recurrence (0.5941 versus 0.5331, p = 0.018) and survival (0.6139 versus 0.5468, p = 0.029). In patients without thrombocytosis, elevated PLR correlated with shorter survival (PFS, P = 0.041; OS, P = 0.017). In contrast, PLR in patients with thrombocytosis did not provide prognostic information. We divided patients into 3 prognostic groups using platelet counts and PLR: high-risk (thrombocytosis with any PLR); intermediate-risk (elevated PLR without thrombocytosis); low-risk (none of the above), which allowed for individualized and accurate survival estimates.
Materials and Methods
The baseline characteristics and clinical outcomes of cervical cancer patients were identified. Patients were grouped according to their pretreatment platelet counts or PLR, and clinicopathological characteristics and patient survival were then compared between these groups. The clinical utilities of the platelet count and PLR were compared using a time-dependent receiver operating characteristic (ROC) analysis.
Conclusions
Pretreatment thrombocytosis and elevated PLR were identified as independent predictors in cervical cancer patients. Platelet counts were superior to PLR for predicting the prognosis of uterine cervical cancer patients. Our prognostic model consisting of platelet counts and PLR offers individualized survival estimates.
Keywords: cervical cancer, thrombocytosis, survival, platelet count, platelet-lymphocyte ratio
INTRODUCTION
Cervical cancer is the second most common type of cancer affecting women worldwide and has an annual incidence of 530,000 new cases. Although current standard treatments for invasive cervical cancer are potentially curative, a significant number of patients develop recurrence and die of disease progression, with approximately 250,000 deaths being reported globally each year [1].
The identification of new prognostic factors for cervical cancer will improve our understanding of cervical cancer biology, contribute to the stratification of patients into risk groups, and identify those at a high risk of recurrence after the standard initial treatment.
Platelet count alterations including the platelet count and platelet-lymphocyte ratio (PLR) have recently been attracting attention as prognostic indicators in cancer patients [2–18]. The relationship between elevated platelet counts and malignancy was initially described in 1872 [19]. Since then, an increasing number of studies have reported thrombocytosis in patients with cancer from various origins, and demonstrated that it is associated with poor patient prognosis [20–23]. To the best of our knowledge, 13 studies have investigated the prognostic implications of thrombocytosis in cervical cancer patients, with about half suggesting that thrombocytosis is an independent prognostic factor in cervical patients (Table 1). A recent study on ovarian cancer indicated that paraneoplastic thrombocytosis is due to the enhancements induced in hepatic thrombopoietin synthesis by tumor-derived IL-6. Moreover, the inhibition of thrombopoietin and IL-6 expression abrogated thrombocytosis in tumor-bearing mice and significantly enhanced the therapeutic efficacy of paclitaxel in mouse models of epithelial ovarian cancer [24]. Thus, thrombocytosis is now regarded not only as a prognostic indicator, but also as a potential therapeutic target in human cancers.
Table 1. Summary of studies that investigated the relationship between platelet counts, platelet-lymphocyte ratios, and survival in patients with cervical cancer.
| Reference | No. | Stage | Treatment | Platelet or PLR | Cut-off value | Results | Multivariate analysis |
|---|---|---|---|---|---|---|---|
| Hernandez et al. [2], 1992 | 113 | I-IV | RT | Platelet | 400 × 103/μl | Independent prognostic indicator of 5-year survival | Yes |
| Rodriguez et al. [3], 1994 | 219 | IB | Surgery | Platelet | 300 × 103/μl | Independent prognostic indicator of 5-year survival | Yes |
| Hernandez et al. [4],1994 | 623 | IB | Surgery | Platelet | 400 × 103/μl | Not independent prognostic indicator of 5-year survival | Yes |
| Lopes et al. [5], 1994 | 643 | I-IV | Surgery or RT | Platelet | 400 × 103/μl | Prognostic indicator of 5-year survival | No |
| De Jonge et al. [6], 1999 | 93 | IB | Surgery | Platelet | 400 × 103/μl | Not independent prognostic indicator of 5-year survival | yes |
| Hernandez et al. [7],2000 | 291 | IIB-IVA | RT | Platelet | 400 × 103/μl | Independent prognostic indicator of OS (patients negative pelvic nodes) | Yes |
| Gadducci et al. [8], 2010 | 46 | IB2-IIB | Surgery | Platelet | 272 × 103/μl | Independent prognostic indicator of OS, but not of PFS | Yes |
| Gadducci et al. [9], 2010 | 140 | IB2-IIB | Surgery | Platelet | 270 × 103/μl | Not independent prognostic indicator of PFS and OS | Yes |
| Qiu et al. [10], 2010 | 318 | I-IV | NA | Platelet | 400 × 103/μl | Not prognostic indicator of OS | No |
| Wang et al. [11], 2012 | 111 | IB2-IIB | Surgery | Platelet | 266 × 103/μl | Not prognostic indicator of PFS and OS | No |
| Zhang et al. [12],2014 | 460 | I-II | Surgery | PLR | 150 | Not prognostic indicator of PFS and OS | No |
| Kawano et al. [13], 2015 | 286 | IB-IVA | RT | Platelet | 350 × 103/μl | Independent prognostic indicator of OS | Yes |
| Xiao et al. [14], 2015 | 238 | I-IV | CCRT | Platelet | 200 × 103/μl | Not prognostic indicator of PFS and OS | No |
| Zhao et al. [15], 2015 | 220 | I-IIA | Surgery | Platelet | 300 × 103/μl | Not independent prognostic indicator of OS | Yes |
| Nakamura et al. [16], 2015 | 32 | NA | CCRT | PLR | 322 | Independent prognostic indicator of 200-day survival | Yes |
| Zheng et al. [17], 2016 | 795 | IA-IIA | Surgery | PLR | 128.3 | Independent prognostic indicator of OS | Yes |
| Chen et al. [18], 2016 | 407 | IB-IIA | Surgery | PLR | 138.35 (PFS), 143.47 (OS) | Independent prognostic indicator of PFS and OS | Yes |
| Present study, 2017 | 684 | IA-IVA | Surgery or RT | Platelet, PLR | 350 × 103/μl (Platelet), 125.23 (PFS), 131.44 (OS) | Both factors are independent prognostic indicator of PFS and OS, Predictive value of platelet count is greater than that of PLR | Yes |
RT, radiotherapy; CCRT, concurrent chemoradiotherapy; PLR, platelet-lymphocyte ratio; PFS, progression free survival; OS, overall survival; NA, not available.
As shown in Table 1, 4 studies have investigated the prognostic implications of increased PLR in cervical cancer patients, with 3 studies suggesting that increased PLR is an independent predictor of survival. However, since most of the studies described above only included surgically-treated early-stage cervical cancer patients, the prognostic significance of PLR in cervical cancer remains unclear. Moreover, the clinical utilities of platelet counts and PLR have not yet been compared, and there is currently no information on how physicians may distinguish between platelet counts and PLR in the management of cervical cancer.
Table 4. Univariate and multivariate analyses for overall survival in cervical cancer patients.
| Univariate analysis | Multivariate analysis 1 | Multivariate analysis 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Hazard ratio | 95% CI | p-value | Hazard ratio | 95% CI | p-value | Hazard ratio | 95% CI | |||
| Age | < 50 | |||||||||
| ≥ 50 | 1.24 | 0.93–1.68 | 0.14 | 0.97 | 0.70–1.37 | 0.88 | 0.93 | 0.67–1.30 | 0.69 | |
| Stage | I-IIA | |||||||||
| IIB-IVB | 4.93 | 3.58–6.91 | < 0.001 | 2.64 | 1.72–4.12 | < 0.001 | 2.64 | 1.72–4.11 | < 0.001 | |
| Histology | SCC | |||||||||
| Non-SCC | 1.14 | 0.82–1.55 | 0.43 | 2.09 | 1.46–2.94 | < 0.001 | 2.05 | 1.44–2.88 | < 0.001 | |
| Pelvic node metastasis | Negative | |||||||||
| Positive | 2.50 | 1.87–3.32 | < 0.001 | 1.77 | 1.31–2.39 | < 0.001 | 1.87 | 1.38–2.52 | < 0.001 | |
| Tumor size (mm) | < 40 | |||||||||
| ≥ 40 | 5.03 | 3.63–7.09 | < 0.001 | 2.78 | 1.83–4.30 | < 0.001 | 2.72 | 1.79–4.20 | < 0.001 | |
| Treatment | Surgery | |||||||||
| Others 3 | 2.26 | 1.70–3.01 | < 0.001 | 1.12 | 0.77–1.63 | 0.56 | 1.15 | 0.80–1.67 | 0.45 | |
| Platelet count (/μl) | < 350,000 | |||||||||
| ≥350,000 | 1.93 | 1.34–2.72 | < 0.001 | 1.56 | 1.06–2.24 | 0.025 | ||||
| PLR | < 131.44 | |||||||||
| ≥ 131.44 | 1.59 | 1.20–2.11 | 0.0012 | 1.41 | 1.06–1.87 | 0.019 | ||||
SCC, squamous cell carcinoma; PLR, platelet-lymphocyte ratio; CI, confidence interval.
1 Multivariate analysis in which PLR is excluded from prognostic variables (platelet count is included).
2 Multivariate analysis in which platelet count is excluded from prognostic variables (PLR is included).
3 Concurrent chemoradiotherapy, radiotherapy and chemotherapy.
In the present study, we first investigated the prognostic significance of elevated platelet counts and PLR in patients with FIGO stage IA-IVA cervical cancer. Then, we compared the clinical utilities of platelet counts and PLR for predicting the survival of patients with cervical cancer. Finally, we established a prognostic model using platelet counts and PLR to predict patient survival.
RESULTS
Prognostic significance of platelet counts
The clinicopathological characteristics of patients according to platelet counts are shown in Table 2. Among 684 patients, 87 (12.7%) had platelet counts equal to or greater than 350,000/ml (the thrombocytosis group) at the time of the initial diagnosis. Patients with thrombocytosis were significantly younger (P < 0.001) and presented with a more advanced clinical stage (P = 0.036) than those without thrombocytosis. Thrombocytosis correlated with significantly shorter PFS (P < 0.001) and OS (P < 0.001) in the univariate analysis and Kaplan-Meier analysis (Tables 3, 4, Figure 1A). In the multivariate analysis (Tables 3, 4), in addition to an advanced clinical stage, non-SCC histology, pelvic node metastasis, and larger tumor size, an elevated platelet count (> 350,000/μl) was found to be an independent prognostic factor of PFS (HR, 1.63; 95% CI, 1.14–2.28; P = 0.0077) and OS (HR, 1.56; 95% CI, 1.06–2.24; P = 0.025).
Table 2. Clinicopathological characteristics of patients according to platelet counts and PLR 1.
| All patients | Thrombocytosis | Normal platelet count | Elevated PLR | Normal PLR | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No | (%) | No | (%) | No | (%) | p-value | No | (%) | No | (%) | p-value | ||
| Age | < 50 | 268 | 39.2 | 52 | 19.4 | 216 | 80.6 | 123 | 45.9 | 145 | 54.1 | ||
| ≥ 50 | 416 | 60.8 | 35 | 8.4 | 381 | 91.6 | < 0.001 | 140 | 33.7 | 276 | 66.3 | 0.0013 | |
| Stage | I-IIA | 378 | 55.3 | 39 | 10.3 | 339 | 89.7 | 132 | 34.9 | 246 | 65.1 | ||
| IIB-IVB | 306 | 44.7 | 48 | 15.7 | 258 | 84.3 | 0.036 | 131 | 42.8 | 175 | 57.2 | 0.035 | |
| Histology | SCC | 511 | 74.7 | 63 | 12.3 | 448 | 87.7 | 189 | 37.0 | 322 | 63.0 | ||
| Non-SCC | 173 | 25.3 | 24 | 13.9 | 149 | 86.1 | 0.6 | 74 | 42.8 | 99 | 57.2 | 0.18 | |
| Pelvic node metastasis | Negative | 517 | 75.6 | 59 | 11.4 | 458 | 88.6 | 204 | 39.5 | 313 | 60.5 | ||
| Positive | 167 | 24.4 | 28 | 16.8 | 139 | 83.2 | 0.071 | 59 | 35.3 | 108 | 64.7 | 0.34 | |
| Tumor size (mm) | < 40 | 328 | 48.0 | 39 | 11.9 | 289 | 88.1 | 117 | 35.7 | 211 | 64.3 | ||
| ≥ 40 | 356 | 52.0 | 48 | 13.5 | 308 | 86.5 | 0.53 | 146 | 41.0 | 210 | 59.0 | 0.15 | |
| Treatment | Surgery | 395 | 57.7 | 47 | 11.9 | 348 | 88.1 | 153 | 38.7 | 242 | 61.3 | ||
| Others 2 | 289 | 42.3 | 40 | 13.8 | 249 | 86.2 | 0.45 | 110 | 38.1 | 179 | 61.9 | 0.86 | |
| PLR | < 131.44 | 421 | 61.5 | 21 | 5.0 | 400 | 95.0 | ||||||
| ≥ 131.44 | 263 | 28.5 | 66 | 33.5 | 197 | 66.5 | < 0.001 | ||||||
| Platelet count (/μl) | < 350,000 | 597 | 87.3 | 197 | 33.0 | 400 | 67.0 | ||||||
| ≥350,000 | 87 | 12.7 | 66 | 75.9 | 21 | 24.1 | < 0.001 | ||||||
| Total | 684 | 100 | 87 | 12.7 | 597 | 87.3 | 263 | 38.5 | 421 | 61.5 | |||
SCC, squamous cell carcinoma; PLR, platelet-lymphocyte ratio.
1 A PLR cut-off value of 131.44 was employed in this analysis.
2 Concurrent chemoradiotherapy, radiotherapy and chemotherapy.
Table 3. Univariate and multivariate analyses for progression-free survival in cervical cancer patients.
| Univariate analysis | Multivariate analysis 1 | Multivariate analysis 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Hazard ratio | 95% CI | p-value | Hazard ratio | 95% CI | p-value | Hazard ratio | 95% CI | p-value | ||
| Age | < 50 | |||||||||
| ≥ 50 | 1.3 | 0.99–1.71 | 0.058 | 1.12 | 0.82–1.55 | 0.47 | 1.06 | 0.78–1.45 | 0.70 | |
| Stage | I-IIA | |||||||||
| IIB-IVB | 3.87 | 2.94–5.17 | < 0.001 | 2.16 | 1.48–3.17 | < 0.001 | 2.16 | 1.48–3.16 | < 0.001 | |
| Histology | SCC | |||||||||
| Non-SCC | 1.13 | 0.84–1.5 | 0.41 | 1.86 | 1.34–2.54 | < 0.001 | 1.87 | 1.35–2.56 | < 0.001 | |
| Pelvic node metastasis | Negative | |||||||||
| Positive | 2.61 | 2.01–3.38 | < 0.001 | 1.91 | 1.45–2.51 | < 0.001 | 2.00 | 1.52–2.64 | < 0.001 | |
| Tumor size (mm) | < 40 | |||||||||
| ≥ 40 | 4.22 | 3.63–7.09 | < 0.001 | 2.66 | 1.84–3.89 | < 0.001 | 2.65 | 1.83–3.86 | < 0.001 | |
| Treatment | Surgery | |||||||||
| Others 3 | 1.94 | 1.50–2.52 | < 0.001 | 0.95 | 0.68–1.37 | 0.80 | 0.99 | 0.70–1.39 | 0.93 | |
| Platelet count (/μl) | < 350,000 | |||||||||
| ≥350,000 | 1.90 | 1.35–2.62 | < 0.001 | 1.63 | 1.14–2.28 | 0.0077 | ||||
| PLR | < 125.23 | |||||||||
| ≥ 125.23 | 1.39 | 1.07–1.79 | 0.012 | 1.31 | 1.01–1.70 | 0.044 | ||||
SCC, squamous cell carcinoma; PLR, platelet-lymphocyte ratio; CI, confidence interval.
1 Multivariate analysis in which PLR is excluded from prognostic variables (platelet count is included).
2 Multivariate analysis in which platelet count is excluded from prognostic variables (PLR is included).
3 Concurrent chemoradiotherapy, radiotherapy and chemotherapy.
Figure 1.
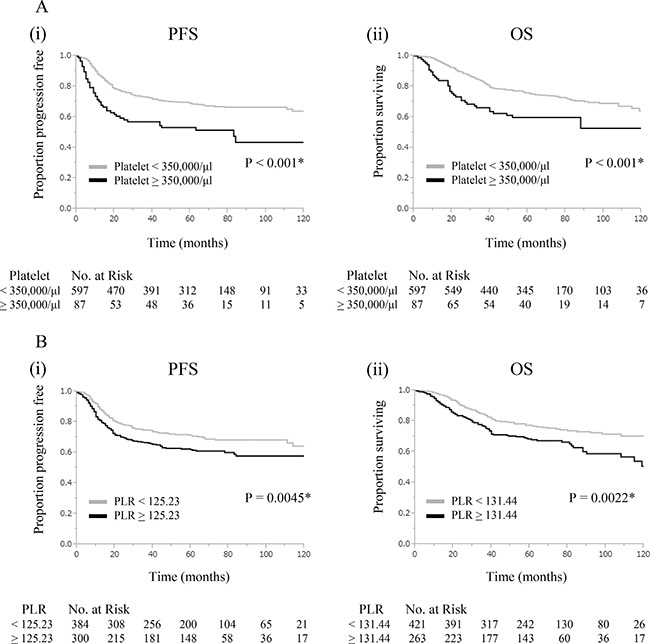
Clinical implications of platelet counts and PLR in cervical cancer patients (A) Significance of elevated platelet counts (Platelet count; ≥ 350,000/μl vs < 350,000/μl). (i) Kaplan-Meier estimates of progression-free survival. (ii) Kaplan-Meier estimates of overall survival. (B) Significance of elevated PLR. (i) Kaplan-Meier estimates of progression-free survival (PLR; ≥ 125.23 vs < 125.23). (ii) Kaplan-Meier estimates of overall survival (PLR; ≥ 131.44 vs < 131.44).
Prognostic significance of PLR
ROC curves were described to select the optimal cut-off value for PLR (Supplementary Figure 1). The cut-off values of PLR for PFS and OS were 125.23 and 131.44, respectively. The clinicopathological characteristics of patients according to PLR are shown in Table 2 and Supplementary Table 1. Among 684 patients, 300 (43.9%) and 263 (38.5%) displayed PLR equal to or greater than 125.23 and 131.44, respectively. Patients with elevated PLR were significantly younger (P = 0.0059, P = 0.0013) and presented with a more advanced clinical stage (P = 0.014, P = 0.035) than those with normal PLR. As shown in Figure 1B, elevated PLR correlated with significantly shorter PFS and OS (PFS: P = 0.0045, OS: P = 0.0022). In the multivariate analysis, in addition to an advanced clinical stage, non-SCC histology, pelvic node metastasis, and larger tumor size, elevated PLR remained an independent prognostic factor of PFS (Table 3: HR, 1.31; 95% CI, 1.01–1.70; P = 0.044) and OS (Table 4: HR, 1.41; 95% CI, 1.06–1.87; P = 0.019).
Comparison of utilities of platelet counts versus PLR
In order to compare the clinical utilities of platelet counts and PLR for predicting patient prognoses, ROC curves for platelet counts and PLR were generated and compared (Figure 2A). The area under the ROC curve (AUC) for predicting recurrence using platelet counts and PLR were 0.5941 (95% CI, 0.5448–0.6415) and 0.5331 (95% CI, 0.4833–0.5822), respectively. The AUC for predicting survival using platelet counts and PLR were 0.6139 (95% CI, 0.5552–0.6695) and 0.5468 (95% CI, 0.4889–0.6034), respectively. Platelet counts showed significantly greater AUC values than PLR for predicting recurrence (p = 0.018) and survival (p = 0.029).
Figure 2. Comparison of clinical utilities of platelet counts and platelet-lymphocyte ratios.
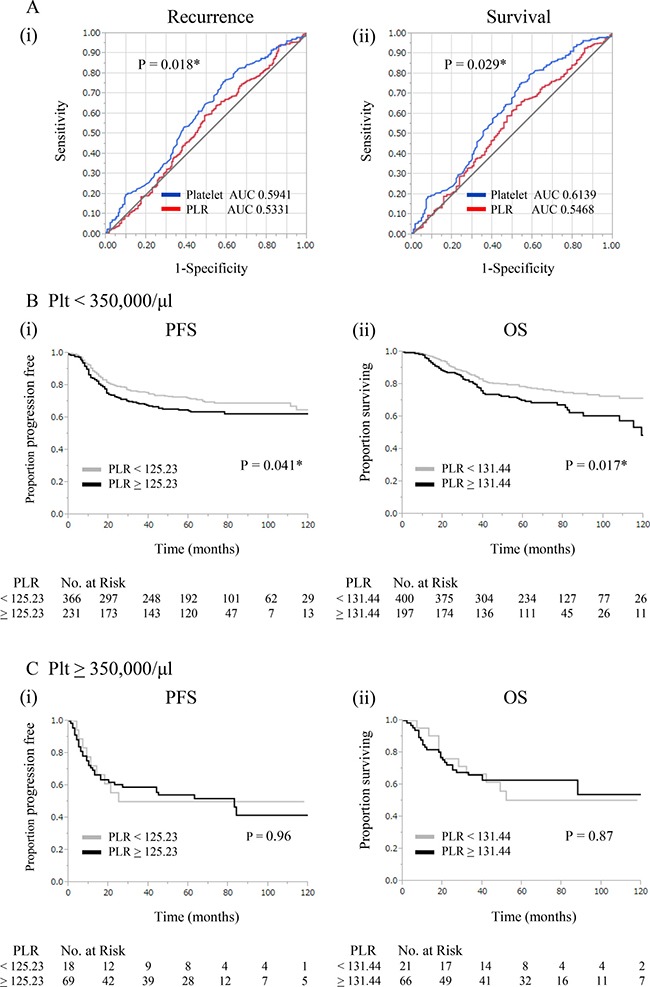
(A) ROC curves for (i) recurrence and (ii) survival at 3 years for platelet counts and PLR. (B) Significance of PLR in patients without thrombocytosis (< 350,000/μl). (i) Kaplan-Meier estimates of progression-free survival (PLR; ≥ 125.23 vs < 125.23). (ii) Kaplan-Meier estimates of overall survival (PLR; ≥ 131.44 vs < 131.44). (C) Significance of PLR in patients with thrombocytosis (≥ 350,000/μl). (i) Kaplan-Meier estimates of progression-free survival (PLR; ≥ 125.23 vs < 125.23). (ii) Kaplan-Meier estimates of overall survival (PLR; ≥ 131.44 vs < 131.44).
Prognostic models using platelet counts and PLR
In order to establish a model for the prediction of life expectancy, PFS and OS were first assessed according to platelet counts and PLR. As shown in Figure 2B, in patients without thrombocytosis, elevated PLR correlated with shorter PFS (P = 0.041) and OS (P = 0.017). In contrast, in patients with thrombocytosis, survival was not influenced by PLR, indicating that it does not provide any prognostic information in this patient population (Figure 2C).
Based on these results, we finally established a prognostic model in which patients were divided into 3 prognostic groups (Figure 3A(i), 3B(i)): high-risk (patients with thrombocytosis regardless of PLR); intermediate-risk (patients with elevated PLR without thrombocytosis); low-risk (none of the above). As shown in Supplementary Table 2, differential treatment outcomes were observed in association with the risk classifications. When PFS and OS were compared between the groups, patients in the high-risk group showed significantly lower PFS and OS rates than those in the intermediate-risk group (Figure 3A (ii): P = 0.021, 3B (ii): P = 0.018). Moreover, the PFS and OS rates of patients in the intermediate-risk group were significantly lower than those in the low-risk group (Figure 3A (ii): P = 0.045, 3B (ii): P = 0.043).
Figure 3. Prognostic model using platelet counts and PLR.
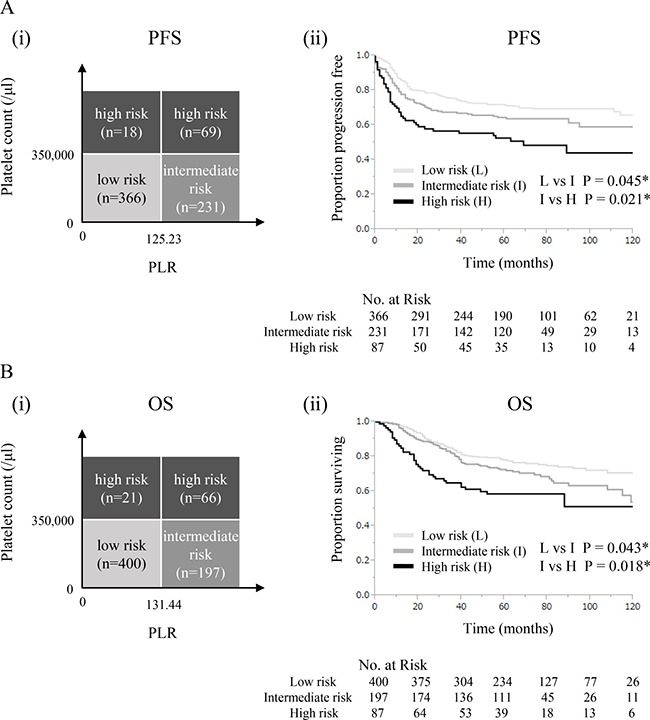
(A) (i) Risk classification for progression-free survival. (ii) Kaplan-Meier estimates of progression-free survival based on risk classification. (B) (i) Risk classification for overall survival. (ii) Kaplan-Meier estimates of overall survival based on risk classification.
DISCUSSION
In the present study, we showed that an elevated platelet count (≥ 350,000/μl) was an independent predictor of shorter PFS and OS in cervical cancer patients. These results are consistent with previous findings (Table 1). Among our study population, 12.7% of patients displayed elevated platelet counts (≥ 350,000/μl), which correlated with a younger age and advanced clinical stage. We also observed elevated PLR (≥ 125.23 for PFS and ≥ 131.44 for OS) in approximately 40% of patients, and identified it as an independent predictor of shorter PFS and OS in cervical cancer patients. This result is also consistent with previous findings (Table 1). However, since most of the studies that previously investigated the significance of increased PLR only included surgically-treated early-stage cervical cancer patients (Table 1), the present study provides a novel insight into PLR in cervical cancer treatment: elevated PLR at the initial diagnosis is prognostically important regardless of the clinical stage and treatment modality. Moreover, our ROC analysis demonstrated, for the first time, that platelet counts are significantly superior to PLR for the prediction of patient prognoses. We consider this result to be clinically important because it suggests that platelet counts need to be preferentially examined in patients with cervical cancer.
There are currently no universally accepted risk classifications that may be applied to all cervical cancer patients: i.e. patients treated with surgery, definitive radiotherapy, and chemotherapy. Thus, the results of the present study may have valuable clinical implications. Since the present study includes stage IA-IVA cervical cancer patients treated with surgery, definitive radiotherapy, or chemotherapy, the prognostic model proposed herein may be applied to all cervical cancer patients. Moreover, our prognostic model requires only low-cost peripheral blood examinations to identify a group of patients at high risk of recurrence. As shown in Figure 3, we demonstrated that it was possible to divide patients into 3 prognostic groups using platelet counts and PLR: high-risk (patients with thrombocytosis regardless of PLR); intermediate-risk (patients with elevated PLR without thrombocytosis); low-risk (none of the above). This prognostic model may have advantages that are relevant to clinical practices: this simple model offers individualized survival estimates (Figure 3A (ii), 3B (ii)). In addition, this model may enable physicians to offer closer follow-ups for patients in the intermediate- and high-risk groups. The results shown in Figures 2, 3 also provide important information on the clinical applications of platelet counts and PLR: we recommend that platelet counts be initially examined for survival estimations in cervical cancer patients. PLR may then be evaluated in patients without thrombocytosis only because it did not provide prognostic information on patients with thrombocytosis.
Based on the poor prognosis of cervical cancer patients who display elevated platelet counts or PLR, novel treatment strategies need to be developed. The mechanisms responsible for increased platelet production in cervical cancer and subsequent increases in the aggressiveness of the disease remain poorly understood. However, theoretically, treatments targeting thrombopoiesis-stimulating cytokines or growth factors, their receptors, or their downstream effectors may exhibit therapeutic efficacy in cervical cancer patients displaying pretreatment thrombocytosis. In a previous study, the inhibition of thrombopoietin or IL-6 prevented the development of thrombocytosis in mice and significantly enhanced the therapeutic efficacy of paclitaxel in mouse models of epithelial ovarian cancer [24]. Thus, in order to obtain a clearer understanding of platelet count alterations and advance the development of novel treatments, further mechanistic investigations on cervical cancer are warranted.
The limitations of our study need to be addressed. The first limitation is that the present study was conducted at a single institution. We intend to verify our clinical findings in collaborative multi-institutional studies in the future. Another limitation is the retrospective nature of the present study. The significance of elevated platelet counts, PLR, and our prognostic model consisting of platelet counts and PLR need to be prospectively evaluated in future studies. The second limitation is the cut-off values used for thrombocytosis. In the present study, we defined elevated platelet counts as greater than or equal to 350,000/μl. The cut-off values for thrombocytosis in previous studies that investigate the significance of thrombocytosis in cervical cancer ranged between 200,000/μl and 400,000/μl, with 400,000/μl being the most popular cut-off value (Table 1). However, most of the studies listed in Table 1 were from countries other than Japan. In studies on various malignant tumors from Japanese institutions, the cut-off values for thrombocytosis were lower: most studies employed a cut-off value between 22,000/μl and 370,000/μl to define thrombocytosis [23, 25–29]. The reason why a lower cut-off value was employed in studies from Japanese institutions currently remains unknown; however, the baseline platelet count in cancer patients may differ due to ethnicity. We also showed that patients with thrombocytosis were significantly younger (P < 0.001) than those without thrombocytosis. This result is consistent with a recent finding on cervical cancer [17]. However, the reason for this phenomenon remains unknown. Thus, the optimal platelet threshold for diagnosing thrombocytosis and the underlying mechanisms responsible for the development of thrombocytosis need to be investigated in future studies.
In conclusion, thrombocytosis and elevated PLR at the time of the initial diagnosis were identified as independent predictors of PFS and OS in FIGO stage IA-IVA cervical cancer patients. Platelet counts were significantly superior to PLR for predicting patient prognoses. Our proposed prognostic model consisting of platelet counts and PLR offers individualized and accurate survival estimates.
MATERIALS AND METHODS
Patients
Permission to proceed with data acquisition and analyses was obtained from the Institutional Review Board of Osaka University Hospital. A list of patients diagnosed with FIGO stage IA-IVA cervical cancer and treated at Osaka University Hospital between November 1993 and December 2011 was generated from our institutional tumor registry, and their clinical data were retrospectively analyzed. Patients who had been diagnosed with other types of cancers within the past 5 years, had a history of splenectomy, myeloproliferative disorders, or acute inflammatory disease were excluded. Of the 684 patients included in the present study, 286 had been examined in a previous clinical study [13].
Treatment and post-treatment follow-up
Patients were treated in accordance with institutional treatment guidelines. Briefly, patients with FIGO stage IA2-IIB cervical cancer and younger than 70 years were treated with radical hysterectomy plus pelvic lymphadenectomy with or without adjuvant radiotherapy as described previously [30]. Adjuvant radiotherapy with or without platinum-based concurrent chemotherapy, was indicated when a patient's pathological report displayed any one of the following ‘high-risk’ prognostic factors: parametrial invasion, pelvic lymph node metastasis, or a positive surgical margin, or one of the following ‘intermediate-risk’ prognostic factors: deep stromal invasion, lymphovascular space invasion, or a large tumor (more than 4 cm in diameter), as reported previously [30]. Patients with FIGO stage III-IV disease, patients with FIGO stage I-II disease and older than 70 years, or patients with FIGO stage IA2-IIB disease and younger than 70 years who desired definitive radiotherapy rather than surgery were treated with definitive radiotherapy consisting of external beam radiation therapy followed by high-dose-rate intracavitary brachytherapy with or without platinum-based concurrent chemotherapy as described previously [31]. Patients with systemic disease were primarily treated with platinum-based chemotherapy as described previously [32, 33]. Follow-up examinations performed after the initial treatment were conducted by gynecological oncologists or/and radiation oncologists at regular intervals in an outpatient clinic, as reported previously [31, 34].
Definition of elevated platelet counts and PLR
During the period between the first presentation and the start day of the initial treatment, all patients underwent at least 2 blood tests including complete blood counts. Thrombocytosis was defined as platelet counts equal to or greater than 350,000/μl on at least 2 separate occasions, as described previously [13]. Elevated PLR for predicting progression-free survival (PFS) or overall survival (OS) were defined as PLR equal to or greater than 125.23 or 131.44, respectively (Supplementary Figure 1). The cut-off values for PLR were defined based on the maximum Youden index (i.e. sensitivity+specificity-1) in the time-dependent receiver operating characteristic (ROC) curve for PFS and OS, as reported previously [35, 36].
Statistical analysis
PFS was defined as the time from the date of therapy to the date of the first physical or radiographical evidence of disease progression. OS was defined as the time from the date of therapy to the date of death.
Time-dependent ROC curves were generated to evaluate the diagnostic performance of platelet counts and PLR for predicting recurrence or death at 3 years after the treatment. Differences in AUCs were analyzed according to the methods described in a previous study [37].
Continuous data were compared between the groups using the Student's t-test or Log-rank test, where appropriate. Frequency counts and proportions were compared between the groups using the chi-squared test or a two-tailed Fisher's exact test, where appropriate. The survival analysis was based on the Kaplan-Meier method and was compared by the Wilcoxon test. Cox's proportional hazards regression analysis was performed to identify significant independent prognostic factors for survival. P-values of < 0.05 were considered to be significant. All analyses were performed using the software JMP Pro version 11.0 (SAS Institute, Cary, NC).
SUPPLEMENTARY MATERIALS FIGURES AND TABLES
Footnotes
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
FUNDING
This study was supported in part by Grant-in-aid for General Scientific Research No. 23592446 from the Ministry of Education, Culture, Sports, Science, and Technology of Japan.
REFERENCES
- 1.Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108. doi: 10.3322/caac.21262. [DOI] [PubMed] [Google Scholar]
- 2.Hernandez E, Lavine M, Dunton CJ, Gracely E, Parker J. Poor prognosis associated with thrombocytosis in patients with cervical cancer. Cancer. 1992;69:2975–2977. doi: 10.1002/1097-0142(19920615)69:12<2975::aid-cncr2820691218>3.0.co;2-a. [DOI] [PubMed] [Google Scholar]
- 3.Rodriguez GC, Clarke-Pearson DL, Soper JT, Berchuck A, Synan I, Dodge RK. The negative prognostic implications of thrombocytosis in women with stage IB cervical cancer. Obstet Gynecol. 1994;83:445–448. [PubMed] [Google Scholar]
- 4.Hernandez E, Heller PB, Whitney C, Diana K, Delgado G. Thrombocytosis in surgically treated stage IB squamous cell cervical carcinoma (A Gynecologic Oncology Group study) Gynecol Oncol. 1994;55:328–332. doi: 10.1006/gyno.1994.1300. [DOI] [PubMed] [Google Scholar]
- 5.Lopes A, Daras V, Cross PA, Robertson G, Beynon G, Monaghan JM. Thrombocytosis as a prognostic factor in women with cervical cancer. Cancer. 1994;74:90–92. doi: 10.1002/1097-0142(19940701)74:1<90::aid-cncr2820740116>3.0.co;2-0. [DOI] [PubMed] [Google Scholar]
- 6.De Jonge ET, Viljoen E, Lindeque BG, Amant F, Nesland JM, Holm R. The prognostic significance of p53, mdm2, c-erbB-2, cathepsin D, and thrombocytosis in stage IB cervical cancer treated by primary radical hysterectomy. Int J Gynecol Cancer. 1999;9:198–205. doi: 10.1046/j.1525-1438.1999.99019.x. [DOI] [PubMed] [Google Scholar]
- 7.Hernandez E, Donohue KA, Anderson LL, Heller PB, Stehman FB. The significance of thrombocytosis in patients with locally advanced cervical carcinoma: a Gynecologic Oncology Group study. Gynecol Oncol. 2000;78:137–142. doi: 10.1006/gyno.2000.5838. [DOI] [PubMed] [Google Scholar]
- 8.Gadducci A, Teti G, Barsotti C, Tana R, Fanucchi A, Orlandini C, Fabrini MG, Genazzani AR. Clinicopathological variables predictive of clinical outcome in patients with FIGO stage Ib2-IIb cervical cancer treated with cisplatin-based neoadjuvant chemotherapy followed by radical hysterectomy. Anticancer Res. 2010;30:201–208. [PubMed] [Google Scholar]
- 9.Gadducci A, Cosio S, Zola P, Tisi G, Ferrero A, Piovano E, Cristofani R, Greco C, Sartori E. Pretreatment platelet and hemoglobin levels are neither predictive nor prognostic variables for patients with locally advanced cervical cancer treated with neoadjuvant chemotherapy and radical hysterectomy: a retrospective Italian study. Int J Gynecol Cancer. 2010;20:1399–1404. doi: 10.1111/IGC.0b013e3181f1574e. [DOI] [PubMed] [Google Scholar]
- 10.Qiu MZ, Xu RH, Ruan DY, Li ZH, Luo HY, Teng KY, Wang ZQ, Li YH, Jiang WQ. Incidence of anemia, leukocytosis, and thrombocytosis in patients with solid tumors in China. Tumour Biol. 2010;31:633–641. doi: 10.1007/s13277-010-0079-8. [DOI] [PubMed] [Google Scholar]
- 11.Wang D, Wu M, Ren T, Wan XR, Feng FZ, Huang HF, Yang JX, Shen K, Xiang Y. [Effects of prechemotherapy hemoglobin and platelet levels in patients with stage Ib2-IIb cervical cancer treated with neoadjuvant chemotherapy followed by radical hysterectomy]. [Article in Chinese] Zhonghua Fu Chan Ke Za Zhi. 2012;47:577–81. [PubMed] [Google Scholar]
- 12.Zhang Y, Wang L, Liu Y, Wang S, Shang P, Gao Y, Chen X. Preoperative neutrophil-lymphocyte ratio before platelet-lymphocyte ratio predicts clinical outcome in patients with cervical cancer treated with initial radical surgery. Int J Gynecol Cancer. 2014;24:1319–1325. doi: 10.1097/IGC.0000000000000219. [DOI] [PubMed] [Google Scholar]
- 13.Kawano M, Mabuchi S, Matsumoto Y, Sasano T, Takahashi R, Kuroda H, Kozasa K, Isohashi F, Ogawa K, Kimura T. Prognostic Significance of Pretreatment Thrombocytosis in Cervical Cancer Patients Treated With Definitive Radiotherapy. Int J Gynecol Cancer. 2015;25:1656–1662. doi: 10.1097/IGC.0000000000000533. [DOI] [PubMed] [Google Scholar]
- 14.Xiao Y, Ren YK, Cheng HJ, Wang L, Luo SX. Modified Glasgow prognostic score is an independent prognostic factor in patients with cervical cancer undergoing chemoradiotherapy. Int J Clin Exp Pathol. 2015;8:5273–5281. [PMC free article] [PubMed] [Google Scholar]
- 15.Zhao K, Deng H, Qin Y, Liao W, Liang W. Prognostic significance of pretreatment plasma fibrinogen and platelet levels in patients with early-stage cervical cancer. Gynecol Obstet Invest. 2015;79:25–33. doi: 10.1159/000365477. [DOI] [PubMed] [Google Scholar]
- 16.Nakamura K, Nishida T, Haruma T, Haraga J, Omichi C, Ogawa C, Kusumoto T, Seki N, Masuyama H, Hiramatsu Y. Pretreatment platelet-lymphocyte ratio is an independent predictor of cervical cancer recurrence following concurrent chemoradiation therapy. Mol Clin Oncol. 2015;3:1001–1006. doi: 10.3892/mco.2015.595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Zheng RR, Huang M, Jin C, Wang HC, Yu JT, Zeng LC, Zheng FY, Lin F. Cervical cancer systemic inflammation score: a novel predictor of prognosis. Oncotarget. 2016;7:15230–42. doi: 10.18632/oncotarget.7378. https://doi.org/10.18632/oncotarget.7378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Chen L, Zhang F, Sheng XG, Zhang SQ, Chen YT, Liu BW. Peripheral platelet/lymphocyte ratio predicts lymph node metastasis and acts as a superior prognostic factor for cervical cancer when combined with neutrophil: Lymphocyte. Medicine (Baltimore) 2016;95:e4381. doi: 10.1097/MD.0000000000004381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Riess L. Zur pathologischen anatomie des blutes. Arch Anat Physiol Wissensch Med. 1872;39:237–249. [Google Scholar]
- 20.Gu ML, Yuan CJ, Liu XM, Zhou YC, FF Di SH Sun, Qu QY. Pre-treatment Elevated Platelet Count Associates with HER2 Overexpression and Prognosis in Patients with Breast Cancer. Asian Pac J Cancer Prev. 2015;16:5537–5540. doi: 10.7314/apjcp.2015.16.13.5537. [DOI] [PubMed] [Google Scholar]
- 21.Gu X, Sun S, Gao XS, Xiong W, Qin S, Qi X, Ma M, Li X, Zhou D, Wang W, Yu H. Prognostic value of platelet to lymphocyte ratio in non-small cell lung cancer: evidence from 3,430 patients. Sci Rep. 2016;6:23893. doi: 10.1038/srep23893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hu C, Chen R, Chen W, Pang W, Xue X, Zhu G, Shen X. Thrombocytosis is a significant indictor of hypercoagulability, prognosis and recurrence in gastric cancer. Exp Ther Med. 2014;8:125–132. doi: 10.3892/etm.2014.1699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sasaki K, Kawai K, Tsuno NH, Sunami E, Kitayama J. Impact of preoperative thrombocytosis on the survival of patients with primary colorectal cancer. World J Surg. 2012;36:192–200. doi: 10.1007/s00268-011-1329-7. [DOI] [PubMed] [Google Scholar]
- 24.Stone RL, Nick AM, McNeish IA, Balkwill F, Han HD, Bottsford-Miller J, Rupairmoole R, Armaiz-Pena GN, Pecot CV, Coward J, Deavers MT, Vasquez HG, Urbauer D, et al. Paraneoplastic thrombocytosis in ovarian cancer. N Engl J Med. 2012;366:610–618. doi: 10.1056/NEJMoa1110352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ito K, Asano T, Yoshii H, Satoh A, Sumitomo M, Hayakawa M. Impact of thrombocytosis and C-reactive protein elevation on the prognosis for patients with renal cell carcinoma. Int J Urol. 2006;13:1365–1370. doi: 10.1111/j.1442-2042.2006.01563.x. [DOI] [PubMed] [Google Scholar]
- 26.Iwasaki A, Hamanaka W, Harnada T, Maekawa S, Enatsu S, Shirakusa T. Significance of platelet counts in patients who underwent surgical treatment for lung metastasis. Int Surg. 2007;92:103–109. [PubMed] [Google Scholar]
- 27.Ishizuka M, Nagata H, Takagi K, Iwasaki Y, Kubota K. Preoperative thrombocytosis is associated with survival after surgery for colorectal cancer. J Surg Oncol. 2012;106:887–891. doi: 10.1002/jso.23163. [DOI] [PubMed] [Google Scholar]
- 28.Kawai K, Kitayama J, Tsuno NH, Sunami E, Watanabe T. Thrombocytosis before pre-operative chemoradiotherapy predicts poor response and shorter local recurrence-free survival in rectal cancer. Int J Colorectal Dis. 2013;28:527–535. doi: 10.1007/s00384-012-1594-4. [DOI] [PubMed] [Google Scholar]
- 29.Naito M, Yamamoto T, Shimamoto C, Miwa Y. Retrospective Analysis of the Risk Factors for Grade IV Neutropenia in Oesophageal Cancer Patients Treated with a Docetaxel, Cisplatin, and 5-Fluorouracil Regimen. Chemotherapy. 2017;62:215–224. doi: 10.1159/000464273. [DOI] [PubMed] [Google Scholar]
- 30.Mabuchi S, Okazawa M, Isohashi F, Matsuo K, Ohta Y, Suzuki O, Yoshioka Y, Enomoto T, Kamiura S, Kimura T. Radical hysterectomy with adjuvant radiotherapy versus definitive radiotherapy alone for FIGO stage IIB cervical cancer. Gynecol Oncol. 2011;123:241–247. doi: 10.1016/j.ygyno.2011.07.009. [DOI] [PubMed] [Google Scholar]
- 31.Mabuchi S, Ugaki H, Isohashi F, Yoshioka Y, Temma K, Yada-Hashimoto N, Takeda T, Yamamoto T, Yoshino K, Nakajima R, Kuragaki C, Morishige K, Enomoto T, et al. Concurrent weekly nedaplatin, external beam radiotherapy and high-dose-rate brachytherapy in patients with FIGO stage IIIb cervical cancer: a comparison with a cohort treated by radiotherapy alone. Gynecol Obstet Invest. 2010;69:224–232. doi: 10.1159/000273207. [DOI] [PubMed] [Google Scholar]
- 32.Mabuchi S, Morishige K, Fujita M, Tsutsui T, Sakata M, Enomoto T, Kimura T. The activity of carboplatin and paclitaxel for recurrent cervical cancer after definitive radiotherapy. Gynecol Oncol. 2009;113:200–204. doi: 10.1016/j.ygyno.2009.02.008. [DOI] [PubMed] [Google Scholar]
- 33.Hisamatsu T, Mabuchi S, Yoshino K, Fujita M, Enomoto T, Hamasaki T, Kimura T. Prediction of progression-free survival and response to paclitaxel plus carboplatin in patients with recurrent or advanced cervical cancer. Int J Gynecol Cancer. 2012;22:623–629. doi: 10.1097/IGC.0b013e3182473277. [DOI] [PubMed] [Google Scholar]
- 34.Mabuchi S, Isohashi F, Yoshioka Y, Temma K, Takeda T, Yamamoto T, Enomoto T, Morishige K, Inoue T, Kimura T. Prognostic factors for survival in patients with recurrent cervical cancer previously treated with radiotherapy. Int J Gynecol Cancer. 2010;20:834–840. doi: 10.1111/IGC.0b013e3181dcadd1. [DOI] [PubMed] [Google Scholar]
- 35.Youden WJ. Index for rating diagnostic tests. Cancer. 1950;3:32–35. doi: 10.1002/1097-0142(1950)3:1<32::aid-cncr2820030106>3.0.co;2-3. [DOI] [PubMed] [Google Scholar]
- 36.Heagerty PJ, Lumley T, Pepe MS. Time-dependent ROC curves for censored survival data and a diagnostic marker. Biometrics. 2000;56:337–344. doi: 10.1111/j.0006-341x.2000.00337.x. [DOI] [PubMed] [Google Scholar]
- 37.DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44:837–845. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.