

Abstract
Background
Inflammation plays an important role in the initiation and progression of acute kidney injury (AKI). However, evidence regarding the prognostic effect of the platelet-to-lymphocyte ratio (PLR), a novel systemic inflammation marker, among patients with AKI is scarce. In this study, we investigated the value of the PLR in predicting the outcomes of critically ill patients with AKI.
Methods
Patient data were extracted from the Multiparameter Intelligent Monitoring in Intensive Care Database III version 1.3. PLR cutoff values were determined using smooth curve fitting or quintiles and were used to categorize the subjects into groups. The clinical outcomes were 30-day and 90-day mortality in the intensive care unit (ICU). Cox proportional hazards models were used to evaluate the association between the PLR and survival.
Results
A total of 10,859 ICU patients with AKI were enrolled. A total of 2277 thirty-day and 3112 ninety-day deaths occurred. A U-shaped relationship was observed between the PLR and both 90-day and 30-day mortality, with the lowest risk being at values ranging from 90 to 311. The adjusted HR (95% CI) values for 90-day mortality given risk values < 90 and > 311 were 1.25 (1.12–1.39) and 1.19 (1.08–1.31), respectively. Similar trends were observed for 30-day mortality or when quintiles were used to group patients according to the PLR. Statistically significant interactions were found between the PLR and both age and heart rate. Younger patients (aged < 65 years) and those with more rapid heart rates (≥89.4 beats per minute) tended to have poorer prognoses only when the PLR was < 90, whereas older patients (aged ≥ 65 years) and those with slower heart rates (<89.4 beats per minute) had higher risk only when the PLR was > 311 (P < 0.001 for age and P < 0.001 for heart rate).
Conclusions
The preoperative PLR was associated in a U-shaped pattern with survival among patients with AKI. The PLR appears to be a novel, independent prognostic marker of outcomes in critically ill patients with AKI.
Keywords: Platelet-to-lymphocyte ratio, Acute kidney injury, Prognosis, Intensive care unit
Background
More than 5 million patients are admitted to intensive care units (ICUs) each year in America [1, 2], and 6–24% of these patients have acute kidney injury (AKI) [3]. In the presence of AKI, patient mortality increases to as high as 60–70%, especially within 1 year after ICU admission [4–6]. Considering the high incidence of AKI in the ICU and its poor prognosis, an increasing number of observational studies over the past 2 decades have been devoted to identifying the clinical predictors of mortality in AKI.
Systemic inflammation is an integral part of disease progression in critical illness and is commonly associated with sepsis, leading to an increased risk of mortality [7, 8]. Inflammation plays an important role in the initiation and progression of AKI [9–11], and morphological and/or functional changes in vascular endothelial cells and/or in the tubular epithelium are observed in patients with AKI. Leukocytes, including lymphocytes, infiltrate the injured kidneys and the entire body via the circulatory system and induce the generation of inflammatory mediators such as cytokines and chemokines, which damage the kidney and other organs [12]. The antithrombotic effects of platelets can evolve into atherogenesis via the secretion of proinflammatory cytokines [13], whereas the binding of platelets to endothelial cells can trigger leukocyte transmigration and adhesion, especially in the presence of shear stress [14]. The platelet-to-lymphocyte ratio (PLR) has been introduced as a potential marker of inflammation in cardiovascular disease (CVD) and tumors, which are also inflammation-related diseases [15–18]. A positive monotonic association between a high PLR and a poor prognosis for these diseases has been reported [15–18]. On the basis of the results of these studies, it is reasonable to speculate that the PLR might affect the prognosis of AKI. However, to the best of our knowledge, no epidemiological study to date has explored the prognostic effect of the PLR in patients with AKI.
Methods
Data source
This study was based on the publicly and freely available database known as the Multiparameter Intelligent Monitoring in Intensive Care Database III version 1.3 (MIMIC-III v1.3). This database comprises de-identified health-related data associated with over 40,000 patients treated in a variety of critical care units at Beth Israel Deaconess Medical Center (Boston, MA, USA) between 2001 and 2012 [15]. To apply for permission to access the database, researchers must complete the National Institutes of Health’s web-based course known as Protecting Human Research Participants (certification number 1605699).
The establishment of this database was approved by the institutional review boards of Massachusetts Institute of Technology (MIT, Cambridge, MA, USA) and Beth Israel Deaconess Medical Center. All included patients were de-identified to protect their privacy.
Population selection criteria
A total of 58,976 ICU admissions were recorded in the MIMIC-III database. Eligible patients were those who were older than 18 years of age at first admission and who stayed in the hospital > 2 days. Patients were excluded from our study if (1) > 5% of their individual data were missing and (2) outliers were present. Outliers were defined as values exceeding the mean ± 3 times the SD.
The occurrence of AKI was determined on the basis of Kidney Disease: Improving Global Outcomes (KDIGO) classification [19], which specifies that serum creatinine (SCr) changes ≥ 1.5 times baseline must have occurred within the prior 7 days; a 0.3 mg/dl increase in SCr must have occurred within a 48-h period; and urine output must be < 0.5 ml/kg/h per 6 h. Stage 1 is defined as an increase in SCr to a level ≥ 1.5 times baseline or 0.3 mg/dl or urine output < 0.5 ml/kg/h per 6 h. Stage 2 is defined as an increase in SCr to a level ≥ 2.0 times baseline or urine output < 0.5 ml/kg/h per 12 h. Stage 3 is defined as an increase in SCr to a level ≥ 3.0 times baseline, an increase in SCr to a level ≥ 4.0 mg/dl, the initiation of renal replacement therapy (RRT), or urine output < 0.5 ml/kg/h per 12 h. Urine output was observed for the first 24 h after ICU admission. For patients who did not have an available SCr value prior to hospitalization, we followed the recommendation of the International Club of Ascites and used the first measured value during hospitalization as the baseline SCr [20].
Date extraction
Patient data were exacted from MIMIC-III using Structured Query Language (SQL) with MySQL tools (version 5.6.24). The extracted data, including patient identifiers, demographic parameters, clinical parameters, laboratory parameters, and scoring systems, were collected from 2001 to 2012 at Beth Israel Deaconess Medical Center. Records containing baseline characteristics were extracted within the first 24 h after patient admission.
Laboratory measurements included platelets, white blood cells, lymphocytes, neutrophils, SCr levels, blood urea nitrogen (BUN) levels, serum potassium levels, serum sodium levels, serum pH, partial pressure of carbon dioxide, partial pressure of oxygen (PO2), serum glucose levels, and urine output. The PLR was defined as the ratio of the absolute platelet count to the absolute lymphocyte count.
Severity-of-illness scores, including the Simplified Acute Physiology Score II (SAPS II), Sequential Organ Failure Assessment (SOFA) score, and Glasgow Coma Scale (GCS) score, were recorded and calculated for each patient. In addition, the Elixhauser comorbidity score was used as a comorbidity estimate. Three other standard scoring systems were evaluated, enabling a comparison with our SAPS II score with glucose variability parameters (SOFA score, and Elixhauser comorbidity score). All scores were calculated using physiological measurements and clinical information according to published recommendations and accepted formulae.
The start date for follow-up was the date of the patient’s admission. The date of death was obtained from Social Security Death Index records from the U.S. government. All patients were followed for at least 3 months. The outcomes of our study were defined as 30-day and 90-day mortality.
Statistical analysis and modeling strategy
Baseline characteristics were grouped by PLR cutoffs and are presented as frequency (percent) for categorical data and as mean (SD) or IQR for continuous data. Comparisons between groups were made using the chi-square test for categorical variables and analysis of variance or the Kruskal-Wallis test for continuous variables. Survival curves were generated using the Kaplan-Meier method and compared using the log-rank test. Cox proportional hazards models were used to test the associations between 90-day mortality (primary outcome) and baseline covariates, with results presented as HRs with 95% CIs. We also analyzed associations between the PLR and 30-day mortality. To determine whether the PLR was independently associated with endpoints, we performed multivariable analysis using a forward selection modeling process.
For each endpoint, two multivariate models were constructed on the basis of PLR group inclusion according to quintiles or cutoffs derived with curve-fitting methods based on 90-day mortality. The second quartile or the lower-limit group was treated as the reference group. In model 1, covariates were adjusted only for age and sex; in model 2, we further adjusted for PO2, ethnicity, GCS score, vasopressin use, ventilator use, systolic blood pressure (SBP), cardiac arrhythmias, valvular disease, pulmonary circulation, chronic pulmonary disease, liver disease, lymphoma, solid tumors, deficiency anemia, heart rate, SBP, potassium, SCr, urine output, BUN, and ph. We conducted stratification analyses to examine whether the effect of the PLR differed across various subgroups classified by AKI stage, RRT use, age, sex, ethnicity, PO2, GCS, heart rate, SBP, potassium, SCr, urine output, BUN, vasopressin use, ventilator use, comorbidities (i.e., cardiac arrhythmias, valvular disease, pulmonary circulation, chronic pulmonary disease, liver disease, lymphoma, metastatic cancer, solid tumors, and deficiency anemias), and cardiac surgery. Multiplicative interactions were estimated by adding interaction terms according to the likelihood ratio test. All statistical analyses were performed using the IBM SPSS Statistics version 19.0 (IBM, Armonk, NY, USA), EmpowerStats (http://www.empowerstats.cn/), and MedCalc (MedCalc Software, Ostend, Belgium) software programs. A two-tailed P value < 0.05 was considered statistically significant.
Results
Subject characteristics
Patient records from 14,354 subjects who underwent ICU treatment at Beth Israel Deaconess Medical Center were initially extracted from the MIMIC-III database. After patients who did not meet the inclusion criteria were excluded, 10,859 eligible subjects were enrolled. The subjects included 5931 men and 4928 women with a mean age of 65.4 (15.8) years. Of these subjects, 6881 (63.4%) patients were recruited from the medical ICU, and 3978 (36.6%) patients were recruited from the surgical ICU.
The overall mean (SD) PLR was 285.7 (256.9). When the patients were divided on the basis of 90-day mortality according to the curve-fitting method (Fig. 1), 1708 (15.7%) were in the low-PLR group (PLR < 90), 6699 (22.6%) were in the mid-PLR group (90–311), and 2454 (22.6%) were in the high-PLR group (PLR > 311). Selected characteristic and hematologic laboratory data across PLR groupings are provided in Table 1. Participants with higher calibrated PLRs (PLR > 311) were more likely to be elderly, female, and white and to report a history of chronic pulmonary disease, metastatic cancer, solid tumors, and iron-deficiency anemia; they also had higher levels of serum potassium, BUN, white blood cells, neutrophils, platelets, urine output, and eGFR and were more likely to use RRT than those with lower PLRs (PLR < 90).
Fig. 1.
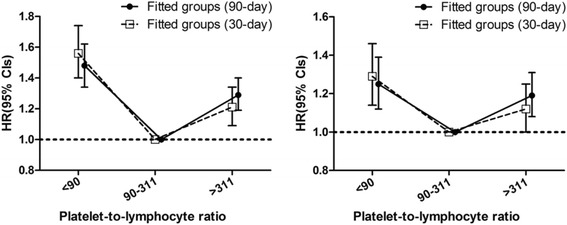
HRs (95% CIs) for all-cause mortality across fitted groups of platelet-to-lymphocyte ratios (fitted groups: model 1 and model 2)
Table 1.
Baseline characteristics of the study population
| Characteristics | Platelet-to-lymphocyte ratio | P value | ||
|---|---|---|---|---|
| <90 | 90–311 | ≥312 | ||
| Platelet-to-lymphocyte ratio | 59.1 | 182.6 | 456.8 | <0.001 |
| Clinical parameters, n (%) | 1708 | 6699 | 2454 | |
| Age, years | 62.3 (15.9) | 65.4 (15.9) | 65.7 (15.5) | <0.001 |
| Sex, n (%) | <0.001 | |||
| Male | 992 (58.1) | 3679 (54.9) | 1260 (51.3) | |
| Female | 716 (41.9) | 3018 (45.1) | 1194 (48.7) | |
| Ethnicity, n (%) | <0.001 | |||
| White | 1095 (64.10) | 4636 (69.2) | 1833 (74.7) | |
| Black | 203 (11.9) | 805 (12.0) | 208 (8.5) | |
| Other | 410 (24.0) | 1256 (18.8) | 413 (16.8) | |
| SBP, mmHg | 120.6 (26.4) | 123.3 (26.3) | 121.9 (26.0) | <0.001 |
| DBP, mmHg | 61.5 (18.6) | 62.2 (18.1) | 61.1 (17.3) | 0.021 |
| Heart rate, beats/minute | 89.9 (20.9) | 88.6 (19.9) | 91.3 (20.0) | <0.001 |
| Vasopressin use, n (%) | <0.001 | |||
| Yes | 844 (49.4) | 2728 (40.7) | 1047 (42.7) | |
| No | 864 (50.6) | 3969 (59.3) | 1407 (57.3) | |
| Ventilator use, n (%) | <0.001 | |||
| Yes | 1063 (62.2) | 3528 (52.7) | 1316 (53.6) | |
| No | 645 (37.8) | 3169 (47.3) | 1138 (6.4) | |
| Comorbidities | ||||
| Cardiac arrhythmias, n (%) | <0.001 | |||
| Yes | 375 (22.0) | 1944 (29.0) | 696 (28.4) | |
| No | 1333 (78.0) | 4753 (71.0) | 1758 (71.6) | |
| Valvular disease, n (%) | 0.051 | |||
| Yes | 177 (15.7) | 740 (11.0) | 228 (9.3) | |
| No | 1531 (89.6) | 5957 (89.0) | 2226 (90.7) | |
| Pulmonary circulation, n (%) | 0.599 | |||
| Yes | 97 (5.7) | 415 (6.2) | 158 (6.4) | |
| No | 1611 (94.3) | 6282 (93.8) | 2296 (93.6) | |
| Chronic pulmonary disease, n (%) | <0.001 | |||
| Yes | 255 (14.9) | 1343 (20.1) | 558 (22.7) | |
| No | 1453 (85.1) | 5354 (79.9) | 1896 (77.3) | |
| Liver disease, n (%) | <0.001 | |||
| Yes | 300 (17.6) | 492 (7.3) | 108 (4.4) | |
| No | 1408 (82.4) | 6205 (92.7) | 2346 (95.6) | |
| Lymphoma, n (%) | <0.001 | |||
| Yes | 59 (3.5) | 123 (1.8) | 49 (2.0) | |
| No | 1649 (96.5) | 6574 (98.2) | 2405 (98.0) | |
| Metastatic cancer, n (%) | <0.001 | |||
| Yes | 62 (3.6) | 280 (4.2) | 203 (8.3) | |
| No | 1646 (96.4) | 6417 (95.8) | 2251 (91.7) | |
| Solid tumor, n (%) | <0.001 | |||
| Yes | 93 (5.4) | 411 (6.1) | 248 (10.1) | |
| No | 1615 (94.6) | 6286 (93.9) | 2206 (89.9) | |
| Deficiency anemias, n (%) | 0.046 | |||
| Yes | 246 (14.4) | 1014 (15.1) | 416 (17.0) | |
| No | 1462 (85.6) | 5683 (84.9) | 2038 (83.0) | |
| Laboratory parameters | ||||
| PO2, mmHg | 118.0 (74.0–279.0) | 113.0 (75.0–237.0) | 107.0 (72.3–201.0) | <0.001 |
| PCO2, mmHg | 39.0 (34.0–46.0) | 40.0 (34.0–47.0) | 40.0 (34.0–47.0) | 0.036 |
| Serum potassium, mmol/L | 4.32 (0.89) | 4.39 (0.91) | 4.44 (0.95) | <0.001 |
| BUN, mg/dl | 30.0 (20.0–47.0) | 31.0 (21.0–49.0) | 33.0 (21.0–52.0) | <0.001 |
| Serum bicarbonate, mmol/L | 23.0 (19.0–26.0) | 24.0 (20.0–27.0) | 23.0 (20.0–27.0) | <0.001 |
| Serum pH | 7.31 (0.14) | 7.32 (0.12) | 7.32 (0.12) | <0.001 |
| White blood cell count, 109/L | 11.0 (7.4–16.5) | 10.6 (7.6–15.1) | 11.8 (8.1–16.5) | <0.001 |
| Neutrophil count, n (%) | 65.9 (18.2) | 77.6 (11.4) | 83.5 (12.9) | <0.001 |
| Lymphocyte count, n (%) | 19.0 (12.0–28.0) | 12.0 (8.0–17.7) | 5.9 (3.8– 8.8) | <0.001 |
| Platelet count, 109/L | 122.0 (67.0–182.) | 220.0 (164.0–287.0) | 285.0 (206.0–383.8) | <0.001 |
| Scoring systems | ||||
| GCS | 14.0 (6.0–15.0) | 15.0 (8.0–15.0) | 15.0(9.0–15.0) | <0.001 |
| SOFA | 7.0 (5.0–10.0) | 5.0 (3.0– 8.0) | 5.0 (3.0– 8.0) | <0.001 |
| Renal function | ||||
| Serum creatinine, mg/dl | 1.50 (1.10–2.40) | 1.60 (1.20–2.40) | 1.60 (1.20–2.50) | 0.340 |
| Urine output, ml/24 h | 1050 (372–2311) | 1050 (395–2325) | 900 (345–2095) | 0.046 |
| eGFR, ml/min/1.73 m2 | 0.88 (0.76–0.94) | 0.87 (0.77–0.95) | 0.84 (0.76–0.94) | <0.001 |
| eGFR change | 2.02 (1.17–4.27) | 1.15 (1.86–3.76) | 2.03 (1.25–4.16) | <0.001 |
| KDIGO stage, n (%) | 0.084 | |||
| Stage 1 | 1081 (63.4) | 4467(66.7) | 1589 (64.8) | |
| Stage 2 | 407 (23.9) | 1456 (21.8) | 573 (23.3) | |
| Stage 3 | 218 (12.8) | 776 (11.6) | 292 (11.9) | |
| Renal replacement therapy | 0.008 | |||
| Yes | 71 (4.2) | 189 (2.8) | 66 (2.7) | |
| No | 1635 (95.8) | 6510 (97.2) | 2388 (97.3) | |
Abbreviations: BUN Blood urea nitrogen, DBP Diastolic blood pressure, eGFR, Estimated glomerular filtration rate; GCS Glasgow Coma Scale, KDIGO Kidney Disease: Improving Global Outcomes, PCO 2 Partial pressure of carbon dioxide, PO 2 Partial pressure of oxygen, SBP Systolic blood pressure, SOFA Sequential Organ Failure Assessment
Normally distributed data are presented as the mean (SD) (analysis of variance); non-normally distributed data are presented as median (IQR) (nonparametric Wilcoxon test); and categorical variables are presented as n (%) (chi-square test)
Association between platelet-to-lymphocyte ratio and 30-day and 90-day outcomes
A total of 2277 thirty-day and 3112 ninety-day deaths occurred during the follow-up period. A U-shaped relationship was observed between the PLR and 90-day mortality, and the patients in the mid-PLR group (90–311) had the lowest 30-day mortality rate when compared with rates in the PLR < 90 and PLR > 311 groups (both P < 0.001). The adjusted HRs (95% CIs) for PLRs < 90 and > 311 were 1.25 (1.12–1.39) and 1.19 (1.08–1.31), respectively. A similar trend was observed for 30-day mortality, and the risk was less evident with higher PLRs (P = 0.047 for PLR > 311). Following the stratification of PLRs into quintiles and using the second quintile (PLR 101.2–155.6) as a reference, both extremely low (<101.2) and extremely high (>330.2) PLRs were associated with an increased risk of 90-day mortality. For 30-day mortality, the lowest PLRs (<101.2, P = 0.001) were associated with an increased risk, whereas marginally increased risk was associated with extremely high PLRs (>330.2, P = 0.088) after adjustment for potential confounders (Figs. 1 and 2 and Table 2).
Fig. 2.
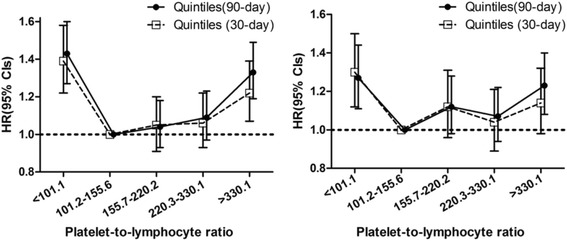
HRs (95% CIs) for all-cause mortality across quintile groups of platelet-to-lymphocyte ratios (quintile groups: model 1 and model 2)
Table 2.
HRs (95% CIs) for all-cause mortality across groups of platelet-to-lymphocyte ratios
| Platelet-to-lymphocyte ratio | No. of patients/deaths | Model 1 | Model 2 | ||
|---|---|---|---|---|---|
| HR (95% CIs) | P value | HR (95% CIs) | P value | ||
| 90-Day all-cause mortality | |||||
| Fitted groups | |||||
| < 90 | 1708/573 | 1.48 (1.34–1.62) | <0.001 | 1.25 (1.12–1.39) | <0.001 |
| 90–311 | 6697/1745 | 1.00 | 1.00 | ||
| ≥ 312 | 2454/794 | 1.29 (1.19–1.40) | <0.001 | 1.19 (1.08–1.31) | <0.001 |
| Quintiles | |||||
| < 101.1 | 2172/694 | 1.43 (1.27–1.60) | <0.001 | 1.27 (1.11–1.44) | <0.001 |
| 101.2–155.6 | 2172/545 | 1.00 | 1.00 | ||
| 155.7–220.2 | 2173/571 | 1.04 (0.93–1.18) | 0.477 | 1.12 (0.98–1.28) | 0.093 |
| 220.3–330.1 | 2171/602 | 1.09 (0.97–1.23) | 0.152 | 1.07 (0.94–1.22) | 0.296 |
| ≥ 330.2 | 2171/700 | 1.33 (1.19–1.49) | <0.001 | 1.23 (1.08–1.40) | 0.002 |
| 30-Day all-cause mortality | |||||
| Fitted groups | |||||
| < 90 | 1708/448 | 1.56 (1.40–1.74) | <0.001 | 1.29 (1.14–1.46) | <0.001 |
| 90–311 | 6697/1273 | 1.00 | 1.00 | ||
| ≥ 312 | 2454/556 | 1.21 (1.09–1.34) | <0.001 | 1.12 (1.00–1.25) | 0.047 |
| P trend | |||||
| Quintiles | |||||
| < 101.1 | 2172/532 | 1.39 (1.22–1.58) | <0.001 | 1.30 (1.12–1.50) | 0.001 |
| 101.2–155.6 | 2172/406 | 1.00 | |||
| 155.7–220.2 | 2173/423 | 1.05 (0.91–1.20) | 0.516 | 1.12 (0.96–1.31) | 0.141 |
| 220.3–330.1 | 2171/432 | 1.06 (0.93–1.22) | 0.388 | 1.04 (0.89–1.21) | 0.649 |
| ≥ 330.2 | 2171/484 | 1.22 (1.07–1.39) | 0.003 | 1.14 (0.98–1.32) | 0.088 |
Models 1 and 2 were derived from Cox proportional hazards regression models: model 1 covariates were adjusted for age and sex; model 2 covariates were adjusted for age, sex, partial pressure of oxygen, ethnicity, Glasgow Coma Scale score, vasopressin use, ventilator use, systolic blood pressure, cardiac arrhythmias, valvular disease, pulmonary circulation, chronic pulmonary disease, liver disease, lymphoma, solid tumor, deficiency anemias, heart rate, potassium creatinine, urine output, blood urea nitrogen, and pH
Subgroup analyses
In the subgroup analyses, the association between the PLR and the risk of 90-day mortality was similar for most strata (P = 0.083–0.983) (Table 3). Significant interactions were observed only for age (P < 0.001). Patients younger than 65 years of age had a significantly higher risk of 90-day mortality for a PLR < 90 (HR 1.37, 95% CI 1.16–1.62, P < 0.001), whereas only older patients (≥65 years) showed an increased risk for a PLR > 311 (HR 1.25 95% CI 1.22–1.40, P < 0.001). Similarly, patients with a heart rate < 89.4 beats per minute had a significantly higher risk of 90-day mortality with a PLR > 311 (HR 1.29, 95% CI 1.22–1.48, P < 0.001), whereas patients with a heart rate ≥ 89.4 beats per minute (aged ≥ 65 years) showed an increased risk only with a PLR < 90 (HR 1.39, 95% CI 1.20–1.61, P < 0.001).
Table 3.
Subgroup analysis of the associations between 90-day all-cause mortality and the platelet-to-lymphocyte ratio
| No. of patients/deaths | Platelet-to-lymphocyte ratio | ||||
|---|---|---|---|---|---|
| <90 | 90–311 | ≥312 | P for interaction | ||
| AKI stage | 0.301 | ||||
| Stage 1 | 7137/1740 | 1.23 (1.05–1.43)a | 1.00 | 1.22 (1.08–1.38)a | |
| Stage 2 | 2436/1474 | 1.23 (1.02–1.50)b | 1.00 | 1.09 (0.92–1.30) | |
| Stage 3 | 1286/876 | 1.38 (1.04–1.82) | 1.00 | 1.30 (0.99–1.72) | |
| Renal replacement therapy | 0.906 | ||||
| Yes | 326/177 | 1.45 (0.97–2.17) | 1.00 | 1.31 (0.86–2.01) | |
| No | 10,533/2935 | 1.24 (1.11–1.39)c | 1.00 | 1.17 (1.06–1.29)a | |
| Age, years | <0.001 | ||||
| < 65 | 4686/1000 | 1.37 (1.16–1.62)c | 1.00 | 1.06 (0.88–1.27) | |
| ≥ 65 | 6035/2054 | 1.09 (0.94–1.27) | 1.00 | 1.25 (1.12–1.40)c | |
| Sex | 0.386 | ||||
| Male | 5931/1741 | 1.22 (1.06–1.41)a | 1.00 | 1.24 (1.09–1.41)c | |
| Female | 4928/1371 | 1.26 (1.06–1.49)a | 1.00 | 1.13 (0.98–1.31) | |
| Ethnicity | 0.409 | ||||
| White | 7564/2134 | 1.25 (1.09–1.44)c | 1.00 | 1.19 (1.06–1.33)a | |
| Black | 1216/254 | 1.24 (0.84–1.81) | 1.00 | 1.33 (0.92–1.93) | |
| Other | 2079/724 | 1.21 (0.98–1.49) | 1.00 | 1.11 (0.90–1.36) | |
| PO2, mmHg | 0.310 | ||||
| < 167.3 | 6433/2108 | 1.29 (1.14–1.47)c | 1.00 | 1.21 (1.08–1.35)a | |
| ≥1 67.3 | 3502/870 | 1.16 (0.95–1.42) | 1.00 | 1.21 (1.00–1.47) | |
| GCS score | 0.938 | ||||
| < 11.4 | 4101/1387 | 1.25 (1.07–1.46)a | 1.00 | 1.21 (1.05–1.39) | |
| ≥ 11.4 | 6499/1663 | 1.24 (1.06–1.45)a | 1.00 | 1.18 (1.04–1.35)b | |
| Heart rate, beats/min | 0.001 | ||||
| < 89.4 | 5811/1503 | 1.08 (0.92–1.28) | 1.00 | 1.29 (1.12–1.48)c | |
| ≥ 89.4 | 4880/1575 | 1.39 (1.20–1.61)c | 1.00 | 1.10 (0.96–1.26) | |
| SBP, mmHg | 0.187 | ||||
| < 122.6 | 5596/1885 | 1.28 (1.12–1.46)c | 1.00 | 1.15 (1.02–1.30)b | |
| ≥ 122.6 | 4800/1070 | 1.18 (0.97–1.43) | 1.00 | 1.26 (1.07–1.47)a | |
| Potassium, mmol/L | 0.633 | ||||
| < 4.39 | 6158/1667 | 1.24 (1.07–1.44)a | 1.00 | 1.19 (1.04–1.36)a | |
| ≥ 4.39 | 4692/1443 | 1.24 (1.05–1.47)b | 1.00 | 1.22 (1.06–1.40)a | |
| Creatinine, mg/dl | 0.816 | ||||
| < 2.28 | 7809/2128 | 1.29 (1.13–1.47)c | 1.00 | 1.21 (1.08–1.35)a | |
| ≥ 2.28 | 3048/982 | 1.17 (0.96–1.44) | 1.00 | 1.15 (0.97–1.37) | |
| Urine output, ml/24 h | 0.083 | ||||
| < 1807 | 7057/2309 | 1.28 (1.13–1.45)c | 1.00 | 1.13 (1.02–1.26)b | |
| ≥ 1807 | 3300/641 | 1.17 (0.92–1.47) | 1.00 | 1.38 (1.12–1.69)a | |
| BUN, mg/dl | 0.615 | ||||
| < 39.2 | 6887/1737 | 1.30 (1.13–1.50)c | 1.00 | 1.23 (1.08–1.40)a | |
| ≥ 39.2 | 3972/1375 | 1.19 (1.00–1.41) | 1.00 | 1.17 (1.01–1.35)b | |
| Vasopressin use | 0.549 | ||||
| Yes | 4619/1784 | 1.29 (1.13–1.48)c | 1.00 | 1.24 (1.09–1.40)a | |
| No | 6240/1328 | 1.17 (0.96–1.42) | 1.00 | 1.11 (0.95–1.29) | |
| Ventilator use | 0.216 | ||||
| Yes | 5907/2098 | 1.26 (1.12–1.43)c | 1.00 | 1.17 (1.05–1.31)a | |
| No | 4952/1014 | 1.21 (0.95–1.54) | 1.00 | 1.21 (1.01–1.45)b | |
| Cardiac arrhythmias | 0.671 | ||||
| Yes | 3015/1040 | 1.13 (0.91–1.39) | 1.00 | 1.19 (1.02–1.40)b | |
| No | 7844/2072 | 1.29 (1.13–1.47)c | 1.00 | 1.19 (1.06–1.34)a | |
| Valvular disease | 0.986 | ||||
| Yes | 1145/339 | 0.75 (0.51–1.10) | 1.00 | 1.37 (1.01–1.87)b | |
| No | 9714/2773 | 1.31 (1.17–1.47)c | 1.00 | 1.18 (1.07–1.31)a | |
| Pulmonary circulation | 0.320 | ||||
| Yes | 670/199 | 1.20 (0.76–1.89) | 1.00 | 1.12 (0.76–1.63) | |
| No | 10,189/2913 | 1.34 (1.11–1.39)c | 1.00 | 1.18 (1.07–1.31)a | |
| Chronic pulmonary disease | 0.289 | ||||
| Yes | 2156/638 | 0.97 (0.72–1.29) | 1.00 | 1.14 (0.94–1.38) | |
| No | 8703/2474 | 1.29 (1.15–1.46)c | 1.00 | 1.21 (1.08–1.34)a | |
| Liver disease | 0.919 | ||||
| Yes | 900/410 | 1.13 (0.89–1.45) | 1.00 | 1.08 (0.78–1.50) | |
| No | 9959/2702 | 1.26 (1.12–1.42)c | 1.00 | 1.21 (1.09–1.33)c | |
| Lymphoma | 0.101 | ||||
| Yes | 231/102 | 1.66 (0.94–2.93) | 1.00 | 1.79 (0.97–3.30) | |
| No | 10,628/3010 | 1.23 (1.10–1.37)c | 1.00 | 1.18 (1.07–1.30)a | |
| Metastatic cancer | 0.901 | ||||
| Yes | 545/317 | 0.97 (0.63–1.49) | 1.00 | 1.11 (0.84–1.45) | |
| No | 10,314/2795 | 1.26 (1.12–1.41)c | 1.00 | 1.15 (1.04–1.27)a | |
| Solid tumor | 0.605 | ||||
| Yes | 752/333 | 1.22 (0.82–1.81) | 1.00 | 1.21 (0.91–1.60) | |
| No | 10,107/2779 | 1.24 (1.10–1.38)c | 1.00 | 1.18 (1.07–1.31)a | |
| Deficiency anemias | 0.852 | ||||
| Yes | 1676/378 | 1.15 (0.91–1.46) | 1.00 | 1.12 (0.77–1.53) | |
| No | 9183/2734 | 1.25 (1.10–1.39) | 1.00 | 1.20 (1.07–1.33) | |
| Cardiac surgery | 0.207 | ||||
| Yes | 1864/635 | 1.16 (0.92–1.45) | 1.00 | 1.24 (1.01–1.52)b | |
| No | 8995/2477 | 1.30 (1.14–1.47)c | 1.00 | 1.16 (1.04–1.29)a | |
Abbreviations: AKI Acute kidney injury, BUN Blood urea nitrogen, GCS Glasgow Coma Scale, PO 2 Partial pressure of oxygen, SBP Systolic blood pressure
a P < 0.01
b P < 0.05
c P < 0.001
HRs (95% CIs) were derived from Cox proportional hazards regression models. Covariates were adjusted as in model 2 (Table 2)
Discussion
In this study, we observed a U-shaped relationship between the PLR and 30-day and 90-day mortality, and both low and high PLRs were associated with increased all-cause mortality. Proctor et al. [21] investigated the correlation between the PLR and overall survival in a large-scale cohort of 8759 patients with cancer. In contrast to our results, their study showed a positive correlation between the PLR and mortality when using a similar PLR cutoff (PLR < 150, HR 1; PLR 150–300, HR 1.19; P < 0.001; PLR > 300, HR 1.71, P < 0.001). Yaprak et al. [22] recently evaluated the correlation between the PLR and mortality in a small cohort of patients with end-stage renal disease (ESRD) and demonstrated that the PLR could independently predict all-cause mortality in this population. A main reason for this difference is the insufficient number of patients with low PLRs. However, our study addresses this limitation. In the Framingham Heart Study, blood cell composition was treated as a prognostic factor for CVD, and the association between hematocrit and CVD mortality showed a U-shaped association in both men and women [23].
Both AKI and chronic kidney disease (CKD) are associated with local and systemic inflammation [24]. Researchers in many observational studies have described high circulating levels of inflammatory mediators and adverse outcomes for these conditions. These inflammatory mediators include blood cells, components of endothelial cells, platelets, lymphocytes, macrophages, mast cells, and fibroblasts. The PLR has been investigated as a new inflammatory marker for predicting major adverse events associated with CVD [16]. In a study of 2563 patients, Velibey et al. [25] demonstrated that increased PLRs are independently associated with a greater risk of contrast-induced AKI in patients undergoing primary percutaneous coronary intervention. A recent study showed that a high PLR is related to the presence of coronary artery disease and is correlated with C-reactive protein and fibrinogen levels [26]. High PLRs in patients with ESRD were also associated with high levels of inflammation. Balta et al. [27] showed that inflammation is better predicted by the PLR than by the neutrophil-to-lymphocyte ratio in ESRD. On the basis of the association between PLR-related inflammation and disease severity, we speculated that excessively high PLRs could predict the same poor outcomes as other inflammation biomarkers in AKI populations.
In a population-based cohort study comparing the mortality rates of 605 ICU patients with those of patients with acute renal failure (ARF), Mehta et al. [28] found that a platelet count < 20,000/mm3 is a criterion for hematologic failure and that the risk of mortality was more than threefold higher among patients who had hematologic failure than among control patients with normal platelet levels (OR 3.39, 95% CI 2.08–5.52). Using data from the Program to Improve Care in Acute Renal Disease, a multicenter observational study of ARF, Chertow et al. [29] examined the correlates of mortality in 618 ICU patients with ARF. Thrombocytopenia was associated with mortality at the time of consultation. In addition, among 512 ICU patients requiring acute dialysis, a platelet count < 50,000/mm3 was a potential risk factor for mortality in multivariate analysis [30]. Thrombocytopenia is common among critically ill patients and is often associated with poor outcomes [31–34]. The mechanisms underlying thrombocytopenia include either reduced platelet production or excessive platelet destruction related to an underlying illness and therapeutic interventions [35]. Taken together, these findings show that low platelet counts could result from a low PLR in patients with AKI and could lead to high mortality, thus helping to explain our observation of a U-shaped relationship between the PLR and mortality.
Although AKI in the ICU is associated with high mortality, other factors appear to contribute to poor outcomes. Potential factors that may affect the outcome of AKI include blood pressure [36], renal function [37], urine output [36], and other clinical parameters (i.e., SCr, BUN, and pH [38]), as well as comorbidities (e.g., cardiac disease [38]). In the present study, when patients were stratified according to potential confounders, no significant interactions were observed for sex, ethnicity, PO2, GCS, SBP, potassium, SCr, urine output, BUN, vasopressin use, or ventilator use. Although possible interactions between all-cause mortality and both age and heart rate were observed, there was no heterogeneity of clinical factors among those effects and the PLR. However, little is known about the mechanism underlying the interaction between age and the PLR. Recently, in a multicenter cross-sectional study of a healthy Indian population, Sairam et al. [39] found lower levels of platelets in elderly people. Kweon et al. [40] investigated median PLRs in a healthy Korean population and suggested that the PLR cutoff values for disease evaluation should be established separately according to age. Therefore, we should consider age when evaluating the relationship between the PLR and mortality among critically ill patients with AKI.
The limitations of this study should be acknowledged. First, it was a single-center retrospective analysis, and different conclusions could be reached when using patient records from other centers. Therefore, subject selection bias cannot be ignored, suggesting that a prospective multicenter study is needed. However, the strength of the present study is its representative and ethnically diverse population. Second, because of a lack of data on kidney function prior to 3 months before patient admission, we could not assess CKD status among patients with AKI or determine the role of CKD in the association between the PLR and mortality. Third, the PLR can be measured in patients only upon admission to the ICU. A single measure of the PLR does not fully reflect inflammation, which would be better assessed by simultaneously measuring other inflammatory mediators. Fourth, these preliminary data suggest that the PLR could be a risk adjustment tool with prognostic implications for AKI. Fifth, to establish the PLR as a prognostic marker, researchers must further validate its clinical significance. The cutoff value must be established in one cohort of patients and tested in another, and the number of patients in each group needs to be considered in statistical analyses. Finally, we did not assess the modification of sepsis and shock, which both might increase patient morbidity and predict higher mortality among patients with AKI [41], on association between PLR and outcomes, owing to lack of related data.
Conclusions
We found a U-shaped relationship between the PLR and mortality in which both low and high PLRs were associated with increased overall mortality in critically ill patients with AKI. The PLR is therefore potentially useful in the clinical setting as a cost-effective and readily available biomarker. Our findings need to be confirmed by other studies, especially large prospective studies with longer follow-up.
Acknowledgements
The authors thank Fang-Fang Zeng for her excellent technical assistance with data management and the manuscript.
Funding
The medical innovation discipline of Zhejiang Province (critical care medicine, Y2015) and Wenzhou Committee of Science and Technology of China (ZS2017008) supported this work.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Declarations
This study was based on the publicly and freely available database known as the Multi Parameter Intelligent Monitoring in Intensive Care III, version 1.3 (MIMIC-III v1.3). This database comprises de-identified health-related data associated with over 40,000 patients treated in a variety of critical care units in the Beth Israel Deaconess Medical Center between 2001 and 2012. To apply for permission to access the database, researchers must complete the National Institutes of Health’s web-based course known as Protecting Human Research Participants (certification number 1605699). The establishment of this database was approved by the institutional review boards of Massachusetts Institute of Technology (Cambridge, MA, USA) and Beth Israel Deaconess Medical Center. All included patients were de-identified to protect their privacy.
Abbreviations
- AKI
Acute kidney injury
- ARF
Acute renal failure
- BUN
Blood urea nitrogen
- CKD
Chronic kidney disease
- CVD
Cardiovascular disease
- DBP
Diastolic blood pressure
- eGFR
Estimated glomerular filtration rate
- ESRD
End-stage renal disease
- GCS
Glasgow Coma Scale
- ICU
Intensive care unit
- KDIGO
Kidney Disease: Improving Global Outcomes
- MIMIC-III
Multiparameter Intelligent Monitoring in Intensive Care Database III
- PCO2
Partial pressure of carbon dioxide
- PLR
Platelet-to-lymphocyte ratio
- PO2
Partial pressure of oxygen
- RRT
Renal replacement therapy
- SAPS II
Simplified Acute Physiology Score II
- SBP
Systolic blood pressure
- SCr
Serum creatinine
- SQL
Structured Query Language
- SOFA
Sequential Organ Failure Assessment
Authors’ contributions
CFZ designed the study; collected, analyzed, and interpreted data; and drafted the manuscript. WYL collected, analyzed, and interpreted data. FFZ and HYS collected and analyzed data and drafted the manuscript. YZ drafted the manuscript and interpreted data. MHZ designed the study, drafted the manuscript, and interpreted data. JYP designed and supervised the study, obtained funding, and drafted the manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to participate
The MIMIC-III database has received ethical approval from the institutional review boards (IRBs) at Beth Israel Deaconess Medical Center and Massachusetts Institute of Technology. Because the database does not contain protected health information, a waiver of the requirement for informed consent was included in the IRB approval.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29(7):1303–10. doi: 10.1097/00003246-200107000-00002. [DOI] [PubMed] [Google Scholar]
- 2.Mayr VD, Dunser MW, Greil V, Jochberger S, Luckner G, Ulmer H, Friesenecker BE, Takala J, Hasibeder WR. Causes of death and determinants of outcome in critically ill patients. Crit Care. 2006;10(6):R154. doi: 10.1186/cc5086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, et al. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294(7):813–8. doi: 10.1001/jama.294.7.813. [DOI] [PubMed] [Google Scholar]
- 4.Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P. Acute renal failure - definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;8(4):R204. doi: 10.1186/cc2872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hofhuis JG, van Stel HF, Schrijvers AJ, Rommes JH, Spronk PE. The effect of acute kidney injury on long-term health-related quality of life: a prospective follow-up study. Crit Care. 2013;17(1):R17. doi: 10.1186/cc12491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.White LE, Hassoun HT, Bihorac A, Moore LJ, Sailors RM, McKinley BA, Valdivia A, Moore FA. Acute kidney injury is surprisingly common and a powerful predictor of mortality in surgical sepsis. J Trauma Acute Care Surg. 2013;75(3):432–8. doi: 10.1097/TA.0b013e31829de6cd. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Adrie C, Pinsky MR. The inflammatory balance in human sepsis. Intensive Care Med. 2000;26(4):364–75. doi: 10.1007/s001340051169. [DOI] [PubMed] [Google Scholar]
- 8.Pierrakos C, Vincent JL. Sepsis biomarkers: a review. Crit Care. 2010;14(1):R15. doi: 10.1186/cc8872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mami I, Tavernier Q, Bouvier N, Aboukamis R, Desbuissons G, Rabant M, Poindessous V, Laurent-Puig P, Beaune P, Tharaux PL, et al. A novel extrinsic pathway for the unfolded protein response in the kidney. J Am Soc Nephrol. 2016;27(9):2670–83. doi: 10.1681/ASN.2015060703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rabb H, Griffin MD, McKay DB, Swaminathan S, Pickkers P, Rosner MH, Kellum JA, Ronco C. Inflammation in AKI: current understanding, key questions, and knowledge gaps. J Am Soc Nephrol. 2016;27(2):371–9. doi: 10.1681/ASN.2015030261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Jansen MP, Emal D, Teske GJ, Dessing MC, Florquin S, Roelofs JJ. Release of extracellular DNA influences renal ischemia reperfusion injury by platelet activation and formation of neutrophil extracellular traps. Kidney Int. 2017;91(2):352–64. doi: 10.1016/j.kint.2016.08.006. [DOI] [PubMed] [Google Scholar]
- 12.Akcay A, Nguyen Q, Edelstein CL. Mediators of inflammation in acute kidney injury. Mediators Inflamm. 2009;2009:137072. doi: 10.1155/2009/137072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kaplan ZS, Jackson SP. The role of platelets in atherothrombosis. Hematology Am Soc Hematol Educ Program. 2011;2011:51–61. doi: 10.1182/asheducation-2011.1.51. [DOI] [PubMed] [Google Scholar]
- 14.Borissoff JI, Spronk HM, Ten CH. The hemostatic system as a modulator of atherosclerosis. N Engl J Med. 2011;364(18):1746–60. doi: 10.1056/NEJMra1011670. [DOI] [PubMed] [Google Scholar]
- 15.Sunbul M, Gerin F, Durmus E, Kivrak T, Sari I, Tigen K, Cincin A. Neutrophil to lymphocyte and platelet to lymphocyte ratio in patients with dipper versus non-dipper hypertension. Clin Exp Hypertens. 2014;36(4):217–21. doi: 10.3109/10641963.2013.804547. [DOI] [PubMed] [Google Scholar]
- 16.Azab B, Shah N, Akerman M, McGinn JJ. Value of platelet/lymphocyte ratio as a predictor of all-cause mortality after non-ST-elevation myocardial infarction. J Thromb Thrombolysis. 2012;34(3):326–34. doi: 10.1007/s11239-012-0718-6. [DOI] [PubMed] [Google Scholar]
- 17.Li X, Chen ZH, Xing YF, Wang TT, Wu DH, Wen JY, Chen J, Lin Q, Dong M, Wei L, et al. Platelet-to-lymphocyte ratio acts as a prognostic factor for patients with advanced hepatocellular carcinoma. Tumour Biol. 2015;36(4):2263–9. doi: 10.1007/s13277-014-2833-9. [DOI] [PubMed] [Google Scholar]
- 18.Tian XC, Zeng FR, Wu DH. Platelet-to-lymphocyte ratio: a prognostic factor for patients with advanced hepatocellular carcinoma? Tumour Biol. 2015;36(7):4935–6. doi: 10.1007/s13277-015-3585-x. [DOI] [PubMed] [Google Scholar]
- 19.Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C, Warnock DG, Levin A, Acute Kidney Injury Network Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Crit Care. 2007;11(2):R31. doi: 10.1186/cc5713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Angeli P, Gines P, Wong F, Bernardi M, Boyer TD, Gerbes A, Moreau R, Jalan R, Sarin SK, Piano S, et al. Diagnosis and management of acute kidney injury in patients with cirrhosis: revised consensus recommendations of the International Club of Ascites. J Hepatol. 2015;62(4):968–74. doi: 10.1016/j.jhep.2014.12.029. [DOI] [PubMed] [Google Scholar]
- 21.Proctor MJ, Morrison DS, Talwar D, Balmer SM, Fletcher CD, O’Reilly DS, Foulis AK, Horgan PG, McMillan DC. A comparison of inflammation-based prognostic scores in patients with cancer: a Glasgow Inflammation Outcome Study. Eur J Cancer. 2011;47(17):2633–41. doi: 10.1016/j.ejca.2011.03.028. [DOI] [PubMed] [Google Scholar]
- 22.Yaprak M, Turan MN, Dayanan R, Akin S, Degirmen E, Yildirim M, Turgut F. Platelet-to-lymphocyte ratio predicts mortality better than neutrophil-to-lymphocyte ratio in hemodialysis patients. Int Urol Nephrol. 2016;48(8):1343–8. doi: 10.1007/s11255-016-1301-4. [DOI] [PubMed] [Google Scholar]
- 23.Gagnon DR, Zhang TJ, Brand FN, Kannel WB. Hematocrit and the risk of cardiovascular disease—the Framingham study: a 34-year follow-up. Am Heart J. 1994;127(3):674–82. doi: 10.1016/0002-8703(94)90679-3. [DOI] [PubMed] [Google Scholar]
- 24.Doi K, Rabb H. Impact of acute kidney injury on distant organ function: recent findings and potential therapeutic targets. Kidney Int. 2016;89(3):555–64. doi: 10.1016/j.kint.2015.11.019. [DOI] [PubMed] [Google Scholar]
- 25.Velibey Y, Oz A, Tanik O, Guvenc TS, Kalenderoglu K, Gumusdag A, Akdeniz E, Bozbay M, Tekkesin AI, Guzelburc O, et al. Platelet-to-lymphocyte ratio predicts contrast-induced acute kidney injury in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Angiology. 2017;68(5):419–27. doi: 10.1177/0003319716660244. [DOI] [PubMed] [Google Scholar]
- 26.Gary T, Pichler M, Belaj K, Hafner F, Gerger A, Froehlich H, Eller P, Rief P, Hackl G, Pilger E, et al. Platelet-to-lymphocyte ratio: a novel marker for critical limb ischemia in peripheral arterial occlusive disease patients. PLoS One. 2013;8(7):e67688. doi: 10.1371/journal.pone.0067688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Balta S, Demirkol S, Kucuk U. The platelet lymphocyte ratio may be useful inflammatory indicator in clinical practice. Hemodial Int. 2013;17(4):668–9. doi: 10.1111/hdi.12058. [DOI] [PubMed] [Google Scholar]
- 28.Mehta RL, Pascual MT, Gruta CG, Zhuang S, Chertow GM. Refining predictive models in critically ill patients with acute renal failure. J Am Soc Nephrol. 2002;13(5):1350–7. doi: 10.1097/01.ASN.0000014692.19351.52. [DOI] [PubMed] [Google Scholar]
- 29.Chertow GM, Soroko SH, Paganini EP, Cho KC, Himmelfarb J, Ikizler TA, Mehta RL. Mortality after acute renal failure: models for prognostic stratification and risk adjustment. Kidney Int. 2006;70(6):1120–6. doi: 10.1038/sj.ki.5001579. [DOI] [PubMed] [Google Scholar]
- 30.Paganini EP, Halstenberg WK, Goormastic M. Risk modeling in acute renal failure requiring dialysis: the introduction of a new model. Clin Nephrol. 1996;46(3):206–11. [PubMed] [Google Scholar]
- 31.Akca S, Haji-Michael P, de Mendonca A, Suter P, Levi M, Vincent JL. Time course of platelet counts in critically ill patients. Crit Care Med. 2002;30(4):753–6. doi: 10.1097/00003246-200204000-00005. [DOI] [PubMed] [Google Scholar]
- 32.Oguzulgen IK, Ozis T, Gursel G. Is the fall in platelet count associated with intensive care unit acquired pneumonia? Swiss Med Wkly. 2004;134(29-30):430–4. doi: 10.4414/smw.2004.10670. [DOI] [PubMed] [Google Scholar]
- 33.Strauss R, Wehler M, Mehler K, Kreutzer D, Koebnick C, Hahn EG. Thrombocytopenia in patients in the medical intensive care unit: bleeding prevalence, transfusion requirements, and outcome. Crit Care Med. 2002;30(8):1765–71. doi: 10.1097/00003246-200208000-00015. [DOI] [PubMed] [Google Scholar]
- 34.Vanderschueren S, De Weerdt A, Malbrain M, Vankersschaever D, Frans E, Wilmer A, Bobbaers H. Thrombocytopenia and prognosis in intensive care. Crit Care Med. 2000;28(6):1871–6. doi: 10.1097/00003246-200006000-00031. [DOI] [PubMed] [Google Scholar]
- 35.Parker RI. Etiology and significance of thrombocytopenia in critically ill patients. Crit Care Clin. 2012;28(3):399–411. doi: 10.1016/j.ccc.2012.04.007. [DOI] [PubMed] [Google Scholar]
- 36.Oh HJ, Shin DH, Lee MJ, Ko KI, Kim CH, Koo HM, Doh FM, Kwon YE, Kim YL, Nam KH, et al. Urine output is associated with prognosis in patients with acute kidney injury requiring continuous renal replacement therapy. J Crit Care. 2013;28(4):379–88. doi: 10.1016/j.jcrc.2012.11.019. [DOI] [PubMed] [Google Scholar]
- 37.Sawhney S, Mitchell M, Marks A, Fluck N, Black C. Long-term prognosis after acute kidney injury (AKI): what is the role of baseline kidney function and recovery? A systematic review. BMJ Open. 2015;5(1):e6497. doi: 10.1136/bmjopen-2014-006497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Cruz DN, Bagshaw SM, Maisel A, Lewington A, Thadhani R, Chakravarthi R, Murray PT, Mehta RL, Chawla LS. Use of biomarkers to assess prognosis and guide management of patients with acute kidney injury. Contrib Nephrol. 2013;182:45–64. doi: 10.1159/000349965. [DOI] [PubMed] [Google Scholar]
- 39.Sairam S, Domalapalli S, Muthu S, Swaminathan J, Ramesh VA, Sekhar L, Pandeya P, Balasubramaniam U. Hematological and biochemical parameters in apparently healthy Indian population: defining reference intervals. Indian J Clin Biochem. 2014;29(3):290–7. doi: 10.1007/s12291-013-0365-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Kweon OJ, Lee MK, Kim HJ, Chung JW, Choi SH, Kim HR. Neutropenia and neutrophil-to-lymphocyte ratio in a healthy Korean population: race and sex should be considered. Int J Lab Hematol. 2016;38(3):308–18. doi: 10.1111/ijlh.12489. [DOI] [PubMed] [Google Scholar]
- 41.Zarjou A, Agarwal A. Sepsis and acute kidney injury. J Am Soc Nephrol. 2011;22(6):999–1006. doi: 10.1681/ASN.2010050484. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.