

Abstract
Background:
Lifestyle modification is an essential factor in the promotion of health in patients with acute coronary syndrome (ACS). One of the interventions to promote lifestyle is interactive follow-up, which, according to the traditional methods, requires spending significant amount of time and cost. Therefore, this study aimed to determine the effectiveness of interactive text message follow-up on health promoting lifestyle of patients with ACS.
Materials and Methods:
This was a randomized controlled trial among 100 patients suffering from ACS during October–February 2016. The participants were randomly assigned to the experimental and control groups. Collection of data on lifestyle was performed before, 3, and 4 months after the beginning of the intervention using Walker's Health Promoting lifestyle questionnaire. Six messages were sent to the intervention groups each week, and participants asked the questions by sending text message, each week 1 message were sent to the control group for 12 weeks. The statistical analysis of data was performed using independent t-test, Chi-square, Mann–Whitney U test, and repeated measures analysis of variance (ANOVA).
Results:
Before the intervention, there was no significant difference between the mean score of lifestyle of the two groups, however, 3 months and 4 months after the beginning of the intervention, the mean score of lifestyle in the intervention group was significantly higher than that of the control group (P < 0.001).
Conclusion:
The interactive text message follow-up is effective in promoting the lifestyle of patients with ACS and can be considered in the planning of follow-up of patients with ACS.
Keywords: Acute coronary syndrome, follow up, health promoting lifestyle, interactive text message, Iran
Introduction
Acute coronary syndrome (ACS) is one of the most common heart diseases, which is a progressive and life-threatening disease around the world and is the most common cause of hospitalization.[1] According to the estimates, it causes 35% of the mortality cases around the world.[2] In Iran, ACS have been the cause 46% of mortality cases, with an incidence rate of 181.4 in every 100,000 individuals.[3]
The ideal treatments of ACS include pharmaceutical, surgical interventions, management of risk factors, and lifestyle modification.[1] This disease can most probably be prevented and is a noncommunicable disease.[4] Eighty percent of the causes of the ACS are risk factors which can be moderated by lifestyle modifications.[5] Therefore, lifestyle modification is considered as one of the strategies used for treating ACS.[6] Lifestyle includes daily activities of a person which influence their health,[7] and a behavior that the person uses to guide his/her own daily activities. These behaviors have a significant impact on the health of the person.[8,9]
An intervention to promote lifestyle is follow-up,[10] which is an important component of services provided by nurses.[11] Various methods are used in the health care system to follow up patients' status. Some of these methods consist of patients' referral to care centers or home visits by health care personnel. Although these methods are effective, they require human resources, time, and are very expensive;[12] therefore, in recent years, the use of mobile phone in following up patients with heart disease has increased, which enables nurses to monitor the patient, train them, and perform nursing interventions.[13] One of the principal functions of mobile phones is text messaging,[12] which is efficient, easy, and cost-effective.[14] However, many cases are one-sided and there are few cases where there is an interaction between the patient and the nurse.[15] Using a mobile phone makes it possible for both the sides to interact with one another.[16] This interaction makes patients motivated to change their behavior and it makes it easier for them to reach their goals.[17]
The efficacy of text message follow-up in the management of ACS and healthy behaviors has been studied in a number of previous studies.[18,25,26,27,28,29,30] Conflicting results have been obtained from these studies regarding the efficiency of this method; whereas the results of a number of these studies confirm the positive effect of the text message follow-up on changing patients' healthy behaviors.[19,20,21,30] The results of a number ofthese studies showed that this method hadbeen unable to affect the healthy behaviors of the patients or management of risk factors.[14,25,26] For instance, Dale et al.[30] (2015) in Auckland hospital, New Zealand aimed to review the effect of a comprehensive rehabilitation program using text message on healthy lifestyle, depression, and anxiety. For 24 weeks, a message was sent to the patients on a daily basis and they were able to ask their own questions. Three months after the beginning of the program, the results showed that sending text message improved healthy lifestyle (P = 0.03), but had no significant impact on anxiety and depression (P > 0.05).[30] The number of these patients is increasing in Iran, with majority being old; it might be difficult for such patients to attend the follow-up sessions. Moreover, nurses are the key members of the health care team who have the most significant relationship with the patients in the health care centers; therefore, they need an appropriate method to use. Taking into consideration the conflicting results of the previous studies and the fact that other methods have been used in such studies along with this one, it is clear that there are only few studies that have focused on the effect of using text messages on the lifestyle of patients diagnosed with ACS. Thus, the present study aims to determine the effect of this method on the health-improving lifestyle of these patients.
Materials and Methods
The present study was a clinical trial (IRCT 2015111625077N1). The study participants consisted of patients with ACS who hospitalized in the cardiac wards of Shahid Chamran Hospital (Isfahan, Iran) during October–February 2016. The sample size was calculated according to power analysis at 95% confidence interval and 80% power, with 43 individuals in each group. Because of the possibility of loss of participants, in total, 100 individuals were included in the study. The participants were randomly divided into two groups (100 same-sized cards). Number 1 was written on 50 of them and number 2 was written on the other 50. All of the 100 cards were put in a sealed envelope. Then each of the participant was asked to choose a card at the time of the random division. If the card they picked said number 1, they would be in the intervention group, and if it said 2, they would be in the control group.
The inclusion criteria consisted of diagnosis of ACS by a cardiologist,[5] age 35–70 years,[10] lack of any recognizedmental condition or mental and motor disabilities,[29] havingaccess to a personal or family mobile phone,[15] being able to read and write and being familiar with Farsi,[29] not having any problems with their vision, having access to a third person who can type and read the text messages for them,[15] being able to do the daily activities,[10] the cardiologist confirmed that the selected patients were eligible for receiving text messages, and finally, their normal blood tests (creatinine, potassium, and blood urea nitrogen). The exclusion criteria included unwillingness to participate in the study,[15] hospitalization or death during the study period,[29] changing their mobile phone number and not informing the researcher,[12] and encountering physical and mental problems resulting in disability at any stage of the research.[14]
Data collection was performed in the two groups of patients before, 3 months after, and 4 months after the beginning of the intervention. The data collection tool comprised two parts. The first part consisted of questions on demographic characteristics andinformation on the disease (age, gender, education, marital status, history of risk factors such as hyperglycemia, hypertension, dyslipidemia, smoking, and history of hospitalization). The second part consisted of Walker's standard health-promoting lifestyle questionnaire that has six subscales (nutrition, physical activity, stress management, interpersonal relationships, health responsibility, and self-realization). This questionnaire is scored using a four-point Likert scale (1 = never, 2 = sometimes, 3 = often, and 4 = always). The minimum score of the questionnaire is 52 and the maximum score is 208. A separate score can be calculated for each area and a higher score is an indication of a better health condition.[9,20] The reliability and validity of this questionnaire has been calculated in Iran, and a Cronbach's alpha of 82% has been calculated for the tools and Cronbach's alpha of 64% to 91% have been reported for the subcategories. The total reliability of the test was 91% and the reliability of the food, physical activity, stress management, interpersonal relationships, taking on responsibility, and self- realization dimensions were 089, 075, 0.78, 0.80, 0.78, and 0.71, respectively.[20] In the present study, The Cronbach's alpha of the scale was0.84, and these patients were eliminated from the study. The patients were informed of the goals of the study and informed consents were obtained from them. Then, the researcher's colleague filled out the questionnaire through interviews with the patients without any information about the groups and the purposes of the study. After primary data collection, mobile phone number of the patients were obtained. To ensure that messages were sent, the researcher activated the delivered option in her mobile phone. Then, the researcher sent one of the prepared messages to ensure that the messages were sent and received at the same time.[13] The patients were asked to give an alternate mobile phone number to the researcher in case they failed to receive more than two messages so that they would receive others.[11] Finally, the participants were randomly divided into two groups.
During the 12 weeks of the text message follow-up, six messages were sent to the participants in the experimental group each week (except the weekends) between 8 AM and 8 PM. If the participants had any questions regarding their disease or their medicine or text messages, they could ask questions from 8 AM to 8 PM via text messages and the researcher would reply to the questions. In addition, the number of messages exchanged between the participants and the researcher was increased for this purpose. Each message had a maximum of 160 characters.[11] The context of the text messages sent to the intervention group comprised training based on the content of the dimensions of Walker's health-promoting lifestyle questionnaireand risk factors of ACS [Table 1].[21] For instance, a message sent to the participants was: Use less salt while cooking food and use garlic or herbs powder instead. One of the questions was: What is metohexal tablet and what are its applications? The answer to this question was that this tablet reduces heart rate and blood pressure and is used to treat chest pain.
Table 1.
Content of text messages in the intervention (IG) and the control group (CG)
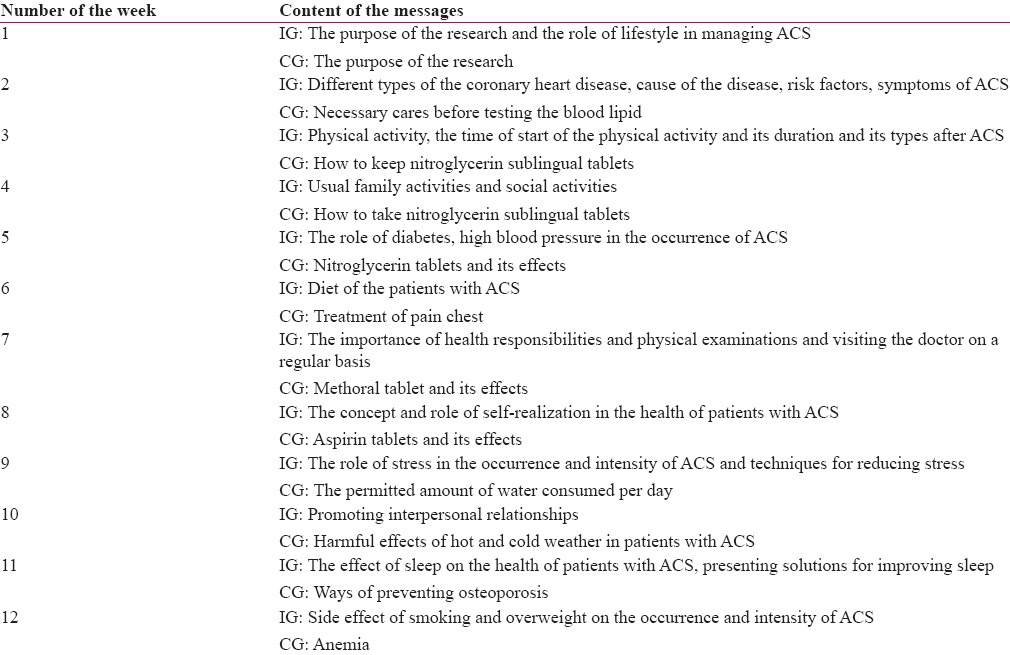
For 12 weeks, the participants in the control group received a message per week containing health care messages unrelated to the health-promoting lifestyle. Their relationship was one-sided and no interaction was allowed. The patients did not send the researcher any messages and did not ask any questions [Table 1]. The questionnaire was completed by the researcher's colleague through interviews in both groups 3 and 4 months after the beginning of the intervention.
Statistical analysis of data was conducted using independent t-test, Chi-square test, Mann–Whitney U test, and repeated measures analysis of variance (ANOVA) in SPSS software (version 20; SPSS Inc., Chicago, IL, USA).
Ethical considerations
The researcher received permission and a written letter of introduction from the faculty of nursing and midwifery of Isfahan's University of Medical Sciences and presented it to the authorities and managers of the research environment. The study participants signed a written consent to participate in the study, which stated that they could exit the study any time they wanted and all of their personal information including their names remained confidential.
Results
Mean age of the study participants was 54.33 years in the intervention group with a standard deviation of 7.89 and was 56.05 years with a standard deviation of 7.71 in the control group. According to the results of the independent t-test, there was no significant difference between the two groups in terms of mean age (P > 0.05). In addition, there was no significant difference between the two groups with respect to gender, education, marital status, history of risk factors such as hyperglycemia, high blood pressure, dyslipidemia, smoking, and record of hospitalization. The results of the independent t-test showed that there was no statistically significant difference between the two groups in terms of the mean of the total score and lifestyle dimensions before the intervention. On the other hand, 3 and 4 months after the beginning of the intervention, the mean of the total score of lifestyle dimensions were significantly higher in the intervention group than the control group (P < 0.001). Repeated-measures ANOVA showed that there was a significant difference between the three different times in the intervention group in terms of the mean of the total score of lifestyle and all its dimensions (P < 0.001) [Table 2]. The mean of the total score of lifestyle and dimensions of nutrition and physical activity were significantly different at the three different times in the intervention group; however, the other dimensions did not experience a significant difference at those times [Table 3].
Table 2.
The mean total and dimensions score of lifestyle in the intervention group at different times
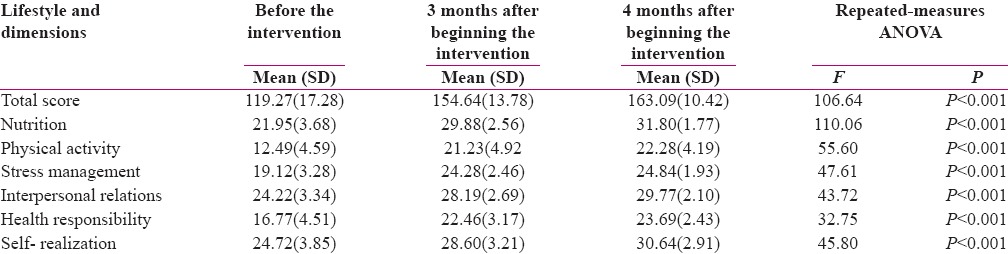
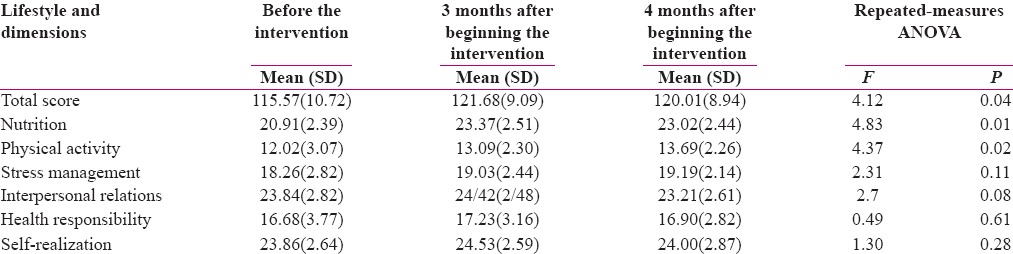
Table 3.
The mean total and dimensions score of lifestyle in the control group at different times
Independent t-test showed that the mean of difference of the total score of lifestyle 3 months after the beginning of the intervention was significantly higher in the intervention group (with a mean of 35.37 and standard deviation of 3.46) than the control group (with a mean of 6.11 and standard deviation 1.68). In addition, the mean of the differences of the score of the six dimensions 3 months after the beginning of the intervention (a mean of 7.93 and standard deviation of 0.76 for the nutrition dimension, a mean of 8.75 and standard deviation of 1.08 for the physical activity dimension, a mean of 5.16 and standard deviation of 0.62 for the stress management dimension, a mean of 3.96 and standard deviation of 0.72 for the interpersonal relationships dimension, a mean of 5.69 and standard deviation of 0.84 for the health responsibility dimension, and a mean of 3.88 and standard deviation of 0.73 for the self- realization dimension) was significantly higher than the control group (a mean of 2.47 and standard deviation of 0.35 for the nutrition dimension, a mean of 1.07 and standard deviation of 0.47 for the physical activity dimension, a mean of 0.77 and standard deviation of 0.37 for the stress management dimension, a mean of 0.58 and standard deviation of 0.42 for the interpersonal relationships dimension, a mean of 0.56 and standard deviation of 0.56 for the health responsibility dimension, and a mean of 0.67and standard deviation of 0.42 for the self- realization dimension) (P < 0.001). The results of the independent t-test showed that the mean of the differences of the total score of lifestyle 4 months after the beginning of the intervention was significantly higher in the intervention group (with a mean of 43.35 and standard deviation of 2.94) than the control group (with a mean of 4.44 and standard deviation 2.17) (P < 0.001). In addition, the mean of the differences of the score of the six dimensions 4 months after the beginning of the intervention (a mean of 9.84 and standard deviation of 0.66 for the nutrition dimension, a mean of 9.8 and standard deviation of 0.96 for the physical activity dimension, a mean of 5.72 and standard deviation of 0.59 for the stress management dimension, a mean of 5.55 and standard deviation of 0.59 for the interpersonal relationships dimension, a mean of 6.76 and standard deviation of 0.84 for the health responsibility dimension, and a mean of 5.92 and standard deviation of 0.61 for the self-realization dimension) was significantly higher than the control group (a mean of 2.12 and standard deviation of 0.52 for the nutrition dimension, a mean of 1.67 and standard deviation of 0.52 for the physical activity dimension, a mean of.92 and standard deviation of 0.57 for the stress management dimension, a mean of −0.63 and standard deviation of 0.56 for the interpersonal relationships dimension, a mean of 0.23 and standard deviation of 0.15 for the health responsibility dimension, and a mean of 0.14 and standard deviation of 0.13 for the self-realization dimension) (P < 0.001).
Discussion
According to the results of this study, interactive text message follow-up affects the health-promoting lifestyle of patients suffering from ACS. There was no significant difference between the two groups (intervention and control group) before the intervention in terms of demographic variables, personal information of patients, the mean of the total score, and the score of the dimensions of the health-promoting lifestyle. In this respect, the study by Khonsari et al. was performed with the aim of determining the effect of a reminder system using an automated text message service on medication adherence following ACS. They found no significant difference between the two groups in terms of demographic variables, information on the disease, medication adherence, and physical activity.[22]
The results of the present study showed that, 3 and 4 months after the beginning of the intervention, mean of the total score and dimensions of lifestyle were significantly higher in the intervention group than those in the control group. In this respect, Maddison et al. studied the effect and the cost-effectiveness of interventions using mobile phone on the physical capacity and physical activity of patients with ischemic heart disease. They found that patients in the experimental group experienced a significant increase in their physical activity, self-efficacy, and quality of life 24 months after the beginning of the intervention (P < 0.05).[23] Moreover, the study by Norman et al. was performed with the aim of determining the effect of a text message follow-up on the weight loss and eating habits. They found that the experimental group patients had lost more weight and experienced an improvement in their eating habits in comparison with the control group (P < 0.05).[24] Antypas and Wangberg studied the impact of an intervention via internet and text messaging on the physical activity of women diagnosed with heart disease after a cardiac rehabilitation program. They found that, 3 months after follow-up, no significant difference was seen between the two groups (control and experimental group) in terms of the mean of physical activity, social support, anxiety, depression, self-efficacy, and medication adherence (P < 0.05).[25]
The results of the present study showed that the mean of the total and its dimensions of lifestyle score of the intervention group significantly differed before and 3 months and 4 months after the intervention. There was a significant difference between the mean of the total score of lifestyle and nutrition and physical activity dimensions of the control group, which differed before and 3 months and 4 months after the intervention (P < 0.05), however, no significant difference was seen between the stress management, interpersonal relationships, responsibility, and spiritual growth dimensions (P > 0.05). Hence, it was expected that, as time passed and the symptoms improved, patients in the control group showed more behaviors which were indicative of better health. In addition, the information obtained from the treatment team, peers, and media can influence patients' health-related behaviors,[28] and sending messages regarding health care can make the results significant. Nonetheless, the results of this study showed that the mean of the total score and the score of the dimensions of lifestyle in the intervention group 3 and 4 months after the beginning of the intervention were higher than the control group. This indicates that the interactive text message follow-up is effective. The study byBoroumand and Moeini was performed with the aim of determining the efficacy of afollow-up program via text messages and telephone on the self-efficacy of patients with coronary heart disease. They found that at the three different times of the study, the scores of cardiac self-efficacy of patients in the experimental group were significantly different (P < 0.001) and the score of cardiac self-efficacy was significantly higher 3 and 4 months after the beginning of the intervention than that before the intervention.[29] The study bySadri et al. was performed with the aim of comparing two methods of text messages (interactive and noninteractive) on anticoagulant adherence of patients with prosthetic heart valve. They found that text message follow-up led to an increase in the mean of the score of anticoagulant adherence in three groups, however, the scores were higher in the interactive group. This result indicates that using text messages to interact with the patients effects anticoagulant adherence (P < 0.001), and a significant difference was seen between the score of anticoagulant adherence in groups with the interactive and noninteractive methods of text messages after the intervention (P < 0.05).[15] Unlike the present study, Frederix et al. performed a study on the effect of a comprehensive rehabilitation program via the internet and text messaging in patients with coronary heart disease. They found that the number of steps taken per day increased in the experimental group, however, the mean of the score of physical activity was not significant and no change was seen in the weight and blood pressure of the patients.[26]
The most important limitation of the present study is that the information were obtained from other sources such as treatment team and media which could affect patients' lifestyle and could not be controlled. Another limitation is that the study was done in a health center. It is suggested that further studies be conducted in various centers with a bigger population. Another limitation was the short follow-up time after intervention. Therefore, it is suggested that further studies be conducted in this respect with longer duration.
Conclusion
According to the findings of the present study, an interactive text message follow-up is a proper method for promoting the lifestyle of patients with ACS. Because ACS is very prevalent and it is essentially important to follow-up, sample and cheap methods have been used to promote the lifestyle of these patients. It also seems that text message follow-up reduces the patients' need to visit the treatment team when it is not necessary. This method can also give the patients quick and easy access to health-related information, and if this relationship is interactive, it can reinforce people's motive to change their behavior and achieve their goals more successfully. When patients ask their questions via text messages, they will be more motivated to read their messages and do not look at them as advertisement and insignificant. In this case, nurses are the key members of the health care team who have the most communication with the patients and have a more comprehensive understanding of the needs of patients in terms of promoting their lifestyle and can use the findings of this study to follow up patients suffering from ACS.
Financial support and sponsorship
Isfahan University of Medical Sciences.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
This study was derived from the Masters' thesis with the research code of 394473 in Isfahan University of Medical Sciences, Isfahan, Iran. The authors wish to thank the Research Deputy of Isfahan University of Medical Sciences, staff of the cardiac wards of Shahid Chamran Hospital, and with ACS who participated in this study.
References
- 1.Chow CK, Redfern J, Thiagalingam A, Jan S, Whittaker R, Hackett M, et al. Design and rationale of the tobacco, exercise and diet messages (TEXT ME) trial of a text message-based intervention for ongoing prevention of cardiovascular disease in people with coronary disease: A randomised controlled trial protocol 2010. BMJ Open. 2012:e000606. doi: 10.1136/bmjopen-2011-000606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.De Waure CH, Lauret GJ, Ricciardi W, Bart Ferket B, Teijink J, Spronk S, et al. Lifestyle Interventions in Patients with Coronary Heart Disease: A Systematic Review. Am J Prev Med. 2013;45:207–16. doi: 10.1016/j.amepre.2013.03.020. [DOI] [PubMed] [Google Scholar]
- 3.Boroumand S, Shahriari M, Abbasi Jebeli M, Baghersad Z, Baradaranard F, Ahmadpoori F. Determine the level of self-efficacy and its related factors in patients with ischemic heart disease: A descriptive correlational study. IJNR. 2015;9:61–9. [Google Scholar]
- 4.Shahsavari S, Nazari F, Karimiyar M, Sadeghi M. Epidemiologic study of hospitalized cardiovascular patients in Jahrom hospitals in 2012- 2013. J Cardiovasc Nurs. 2013;2:14–21. [Google Scholar]
- 5.Nasrabadi T, Goodarzi Zadeh N, Shahrjerdi A, Hamta A. The Effect of Education on Life Style Among Patients Suffering from Ischemic Heart Disease. J Mazand Univ Med Sci. 2010;20:72–9. [Google Scholar]
- 6.Shahabinejad M, Bakhshi H, Rezaei M, Khodadi A. The survey of life style of acute coronary syndrome in bed in CCU of Aliyebne Abitaleb university hospital of Rafsanjan during 2006. J Nurs Midwifery Rafsanjan. 2010;3:50–6. [Google Scholar]
- 7.Abedi HA, Bik Mohammadi S, Abdeyazdan Gh, Nazari H. A Survey on the lifestyle of the heart disease patients after discharge from hospital in urmia seyyed alshohada in 1391. J Urmia Nurs Midwifery Fac. 2014;11:944–54. [Google Scholar]
- 8.Walker SN, Sechrist KR, Pender NJ. The health promoting lifestyle profile: Development and psychometric characteristics. Nurs Res. 1987;36:76–81. [PubMed] [Google Scholar]
- 9.Booth JN, Levitan EB, Brown TM, Farkouh ME, Safford MM, Muntner P. Effect of Sustaining Lifestyle Modifications (Nonsmoking, Weight Reduction, Physical Activity, and Mediterranean Diet) After Healing of Myocardial Infarction, Percutaneous Intervention, or Coronary Bypass (from the REasons for Geographi and Racial Differences in Stroke Study) Am J Cardiol. 2014;113:1933–40. doi: 10.1016/j.amjcard.2014.03.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Taherian A, Mohammadi F, Hosseini MA, Rahgozar M, Fallahi Khoshknab M. Effectiveness of education and follow-up in home on knowledge and health behaviors in patients with Myocardial Infarction. J Nurs. 2007;2:7–13. [Google Scholar]
- 11.Mousavifar SA, Zolfaghari M, Pedram Sh, Haghani H. Examine the effectiveness of two methods follow-up (mobile and phone) on adherence to treatment in patients with diabetes. Iran J Diabetes Lipid Disord. 2011;10:407–18. [Google Scholar]
- 12.Goodarzi M, Ebrahimzadeh I. Impact of distance education via short message service of mobile phone on metabolic control of patients with type 2 diabetes mellitus in Karaj-Iran. Horizon Med Sci. 2014;19:224–34. [Google Scholar]
- 13.Hemmati Maslakpak M, Parizad N, Khalkhali H. The effect of tele-education by telephone and short message service on glycaemic control in patient with type 2 diabetes. J Urmia Nurs Midwifery Fac. 2012;10:580–8. [Google Scholar]
- 14.Sadeghi Shermeh M, Ghafuri F, Tadrissi D, Tayyebi A. The effect of two methods, follow-up care by telephone and short message services on prothrombin time in patients with valve replacement surgery in hospitals of Tehran. Med Surg Nurs J. 2012;1:36–41. [Google Scholar]
- 15.Sedri N, Asadi Noughabi AA, Zolfaghari M, Haghani H, Tavan A. Comparison of the effect of two types of short message service (interactive and non-interactive) on anticoagulant adherence of patients with prosthetic heart valve. J Nurs Educ. 2014;2:1–11. [Google Scholar]
- 16.Riley WT, Rivera DE, Atienza AA, Nilsen W, Allison SM, Mermelstein R. Health behavior models in the age of mobile interventions: Are our theories up to the task? Transl Behav Med. 2011;1:53–71. doi: 10.1007/s13142-011-0021-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Burke LE, Conroy MB, Sereika SM, Elci OU, Styn MA, Acharya SD, et al. The Effect of Electronic Self-Monitoring on Weight Loss and Dietary Intake: A Randomized Behavioral Weight Loss Trial. Obesity. 2012;19:338–44. doi: 10.1038/oby.2010.208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Stephens J, Allen J. Physical activity and reduce weight are two important health behaviors in management of ACS. J Cardiovasc Nurs. 2014;28:320–9. doi: 10.1097/JCN.0b013e318250a3e7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hosseinnejad M, Klantarzadeh M. Lifestyle among Students of Islamic Azad University, Kerman Branch based on the Pender's Health Promotion model. J Health Educ Health Promotion. 2014;4:15–28. [Google Scholar]
- 20.Mohammadi Zaidi I, Pakpoor Hajiagha A, Mohammadi Zaidi B. Validity and reliability of the Persian version of health-promoting lifestyle. J Mazandaran Univ Med Sci. 2010;21:103–13. [Google Scholar]
- 21.Eshah NF. Predischarge education improves adherence to a healthy lifestyle among Jordanian patients with acute coronary syndrome. Nurs Health Sci. 2013;15:273–9. doi: 10.1111/nhs.12018. [DOI] [PubMed] [Google Scholar]
- 22.Khonsari S, Subramanian P, Chinna K, Latif LA, Ling LW, Gholami O. Effect of a reminder system using an automated short message service on medication adherence following acute coronary syndrome. Eur J Cardiovasc Nurs. 2015;14:170–9. doi: 10.1177/1474515114521910. [DOI] [PubMed] [Google Scholar]
- 23.Maddison R, Pfaeffli L, Wittaker R, Stewart R, Jiang Y, Kira G, et al. A mobile phone intervention increases physical activity in people with cardiovascular disease: Results from the HEART randomized controlled trial. Eur J Prev Cardiol. 2015;22:701–9. doi: 10.1177/2047487314535076. [DOI] [PubMed] [Google Scholar]
- 24.Norman GJ, Kolodziejczyk JK, Adams MA, Patrick K, Marshall SJ. Fruit and vegetable intake and eating behaviors mediate the effect of a randomized text-message based weight loss program. Prev Med. 2013;56:3–7. doi: 10.1016/j.ypmed.2012.10.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Antypas K, Wangberg S. An Internet- and Mobile-Based Tailored Intervention to Enhance Maintenance of Physical Activity After Cardiac Rehabilitation: Short-Term Results of a Randomized Controlled Trial. J Med Internet Res. 2014;16:e77. doi: 10.2196/jmir.3132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Frederix I, Hansen D, Coninx K, Vandervoort P, Vandijck D, Hens N, et al. Medium-Term Effectiveness of a Comprehensive Internet-Based and Patient-Specific Tele rehabilitation Program With Text Messaging Support for Cardiac Patients: Randomized Controlled Trial. J Med Internet Res. 2015;17:e185. doi: 10.2196/jmir.4799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Park LG, Howie-Esquivel J, Chung ML, Dracup K. A text messaging intervention to promote medication adherence for patients with coronary heart disease: A randomized controlled trial. Patient Educ Counsel. 2014;94:261–8. doi: 10.1016/j.pec.2013.10.027. [DOI] [PubMed] [Google Scholar]
- 28.Shamsizadeh M. Effects of peer education on anxiety and self-efficacy in patients for elective coronary artery bypass graft surgery [Thesis] Tehran, Iran: School of Nursing and Midwifery, Tehran University of medical sciences; 2012. pp. 48–50. [Google Scholar]
- 29.Boroumand S, Moeini M. The effect of a text message and telephone follow- up program on cardiac self-efficacy of patients with coronary artery disease: A randomized controlled trial. Iran J Nurs Midwifery Res. 2016;21:171–6. doi: 10.4103/1735-9066.178243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Dale LP, Whittaker R, Jiang Y, Stewart R, Rolleston A, Maddison R. Text Message and Internet Support for Coronary Heart Disease Self-Management: Results From the Text4Heart Randomized Controlled Trial. J Med Internet Res. 2015;17:e237. doi: 10.2196/jmir.4944. [DOI] [PMC free article] [PubMed] [Google Scholar]