

Abstract
Background:
Cardiovascular diseases are the most important causes of morbidity and mortality in the world, and cardiac surgery is one of the treatments that have complication for patients. One of the most important current psychological complications after cardiac surgery is delirium. For its prevention and treatment, considerable attention should be paid to the role of family. This study has been conducted for assessing the effect of the relationship between the family and patient on the incidence of delirium in hospitalized patients in cardiovascular surgery intensive care unit (ICU) of Isfahan Shahid Chamran hospital.
Materials and Methods:
This study is a two-group, single-blind (for the questioner) clinical trial that was conducted among 68 patients in the cardiac surgery ICU of Shahid Chamran hospital affiliated to the Isfahan University of Medical Science in 2013. Sampling was convenient sampling, and the patients were allocated to two groups (n = 34 patients) based on random numbers table. The day after the surgery, one of the family members in the intervention group who had received education the day before was allowed to visit the patient in the morning shift. In the control group, patients received routine care. Two groups were assessed for delirium twice a day for a total of three times (two times in the morning and one time in the evening) with use of Richmond Agitation Sedation Scale and Confusion Assessment Method –ICU (CAM – ICU) scale.
Results:
In the intervention group, 41.18% patients were females and 58.82% patients were males, and in the control group, 29.42% patients were females and 70.58% were males. Mean and SD of patients' age in the intervention group was 55.11 (12.11) and in the control group 54.12 (13.11) years. Based on study results, incidence of delirium in the morning after surgery (second day) in intervention group was 11.76%, and in control group it was 23.53%. In the third day, it was 8.83% in intervention group and 20.58% in control group. Chi-square test showed a significant difference in incidence of delirium during the second (P = 0.04) and the third (P = 0.03) days of surgery in the two groups. In the control group, the incidence of delirium in the evening was 32.35%, which was more than that in the morning. Cochran test showed a significant difference in the morning and afternoon shifts in the control group (P = 0.004).
Conclusions:
Effective communication between the patient and family, as a nonmedical method, can reduce delirium after cardiac surgery, especially, at the end of the day; nurses should pay more attention to the prevention of delirium.
Keywords: Delirium, family, intensive care unit, nursing care, open cardiac surgery, therapeutic relationship
Introduction
Cardiac surgery is an important intervention in cardiac diseases that preserves the patients and improves their quality of life (QOL); it is a crucial event for the patients as well as their families.[1] Among the most important cardiac postsurgery complications in the intensive care unit (ICU) are cognitive disorders such as delirium.[2]
Approximately one-third to one-fourth of the patients experience delirium from the second to the fifth day after the surgery.[3] This syndrome with an incidence rate of 30–73% increases mortality by 20–30%,[4] leading to frequent hospitalizations, attention disorders, memory and perception impairment, poor function, prolonged hospitalization, and reduction of QOL.[5,6] Caring patients in ICU can be stressful and difficult, which can get more difficult in delirium even for skilled and experienced nurses.[7] For prevention and treatment of mental problems, family is at the heart of attention,[8] it can be used for patients' empowerment, education, relief, and peace.[9] Bruntonet al. (2010) believed that family participation is effective for the prevention of incidence of delirium among the elderly in ICU.[10] Zolfaghariet al. (2010), in a study on the effect of multifactorial intervention on prevention of delirium incidence and on the length of hospitalization of open cardiac surgery patients, reported that the intervention reduced delirium incidence up to approximately 25%.[11] Blacket al. (2010)[12], in a study on family's participation in mental care of critical patient hospitalized in ICU, reported that it had no significant effect on reduction of delirium. Meanwhile, in case of delirium, the patient undergoes medicational treatment or physical limitations and is separated from the family after hospitalization.
As research showed a reduction in patients' anxiety through presence of family in the ICU and in patients' experiencing psychological stress (through a proper communicational model), the incidence of delirium and its complications for the patients, the family, and the society can be prevented through psychological support, given by the family after the surgery. Therefore, with regard to the role of nurses in diagnosis, prevention and treatment of delirium, and with respect to the communicational role of the family and the importance of proper communication in the occurrence of this syndrome, the present study aimed to investigate the effect of family–patient communication on the incidence of delirium in hospitalized patients in cardiovascular surgery ICU of the Isfahan Shahid Chamran hospital in 2013.
Materials and Methods
This study was a randomized controlled clinical trial conducted in 2013 (Trial Registration Number: IRCT201604107391N3). This research was conducted on 68 patients, derided in two groups, who underwent open heart surgery in the ICU of Shahid Chamran hospital in Isfahan (Iran). The patients who met the inclusion criteria were selected through convenient sampling using a random number table, and were assigned into two groups of study and control. P1 and p2 were the incidence of delirium in patients, with or without a family visit. And respectively, they were estimated.1and.33 in the pilot study. According to confidence level of 95% and test potency of 75%, the estimated sample size was 31 people. Considering the possible sample loss and to increase accuracy, final sample size was determined at 34 subjects per each group.
Inclusion criteria were age of 18–70 years, availability of immediate family members, no history of addiction to drugs, alcohol, and cigarette smoking, no delirium, consciousness level disorder and mental diseases before surgery, no history of blindness and deafness, elective open heart surgery, no family history for surgery, and no intubation with a tracheal tube. In cases of patients' or their family's reluctance to continue participation, death, or postsurgery acute complications, the patients were excluded from the study. The tool adopted in the present study was a two-section questionnaire. The first section included subjects' and family members' demographic information such as age, sex, education level, occupational status, marital status, and patients' vital signs and surgery-related information, which were referred to the academic members of adult health department, ICU, and psychiatry nursing department in nursing and midwifery school of Isfahan to establish the content validity after reviewing the related texts and articles; finally, its content validity was established. The second section was a tool to investigate delirium including Confusion Assessment Method –ICU (CAM – ICU), designed to assess the patients concerning delirium. The sensitivity and specificity of this scale were reported to be over 90–95% in various studies. In Daly's study, its sensitivity and specificity were reported 95% and 89%, respectively.[13]
A part of this scale was for determining the level of irritability based on Richmond Agitation Sedation Scale (RASS) that was scored from −5 to +4.[14]
On the scale of confusion assessment, four stages were investigated. The first stage is for sudden onset and unstable periods. The second was for patients' disorientation; the third thought disorder, and the fourth unstable level of consciousness. If the patients obtains the minimum scores (score one in any stage) in stages one and two or any of the third or the fourth stage (obtaining scores of 3–4), they are known to suffer from delirium, and in case of obtaining scores 0, 1, and 2, the presence of delirium was rejected. To conduct the study, after obtaining the permission from the ethics committee and coordinating with related units, the researcher referred to cardiac ward and selected the patients, meeting the inclusion criteria, who were hospitalized for an elective open heart surgery, and after explanation about the research goal and obtaining the informed written consent from the patients and their families, randomly assigned them to study and control groups by random number table. Researcher held a 2-hour class for the families to familiarize them with the goal, signs, causes, prevention methods of delirium, and communicational methods, and distributed pamphlets among them. These materials were reviewed before each visit with the family members. The nurses of cardiac surgery ICU were explained about the study in 2-hour sessions. The day before the surgery, the patients in the study and control groups were assessed by RASS and CAM- ICU scales for any existing delirium. After surgery, to administrate critical care, the patients were transferred to cardiac surgery ICU and underwent critical care for 48–72 h. To administrate the intervention, from the day after the surgery, when the patient was separated from the ventilation device and was able to communicate, after coordinating with the ICU staff and at a certain time of morning shift (once a day), a family member in the study group (selected by the patient and after undergoing necessary education) was permitted to attend by the patient for 30–40 minutes and communicated with him/her, based on the already received education after wearing a disposable gown, shoes cover, a mask, and disinfection of the hands with an antibacterial spray. For the patients in the control group, no special visit was scheduled and the family visited their patients based on hospital regulations, although their visits were recorded. Structured visits and communications in the study group were administrated from the day after the surgery until discharge from the ICU, and with a total of two visits for each participant in the study group (morning of the second and the third days of hospitalization in the ICU). Therefore, two groups of control and study were assessed by delirium questionnaire (two times in the morning of the second and the third day and one time in the evening of the second day). Environmental conditions were identical for both the groups to reduce the effect of environmental factors. Communicational method was explained to the family members who attended the study. If the patient wore glasses or used a hearing aid device, it was given to him/her. Then after attending by the patient's bed and holding his/her hand, the patient was oriented about his/her current location, date and time, and was explained the reason for being in such a ward. Through coordination with the nurses, patients' personal important and meaningful stuffs were brought from home and laid by him/her. The researcher warmly talked with the patients and let them express their feelings. Finally, the patients were encouraged to maintain their dependency and ability, and they were assured to be supported by the family and to have a beautiful and clear future.[15,16,17]
In both the groups of study and control, delirium was assessed twice a day once in the morning (after relatives' visit) and once in the evening through CAM-ICU in the ward by a staff nurse who was trained about filling in the scales and was blind to the study and control groups. Data were analyzed through the Statistical Package for the Social Sciences version 20 (SPSS 20, Chicago, IL), and by descriptive statistical tests such as frequency distribution and distribution, mean and SD, and inferential statistics (Chi-square, Mann–Whitney, independent t-test, and Fisher's exact test).
Ethical considerations
The ethics committee of the Isfahan University of Medical Sciences approved this study under code IR.MUI.REC.1392.3.010. Informed consent form was completed by patients and their families.
Results
In the present study, 68 patients were investigated. There was no significant difference in both groups concerning demographic characteristics including age, sex, marital status, occupation, level of education, type of surgery, and the narcotics and tranquilizers they took after surgery [Tables 1 and 2].
Table 1.
Variables of age and length of surgery in two groups
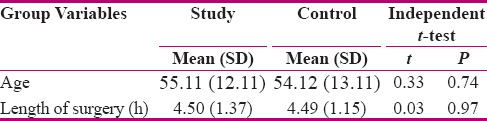
Table 2.
Frequency distribution of patients’ demographic characteristics in two groups

There were 41.18% male and 58.82% female participants. Regarding the relationship with the patient, 35.29% were spouses, 50% children; 5.88% were sisters; 2.94% brothers, and 5.88% were other relatives.
There was no significant difference in the two groups concerning delirium and RASS the day before the surgery. After data analysis, Chi-square test showed the incidence of delirium on the morning of the second postoperative day as 11.76% and 23.53% in study and control groups, respectively. The incidence was 8.83% in study and 26.58% in control group in the morning of the third postoperative day. Chi-square test showed a significant difference in the incidence of delirium between the two groups in the morning of the second day (χ2 = 3.98, P = 0.04) and the third day (χ2 = 4.12, P = 0.03). This value was 11.76% in study and 32.35% in control groups in the evening of the second postoperative day. Chi- square test showed a significant difference between two groups (χ2 = 8.38; P = 0.04). Chi- square test also showed a significant difference in comparison of relative frequency of delirium in the first (P = 0.04), the second (P = 0.04), and the third time between study and control groups [Tables 3 and 4].
Table 3.
Comparison of the relative frequencies of delirium in two groups on the second and the third days postsurgery
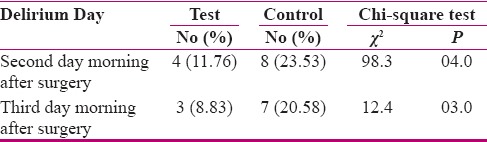
Table 4.
Comparison of the relative frequencies of delirium in two groups on the first, the second, and the third times

Discussion
Results showed that appropriate relationship of the family with the patient, through structured and regular visits to the patients after cardiac surgery, notably reduced the incidence of delirium in the patients in the study group. These regular and structured post cardiac surgery visits can diminish delirium by 21%. This value was measured at different morning and evening time points in the two groups and showed the restlessness and delirium to be more during the ending hours of a day, according to which the importance of the evening visits can be emphasized.
Because delirium is among the most common complications in cardiac surgery ICU and can be harmful for the patients, its diagnosis and prevention is very important. Based on the results, family members can be used to make the feeling of health and ability in their patient to cope with this condition.[18,19] Ghanavati et al.[2] (2009) claimed that the incidence of delirium was less in married patients, compared to single ones, such that 40% of the married and 77% of the single patients suffered from cognitive disorders. Their finding shows that being single and lonely is a risk factor for the incidence of delirium. It can be due to more familial support and fulfillment of the needs leading to patients' feeling of safety among married patients during their hospitalization. Meanwhile, in the present study, with regard to patients' age and because 97.1% and 94.1% of the patients in study and the control groups were married, respectively, this association could not be investigated.
Brunton et al., in a study on family participation in the prevention of delirium in the elderly, hospitalized in ICU, showed that family members could be used to prevent delirium. In fact their results support the role of family participation in the prevention of delirium,[10] and are consistent with the present study. Dalyet al. (2010) reported no significant reduction in the incidence of patients' cognitive disorders and aggression indexes, which resulted from communication and structured visits among ICU patients,[13] which was not in line with the present study. The reason for this controversy may be the difference in the content of conducted communication and research. Our obtained results and other studies show that involvement of the family in patients' situation can bring about patients' education, relief, peace and feel of safety, and reduce delirium.[10] Family members should be counted as a treatment team through formation of a positive environment and its direct effect on disease outcomes.[11] The most important limitation of this study was the follow-up time, so it is suggested that further studies be conducted in this respect with longer follow-up duration.
Conclusion
With regards to our obtained results, it can be concluded that attendance of the family by the patient after the cardiac surgery can be a non- medicational strategy in the prevention of delirium. Involvement of patients' family and their support after the surgery can prevent delirium and its resulting complications, imposed to the patients, their family, and finally, the society, especially when the ICU nurses are busy and have inadequate time to care and screen patients' mental and psychological problems.
Therefore, with respect to high incidence of postcardiac surgery delirium and its numerous complications, conducting such research and complications plays an essential role in improvement of health and life expectancy among cardiac surgery patients.
Financial support and sponsorship
Isfahan University of Medical Science.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
This article was derived from a research project No 392010, dated April 9, 2013. The authors appreciate all the individuals who helped us with research including nursing and the staff in ICU of Isfahan Shahid Chamran Hospital, nursing authorities in the hospital, vice-chancellery of nursing and midwifery school in Isfahan University of Medical Sciences as well as all patients and their families attending this study.
References
- 1.Meyer K. Pre-operative health education for patients undergoing cardiac surgery (Doctoral dissertation) 2009 [Google Scholar]
- 2.Ghanavati A, Foroughi M, Ismaili SA, HasanTash S, et al. Incidence of delirium after cardiac surgery and intra operative confounders. Iran J Surg. 1388;17:10–1. [Google Scholar]
- 3.Tashakori A, Shanesaz A, Khajemogehi N. To compare the incidence of postoperative delirium in patients with open heart surgery and general surgery in Ahvaz Golestan hospital in 1378. Med J Ahwaz. 1383;41:37–43. [Google Scholar]
- 4.Chang Y, Tsai Y, Lin P, Chen M. Prevalence and risk factors for postoperative delirium in a cardiovascular intensive care unit. Am J Crit Care. 2010;17:567–75. [PubMed] [Google Scholar]
- 5.Koster S, Hensens A, der Palen J. The Long-term cognitive and functional outcomes of postoperative delirium after cardiac surgery. Ann Thorac Surg. 2009;87:1469–74. doi: 10.1016/j.athoracsur.2009.02.080. [DOI] [PubMed] [Google Scholar]
- 6.Maldonado J, Wysong A, Starre V, Block T. Dexmedetomidine and the reduction of postoperative delirium after cardiac surgery. Psychosom Med. 2009;50:206–17. doi: 10.1176/appi.psy.50.3.206. [DOI] [PubMed] [Google Scholar]
- 7.Llenore E, Robin Ogle K. Nurse-patient communication in the intensive care unit: A review of the literature. Aust Crit Care. 2000;12:142–5. doi: 10.1016/s1036-7314(99)70599-0. [DOI] [PubMed] [Google Scholar]
- 8.Koshan M, Vaghei C. Psychiatric nurses, mental health one andishe rafi Publications. 1388:28. [Google Scholar]
- 9.Rabi Siahkali S, Avaze A, Eskandari F, Khalegh dost mohamadi T, et al. Reading anxiety and psychological and environmental factors affecting the families of intensive care unit patients. J Crit Care Nurs. 1389;3:175–80. [Google Scholar]
- 10.Brunton D, Henneman E, Inouye SH. Feasibility of family participation in a delirium prevention program for hospitalized older adults. J Gerontol Nurs. 2010;36:22–33. doi: 10.3928/00989134-20100330-02. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Zolfaghari M, Arbabi M, Pedram Razi S, Biat K, Bavi A. Effectiveness of a Multifactor Educational Intervention on Delirium Incidence and Length of Stay in Patients with Cardiac Surgery. Hayat. 2012;18:67–78. [Google Scholar]
- 12.Black P, Boore J, Parahoo K. The effect of nurse-facilitated family participation in the psychological care of the critically ill patient. J Adv Nurs. 2010;67:1091–101. doi: 10.1111/j.1365-2648.2010.05558.x. [DOI] [PubMed] [Google Scholar]
- 13.Daly BJ, Douglas SL, O'Toole E, Gordon NH, Hejal R, Peerless J, et al. Effectiveness trial of an intensive communication structure for families of long-stay ICU patients. Chest J. 2010;138:1340–48. doi: 10.1378/chest.10-0292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ely EW, Inouye SK, Bernard GR, Gordon S, Francis J, May L, et al. Delirium in mechanically ventilated patients validity and reliability of the confusion assessment method for the Intensive care unit (CAM-ICU) JAMA. 2001;286:2703–10. doi: 10.1001/jama.286.21.2703. [DOI] [PubMed] [Google Scholar]
- 15.Treece N, Patsy D. Communication in the intensive care unit about the end of life. AACN Adv Crit Care. 2007;18:414. doi: 10.1097/01.AACN.0000298633.38029.2d. [DOI] [PubMed] [Google Scholar]
- 16.Stevenson CH. Patient and person empowering interpersonal relationships in nursing. Elsevier: 2004. p. 5. [Google Scholar]
- 17.Gagnon P, Charbonnea C. Delirium in advanced cancer: A psycho educational intervention for family care giver. J Palliative Care. 2008;18:253–61. [PubMed] [Google Scholar]
- 18.Gay EB, Pronovost PJ, Bassett RD, Nelson JE. The intensive care unit family meeting: making it happen. Journal of critical care. 2009;24:e1-629. e12. doi: 10.1016/j.jcrc.2008.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Curtis JR, Ciechanowski PS, Downey L, Gold J, Nielsen EL, Shannon SE, et al. Development and evaluation of an interprofessional communication intervention to improve family outcomes in the ICU. Contemporary Clinical Trials. 2012;33:1245–54. doi: 10.1016/j.cct.2012.06.010. [DOI] [PMC free article] [PubMed] [Google Scholar]