

Abstract
The long-term dialysis therapy for end-stage renal disease takes a heavy toll of quality of life of the patient. Several factors such as fatigue and decreased physical capability, impaired social and mental functioning, contribute to this forlorn state. To meld maintenance dialysis treatment with a regular employment can be a serious test. A cross-sectional study of employment of patients on hemodialysis and peritoneal dialysis in a state government tertiary institute in South India was performed between June 2015 and December 2015. Patients who completed 3 months of regular dialysis were only included in the study. The number of patients on hemodialysis was 157 and on peritoneal dialysis was 69. The employment status before the initiation of dialysis was 60% (93 out of 155) and 63.7% (44 out of 69) in hemodialysis and peritoneal dialysis, respectively. After initiation, the loss of employment was observed in 44% (41 out of 93) in hemodialysis and 51.2% (26 out of 44) in peritoneal dialysis (P = 0.2604). Even though there was fall of absolute number of job holders in both the blue and white collar jobs, the proportion of jobholders in the white collar job holders improved. On univariate analysis, the factors which influenced the loss of employment were males, age between 50 and 60 years, number of comorbidities >2, illiteracy and blue collar versus white collar job before the initiation of dialysis. The majority of patients had the scores above 80 on Karnofsky performance scale and the majority belonged upper and middle classes than lower classes on modified Kuppuswamy's socioeconomic status scale; however, the loss of employment was also disproportionately high. There appeared a substantial difference in the attitude of the patients toward the employment. There was no difference between hemodialysis and peritoneal dialysis in the loss of employment of our patients.
Keywords: Blue collar job, employment, hemodialysis, peritoneal dialysis, white collar job
Introduction
The long-term dialysis therapy for end-stage renal disease (ESRD) takes a heavy toll of quality of life of the patient. Several factors such as fatigue and decreased physical capability, impaired social and mental functioning, contribute to this forlorn state.[1,2,3,4] To meld maintenance dialysis treatment with a regular employment can be a serious test. It is, therefore, not astonishing that the frequency of employed long-term dialysis patients is low at 10%–30%.[4,5,6,7] The factors associated with increased employment after initiation of dialysis have been studied before,[8] but the data on employment rates of the ESRD patients on dialysis from India are exiguous. The aim of this study was to investigate the employment rates in maintenance dialysis patients.
Materials and Methods
A cross-sectional study of hemodialysis and peritoneal dialysis patients in a state government tertiary institute in South India was performed between June 2015 and December 2015. Patients who completed 3 months of regular dialysis were only included in the study. These patients were not on waitlist for renal transplantation. The data were collected in a pro forma by eliciting information from patients. A written consent was taken from the patient before collecting data. A few definitions utilized in the study were:
Unemployed: Persons outside the labor force – homemakers, students, those on disability pension, retired, or unknown. These groups of patients were not included in the study
Blue collar job: Person who performs manual labor or physical work
White collar job: A person who performs professional, managerial, or administrative work
Literate: Able to read and write.
The data collected included, patient's name, age, sex, literacy, etiology of ESRD, modality of dialysis, start date of renal replacement therapy (RRT), the presence of comorbid conditions, and the employment. Patients who changed from hemodialysis to peritoneal dialysis and vice versa for medical indication were not included in the study. All patients' dialysis was funded by government, quasi-government and insurance agencies.
The scales employed were:
Socioeconomic status (SES) by modified Kuppuswamy socioeconomic status scale:[9] SES is one of the most important social determinants of health and disease. The most widely used scale for urban populations is modified Kuppuswamy's socioeconomic status scale. This scale consists educational, occupational, and economic criteria
Performance of the patient by Karnofsky performance scale:[10] The performance status assessment is devised to quantify cancer patients' general well-being and activities of daily life. It is also used in randomized controlled trials as a measure of quality of life.
Statistics
The data generated included the continuous variables such as age of the patient, Karnofsky performance scale, modified Kuppuswamy's socioeconomic status scale, and comorbidities, and the categorical variables such as the sex of the patient and the educational status. The tests of significance used were, for the continuous variables, Student's t-test and for the categorical variables, Chi-square test.
Results
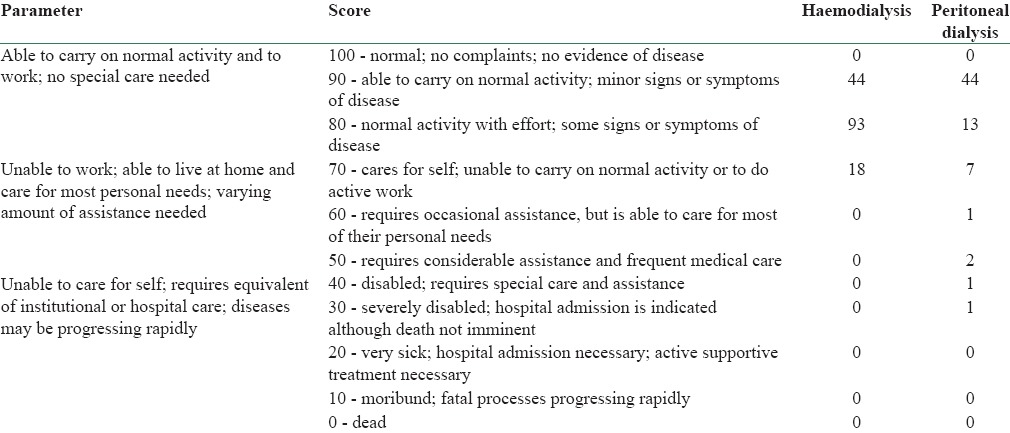
A cross-sectional study of hemodialysis and peritoneal dialysis patients who finished 3 months on dialysis was done. The study was done in a state government tertiary institute in South India between June 2015 and December 2015. Our institute has 37 hemodialysis stations. Patients were provided hemodialysis based on waitlist. The number of patients on hemodialysis was 157 and on peritoneal dialysis was 69. The patient characteristics is given in the Table 1. The comorbid conditions are mentioned in Table 2. All patients were from an urban area. The SES by modified Kuppuswamy's socioeconomic status scale is given in Table 3. Table 4 shows the Karnofsky performance scale of the patients.
Table 1.
Characteristics of patients
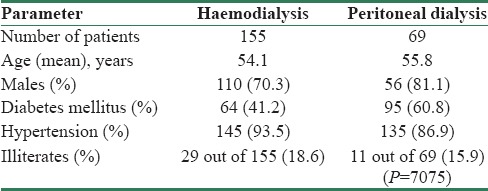
Table 2.
Comorbid conditions
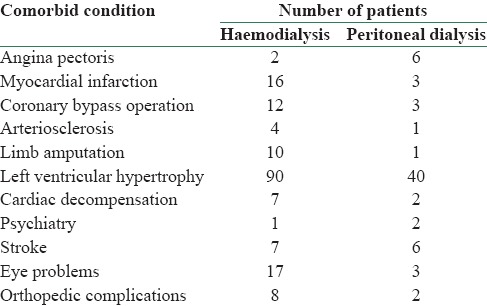
Table 3.
Modified Kuppuswamy's socioeconomic status scale
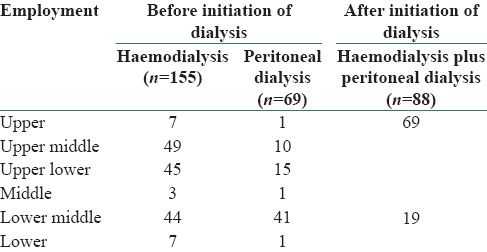
Table 4.
Karnofsky performance scale
The employment status before initiation of dialysis was 60% (93 out of 155) and 63.7% (44 out of 69) in hemodialysis and peritoneal dialysis, respectively [Table 5]. The major reasons for unemployment before initiation of dialysis were dependence on their life partners and off springs. In the former group, it was male patients dependent on income of the lady of the house. After initiation, the loss of employment was observed in 44% (41 out of 93) in hemodialysis and 51.2% (26 out of 44) in peritoneal dialysis (P = 0.2604) [Tables 6 and 7]. On comparison between continuous ambulatory peritoneal dialysis (CAPD) and automated peritoneal dialysis (APD), the loss of employment after initiation of dialysis was observed in 69.6% (23 out of 33) in CAPD and 27.2% (3 out 11) in APD (P = 0.0132) [Table 7]. The loss of blue collar job after initiation of dialysis was observed in 78.0% (32 out of 41) in hemodialysis and 74.0% (20 out of 26) in peritoneal dialysis (P = 1.000). Out of twenty patients on peritoneal dialysis who lost the blue collar job, three were on APD and seventeen were on CAPD. The loss of white collar job after initiation of dialysis was observed in 22.0% (9 out of 38) in hemodialysis and 35.2% (6 out of 17) in peritoneal dialysis (P = 0. 5135). All six peritoneal dialysis patients were on CAPD. Even though there was fall of absolute number of job holders in both the blue and white collar jobs, the proportion of job holders in the white collar job holders improved [Tables 5 and 6].
Table 5.
Employment before initiation of dialysis

Table 6.
Employment after initiation of dialysis

Table 7.
Employment before and after dialysis

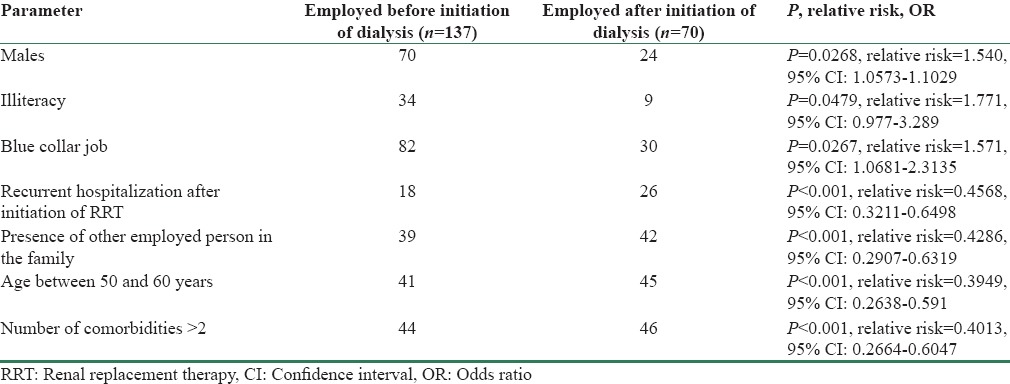
On univariate analysis [Table 8], the factors which influenced the loss of employment were males (P = 0.0320, relative risk = 1.251; 95% confidence interval [CI]: 1.046–1.495), age between 50 and 60 years (P = 0.0436, relative risk = 1.354, 95% CI: 1.029–1.781), number of comorbidities >2 (P = 0.0289, relative risk = 1.636, 95% CI: 0.9911–2.702), illiteracy (P < 0.0001, relative risk = 0.5504, 95% CI: 0.4365–0.6941), blue collar versus white collar job before the initiation of dialysis (P = 0.0268, relative risk = 1.397, 95% CI: 1.031–1.892), history of recurrent hospitalization after initiation of RRT (P = 0.0168, relative risk = 1.117, 95% CI: 1.0–1.782), presence of other employed person in the family (P = 0.0218, relative risk = 1.314, 95% CI: 1.09–2.02). There was no significant influence of other age groups, specific education status, hemodialysis versus peritoneal dialysis, and CAPD versus APD. As all patients' dialysis was funded by government, quasi-government and insurance agencies, the funding for dialysis was not considered for univariate analysis.
Table 8.
Factors which influenced the loss of employment
Discussion
The employment in ESRD patients before initiation of dialysis was 61.1%. The employment rates declined to 29.9% after initiation of dialysis [Table 7]. We included the patients who completed 3 months of dialysis at our institute. No study from India published data on employment rates before the initiation of dialysis. The data from other countries suggested that the large proportions of ESRD patients were unemployed before the initiation of dialysis. It was given as 20% and 35%.[11,12] Our institute is a part of an organization which runs several educational institutes, temples, orphanages, and allied health services. The employees and dependents of this organization form the major group of our patients. Hence, the possibility of being employed was high among our patients.
Only for a minority of unemployed patients before dialysis were likely to become employed after the initiation of dialysis. The dialysis creates a whole range of obstacles to employment which included health-related barriers, economic barriers, and attitudinal barriers.[13] It was, therefore, prudent to direct the efforts to prevent unemployment after initiation of dialysis.
The predialysis educational level and employment status of the patient emerged as strong independent predictors of employment for patients after the initiation of dialysis. Illiteracy (P < 0.0001, relative risk = 0.5504, 95% CI: 0.4365–0.6941) and blue collar versus white collar job before the initiation of dialysis (P = 0.0268, relative risk = 1.397, 95% CI: 1.031–1.892) were the strong predictors of the loss of employment after the initiation of dialysis. The explanations for these findings seem fairly simple, i.e., more educated and/or white collar workers were suited to have more employment opportunities, to receive salaries that exceed disability incomes, to have insurance benefits available to them, to have employment that require less heavy physical labor, and to have employment that lend themselves to flexible work hours for accommodating dialysis scheduling. For the less-educated and blue collar workers, an opposite set of circumstances works against them. They are lack of openings to shift to less labor-intensive works, obdurate work hours, and inability to obtain social support because of the marginalized status.
The other predictors of the loss of employment after initiation of dialysis were male sex, age between 50 and 60 years, and number of comorbidities >2. This had to be read in association with the Karnofsky performance scale and modified Kuppuswamy's socioeconomic status scale of our patients. The majority of patients had the scores above 80 on Karnofsky Performance Scale [Table 4] and the majority belonged upper and middle classes than lower classes on modified Kuppuswamy's socioeconomic status scale; however, the loss of employment was also disproportionately high. That means there was no significant difference found between working and nonworking patients with regard to the objective health indicators such as the Karnofsky performance scale and modified Kuppuswamy's socioeconomic status scale. The substantial differences should have been in attitude of the patients toward the employment. The patients who were not employed seemed to “perceive” their health as precarious and a serious problem vis-a-vis employment even though it was not so. We have not explored the impact of attitudes of patients on return to employment. It had been suggested that the employment status was found to relate in a significantly positive manner to patients' perceptions of others' expectations regarding their ability to work[14] and the return to employment might be improved if providers are themselves convinced that ESRD and employment are compatible and if providers also are able to convince patients as well.[15]
There was no difference between hemodialysis and peritoneal dialysis in the loss of employment of our patients. This is against the impression that the peritoneal dialysis offers freedom from the treatment schedules and possibility for out-of-work-hours dialysis, making it a suitable option for employed patients. Finnish Registry for Kidney Diseases reported that a functioning transplant, APD therapy, and home hemodialysis therapy were connected with a higher employment rate in patients with ESRD compared with in-center HD therapy. The same registry reported that the employment rate of patients on CAPD therapy was not higher compared with patients on in-center HD therapy. In another study[7] also, the treatment modality (hemodialysis vs. peritoneal dialysis) did not predict loss of work and most patients who were employed before starting dialysis therapy were able to maintain their work.
It is axiomatic to quote that the proof of pudding is in eating to express the outcome acceptability as the deciding parameter of a situation. In this context, the general trend from many parts of the world mentions the inability to bring back the patients of ESRD to productivity through employment despite providing support in the form of dialysis facility. Thus, bringing into the light, that in addition to an active participation of nephrologists, the involvement of the personnel from the social organizations is the need of hour. An encompassing and holistic support from the government and the non-governmental organizations is mandatory in this humongous challenge.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Merkus MP, Jager KJ, Dekker FW, de Haan RJ, Boeschoten EW, Krediet RT. Physical symptoms and quality of life in patients on chronic dialysis: Results of The Netherlands Cooperative Study on Adequacy of Dialysis (NECOSAD) Nephrol Dial Transplant. 1999;14:1163–70. doi: 10.1093/ndt/14.5.1163. [DOI] [PubMed] [Google Scholar]
- 2.Merkus MP, Jager KJ, Dekker FW, Boeschoten EW, Stevens P, Krediet RT. Quality of life in patients on chronic dialysis: Self-assessment 3 months after the start of treatment. The NECOSAD Study Group. Am J Kidney Dis. 1997;29:584–92. doi: 10.1016/s0272-6386(97)90342-5. [DOI] [PubMed] [Google Scholar]
- 3.Moore GE, Parsons DB, Stray-Gundersen J, Painter PL, Brinker KR, Mitchell JH. Uremic myopathy limits aerobic capacity in hemodialysis patients. Am J Kidney Dis. 1993;22:277–87. doi: 10.1016/s0272-6386(12)70319-0. [DOI] [PubMed] [Google Scholar]
- 4.Molsted S, Aadahl M, Schou L, Eidemak I. Self-rated health and employment status in chronic haemodialysis patients. Scand J Urol Nephrol. 2004;38:174–8. doi: 10.1080/00365590310020015. [DOI] [PubMed] [Google Scholar]
- 5.Kutner NG, Brogan D, Fielding B. Employment status and ability to work among working-age chronic dialysis patients. Am J Nephrol. 1991;11:334–40. doi: 10.1159/000168333. [DOI] [PubMed] [Google Scholar]
- 6.Kutner N, Bowles T, Zhang R, Huang Y, Pastan S. Dialysis facility characteristics and variation in employment rates: A national study. Clin J Am Soc Nephrol. 2008;3:111–6. doi: 10.2215/CJN.02990707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.van Manen JG, Korevaar JC, Dekker FW, Reuselaars MC, Boeschoten EW, Krediet RT. NECOSAD Study Group. Netherlands Cooperative Study on Adequacy of Dialysis. Changes in employment status in end-stage renal disease patients during their first year of dialysis. Perit Dial Int. 2001;21:595–601. [PubMed] [Google Scholar]
- 8.Helanterä I, Haapio M, Koskinen P, Grönhagen-Riska C, Finne P. Employment of patients receiving maintenance dialysis and after kidney transplant: A cross-sectional study from Finland. Am J Kidney Dis. 2012;59:700–6. doi: 10.1053/j.ajkd.2011.08.025. [DOI] [PubMed] [Google Scholar]
- 9.Mishra D, Singh HP. Kuppuswamy's socioeconomic status scale – A revision. Indian J Pediatr. 2003;70:273–4. doi: 10.1007/BF02725598. [DOI] [PubMed] [Google Scholar]
- 10.Altilio T, Otis-Green S. Oxford Textbook of Palliative Medicine. Oxford: Oxford University Press; 1993. p. 109. [Google Scholar]
- 11.Holley JL, Nespor S. An analysis of factors affecting employment of chronic dialysis patients. Am J Kidney Dis. 1994;23:681–5. doi: 10.1016/s0272-6386(12)70278-0. [DOI] [PubMed] [Google Scholar]
- 12.IV. Patient characteristics at the start of ESRD: Data from the HCFA medical evidence form. Am J Kidney Dis. 1999;34(2 Suppl 1):S63–73. doi: 10.1053/AJKD034s00063. [DOI] [PubMed] [Google Scholar]
- 13.Curtin RB, Oberley ET, Sacksteder P, Friedman A. Differences between employed and nonemployed dialysis patients. Am J Kidney Dis. 1996;27:533–40. doi: 10.1016/s0272-6386(96)90164-x. [DOI] [PubMed] [Google Scholar]
- 14.Antonoff A, Mallinger M. Vocational rehabilitation: Limitations and resistance of renal patients. Perspectives. 1990;11:43–53. [Google Scholar]
- 15.Rasgon S, Schwankovsky L, James-Rogers A, Widrow L, Glick J, Butts E. An intervention for employment maintenance among blue-collar workers with end-stage renal disease. Am J Kidney Dis. 1993;22:403–12. doi: 10.1016/s0272-6386(12)70143-9. [DOI] [PubMed] [Google Scholar]