

Abstract
The hand is a complex anatomical structure with the component bones susceptible to a combination of environmental and genetic factors that may affect the bone length and width. The alterations may involve a single bone or specific group of bones. The metacarpophalangeal pattern profile (MCPP) developed by Poznanski, Garn, and others (Poznanski et al. Birth Defects VIII (5): 125–131, 1972) is a graphic representation of the relative lengthening and shortening of the 19 tubular bones of the hand useful for diagnosis, comparison of dissimilar patients, and gene carrier detection. The profile hand bone measurements are derived from posteroanterior hand radiographs and are standardized for age and sex. Specific profiles have been developed for several syndromes. Therefore, MCPP analysis has developed from a method of describing changes in the hand to a technique useful in assigning a diagnosis to a specific syndrome and evaluation of skeletal development. The current status of MCPP analysis in clinical genetics, particularly with the Prader-Labhart-Willi and Sotos syndromes, is discussed.
Keywords: Prader-Labhart-Willi syndrome, Sotos syndrome, Discriminant analysis, Correlation studies
Metacarpophalangeal pattern profile analysis (MCPP) is an application of an anthropometric technique that has been utilized increasingly in clinical genetics to evaluate individuals with a variety of congenital malformation syndromes. A number of biological anthropologists were instrumental in the development and application of this method (Garn et al., 1972). More recently a number of investigators have broadened the analysis of hand bone lengths by applying multivariate statistical methods in an effort to provide an additional diagnostic tool for certain disorders (Landry et al., 1979; Butler et al., 1982).
The hand is a complex anatomical structure. There are 28 component bones susceptible to a combination of factors (e.g., environmental and genetic) that may alter length and width. The alterations may involve a single bone or specific group of bones in a digit (e.g., Holt-Oram syndrome) or within a row of bones such as the metacarpals (Proger et al., 1968; Poznanski et al., 1970). There are syndromes in which non-homologous segments of the hand are affected and others characterized by size reduction of a single segment such as the middle phalanx of the fifth digit (Garn et al., 1972).
Investigators in the past have attempted to examine specific hand bones in syndromes, for example, Down syndrome and the “metacarpal sign” or gradient of metacarpal shortening in Turner syndrome described by Archibald et al. (1959). Ratios of length and width of major hand bones have also been examined in Marfan syndrome and other connective tissue disorders (Parish, 1967).
These methods were helpful in certain conditions, but there was a need to describe the overall relationship of the hand bone lengths. Subtle changes may be detected by examining the overall relationship that may be overlooked in the routine radiological hand examination. An MCPP was developed by Garn et al. (1972) and Poznanski et al. (1972a) as an approach to the above problems. MCPP analysis is a graphic method of depicting lengthening and shortening of the tubular hand bones and their relationship to one another (Poznanski et al., 1972a). The hand bone lengths used for the profile are measured from posteroanterior radiographs and converted to Z scores from established bone length standards for age and sex (Garn et al., 1972; Poznanski, 1974). MCPP analysis as a tool for diagnosis has been applied to several syndromes as represented by published profiles in Table 1. Several of these syndromes have specific patterns that are easily recognized, while other patterns are not as striking and detailed statistical analysis is required before clinical application.
TABLE 1.
Syndromes analyzed for metacarpophalangeal pattern profile
We have recently derived a method of MCPP analysis for the Prader-Labhart-Willi and Sotos syndromes to evaluate the potential of this technique to serve as an additional diagnostic criterion, particularly for the younger patient.
MATERIALS AND METHODS
Posteroanterior hand radiographs were obtained for 38 individuals (23 males and 15 females with an age range from 0.2 to 38.5 years and a mean age of 12.2 years) whose clinical features (neonatal hypotonia, neonatal feeding problems, delayed developmental milestones, mental retardation, obesity [87% of individuals with triceps skinfolds > 85th percentile], small hands and feet, hypogonadism and chromosome 15 deletions [54% of individuals]) were consistent with the diagnosis of Prader-Labhart-Willi syndrome (PLWS). Therefore, two PLWS groups were identified, with 20 individuals and the chromosome 15 deletion in one group and 18 individuals with normal chromosomes in the second group.
Posteroanterior hand radiographs were also obtained for 16 individuals whose clinical features (large size at birth, large hands and feet, macrocephaly, downslanting palpebral fissures, hypertelorism, poor coordination, and variable mental retardation) were consistent with the diagnosis of Sotos syndrome. This group included 11 males and 5 females ranging in age from 0.8 to 13.8 years, with a mean age of 5.4 years.
The metacarpophalangeal bone lengths of each subject were measured to the nearest 0.1 mm with a vernier caliper and compared to bone length standards appropriate for age and sex (Garn et al., 1972; Poznanski, 1974). Through these comparisons, Z score values for the 19 bones of each subject were obtained (Z score = observed bone length minus mean bone length divided by the standard deviation associated with the particular age and sex of normal standards). The MCPP for a given individual is, therefore, the set of 19 Z scores, which may be plotted on a graph or subjected to various statistical methods for study and comparison with the MCPP of other individuals or groups of individuals.
A mean pattern profile, based on the average Z score for each bone of the individual, was derived. The pattern of each individual was compared to the group mean pattern via a correlation program which produces Pearsonian r values.
A forward stepwise method of discriminant analysis was performed on the 19 Z scores and age for the individuals with Prader-Labhart-Willi or Sotos syndromes and a control group of 41 normal subjects whose hand radiographs were randomly obtained from the records of Indiana University School of Dentistry, Department of Orthodontics. The sample of 41 control subjects included 17 males and 24 females, with an age range of 9.5 to 18 years and a mean age equal to 13.1 years. The purpose of applying the discriminant method was to discover whether a smaller combination of variables would clearly separate groups of affected individuals from normal subjects, thus providing an easily applied diagnostic tool for the clinician evaluating a patient suspected of having one of these disorders.
RESULTS
Figure 1A presents the mean pattern profile based on the 38 individuals with Prader-Labhart-Willi syndrome. It is essentially flat with no obvious vertical deviations. The mean Z scores fall between −1.7 and −2.3. Therefore, each hand bone was significantly shorter than normal at the 5% level. From the profile, it appears that the distal hand bones are shorter than the proximal bones. The mean Z scores of the two groups of PLWS individuals based on the chromosome results (deletion or nondeletion) showed two separate profiles (Fig. 1B). An obvious separation of the two profiles exists when comparing the metacarpals, but there is overlap for the remaining bones.
Fig. 1.
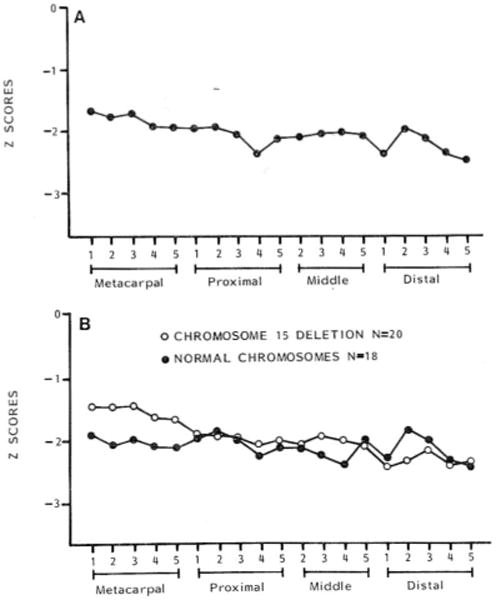
A. Mean metacarpophalangeal pattern profile produced from the individual hand profiles of 38 Prader-Labhart-Willi syndrome patients with and without the chromosome deletion. B. Mean metacarpophalangeal pattern profile for chromosome deletion (N = 20) and nondeletion (N = 18) Prader-Labhart-Willi syndrome individuals.
The Pearsonian r test to assess similarity between the individual patterns and their group mean reveal 14 of 20 members of the deletion chromosome group and seven of 18 nondeletion members with a significant positive correlation at the 5% level. Thus, the deletion chromosome group appears more homogeneous, which contrasts with the heterogeneity of the nondeletion group.
A stepwise discriminant analysis of all 38 PLWS and 41 control individuals resulted in a correct classification rate of 96.2%. This discriminant function was based on three of the 19 hand bones plus age. The three MCPP variables in the discriminant function were Z scores representing (1) the fifth distal phalanx, (2) the fifth middle phalanx, and (3) the fifth metacarpal. Therefore, all of the discriminating variables between the control and PLWS individuals were of the fifth finger.
The mean pattern profile based on the 16 individuals with Sotos syndrome contains one major peak in the proximal phalangeal area (Butler et al., 1985). The mean Z scores fall between 1.5 and 3.5. Any Z score of 0.5 or higher is significantly different from zero; therefore, each hand bone is significantly longer than the mean for normal individuals at the 5% level. From the profile, it appears that the distal hand bones are relatively short compared with the proximal bones. Next, the correlation program was used to assess similarity between the mean pattern and the pattern of each of the 16 individuals. A significant positive correlation was found in 12 of the 16 individuals.
Discriminant analysis of the normal and Sotos syndrome cases resulted in a discriminant function based on two of the 19 MCPP variables plus age (Table 2). In the discriminant analysis, patients with Sotos syndrome were distinguished from the normal control group at an overall correct classification rate of 100% for our sample.
TABLE 2.
Discriminant analysis for MCPP Z score variables1
| Variables in function | Discriminant loading | Discriminant coefficient |
|---|---|---|
| 3rd proximal phalanx | −0.68 | −1.16 |
| 2nd middle phalanx | −0.42 | 0.60 |
| Age (years) | 0.69 | 0.65 |
Sotos syndrome (N = 16) vs. normal (N = 41).
DISCUSSION
The small and large hand sizes in Prader-Labhart-Willi and Sotos syndromes, respectively, are well known clinically. The mean pattern profiles based on the individuals we have studied confirm these impressions in quantitative terms.
Hand pattern profiles should not change with age, although the influence of certain factors (e.g., malnutrition) on the hand profile is not known (Hayes and Say, 1977). Thus metacarpophalangeal pattern profiles of affected individuals have shown good consistency from one age to another in normal individuals and in subjects with recognized syndromes (Hayes and Say, 1977).
The results of discriminant analysis suggest that effective classification of PLWS and Sotos syndrome indivduals compared with normal individuals on the basis of MCPP data is possible. These observations suggest the potential of this multivariate statistical method in the evaluation of patients in whom either Prader-Labhart-Willi or Sotos syndromes are suspected. The advantage of discriminant analysis is the possibility that group separation will be maximized on the basis of two to three hand bone lengths alone, thus providing all the information needed to separate affecteds from normal. A suspected patient’s D score value for these variables could then be entered into the linear equation to determine whether the individual’s discriminant score falls within the range of scores for affected individuals. Poznanski (1984) has emphasized the superiority of discriminant analysis in correctly classifying affected and normal individuals as compared with correlation studies. Similarly he stressed the potential of multivariate statistical methods for improving the recognition of similarities and differences between patterns.
Discriminant analysis was also used by Landry et al. (1979) to separate hand patterns among several syndromes (Down, Turner, achondroplasia, and normal). Their analysis of the MCPP data resulted in approximately 20% improvement in classification over the use of correlation studies (Landry et al., 1979). Their results suggested that certain congenital malformation syndromes may be grouped with good accuracy on the basis of MCPP data, and encouraged the development of an automated system for pattern recognition in the diagnosis of certain syndromes.
Discriminant analyses of MCPP data of other syndromes have been undertaken. Kaler et al. (1982) examined MCPP data from individuals with Crouzon syndrome with a stepwise forward discriminant analysis program. They found that these individuals could be discriminated from a normal control population with a correct classification rate of 88.3% by the use of only three of the 19 MCPP variables. Although the Crouzon syndrome hand is considered radiologically normal, subtle differences were identified via discriminant analysis of MCPP data that may have been overlooked with correlation studies.
Not only may MCPP analysis be used as a diagnostic tool, but it may have value in nosology. Kaler et al. (1982) found high correlations (+0.69 to +0.88) when comparing mean pattern profiles of individuals with Crouzon, Pfeiffer, and Carpenter syndromes. On the basis of the hand profile studies, they suggested there may be a common developmental mechanism, varying in extent, which acts on the hand skeleton in each of the three (Crouzon, Pfeiffer, and Carpenter) genetically distinct craniosynostosis syndromes.
The role of physical anthropologists such as Stanley Garn and others in the development and application of hand profiles should be emphasized. MCPP is an anthropometric method of demonstrated value in medical genetics, representing a salient example of the contribution that applied biological anthropology may lend to clinical medicine.
Acknowledgments
The authors wish to thank Drs. Rebecca Wappner, Bryan Hall, Patricia Bader, and Andree Walczak for allowing us to evaluate their patients. This research was supported by PHS-5T32 GM07468 (M.G.B.) and PHS-T32 DE07043 (F.J.M. and S.G.K.). The authors acknowledge use of the facilities of Computing Services, Indiana University-Purdue University at Indianapolis. An earlier version of this paper was presented in the symposium “Application of Anthropological Methods in Medical Genetics” on April 12, 1984 at the 53rd Annual Meeting of the American Association of Physical Anthropologists, Philadelphia. We thank Judy Copeland for expert preparation of the manuscript.
Contributor Information
MERLIN G. BUTLER, Division of Genetics, Department of Pediatrics, Vanderbilt University School of Medicine, Nashville, Tennesse 37232
F. JOHN MEANEY, Department of Medical Genetics, Indiana University School of Medicine, and Genetic Diseases Section, Division of Maternal and Child Health, Indiana State Board of Health, Indianapolis, Indiana 46206.
STEPHEN G. KALER, Department of Pediatrics, Loyola University School of Medicine, Chicago, Illinois
LITERATURE CITED
- Archibald RM, Finby N, DeVito F. Endocrine significance of short metacarpals. J Clin Endocrinol Metab. 1959;19:1312–1322. doi: 10.1210/jcem-19-10-1312. [DOI] [PubMed] [Google Scholar]
- Arias S, Zimmer E. 2nd International Congress of Auxology. La Habanna, Cuba: 1979. p. 161. Abstract. [Google Scholar]
- Arias S, Penchaszadeh VB, Pinto-Cisternas J, Larrauri S. The IVIC syndrome: A new autosomal dominant complex pleiotropic syndrome with radial ray hypoplasia, hearing impairment, external ophthalmoplegia and thrombocytopenia. Am J Med Genet. 1980;6 doi: 10.1002/ajmg.1320060105. 1980. [DOI] [PubMed] [Google Scholar]
- Arias S, Rodriguez A, Segovia J, Zimmer E. El perfil metacarpofalangico por edad y sexo en el venezolano y en la osteochondrodisplasia tipo Irapa. Acta Cient Venz. 1979;2(29 Suppl):109. [Google Scholar]
- Butler MG, Meaney FJ. Metacarpophalangeal pattern profile analysis in Prader-Willi syndrome: A follow-up report on 38 cases. Clin Genet. 1985;28:27–30. doi: 10.1111/j.1399-0004.1985.tb01213.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Butler MG, Kaler SG, Yu PL, Meaney FJ. Metacarpophalangeal pattern profile analysis in Prader-Willi syndrome. Clin Genet. 1982;22:315–320. doi: 10.1111/j.1399-0004.1982.tb01846.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Butler MG, Meaney FJ, Kittur S, Hersh JH, Hornstein L. Metacarpophalangeal pattern profile analysis in Sotos syndrome. Am J Med Genet. 1985;20:625–629. doi: 10.1002/ajmg.1320200408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dijkstra PF. Analysis of metacarpophalangeal pattern profiles. Fortschr Rontgenstr. 1983;139:158–159. doi: 10.1055/s-2008-1055862. [DOI] [PubMed] [Google Scholar]
- Escobar V, Bixler D. The acrocephalosyndactyly syndromes: A metacarpophalangeal pattern profile analysis. Clin Genet. 1977;11:295–305. doi: 10.1111/j.1399-0004.1977.tb01316.x. [DOI] [PubMed] [Google Scholar]
- Felman AH, Frias JL. The trichorhinophalangeal syndrome: Study of 16 patients in one family. Am J Roentgenol. 1977;129:631–638. doi: 10.2214/ajr.129.4.631. [DOI] [PubMed] [Google Scholar]
- Fenger K, Niebuhr E. Measurements on hand radiographs from 32 cri-du-chat probands. Pediatr Radiol. 1978;129:137–141. doi: 10.1148/129.1.137. [DOI] [PubMed] [Google Scholar]
- Gall JC, Stern AM, Poznanski AK. Otopalato-digital syndrome: Comparison of clinical and radiographic manifestations in males and females. Am J Hum Genet. 1972;24:24–36. [PMC free article] [PubMed] [Google Scholar]
- Garn SM, Hertzog KP, Poznanski AK, Nagy JM. Metacarpophalangeal length in the evaluation of skeletal malformation. Radiology. 1972;105:375–381. doi: 10.1148/105.2.375. [DOI] [PubMed] [Google Scholar]
- Giedion A, Prader A. Hand-foot-uterus (HFU) syndrome with hypospadias: The hand-foot-genital (HFG) syndrome. Pediatr Radiol. 1976;4:96–102. doi: 10.1007/BF00973951. [DOI] [PubMed] [Google Scholar]
- Halal F. Male to male transmission of cerebral gigantism. Am J Med Genet. 1982;12:411–419. doi: 10.1002/ajmg.1320120405. [DOI] [PubMed] [Google Scholar]
- Halal F, Preus M. The hand profile in de Lange syndrome: Diagnostic criteria. Am J Med Genet. 1979;3:317–323. doi: 10.1002/ajmg.1320030402. [DOI] [PubMed] [Google Scholar]
- Hayes M, Say B. Hand pattern profile analysis (HPPA) Clin Pediatr. 1977;16:988–991. doi: 10.1177/000992287701601105. [DOI] [PubMed] [Google Scholar]
- Kaler SG, Bixler D, Yu PL. Metacarpophalangeal pattern profile in ACPS type II (Carpenter syndrome) J Craniof Genet Dev Biol. 1981;1:373–381. [PubMed] [Google Scholar]
- Kaler SG, Bixler D, Yu PL. Radiographic hand abnormalities in fifteen cases of Crouzon syndrome. J Craniof Genet Dev Bio. 1982;2:205–213. [PubMed] [Google Scholar]
- Landry DJ, Vanhoutee JJ, Raeside DE. The application of pattern recognition techniques in the analysis of metacarpophalangeal lengths. Invest Radiol. 1979;14:288–294. doi: 10.1097/00004424-197907000-00004. [DOI] [PubMed] [Google Scholar]
- Miura T. Congenital familial hypoplastic thumb associated with congenital amputation of the toe. J Hand Surg. 1984;9A:420–422. doi: 10.1016/s0363-5023(84)80235-x. [DOI] [PubMed] [Google Scholar]
- Mooij PD, Dalinghaus-Nienhuis AJ, Wijnands MC, van der Kamp JJP. Genetic counseling in pseudopseudohypoparathyroidism. Prog Clin Biol Res. 1985;200:277–281. [PubMed] [Google Scholar]
- Parish JG. Skeletal hand charts in inherited connective tissue disease. J Med Genet. 1967;4:227–238. doi: 10.1136/jmg.4.4.227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Park E. Radiological anthropometry of the hand in Turner’s syndrome. Am J Phys Anthropol. 1977;46:463–468. doi: 10.1002/ajpa.1330460312. [DOI] [PubMed] [Google Scholar]
- Peeters FLM. Radiological manifestations of the Cornelia de Lange syndrome. Pediatr Radiol. 1975;3:41–46. doi: 10.1007/BF00973365. [DOI] [PubMed] [Google Scholar]
- Poznanski AK. The Hand in Radiological Diagnosis. Philadelphia: W.B. Saunders; 1974. [Google Scholar]
- Poznanski AK. The Hand in Radiological Diagnosis. Philadelphia: W.B. Saunders; 1984. [Google Scholar]
- Poznanski AK, Gall JC, Stern AM. Skeletal manifestations of the Holt-Oram syndrome. Radiology. 1970;94:45–53. doi: 10.1148/10.1148/94.1.45. [DOI] [PubMed] [Google Scholar]
- Poznanski AK, Garn SM, Gall JC, Stern AM. Metacarpophalangeal pattern profiles in the evaluation of skeletal malformations. Radiology. 1972a;104:1–11. doi: 10.1148/104.1.1. [DOI] [PubMed] [Google Scholar]
- Poznanski AK, Garn SM, Gall JC, Stern AM. Objective evaluation of the hand in the Holt-Oram syndrome. Birth Defects. 1972b;VIII(5):125–131. [Google Scholar]
- Poznanski AK, MacPherson RI, Gorlin RJ, Garn SM, Nagy JM, Gall JC, Stern AM, Dijkman DJ. The hand in the otopalato-digital syndrome. Ann Radiol. 1973;16:203–209. [Google Scholar]
- Poznanski AK, Schmickel RD, Harper HAS. The hand in the trichorhinophalangeal syndrome. Birth Defects. 1974;XIX(9):209–219. [PubMed] [Google Scholar]
- Poznanski AK, Werder EA, Giedion A. The pattern of shortening of the bones of the hand in PHP and PPHP: A comparison with brachdactyly E, Turner syndrome and acrodysostosis. Radiology. 1977;123:707–718. doi: 10.1148/123.3.707. [DOI] [PubMed] [Google Scholar]
- Proger L, Steinbach HL, Moskowitz P. Roentgenographic abnormalities in phenotypic females with gonadal dysgenesis: A comparison of chromatin positive patients and chromatin negative patients. Am J Roentgenol. 1968;104:899–919. doi: 10.2214/ajr.104.4.899. [DOI] [PubMed] [Google Scholar]
- Robinow M, Chumlea WC. Standards for limb bone length ratios in children. Radiology. 1982;143:433–436. doi: 10.1148/radiology.143.2.7071345. [DOI] [PubMed] [Google Scholar]
- Say B, Barber N, Poznanski AK. Pattern profile analysis of the hand in trichorhinophalangeal syndrome. Pediatrics. 1977;59:123–128. [PubMed] [Google Scholar]
- Schinzel A. Trisomy 9p, a chromosome aberration with distinct radiologic findings. Radiology. 1979;130:125–133. doi: 10.1148/130.1.125. [DOI] [PubMed] [Google Scholar]
- Shprintzen RJ, Goldberg RB, Saenger P, Sidoti EJ. Male-to-male transmission of Robinow’s syndrome. Am J Dis Child. 1982;136:594–597. doi: 10.1001/archpedi.1982.03970430026007. [DOI] [PubMed] [Google Scholar]
- Young RS, Bader P, Palmer CG, Kaler SG, Hodes ME. Brief clinical report: Two children with denovo del (9p) Am J Med Genet. 1983;14:751–757. doi: 10.1002/ajmg.1320140416. [DOI] [PubMed] [Google Scholar]