

Abstract
Objective
Alcohol-impaired driving remains a serious public health concern despite the fact that drinking and driving risks are widely disseminated and well understood by the public. This research examines the motivational conditions under which providing risk information can exacerbate rather than decrease potential drinking drivers’ willingness to drive while impaired.
Method
In a hypothetical drinking and driving scenario, three studies investigated participants’ self-reported likelihood of drinking and driving as a function of (1) accessibility of information regarding risk associated with drinking and driving, (2) motivation to drive, and (3) need for cognitive closure (NFC).
Results
Across the three studies, participants self-reported a higher likelihood of driving when exposed to high-risk information (vs. low-risk information) if they were high in NFC. Risk information did decrease self-reported likelihood of driving among low NFC participants (Studies 1–3). Furthermore, this effect was exacerbated when the relevant motivation (to get home conveniently) was high (Study 3).
Conclusions
These findings have important implications for impaired-driving prevention efforts. They suggest that at least under some circumstances risk information can have unintended negative effects on drinking and driving decisions. The results are consistent with the motivated cognition literature, which suggests that people process and use information in a manner that supports their most accessible and important motivation despite potentially negative consequences.
Keywords: motivation, drinking and driving, risk information, need for closure
Alcohol-impaired driving remains a serious public health threat, contributing to over 12,000 fatalities each year (Stahre, Roeber, Kanny, Brewer, & Zhang, 2014). Although some sanctions (e.g., ignition interlock, incarceration) attempt to physically prevent individuals from drinking and driving, the majority of prevention efforts attempt to influence the decision-making of potential drinking drivers through information and education that disseminate the risks of drinking and driving. The underlying assumption of these efforts is that informing people that drinking and driving elevates their risk of very serious consequences (i.e., crash or arrest) might motivate them to behave differently (Ross, 1984).
Indeed, this assumption is rooted in theories of behavioral decision making (Azjen, 1985; Brown, Goldman, & Christiansen, 1985; Fishbein & Ajzen, 1975; Vuchinich & Tucker, 1988), which articulate that individuals’ decisions to engage in health-compromising behavior such as drinking and driving, involve the subjective weighting of perceived costs and benefits associated with the behavior. Thus presenting people with information about the risks of negative consequences should alter their decision and lower the likelihood of engaging in that behavior.
A large empirical literature supports the validity of these theories for a variety of health-compromising behaviors (Conner, Warren, Close, & Sparks, 1999; Godin & Kok, 1996; Marcoux & Shope, 1997). However, there is little evidence that the programs designed specifically to inform audiences about risks are successful in changing harmful behavior (Botvin, 1990; Cronce & Larimer, 2011; Hawkins, Catalano, & Miller, 1992; Larimer & Cronce, 2002; National Institute on Alcohol Abuse and Alcoholism, 2002; National Institute on Drug Abuse, 1997) (for an exception see Centers for Disease Control and Prevention, 2014). Indeed, the National Institute for Alcohol Abuse and Alcoholism has categorized drinking interventions in terms of their effectiveness (NIAAA, 2012). Tier 4 interventions—those with demonstrated evidence of ineffectiveness—included stand-alone knowledge based or informational interventions (Larimer & Cronce, 2007; DeJong & Langford, 2002) as well as interventions that provide feedback on blood alcohol concentrations (Johnson et al., 2008; Johnson & Clapp, 2011). Further, several studies have found that holding negative expectancies about substance use was related to greater substance use and dependence (Connor, Gullo, Feeney, & Young, 2011; Li & Dingle, 2012) —which is inconsistent with the hypothesis that risk perception necessarily reduces engagement in health-compromising behaviors. Dovetailing this, evidence from a series of experimental studies suggests that exposure to messages about responsible drinking actually increased alcohol consumption among participants in a laboratory bar setting (Moss et al., 2015).
The current research takes advantage of the advances in motivation and self-regulation to understand better the impact of risk information on the decision to drink and drive. Specifically, it is possible that when driving is believed to be an instrumental means to one’s current goals or motivations (i.e., conveniently reaching one’s destination) accessibility of information inconsistent with this perception or belief (i.e. information about potential negative consequences) may increase rather than decrease the likelihood of driving. This is presumably possible because individuals’ active goals operate on relevant stimuli and information to produce goal-appropriate outcomes (Aarts, Dijksterhuis, & Vries, 2001; Balcetis & Dunning, 2006; Ferguson & Bargh, 2004; Förster, Liberman, & Higgins, 2005; Moskowitz, 2002). This includes finding appropriate means (Kruglanski et al., 2002), actively suppressing incompatible goals such as health and safety (Shah, Friedman, & Kruglanski, 2002; Shah & Kruglanski, 2003), and processing the information to fit with the current motivational state (Bélanger, Kruglanski, Chen, & Orehek, 2014).
For instance, a smoker may be fully aware of the negative consequences associated with smoking, but in a state of craving may suppress health-related concern and focus attention on the relaxing aspects of the behavior. Similarly, one can imagine a person who consumed a considerable amount of alcohol faced with the decision to drive home. This person may be highly motivated to drive for a number of reasons and may therefore be compelled to actively disregard or distort information regarding potential negative consequences associated with driving while intoxicated. Thus, risk information that might otherwise have helped attenuate the risky decision to drive may trigger a myopic response in favor of the most valued goal (i.e. to get home quickly and conveniently).
In addition to specific motivational states (e.g., desire to reach one’s destination conveniently), information processing may be altered by general motivational tendencies such as need for cognitive closure (NFC). NFC reflects the motivation to form definitive judgments and an aversion to ambiguity and inconsistency (Kruglanski & Webster, 1996; Webster & Kruglanski, 1994). It could be invoked by the situation (e.g., time pressure, alcohol consumption) or reflect a dispositional trait. When making a decision, individuals high in NFC are prone to “seizing and freezing” on the information that allows a quick judgment or decision, as opposed to engaging in a more careful review of potentially relevant information, and disregard subsequent inconsistent information (Kruglanski, 2004). Thus, it is possible that when driving is perceived as an instrumental means to one’s current goals or motivations (i.e., conveniently reaching one’s destination), high NFC individuals would overemphasize such goals and focus on information relevant to goal attainment. As a consequence, they may be more likely to engage in behaviors perceived as instrumental to these goals (driving) and disregard or even distort the information inconsistent with their goals (risk information).
Current Research
Three experimental studies were conducted to test the hypothesis that risk information about driving under the influence can actually increase the likelihood of drinking and driving when the goal of getting home quickly and conveniently is accessible and driving is perceived as instrumental to this goal. In a hypothetical drinking and driving scenario, participants’ self-reported likelihood of drinking and driving was investigated as a function of (1) accessibility of risk information (i.e., information about the negative consequences of drinking and driving and (2) motivation to drive. (i.e., convenience). Furthermore, to identify individuals most vulnerable to the failure to take risk information into account when making decisions about drinking and driving, the current research explored the moderating role of NFC.
Study 1
Study 1 represents the first attempt to explore the role of accessibility of risk information (high accessibility vs. low accessibility) on participants’ self-reported likelihood to drink and drive and to explore the extent to which NFC as an individual variable moderates this relationship. Accessibility of risk information was subtly manipulated by exposing participants to words related to drinking and driving vs. neutral words. Subsequently, they were presented with a drinking and driving scenario and asked to estimate the likelihood that they would drive in that scenario.
Methods
Recruitment, data collection, and the research methods were approved by the Pacific Institute for Research and Evaluation and University of Maryland’s IRB board.
Participants
A haphazard sample of 58 participants (age 18 and older) was recruited from the waiting areas of a Maryland Motor Vehicle Administration office. We reasoned that recruiting at this location would allow us to sample from a diverse population of drivers. The sample size was based on several pilot studies designed to develop and assess the effectiveness of the materials used in the current study. Specifically, in three studies assessing the effects of accessibility of risk information and NFC on self-reported intentions to drink and drive, the omega-square effect size of the interaction ranged between .08 to .10 which is considered to be medium to large (Murphy & Myoros, 2004). Based on a power analysis, we reasoned that a sample of 52 will give us .80 power to detect effect sizes similar to those observed in the pilot studies at alpha set at .05.
A $15 incentive was offered to encourage individuals to take part in the study. An information sheet described the research and the rights of participants, but in order to maintain the anonymity of the research there was no signed consent document. Participants read through and completed the study materials while they waited. Two participants did not complete the dependent measure and another two did not respond to the driving and drinking item and were excluded. Thus the final sample consisted of 54 participants.
Roughly equal numbers of men and women participated (46.9% male). The majority of participants were Caucasians (36.5%), followed by African American (25%), Asian (22.9%), and “Other” (14.6%). Slightly over one quarter (29.2%) indicated Hispanic ethnicity. The median age was 37 with 4.3% under age 211.
Procedure
Participants received a packet of five one-sided pages containing all the study materials in a manila envelope. Across all conditions, the first page contained questions on basic demographic information (sex, age, race and ethnicity).
The second page contained a short version of the NFC questionnaire (Roets & Van Hiel, 2011) (labeled “Personality Type”). The questionnaire consisted of 15 items assessing the individual’s preference for order, predictability, and stable and reliable knowledge (e.g., “I don’t like situations that are uncertain”). Participants were asked to express their agreement with the statement presented in each item on a 6-point scale (1- strongly disagree to 6 - strongly agree).
The third page contained the manipulation of accessibility of risk information and it was labeled “Word Destruction Task.” The task was described as a test of word knowledge and creativity. In this task, participants were provided with a list of 10 regular English words and were instructed to create up to three new words using the letters extant in each word on the list. For example, if the word on the list was hamster, participants could create ham, tram, master, Taser, etc. In the high accessibility condition (approximately half of the study packets randomly distributed to participants), four of the words provided were related to drinking and driving risk (crashed, police, reckless, caught) whereas six of the words were unrelated to drinking and driving. The words were selected based on a pretest in which a sample of online participants were asked to generate words related to the risks of drinking and driving. Participants generated a total of 97 words. The words used in this study were the words that had the highest frequency among the 97 words (between 10 and 72). The task is based on considerable evidence suggesting that the mere exposure to words activates semantically related concepts in memory (Tulving, 1983) and may increase the probability of using those concepts in subsequent judgments (Higgins, Rholes, & Jones, 1977; Srull & Wyer, 1979). Thus exposure to words related to drinking and driving should remind participants of the risks associated with drinking and driving. In the low accessibility condition, none of the words was directly related to driving, alcohol consumption, crashing, arrest, or injury.
The manipulation was followed by a page labeled “Dilemma Decisions.” Participants were told that people sometimes are faced with making tough choices between competing options, and that, as part of the research, they would read one scenario (randomly selected from a larger set) that detailed having to make one such tough decision. They were asked to read the scenario and imagine themselves being in that situation. The scenario consisted of a two-paragraph vignette and described a hypothetical drinking and driving situation (MacDonald, Zanna, & Fong, 1995) designed to induce the motivation to get home conveniently as well as to present driving as an instrumental means to fulfill this motivation across all participants. Specifically, the participant was meeting with an old friend who he or she had not seen for several years. The meeting involved food and drinks; the participant was having a good time and thus, the get-together took much longer than anticipated, and inadvertently the participant drank more than intended. At the end of the evening, participant was feeling tired and wanted to get home. He or she had to decide between driving home or calling and then waiting for a taxi. After reading the vignette, participants were asked to indicate the percent chance (0–100) that they would choose to drive home (versus call for a taxi) in this situation. This score was used as the primary dependent variable.
The last page contained additional measures of drinking and driving. Specifically, to ensure that driving does represent an instrumental means to the goal of reaching one’s destination conveniently, participants were asked to rate how convenient driving is compared to other means of transportation on a scale from 1 (not at all convenient) to 9 (very convenient). Participants also reported driving frequency (0 = never to 4 = daily), and the frequency of driving within two hours of drinking during the past six months (0 = never to 4 = four or more times a week). After completing the questionnaire, participants placed the material into the manila envelope, sealed it, returned it to the research assistant, and received their incentive.
Results and Discussion
Preliminary analyses revealed that participants perceived driving as more convenient (M = 7.60, SD = 2.05) compared to other means of transportation. Over 80% of the participants reported that they drove on average several times a week or daily. Furthermore, 10% of the sample reported driving within two hours of drinking during the past six months. Because this variable was significantly correlated with the main dependent variable (r = .36, p = .007) it was used as a covariate in the subsequent analyses. Self-reported likelihood of driving did not vary as a function of convenience of driving, frequency of driving, race, age, or sex. These variables were therefore not included in any further analyses.
Participants’ self-reported likelihood of driving ranged from 0 to 100 (M = 20.63, SD = 30.63). The NFC scores were computed by adding participants’ answers across the 15 items (α = .80, M = 50.78, SD = 11.86). This score was used as a continuous variable in the subsequent analyses. A general linear model regression was used to test the effect of NFC and accessibility of risk information on self-reported likelihood of driving. The analysis was conducted using the PROCESS macro (Hayes, 2012), which automatically centers the continuous variables and computes the interaction terms. The value of the statistical tests were compared to the critical value for each test corresponding to the standard α = .05. Driving within two hours of drinking during the past six months was used as a covariate and significantly predicted self-reported likelihood of driving (B = 46.71, SE = 13.63, t (49) = 3.42, p = .001, 95% CIs [19.30, 74.12]). The analysis revealed a significant interaction between NFC and accessibility of risk information on the likelihood-of-driving score, B = 1.59, SE = .65 t (49) = 2.43, p = .001, 95% CIs [.28, 2.90], η2 = .092. As predicted, accessibility of risk information (high vs. low) was associated with higher self-reported likelihood of driving, but only among participants high in NFC (defined as 1 SD above the sample mean), B = 26.84, SE = 11.15, t (49) = 2.40, p = .019, 95% CIs [4.24, 49.25]. However, among participants low in NFC (defined as 1 SD below the sample mean), accessibility of risk information was not associated with self-reported likelihood of driving (B = −10.98, SE = 10.79, t (49) = −1.46, p = .314, 95% CIs [− 32.68, 10.71]). The findings are depicted in Figure 1.
Figure 1.
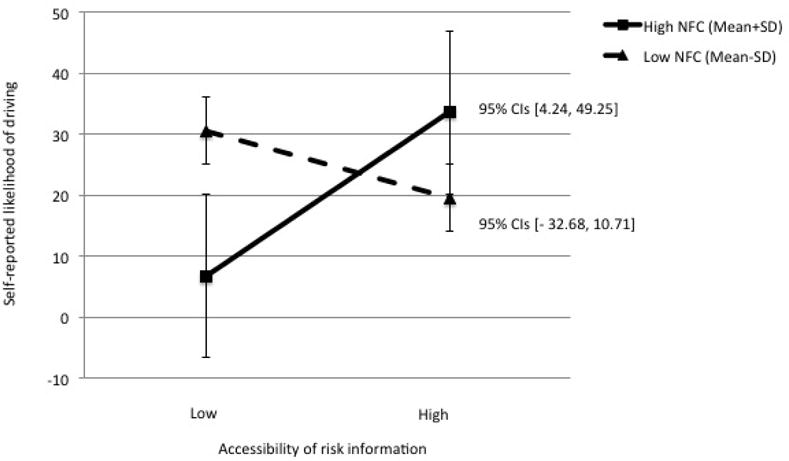
Self-reported likelihood of driving after drinking as a function of accessibility of risk information and need for closure (Study 1).
The results in Study 1 offer preliminary support for the hypothesis regarding the potential negative consequences that the accessibility of risk information may have on individuals’ decision to engage in drinking and driving. Specifically, they suggest that under certain motivational conditions (when driving is perceived as instrumental to individuals’ goals to reach their destination conveniently), the individuals high in NFC may be more likely to seize and freeze on the current goals (convenience) and the behavior perceived as instrumental to such goals (driving). As a consequence, the information inconsistent with such states (i.e., risk information) is likely to be processed in a way that presumably justifies the decision to engage in relevant behavior, resulting in higher self-reported likelihood of drinking and driving.
Although these findings are encouraging, the study is not without limitations. Risk information was presented very subtly. One could argue that such brief presentation might have allowed participants to disconsider it more easily, rather than use it to justify their decision. Given this limitation, a second study was designed to replicate these findings using a more explicit (rather than subtle) and a more ecologically valid manipulation of risk information.
Study 2
Similar to Study 1, Study 2 employed a one-way experimental design to test the effects of accessibility of risk information (high accessibility vs. low accessibility) on self-reported likelihood of drinking and driving and to explore the moderating role of NFC.
Methods
Recruitment, data collection, and the research methods were approved by the Pacific Institute for Research and Evaluation and University of Maryland’s IRB board.
Participants
A haphazard sample of 60 participants (age 18 and older) was recruited from the waiting areas of a Maryland Motor Vehicle Administration office and offered a $15 incentive to take part in the study. Decisions regarding the sampling method and the sample size were similar to those reported for Study 1. Similar to Study 1, an information sheet described the research and the rights of participants, but there was no signed consent document. Participants read through and completed the study materials while they waited. Data from one participant was excluded due to uniform responses to one questionnaire indicating a potential response bias. One participant did not complete the dependent measure, and two participants did not respond to the driving after drinking question. Thus the final sample consisted of 56 participants.
Roughly equal numbers of men and women participated (52.8% male). Forty-three percent of the participants were African Americans and 40.8% were Caucasians. The remainder identified as Asian, Multiracial, or “Other.” Over one quarter (25.5%) indicated having Hispanic ethnicity. The median age was 40, and less than 6% of the sample was under age 21.
Procedure
As in Study 1, participants received a packet of four one-sided pages containing all the study materials in a manila envelope. Across all conditions, the first page contained questions on basic demographic information (sex, age, race, and ethnicity), and the second page contained the NFC questionnaire.
The third page was labeled “Dilemma Decisions” and contained the manipulation of accessibility of risk information. Similar to Study 1, participants were presented with a scenario describing a drinking and driving situation and asked to imagine themselves in that situation. The first two paragraphs were identical to those presented in Study 1. However, instead of presenting the participant as being dead tired and wanting to get home, the scenario in this study simply stated that it was time to get home, and the participant had to decide between driving home or calling and then waiting for a taxi. In this study, the vignette included a third paragraph containing the manipulation of risk information. Specifically, in the low accessibility of risk information condition, the vignette indicated that the participant was not 100% sure that it was safe to drive, but that the roads were well lit and familiar. In the high accessibility of risk information condition, the vignette indicated that the participant was not 100% sure that it was safe to drive, but that the roads were dark and not very familiar. Similar to Study 1, after reading the vignette, participants were asked to indicate the percent chance (0–100) that they would choose to drive home (versus call for a taxi) in this situation. This score was used as primary dependent variable.
The last page contained the additional measures of drinking and driving that were also used in Study 1. After completing the questionnaire, participants placed the material into the manila envelope, sealed it, returned it to the research assistant, and received their incentive.
Results and Discussion
All statistical tests were compared to the critical value for each test corresponding to the standard α = .05. Similar to Study 1, compared to other means of transportation, driving was perceived as more convenient (M = 7.60, SD = 1.96). Eighty percent of the participants reported that they drove on average several times a week or daily. Twenty percent of the sample reported driving within two hours of drinking during the past six months. None of the measures were related to participants’ self-reported likelihood of driving in the scenario. Furthermore, self-reported likelihood of driving did not vary as a function of race, age, or sex. As a consequence, these variables were not included in any further analyses.
Self-reported likelihood of drinking and driving ranged from 0 to 100 with an average of 31.76 (SD = 36.29). Participants’ NFC scores were computed by adding their answers across the 15 items (α = .79, M = 49.50, SD = 11.16). This score was used as a continuous variable in subsequent analyses. A general linear model regression was used to test the effect of NFC and accessibility of risk information on self-reported likelihood of driving. The analysis revealed a significant interaction between NFC and accessibility of risk information on the likelihood-of-driving score, B = − 2.69, SE = .96, t (52) = − 2.78, p = .007, 95% CIs [− 4.63, − .75], η2 = .126). Similar to Study 1, accessibility of risk information (high vs. low) was associated with higher likelihood of driving, but only among participants high in NFC (defined as 1 SD above the sample mean), B = − 39.45, SE = 14.23, t (52) = − 2.77, p = .007, 95% CIs [− 68.01, −10.88]. However, among participants low in NFC (defined as 1 SD below the sample mean), accessibility of risk information was not associated with likelihood of driving (B = 20.69, SE = 14.09, t (52) = 1.46, p = .148, 95% CIs [− 7.60, 48.98]). The findings are depicted in Figure 2.
Figure 2.
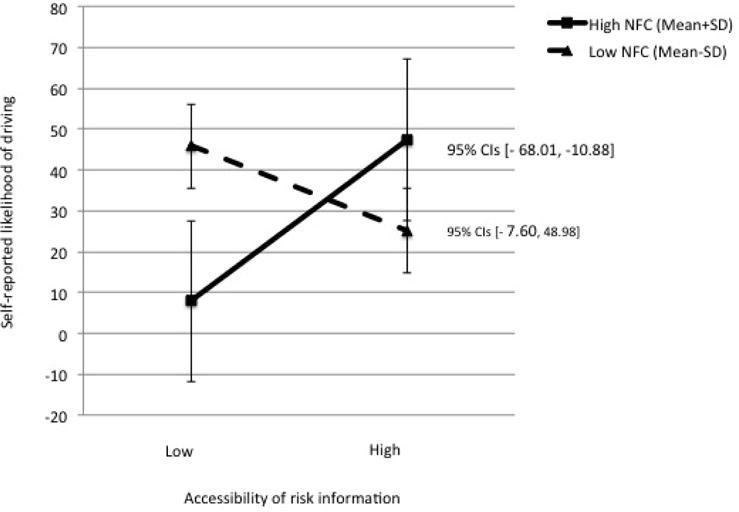
Self-reported likelihood of driving after drinking as a function of accessibility of risk information and need for closure (Study 2).
The results obtained in Study 2 replicate those from Study 1 and offer further support for the notion that risk information may inadvertently increase one’s willingness to drive after drinking when driving is perceived as an instrumental means to a current motivation or goal (e.g., convenience). This effect was significant only among high NFC participants who might have seized on the goal of getting home conveniently (based on information early in the vignette) and processed the subsequent risk information in a manner consistent with this goal. However, participants low in NFC, who are less likely to seize and freeze on a current goal and on the behavior that fulfills it immediately, were not affected by the risk information provided.
Studies 1 and 2 offer consistent support for the hypotheses. However, in both studies the motivation to get home quickly and conveniently was presumably present across conditions being induced through the vignette. The third and last study aimed to directly manipulate motivation and show that the effects obtained in Studies 1 and 2 only occur in the presence of a relevant motivation and do not occur when such motivation is absent.
Study 3
Study 3 explored participants’ self-reported likelihood of driving as a function of motivation to get home quickly and conveniently (high vs. low), accessibility of risk information (high accessibility vs. low accessibility), and NFC. Motivation manipulation was embedded in a hypothetical drinking and driving scenario similar to the one used in the previous two studies. The accessibility of risk information was manipulated using a word search puzzle task (Bargh, Gollwitzer, Lee-Chai, Barndollar, & Trotschel, 2001).
Methods
Participants
Participants were 56 individuals aged between 18 and 56 recruited on and around the campus of a large mid-Atlantic university. The samples in Study 1 and 2 included a wider range of drivers, however, there were very few young drivers (21 and younger). This may be particularly problematic given that 1 in 10 young (teens 16 and older) drivers drink and drive and that they are 3 times more likely than experienced drivers to be in a fatal crash (CDC, 2012). Thus, in Study 3, we specifically targeted younger drivers who are more at risk to suffer the consequences of drinking and driving. We reasoned that by recruiting on a university campus we would get access to younger drivers and we would be able to better generalize our findings. The median age was 21, only three participants were older than 24. Almost two thirds were male (68.4%). Three quarters (75.4%) identified as Caucasians (non-Hispanic). Participants were offered a $10 gift card as incentive for participating.
Procedure
A research assistant approached potential participants on and around campus and invited them to take part in a brief study on “Personality and Choices.” Individuals who expressed interest were given a manila envelope containing the study materials, printed and stapled in the order in which they were to be filled out. The study was anonymous, and the IRB granted a waiver of documentation of informed consent.
Participants first provided basic demographic information and completed the NFC questionnaire. As in previous studies, participants then read an introductory paragraph about “dilemmas” in which individuals needed to select between two difficult choices. The dilemma described a hypothetical drinking and driving scenario. The scenario was similar to the one used in Studies 1 and 2 adapted for a student sample. Rather than catching up with an old friend, participants read about hanging out with friends and the event escalating into a party where they consumed more alcohol than anticipated. The participant was faced with the dilemma of driving home or calling a taxi. To emphasize the instrumentality of driving, the limitations of calling for a taxi (e.g., calling, then waiting) were mentioned. To manipulate motivation, in the high convenience motivation condition, the participant was asked to imagine feeling dead tired and simply longing to go home and go to bed. In the low convenience motivation condition, participants were asked to imagine having a less compelling reason to drive home—they wanted to get home in time to make plans with roommates for going to brunch the next day.
Next, participants were given a word search puzzle to complete. The puzzle was used to manipulate the accessibility of risk information and was presented as a distractor task. Participants were provided with a 20-×-20 grid of English letters, along with a word list of 16 words, and asked to circle as many of the 16 words from the list as they could in a period of 10 minutes (Bargh et al., 2001). In the high accessibility of risk information condition, 6 of the 16 words from the neutral list were replaced with words relevant to the risks of drinking and driving (i.e., crash, police, swerve, arrest, risky, drink). Exposure to words related to risk was expected to increase the accessibility of the risk related to drinking and driving without participants blatantly relating them to the later task. In the low accessibility of risk information condition, all 16 words were unrelated to drinking and driving. As in the previous studies, participants were subsequently asked to indicate the percent chance that they would drive in the situation depicted in the scenario. The responses on this measure represented the dependent measure.
Participants also filled out the additional measures of drinking and driving that were used in Studies 1 and 2. They returned the envelope containing the completed questionnaires to the research assistant and were compensated for their participation.
Results and Discussion
As in Study 1 and 2, all statistical tests were compared to the critical value for each test corresponding to the standard α = .05. Compared to other means of transportation, driving was perceived as more convenient (M = 8.07, SD = 1.24). Ninety percent of the participants reported that they drove on average several times a week or daily. Over 60% of the sample reported driving within two hours of drinking during the past six months. Because this variable was significantly correlated to the dependent variable (r = .47, p < .01), it was used as a covariate in the subsequent analyses. Self-reported likelihood of driving did not vary as a function of race, age, or sex; perceived convenience of driving; or frequency of driving. As a consequence, these variables were not included in any further analyses.
Self-reported likelihood of driving ranged from 0 to 90, with an average of 28.59 (SD = 30.46). Participants’ NFC score was computed using the standard method (α = .71, M = 47.3, SD = 8.4) and used it as a continuous variable in subsequent analyses. A general linear model was conducted to test the effects of motivation, accessibility of risk information, and NFC on self-reported likelihood of driving controlling for driving within two hours of drinking during the past six months. Driving within two hours of drinking during the past six months significantly predicted self-reported likelihood of driving, B = 16.45, SE = 4.66, t (47) = 3.52, p = .001, 95% CIs [7.06, 25.85]. In addition, the analysis revealed a significant three-way interaction, B = 4.60, SE = 2.07, t (47) = 2.21, p = .031, 95% CIs [.42, 8.77], η2 = .064. Within the high convenience motivation condition, there was a two-way interaction between risk information and NFC that replicates the pattern of findings obtained in Studies 1 and 2 (B = − 3.53, SE = 1.55, t (47) = − 2.27, p = .027, 95% CIs [−6.65, −.41]). Specifically, accessibility of risk information (high vs. low) was associated with higher self-reported likelihood of driving in the scenario, but only among high NFC participants (B = − 34.26, SE = 17.04, t (47) = − 2.00, p = .050, 95% CIs [− 68.55, − 0.036]). There was no significant relation between risk information and self-reported likelihood of driving among low NFC participants (B = 4.49, p = .767). The findings are represented in Figure 3a. In the low convenience motivation condition, neither the interaction between NFC and accessibility of risk information (B = 1.07, p = .764), nor the simple effects of risk information (B = 4.49, p = .767 for low NFC participants and B = 20.88, p = .172 for high NFC participants) were statistically significant (see Figure 3b)2.
Figure 3.
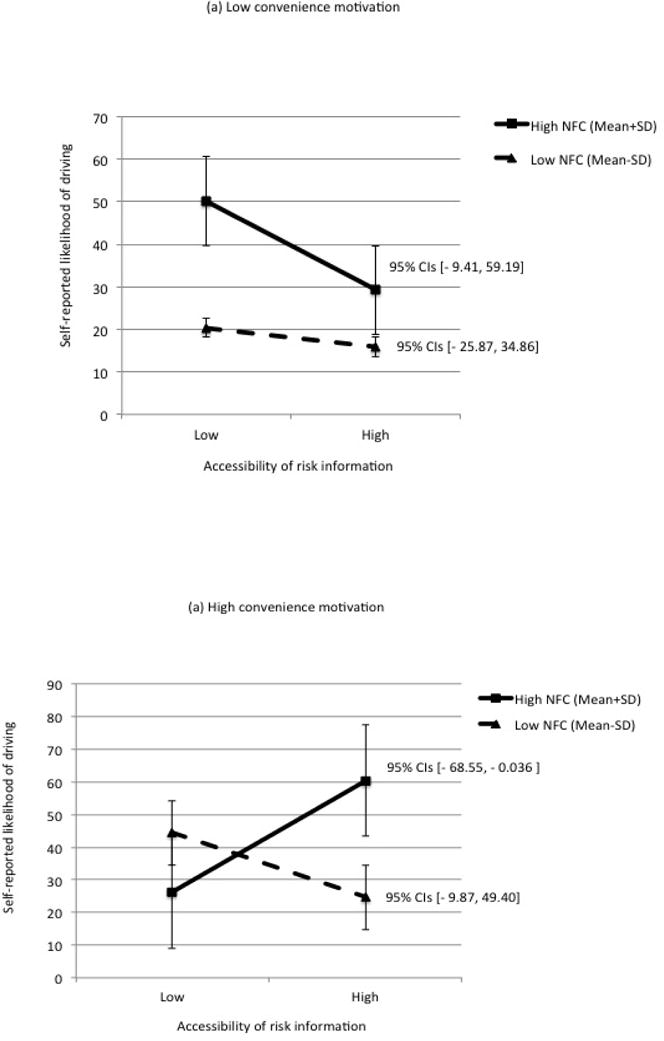
Self-reported likelihood of driving after drinking as a function of convenience motivation, accessibility of risk information, and need for closure (mean +/ −SD) (Study 3).
Once again, accessibility of information regarding the risks associated with drinking and driving appear to have unintended consequences and increase rather than decrease one’s self-reported likelihood of driving after drinking when the person is motivated to get home quickly and conveniently and is high in NFC. This presumably happens because risk information is inconsistent with the person’s current goals and the behaviors that are instrumental to achieving these goals (driving). None of these effects are significant in the absence of the relevant motivation, which further supports the notion that people process and use information to advance their current goals.
Conclusions and Implications
Information about the risks of drinking and driving is widely disseminated—from driver’s education classes and Alcohol 101 courses on college campuses to television and radio publicity campaigns and public service announcements. Such information has the clear purpose of influencing the future decisions of people faced with the opportunity to drive while impaired. Yet results from three studies showed that under some circumstances, accessibility of risk information inadvertently increases their willingness to drive. This may be the case because this information may not necessarily be applicable and translated into behavior if it is inconsistent with one’s current goals. Thus, someone who strongly wishes to get home quickly and conveniently after a night of drinking may be compelled to drive (if driving is the most instrumental behavior) despite being aware of the potential negatives consequences.
Indeed, across three studies in the presence of the motivation to get home quickly and conveniently, when driving is emphasized as the most instrumental means to fulfill this motivation, presenting participants with risk information (and thus increasing the accessibility of negative consequences of drinking and driving) resulted in higher self-reported likelihood of driving in a hypothetical drinking and driving scenario. This was particularly true for people high in NFC who are motivated to reduce uncertainty, reach their goals, and attain closure as quickly as possible, even if doing so requires suppressing or ignoring incompatible, albeit relevant, information on risks.
Whereas decision-making typically may involve weighing the costs and benefits of behavior, information inconsistent with one’s goals may produce polarized decisions and actions. Although the current findings do not speak about the nature of this “polarization”, it is possible that high NFC individuals who are motivated to get home quickly and conveniently and perceive driving as the most instrumental means may experience dissonance in the presence of risk information. Greater self-reported willingness to drive may represent the result of a dissonance reduction process whereby the people actively attempt to gather information consonant with the behavior that serves their goal (e.g. the benefits of driving). If this is the case, the findings should be mediated by a decrease in perceived riskiness of the behavior. Finally, another potential explanation is provided by the research on goal pursuit (Kruglanski et al. 2015). This perspective suggests that a behavior is that serves a goal is perceived to be particularly instrumental to that goal to the extent to which it interferes with alternative goals. Thus it is possible that accessibility of risk information, which interferes with their alternative goals of safety, increases the perceived instrumentality of driving resulting in greater willingness to engage in this behavior. If this hypothesis is true, when presented with risk information, people should perceive the behavior as more risky (compared to less risky as suggested by the approach above) but the increase in perceived riskiness should result in an increase in perceived instrumentality, which in turn will increase the willingness to drive after drinking. All these possibilities should be explored in future research to provide a better understanding of when and why risk information may have inadvertent consequences.
Although in the current studies NFC was measured as a trait, need for closure may be situationally induced under time pressure (Kruglanski & Freund, 1983) and by noise or fatigue (Kruglanski & Webster, 1991; Webster, Richter, & Kruglanski, 1996). Importantly, NFC may also be elevated by alcohol intoxication (Lange, 2002; Webster, 1993). Thus, the above findings may be relevant not only among people high in the trait of NFC, but to everybody who experiences stress, fatigue, time pressure, and, indeed, alcohol intoxication, which makes the findings presented herein regarding drinking and driving particularly relevant to public health. Future studies should test the possibility that a situationally induced need for closure may also alter the impact of risk information on decisions to engage in risky behavior in general and drunk driving in particular.
These laboratory results are promising and may provide some insight into the limited impact that prevention campaigns seem to have on health-compromising behaviors. However, they do not suggest that existent risk information program might actually increase real-world drunk driving. Instead, they point out to the possibility that the limited effectiveness of risk information observed in field studies may be the result of those programs having divergent effects—decreasing risk for some, increasing it for others, and balancing out in aggregate—as a function of individual’s motivations. It is noteworthy that risk information in these studies is presented in a much more subtle way that in the typical messages designed to reduce drunk driving. One may argue that presenting the information in such manner may make it easier to ignore or distort. A related issue refers to the fact that the current studies are based on scenarios and on self-reported likelihood of driving after drinking. One could argue that this methodology taps into “rational” decision making which may be different than what actually happens when the person is intoxicated and thus more likely to act “impulsively.” Indeed, several well-known dual-process models suggest that engagement in substance use–related behavior is not necessarily premeditated or intended based on risk–benefits calculations, but rather the result of automatic processes set in motion by internal and external cues (i.e., negative emotions, the presence of drug cues such as an ash tray, or the presence of one’s friends) (Gerrard, Gibbons, Houlihan, Stock, & Pomery, 2008; Stacy & Wiers, 2010). In other words, the person does not intend to engage in risk behavior, but she does when the situation “suggests” or “prompts” it. Although the participants in these studies are not necessarily in such situation, alcohol intoxication does increase one’s NFC. Furthermore, it is important to keep in mind that the information regardless of the manner in which it is presented is processed as a function of individual’s motivation and the extent to which the information is relevant to such motivation. Thus, it is possible that alcohol intoxication may in fact exacerbate these effects. Indeed, the alcohol myopia model suggests that alcohol causes individuals to limit their focus to some pieces of information (e.g., benefits) at the expense of other information (e.g., risks), which can result in extreme judgments (Giancola, Duke, & Ritz, 2011; Steele & Josephs, 1990). Future research should focus on how motivation and information interact to affect individual’s behavior in more ecological settings, when individuals are intoxicated.
In order to develop and implement effective behavioral prevention and intervention strategies, one should take into account that audiences are not passive recipients of information. People’s personal goals impact the way information is perceived, processed, and translated into behavior. Furthermore, although some goals are stable, others fluctuate on a moment-to-moment basis depending on the individual’s environment and may have a profound impact on how the prevention and intervention efforts impact behavioral decisions. Although health-compromising behaviors interfere with concerns for health and safety and may appear irrational from the societal perspective, these behaviors satisfy important goals that the person may have in the moment (Kopetz & Orehek, 2015). In this case, the information that contradicts the instrumentality of these behaviors to one’s goals is very likely to be distorted and to have unintended consequences. A potentially more effective strategy is to increase people’s awareness and access to alternative behaviors that fulfill the goal without the associated negative consequences. For instance, messages like “Stay alive, don’t drink and drive” that emphasize the negative consequences of drinking and driving could be replaced by messages that provide alternatives such as “Take a taxi/Uber, don’t drink and drive.”
Footnotes
Although some of the participants are under the legal age for drinking, we believe that by including them the sample represents more accurately the population that drinks and drive. CDC (2012) reports that 1 in 10 teens aged 16 and older drink and drive; the percentage of teen drunk driving ranges between 5% to 15% depending on the state. Teen drivers are 3 times more likely than more experienced drivers to be in a fatal crash. Drinking any alcohol greatly increases this risk for teens. We believe that not including people who are not at a legal age for drinking would ignore a segment of the population that is most at risk for drinking and driving.
To test for the effect of age, we re-ran the analyses excluding participants younger than 21. In Study 1, there were 9 participants under the legal age of drinking; the findings remain significant B = 1.46, SE = .68 t (40) = 2.14, p = .038, 95% CIs [.082, 2.85], η2 = .085. In Study 2, there were only 3 participants under the age of 21. When we excluded them from the analysis, the results did not change: B = −2.18, SE = .1.00 t (47) = − 2.16, p = .035, 95% CIs [−4.20, −.158], η2 = .086. In Study 3, there were 20 people under the age of 21. The findings are not significant anymore when we exclude them. However, that should not be surprising given that removing 20 subjects reduces statistical power considerably. Given that the results in the previous studies are not affected by this variable, we believe that in Study 3, the lack of significance is due to the fact that the sample size drops to 36, which is too small to detect the effect of a 3-way interaction.
References
- Aarts H, Dijksterhuis A, Vries P. On the psychology of drinking: Being thirsty and perceptually ready. British Journal of Psychology. 2001;92(4):631–642. doi: 10.1348/000712601162383. [DOI] [PubMed] [Google Scholar]
- Azjen I. From intentions to actions: A theory of planned behavior. In: Kuhl J, Beckmann J, editors. Action control: From cognition to behavior. Berlin, Heidelber, New York: Springer-Verlag; 1985. [Google Scholar]
- Balcetis E, Dunning D. See what you want to see: motivational influences on visual perception. Journal of Personality and Social Psychology. 2006;91(4):612. doi: 10.1037/0022-3514.91.4.612. [DOI] [PubMed] [Google Scholar]
- Bargh JA, Gollwitzer PM, Lee-Chai A, Barndollar K, Trotschel R. The automated will: Nonconscious activation and pursuit of behavioral goals. Journal of Personality and Social Psychology. 2001;81:1014–1027. [PMC free article] [PubMed] [Google Scholar]
- Bélanger JJ, Kruglanski AW, Chen X, Orehek E. Bending perception to desire: Effects of task demands, motivation, and cognitive resources. Motivation and Emotion. 2014;38(6):802–814. [Google Scholar]
- Botvin GJ. Substance abuse prevention: Theory, practice, and effectiveness. Criminal Justice and Behavior. 1990;13:461–519. [Google Scholar]
- Brown SA, Goldman MS, Christiansen BA. Do alcohol expectancies mediate drinking patterns of adults? Journal of Consulting and Clinical Psychology. 1985;53(4):512–519. doi: 10.1037//0022-006x.53.4.512. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. Tips From Former Smokers campaign results. CDC News Room: Digital Press Kit. 2014 Feb 28; Retrieved from http://www.cdc.gov/media/dpk/2013/dpk-TIPS-campaign-results.html.
- Conner M, Warren R, Close S, Sparks P. Alcohol consumption and the Theory of Planned Behavior: An examination of the cognitive mediation of past behavior. Journal of Applied Social Psychology. 1999;29:1676–1704. [Google Scholar]
- Connor JP, Gullo MJ, Feeney GF, Young RM. Validation of the Cannabis Expectancy Questionnaire (CEQ) in adult cannabis users in treatment. Drug and alcohol dependence. 2011;115(3):167–174. doi: 10.1016/j.drugalcdep.2010.10.025. [DOI] [PubMed] [Google Scholar]
- Cronce JM, Larimer ME. Individual-focused approaches to the prevention of college student drinking. Alcohol Research Health. 2011;34(2):210–221. [PMC free article] [PubMed] [Google Scholar]
- Ferguson MJ, Bargh JA. Liking is for doing: The effects of goal pursuit on automatic evaluation. Journal of Personality and Social Psychology. 2004;87:557–572. doi: 10.1037/0022-3514.87.5.557. [DOI] [PubMed] [Google Scholar]
- Fishbein M, Ajzen I. Belief, attitude, intention, and behavior: An introduction to theory and research. Reading, MA: Addison-Wesley; 1975. [Google Scholar]
- Förster J, Liberman N, Higgins ET. Accessibility from active and fulfilled goals. Journal of Experimental Social Psychology. 2005;41(3):220–239. [Google Scholar]
- Gerrard M, Gibbons FX, Houlihan AE, Stock ML, Pomery EA. A dual-process approach to health risk decision making: The prototype willingness model. Developmental Review. 2008;28(1):29–61. doi: 10.1016/j.dr.2007.10.001. [DOI] [Google Scholar]
- Godin G, Kok G. The theory of planned behavior: A review of its applications to health behaviors. American Journal of Health Promotion. 1996;22(2):87–98. doi: 10.4278/0890-1171-11.2.87. [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Catalano RF, Miller JY. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: Implications for substance abuse prevention. Review. Psychological Bulletin. 1992;112(1):64–105. doi: 10.1037/0033-2909.112.1.64. [DOI] [PubMed] [Google Scholar]
- Hayes AF. PROCESS: A versatile computational tool for observed variable mediation, moderation, and conditional process modeling [White paper] 2012 Retrieved from http://imaging.mrc-cbu.cam.ac.uk/statswiki/FAQ/SobelTest?action=AttachFile&do=get&target=process.pdf.
- Higgins ET, Rholes WS, Jones CR. Category accessibility and impression formation. Journal of Experimental Social Psychology. 1977;13(2):141–154. [Google Scholar]
- Kruglanski AW. The quest for the gist: On challenges of going abstract in social and personality psychology. Personality and Social Psychology Review. 2004;8(2):156–163. doi: 10.1207/s15327957pspr0802_9. [DOI] [PubMed] [Google Scholar]
- Kruglanski AW, Freund T. The freezing and unfreezing of lay-inferences: Effects of impressional primacy, ethnic stereotyping, and numerical anchoring. Journal of Experimental Psychology. 1983;19:448–468. [Google Scholar]
- Kruglanski AW, Shah JY, Fishbach A, Friedman RS, Chun WY, Sleeth-Keppler D. A theory of goal systems. In: Zanna M, editor. Advances in Experimental Social Psychology. San Diego, CA: Academic Press; 2002. pp. 331–378. [Google Scholar]
- Kruglanski AW, Webster DM. Group members’ reactions to opinion deviates and conformists at varying degrees of proximity to decision deadline and of environmental noise. Journal of personality and social psychology. 1991;61(2):212. doi: 10.1037//0022-3514.61.2.212. [DOI] [PubMed] [Google Scholar]
- Kruglanski AW, Webster DM. Motivated closing of the mind: “Seizing” and “freezing”. Psychological Review. 1996;103:263–283. doi: 10.1037/0033-295x.103.2.263. [DOI] [PubMed] [Google Scholar]
- Lange JE. Alcohol’s effect on aggression identification: A two-channel theory. Psychology of Addictive Behaviors. 2002;16(1):47–55. doi: 10.1037//0893-164x.16.1.47. [DOI] [PubMed] [Google Scholar]
- Larimer ME, Cronce JM. Identification, prevention and treatment: A review of individual-focused strategies to reduce problematic alcohol consumption by college students. Journal of Studies on Alcohol. 2002;14(Suppl):148–163. doi: 10.15288/jsas.2002.s14.148. [DOI] [PubMed] [Google Scholar]
- Li HK, Dingle GA. Using the Drinking Expectancy Questionnaire (revised scoring method) in clinical practice. Addictive behaviors. 2012;37(2):198–204. doi: 10.1016/j.addbeh.2011.10.002. [DOI] [PubMed] [Google Scholar]
- MacDonald TK, Zanna MP, Fong GT. Decision making in altered states: effects of alcohol on attitudes toward drinking and driving. Journal of personality and social psychology. 1995;68(6):973. doi: 10.1037//0022-3514.68.6.973. [DOI] [PubMed] [Google Scholar]
- Marcoux BC, Shope JT. Application of the theory of planned behavior to adolescent use and misuse of alcohol. Health Education Research. 1997;12:323–331. [Google Scholar]
- Moskowitz GB. Preconscious effects of temporary goals on attention. Journal of Experimental Social Psychology. 2002;38(4):397–404. [Google Scholar]
- Moss AC, Albery IP, Dyer KR, Frings D, Humphreys K, Inkelaar T, Speller A. The effects of responsible drinking messages on attentional allocation and drinking behaviour. Addictive Behaviors. 2015;44:94–101. doi: 10.1016/j.addbeh.2014.11.035. [DOI] [PubMed] [Google Scholar]
- National Institute on Alcohol Abuse and Alcoholism. How to reduce high-risk college drinking: Use proven strategies, fill research gaps (Final Report of the Panel on Prevention and Treatment, Task Force of the National Advisory Council on Alcohol Abuse and Alcoholism) Washington, DC: National Institutes of Health; 2002. [Google Scholar]
- National Institute on Drug Abuse. Validity of Self-Reported Drug Use: Improving the Accuracy of Survey Estimates. Rockville, MD: NIDA; 1997. [Google Scholar]
- Roets A, Van Hiel A. Item selection and validation of a brief, 15-item version of the Need for Closure Scale. Personality and Individual Differences. 2011;50(1):90–94. [Google Scholar]
- Ross HL. Deterring the drinking driver: Legal policy and social control. 2nd. Lexington, MA: Lexington Books; 1984. [Google Scholar]
- Shah JY, Friedman R, Kruglanski AW. Forgetting all else: On the antecedents and consequences of goal shielding. Journal of Personality and Social Psychology. 2002;83:1261–1280. [PubMed] [Google Scholar]
- Shah JY, Kruglanski AW. When opportunity knocks: Bottom-up priming of goals by means and its effects on self-regulation. Journal of Personality and Social Psychology. 2003;84:1109–1122. doi: 10.1037/0022-3514.84.6.1109. [DOI] [PubMed] [Google Scholar]
- Srull TK, Wyer RS. The role of category accessibility in the interpretation of information about persons: Some determinants and implications. Journal of Personality and Social Psychology. 1979;37(10):1660–1672. [Google Scholar]
- Stacy AW, Wiers RW. Implicit cognition and addiction: a tool for explaining paradoxical behavior. Annual Review of Clinical Psychology. 2010;6:551–575. doi: 10.1146/annurev.clinpsy.121208.131444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stahre M, Roeber J, Kanny D, Brewer RD, Zhang X. Peer Reviewed: Contribution of Excessive Alcohol Consumption to Deaths and Years of Potential Life Lost in the United States. Preventing chronic disease. 2014;11 doi: 10.5888/pcd11.130293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tulving E. Ecphoric processes in episodic memory. Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences. 1983;302(1110):361–370. doi: 10.1098/rstb.1983.0060. [DOI] [Google Scholar]
- Vuchinich RE, Tucker JA. Contributions from behavioral theories of choice to an analysis of alcohol abuse. Journal of Abnormal Psychology. 1988;97(2):181. doi: 10.1037//0021-843x.97.2.181. [DOI] [PubMed] [Google Scholar]
- Webster DM. Groups under the influence: alcohol’s motivational and cognitive effects on collective judgements. University of Maryland at College Park; 1993. [Google Scholar]
- Webster DM, Kruglanski A. Individual differences in need for cognitive closure. Journal of Personality and Social Psychology. 1994;67:1049–1062. doi: 10.1037//0022-3514.67.6.1049. [DOI] [PubMed] [Google Scholar]
- Webster DM, Richter L, Kruglanski AW. On leaping to conclusions when feeling tired: Mental fatigue effects on impressional primacy. Journal of Experimental Social Psychology. 1996;32(2):181–195. [Google Scholar]