

Abstract
Anaplastic thyroid carcinoma (ATC) is difficult to distinguish from other cancers, especially when its pathological features are atypical for ATC or when the tumor is totally undifferentiated and occurs after a considerable lapse of time, in an area remote from the original site of the tumor. Here, we present two patients (68-year-old man and 56-year-old woman) with rare manifestations of ATC, which were initially thought to be other malignancies. Immunohistochemical tests, using various markers, failed to provide information about the origin of these tumors. However, both patients had a history of papillary thyroid carcinoma (PTC) from several years ago and BRAF mutations were observed in the undifferentiated tumors, as well as in the previous PTCs. Therefore, we could make a diagnosis of ATC derived from PTC. As such, BRAF mutation analysis may serve as a useful tool for ATC diagnosis in challenging ATC cases.
Keywords: Anaplastic Thyroid Carcinoma, BRAF, Papillary Thyroid Carcinoma, Immunohistochemistry
Graphical Abstract
INTRODUCTION
Although anaplastic thyroid carcinoma (ATC) is a highly aggressive thyroid gland malignancy with a median survival of 3 to 5 months, there are currently no adequate treatment options (1). ATC is known to be difficult to distinguish from other poorly differentiated neoplasms or soft tissue sarcomas, especially when it manifests in an area remote from the original tumor, because it often lacks differentiating attributes.
BRAF is the most commonly mutated gene in thyroid cancer. The prevalence of BRAF mutations in papillary thyroid carcinoma (PTC) ranges from 27.3% to 87.1% (2,3), and is significantly higher in Asia, especially Korea, in comparison to western countries. However, BRAF mutations are detected in only 25% of ATC cases (4), and the diagnostic roles of these mutations in ATCs remain elusive.
Here, we present two patients with rare manifestations of ATC, which were initially thought to be other malignancies. BRAF mutations were present in their ATCs, as well as in their primary PTCs, providing a vital clue for their final diagnosis.
CASE DESCRIPTION
Case 1
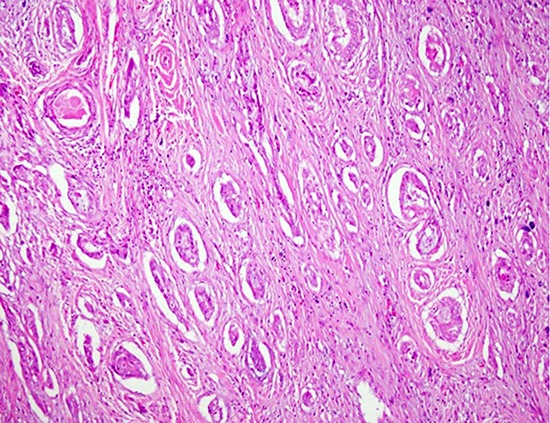
A 68-year-old man complained of a neck mass with laryngeal invasion and underwent a wide excision of the thyroid bed and a complete laryngectomy in October 2010. The patient was initially diagnosed with a sarcomatoid carcinoma of the neck with unusual histology. The tumor showed epithelioid-tubular structures containing mucin pools, with a fibrous or sarcomatous background, which is not consistent with the typical morphological features of ATC (Fig. 1A and 1B). The patient received adjuvant radiotherapy (42 Gy) and chemotherapy. However, the size of the residual neck mass and lung nodules increased, and the patient died 9 months after their last operation.
Fig. 1.

Histological and immunohistochemical features of case 1. (A) Sarcomatoid carcinoma of the neck shows the tubular structures with the sarcomatous background (H & E staining, × 100). (B) Tubular structures have mucin pools (H & E staining, × 200). (C) Both components were positive for CK7 (× 40). (D) Direct sequencing of the BRAF gene shows a missense mutation (c.1799T>A). (E, F) Neck lymph nodes, that were dissected 3 years ago, show the histology of papillary carcinoma (H & E staining, × 100) (E) and the presence of BRAF (× 100) (F).
H & E = hematoxylin and eosin, CK = cytokeratin.
The patient had a history of total thyroidectomy for a PTC 6 years previously. In addition, the patient underwent a dissection of neck lymph nodes for PTC recurrence and a total of 200 mCi of radioactive iodine (131I) therapy 3 years previously.
The patient's tissue samples were reviewed retrospectively, and additional immunohistochemistry (IHC) staining and direct sequencing of the BRAF gene were performed. The primary PTC samples could not be included due to their poor quality. High expression levels of thyroid transcription factor-1 (TTF-1), thyroglobulin (Tg), paired box gene 8 (PAX8), and human bone marrow endothelial cell-1 (HBME-1) were observed in the recurrent node, but not in the laryngeal mass (Table 1). Other data obtained through IHC testing showed identical results for both the recurrent neck node and the laryngeal tumor: positivity for vimentin, p53, cytokeratin (CK) 7 (Fig. 1C), and galectin-3; focal positivity for CK19; and negativity for CK20. Although the histopathological findings, as well as the IHC results, of the undifferentiated larynx tumor did not suggest that it originated from the thyroid, the positive result for the BRAF V600E mutation, by direct sequencing, indicated a possible PTC origin for the ATC (Fig. 1D). Thus, we performed a BRAF mutation analysis using IHC on metastatic PTC samples in the patient's neck lymph nodes (Fig. 1E), which subsequently revealed the presence of a BRAF mutation (Fig. 1F). This suggests that the laryngeal mass could have been an anaplastic transformation from the PTC, rather than a primary sarcomatoid carcinoma of the larynx.
Table 1. Immunohistochemical staining and BRAF mutation results.
| Variables | Case 1 | Case 2 | |||
|---|---|---|---|---|---|
| Lymph node PTC | Larynx ATC | Thyroid PTC | Lymph node PTC | Brain ATC | |
| TTF-1 | ++ | − | ++ | + | − |
| Tg | ++ | − | ++ | + | − |
| Vimentin | Focal + | ++ | Focal + | + | ++ |
| p53 | + | + | + | + | ++ |
| CK7 | ++ | ++ | ++ | ++ | ++ |
| CK20 | − | − | − | − | − |
| CK19 | ++ | + | Focal + | Focal + | + |
| Galectin-3 | ++ | Focal + | ++ | + | Focal + |
| HBME-1 | ++ | Focal + | ++ | + | + |
| PAX8 | ++ | − | ++ | ++ | ++ |
| BRAF (IHC) | ++ | + | ++ | ++ | ++ |
| BRAF (direct sequencing) | Not tested | Positive | Not tested | Positive | Positive |
PTC = papillary thyroid carcinoma, ATC = anaplastic thyroid carcinoma, TTF-1 = thyroid transcription factor-1, Tg = thyroglobulin, CK = cytokeratin, HBME-1 = human bone marrow endothelial cell-1, PAX8 = paired box gene 8.
Case 2
A 56-year-old woman was admitted with a generalized tonic-clonic seizure on October 2013. Subsequent imaging studies found a 2.9 × 2.8 cm mass in the left parietal lobe of brain. Although a gamma knife surgery was performed, the tumor size increased to 5.5 × 5.1 cm over the 5 months following the surgery. Craniotomy and tumor removal were performed and histopathological findings suggested an undifferentiated carcinoma, the origin of which was difficult to determine (Fig. 2A). The patient died one month later owing to rapid growth of the brain tumor.
Fig. 2.

Histological and immunohistochemical features of case 2. (A) Metastatic lesion of the brain shows an undifferentiated histology (H & E staining, × 200). (B-D) Metastatic foci of the brain were negative for TTF-1, (B) but positive for PAX8, (C) and BRAF (D) (× 100). (E, F) The neck node, which was removed one year earlier, shows the presence of papillary carcinoma (E) (H & E, × 200) and a missense mutation in the BRAF gene (c.1799T>A) (F).
H & E = hematoxylin and eosin, TTF-1 = thyroid transcription factor-1, PAX8 = paired box gene 8.
The patient's clinical history revealed that she had been diagnosed with a PTC 12 years previously for which she had undergone a total thyroidectomy with neck node dissection followed by a total of 390 mCi of 131I therapy. The patient exhibited no further signs of disease for 11 years after the treatment, until a palpable neck mass was detected in 2014. She was subsequently diagnosed with PTC recurrence and received a neck mass excision with a modified radical neck node dissection.
The histopathological findings of her brain tumor were different from those obtained from the recurrent PTC, and the serum Tg level at the time was only 3.22 ng/mL (reference range 0–52 ng/mL) with an anti-Tg level of 57 U/mL (reference range 0–60 U/mL) and a thyroid stimulating hormone (TSH) level of < 0.05 μIU/mL (reference range 0.4–4.1 μIU/mL). However, given the PTC history, IHC testing, using various markers, was performed to identify whether the tumor had originated from the PTC or from another source (Table 1). The expression levels of CK7, CK20, and HBME-1 were consistent with those found from the tissue samples. However, thyroid specific markers (TTF-1 and Tg) were present in lower levels in the recurrent neck node and were totally absent in the brain tumor (Fig. 2B). On the other hand, vimentin and p53 had high expression levels, and the PAX8 level was consistently maintained (Table 1, Fig. 2C). Considering the fact that BRAF mutations persist when a brain tumor originates from a PTC with a BRAF mutation, we performed BRAF analyses on the samples. All tissues were positive for the BRAF mutation-specific IHC (Fig. 2D), and the BRAF mutation was confirmed by the direct sequencing of the brain tumor as well as the neck node lesion having features of hobnail-pattern papillary carcinomas (Fig. 2E and 2F). Based on these results, we concluded that her brain tumor was an anaplastic transformation originating from her PTC.
DISCUSSION
Although ATCs may appear de novo, in most cases, they develop by dedifferentiation from preexisting differentiated thyroid carcinoma. Therefore, ATCs often have clinicopathological features originating from the thyroid, which allow for their clear diagnosis. However, in some cases, when an ATC develops in an area remote from the underlying thyroid cancer after a considerable lapse of time and only has undifferentiated histological characteristics, the distinction between ATCs and other undifferentiated neoplasms or soft tissue sarcomas becomes difficult.
Common histological features used for ATC diagnosis are its characteristic epithelioid-squamous and sarcomatoid appearances. The latter is the most frequent patterns seen in ATC and is characterized by the presence of spindle and giant cells in the tissue (5,6,7). In our first patient, the laryngeal tumor showed an atypical histological profile, with tubular structures containing mucin pools with a sarcomatous background. In addition, IHC testing was not able to convincingly prove that the malignancy originated from the thyroid: the test results were negative for TTF-1, Tg, and PAX8. However, the patient had a history of PTC and there was no clinical evidence of another origin. Moreover, both the laryngeal lesion and the recurrent node were positive for the presence of a BRAF mutation, which helped to diagnose the laryngeal tumor as an anaplastic transformation from a previous PTC. Our second patient also had a history of PTC without any other primary malignancies. Her metastatic brain tumor could be diagnosed as an ATC, owing to the consistent levels of PAX8 expression in her IHC samples. In addition, since a BRAF mutation was found in her PTC samples, as well as in those obtained from her brain tumor, we could further confirm the validity of our diagnosis. In both patients, we excluded a diagnosis of cutaneous melanoma, in which BRAF mutations can be detected, because of the negative IHC results of tumor markers for melanoma such as S-100, HMB-45, and Melan-A. Considering the high prevalence of BRAF mutations in PTCs, genetic screening of BRAF mutations can serve as a useful tool for diagnosing ATCs suspected to have arisen from a dedifferentiation of a PTC.
Previous studies suggest that TTF-1 and Tg immunoreactivities are lacking in typical ATCs (8,9) and that loss-of-function mutations in the p53 gene contribute to the progression of a PTC into an ATC (10,11). Similarly, our cases demonstrated that as a well-differentiated PTC progresses to an ATC, the immunoreactivities of TTF-1 and Tg decrease, while those of p53 increase. Furthermore, unlike TTF-1 and Tg, the expression of PAX8 is known to be often retained in ATCs (12). In our first case, the ATC in larynx tested negative for PAX8, but positive for BRAF. This suggests that BRAF could be a more accurate marker than PAX8 for distinguishing ATCs from head and neck cancers in cases of ATC transformed from a BRAF-mutated PTC.
In both the presented cases, a BRAF mutation was detected through both DNA-based direct sequencing and IHC staining, using the mutation-specific antibody clone. Ilie et al. (13) have previously reported that the sensitivity and specificity of BRAF IHC were 98.7% and 100%, respectively. Although direct sequencing assays are the standard method for detecting BRAF mutations, IHC testing for BRAF can be used as a replacement when DNA extraction is difficult due to poor-quality formalin-fixed paraffin-embedded samples, or when quicker results are required.
In conclusion, our cases indicated that BRAF mutation analysis could be an effective diagnostic tool for ATCs, particularly when the patient has a history of PTC and when it is difficult to clinicopathologically distinguish ATCs from the undifferentiated tumors originating from other organs.
Footnotes
Funding: This research was supported by a grant from Seoul National University Hospital (grant number: 26-2015-0020).
DISCLOSURE: The authors have no potential conflicts of interest to disclose.
AUTHOR CONTRIBUTION: Conceptualization: Song YS, Park YJ, Won JK. Data curation: Jung CK, Jung KC, Won JK. Investigation: Jung CK, Jung KC, Won JK. Writing - original draft: Song YS, Won JK.
References
- 1.Nagaiah G, Hossain A, Mooney CJ, Parmentier J, Remick SC. Anaplastic thyroid cancer: a review of epidemiology, pathogenesis, and treatment. J Oncol. 2011;2011:542358. doi: 10.1155/2011/542358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Goutas N, Vlachodimitropoulos D, Bouka M, Lazaris AC, Nasioulas G, Gazouli M. BRAF and K-RAS mutation in a Greek papillary and medullary thyroid carcinoma cohort. Anticancer Res. 2008;28:305–308. [PubMed] [Google Scholar]
- 3.Kim SK, Song KH, Lim SD, Lim YC, Yoo YB, Kim JS, Hwang TS. Clinical and pathological features and the BRAF (V600E) mutation in patients with papillary thyroid carcinoma with and without concurrent Hashimoto thyroiditis. Thyroid. 2009;19:137–141. doi: 10.1089/thy.2008.0144. [DOI] [PubMed] [Google Scholar]
- 4.Nikiforova MN, Kimura ET, Gandhi M, Biddinger PW, Knauf JA, Basolo F, Zhu Z, Giannini R, Salvatore G, Fusco A, et al. BRAF mutations in thyroid tumors are restricted to papillary carcinomas and anaplastic or poorly differentiated carcinomas arising from papillary carcinomas. J Clin Endocrinol Metab. 2003;88:5399–5404. doi: 10.1210/jc.2003-030838. [DOI] [PubMed] [Google Scholar]
- 5.Carcangiu ML, Steeper T, Zampi G, Rosai J. Anaplastic thyroid carcinoma. A study of 70 cases. Am J Clin Pathol. 1985;83:135–158. doi: 10.1093/ajcp/83.2.135. [DOI] [PubMed] [Google Scholar]
- 6.Rosai J, Saxén EA, Woolner L. Undifferentiated and poorly differentiated carcinoma. Semin Diagn Pathol. 1985;2:123–136. [PubMed] [Google Scholar]
- 7.Venkatesh YS, Ordonez NG, Schultz PN, Hickey RC, Goepfert H, Samaan NA. Anaplastic carcinoma of the thyroid. A clinicopathologic study of 121 cases. Cancer. 1990;66:321–330. doi: 10.1002/1097-0142(19900715)66:2<321::aid-cncr2820660221>3.0.co;2-a. [DOI] [PubMed] [Google Scholar]
- 8.LiVolsi VA, Brooks JJ, Arendash-Durand B. Anaplastic thyroid tumors. Immunohistology. Am J Clin Pathol. 1987;87:434–442. doi: 10.1093/ajcp/87.4.434. [DOI] [PubMed] [Google Scholar]
- 9.Miettinen M, Franssila KO. Variable expression of keratins and nearly uniform lack of thyroid transcription factor 1 in thyroid anaplastic carcinoma. Hum Pathol. 2000;31:1139–1145. doi: 10.1053/hupa.2000.16667. [DOI] [PubMed] [Google Scholar]
- 10.Donghi R, Longoni A, Pilotti S, Michieli P, Della Porta G, Pierotti MA. Gene p53 mutations are restricted to poorly differentiated and undifferentiated carcinomas of the thyroid gland. J Clin Invest. 1993;91:1753–1760. doi: 10.1172/JCI116385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Fagin JA. Tumor suppressor genes in human thyroid neoplasms: p53 mutations are associated undifferentiated thyroid cancers. J Endocrinol Invest. 1995;18:140–142. doi: 10.1007/BF03349723. [DOI] [PubMed] [Google Scholar]
- 12.Bishop JA, Sharma R, Westra WH. PAX8 immunostaining of anaplastic thyroid carcinoma: a reliable means of discerning thyroid origin for undifferentiated tumors of the head and neck. Hum Pathol. 2011;42:1873–1877. doi: 10.1016/j.humpath.2011.02.004. [DOI] [PubMed] [Google Scholar]
- 13.Ilie MI, Lassalle S, Long-Mira E, Bonnetaud C, Bordone O, Lespinet V, Lamy A, Sabourin JC, Haudebourg J, Butori C, et al. Diagnostic value of immunohistochemistry for the detection of the BRAF (V600E) mutation in papillary thyroid carcinoma: comparative analysis with three DNA-based assays. Thyroid. 2014;24:858–866. doi: 10.1089/thy.2013.0302. [DOI] [PubMed] [Google Scholar]