

Abstract
AIM
To evaluate the prevalence, risk factors and outcome of acute kidney injury (AKI) in very low birth weight (VLBW) infants.
METHODS
In this retrospective study of VLBW infants, we analyzed the prevalence of AKI, as defined by changes in serum creatinine and urine output, associated risk factors and outcomes.
RESULTS
A total of 293 VLBW infants (mean gestational age 28.7 wk) were included, of whom 109 weighed less than 1000 g at birth. The overall prevalence of AKI was 11.6% (22% in infants with a birth weight under 1000 g and 5.4% those heavier). A total of 19 (55%) affected infants died, with a mortality rate of 58% in infant less than 1000 g and 50% in those heavier. After adjusting for confounding variables, only necrotizing enterocolitis (NEC) remained associated with AKI, with odds ratio of 4.9 (95%CI: 1.9-18.6). Blood pressure and glomerular filtration rate (GFR) were not different between affected infants and the others upon discharge from hospital. A normal GFR was documented in all affected infants at one year of age.
CONCLUSION
Using Kidney Disease Improving Global Outcomes definition of AKI, it occurred in over 10% of VLBW infants, more commonly in infants with lower birth weight. NEC was an independent associated risk factor. Renal function, as defined by GFR, was normal in all surviving affected infants 10 to 12 mo later.
Keywords: Newborn, Case-control, Risk factors, Acute renal failure, Mortality, Kidney Disease Improving Global Outcomes
Core tip: Our study is the first study form United Arab Emirates, dealing with neonatal acute kidney injury (AKI); After using many different definition in reporting AKI in the past, Kidney Disease Improving Global Outcomes started a new definition trying to stage AKI into different stages; Retrospectively our study is using this definition and apply it to all infants admitted to our unite to identify the incidence and risk factors associated with AKI in different gestational age; Our study revealed that extreme premature babies are more susceptible to AKI and this disease is linked to other neonatal morbidities like Necrotizing Enter colitis, sepsis and can predict higher mortality.
INTRODUCTION
At birth the kidneys receive 2.5% to 4% of the cardiac output which subsequently increases to 6%, 10%, 15%, at 24 h, one week and six weeks of age respectively[1,2]. Similarly, the glomerular filtration rate (GFR) improves steadily over the first few months of life, reaching adult level by the age of two years[3,4]. Preterm infants are more likely to develop acute kidney injury (AKI) as they usually require intensive care admission, are more prone to develop sepsis and hypotension, in addition to being administered potentially nephrotoxic medications[5]. AKI is defined as a decline in kidney function that includes fluid imbalance and electrolytes disturbances with elevated waste products[6]. Although serum creatinine (SCr) measurement is commonly used to evaluate kidney function, it unfortunately remains a suboptimal test for kidney injury[5]. This is because a significant loss of kidney function must occur before SCr starts to rise[3]. Furthermore, as in first few days of life the infant’s SCr concentration directly reflects his mother’s, baseline neonatal SCr level cannot easily be defined during that period[7].
Over the last two decades, AKI has been studied in different age group, including neonates[8]. It has been shown to be common in the neonatal period, especially among preterm infants, but also in term infants with birth asphyxia or those requiring extracorporeal membrane oxygenation (ECMO) therapy[9,10]. In very low birth weight (VLBW) neonates, the reported incidence of AKI varied between 12% and 39%, with a mortality rate reaching up to 70%[11-13]. Risk factors associated with it include essentially pre-renal causes[12], VLBW[14], prematurity[14], low Apgar scores[15], sepsis[16,17], hypotension requiring inotropic support[12,17,18], patent ductus arteriosus (PDA)[15], necrotizing enterocolitis (NEC)[12,17], surgery[17], cerebral insult[17] or exposure to nephrotoxic medications such as vancomycin, gentamicin or ibuprofen[15].
Most reports, however, were retrospective single-center studies, with small sample size and using various definitions of AKI. Recently, a simplified definition, staging neonatal AKI into three stages (mild, moderate, and severe) and relying on changes in SCr and urine output, has been developed by the Kidney Disease Improving Global Outcomes (KDIGO)[19]. With this new definition, studies are now needed to validate this definition and its staging system to predict mortality and morbidity. In addition, very little has been published on neonatal AKI in this part of the world.
This study aims, therefore, to retrospectively ascertain the incidence of AKI in VLBW infants admitted to a tertiary neonatal intensive care unit between 2013 and 2015, using the new KDIGO definition. Associated risk factors and outcomes of infants with and without AKI will be evaluated.
MATERIALS AND METHODS
This is a retrospective case-control study on AKI in a cohort of VLBW infants.
Inclusion criteria
VLBW infants admitted to a 41-bed tertiary neonatal intensive care unit (NICU) in Al Ain, United Arab Emirates during a three-year period (between January 1st, 2013- December 31st, 2015) were included.
Exclusion criteria
These included infants with congenital renal disorder or who died in first 24 h of life without enough time to assess kidney function.
Data collection
Data file was retrospectively collected from the patients’ electronic medical record and included: Demographic data (gestational age, birth weight, gender, nationality), maternal age, prenatal exposure to corticosteroid, mode of delivery, occurrence of AKI, associated risk factors (hypotension, need for inotropic medication, intraventricular haemorrhage (IVH), NEC, PDA, duration of mechanical ventilation, sepsis, surgery, placement of umbilical arterial catheter, postnatal medications such as corticosteroids, ibuprofen, dopamine, antibiotics such as gentamycin, vancomycin, urine output if documented, hypotension, estimated GFR calculated during the peak of creatinine rise, therapy with loop diuretics, normal saline bolus infusions, mean blood pressure and SCr at the time of discharge. Outcome data included survival and duration of hospitalization, follow up at 12 mo of age with calculation of the estimated GFR.
AKI was defined using KDIGO criteria in neonates[5,19]. Both, changes in SCr value or urine output were identified for each patient in order to classify the degree of AKI. GFR was calculated with the Schwartz formula using the highest SCr concentration at the time of AKI diagnosis[4]. Sepsis was defined by a positive blood culture. Clinical sepsis was defined when a symptomatic infant had no growth in the blood culture but had elevated serum C reactive protein (CRP) concentration, or leukopenia, or leucocytosis, or an elevated immature to total neutrophils (IT) ratio and received at least seven days of antibiotics[20]. Necrotising enterocolitis was defined according to Bell’s criteria[21] and intra ventricular haemorrhage according to Papile’s classification[22].
The study was approved by the institutional research review board. Statistical analysis was done by a professional biostatistician. The normality of continuous variables was checked with the Shapiro-Wilk W test (only the gestational age had a normal distribution). Normally distributed variables were reported as mean and SD and the others as median value and range. AKI prevalence was reported as mean with 95% confidence intervals (CI).
Patient with AKI (cases) were compared with those without AKI (controls). In the univariate analysis, the comparison of the normally distributed continuous variables was conducted with the Analysis of Variance test (ANOVA) and those with non-normal distribution with the Kruskal-Wallis test. Proportions were compared with the χ2 test and the Fisher exact test was used for small proportions. For all statistical analysis, significance was defined by a 2-tailed P < 0.05.
All factors associated in the univariate model with AKI or mortality of any cause with a P-value < 0.1 were subsequently entered in a logistic regression model. In that model, only the associations with a P-value < 0.05 were considered statistically significant and their odds ratio (OR) with 95%CI were calculated.
RESULTS
A total of 304 patients were included in this study. Eleven patients were excluded due to missing data or congenital renal anomalies or because they died in first 24 h of life. The remaining 293 infants were included in the analysis. Their general characteristics are detailed in Table 1. Some data were missing from a few children.
Table 1.
Characteristics of the 293 studied infants, n (%) unless stated otherwise
| Males | 142 (48) |
| Birth weight (g): median (range) | 1130 (450-1860) |
| Gestational age (mean, SD) | 28.7 (2.8) |
| Mode of delivery | |
| Vaginal delivery | 53 (18) |
| Cesarean section | 240 (82) |
| Maternal steroids | 217 (74) |
| Intraventricular hemorrhage | |
| Grade 1 | 16 (5) |
| Grade 2 | 10 (3) |
| Grade 3 | 13 (5) |
| Grade 4 | 16 (5) |
| Periventricular leukomalacia | 12 (4) |
| Necrotizing enterocolitis | 30 (10) |
| Patent ductus arteriosus | |
| Tiny | 34 (11) |
| Moderate | 39 (13) |
| Large | 25 (8) |
| Sepsis | |
| Clinical sepsis | 61 (21) |
| Sepsis with normotension | 24 (8) |
| Sepsis with hypotension | 26 (9) |
| Duration of mechanical ventilation (d): median (range) | 3 (1-410) |
| Surgery required | 22 (7) |
| Inotrope use | 59 (20) |
| Ibuprofen use | 63 (21) |
| Vancomycin use | 84 (29) |
| Gentamycin use | 203 (69) |
| Post natal Steroids use | 38 (13) |
| Umbilical arterial catheter use | 158 (54) |
| Oliguria | |
| < 0.5 mL/kg per hour for 6 h | 3 (1) |
| < 0.3 mL/kg per hour for 24 h | 10 (3) |
| Hypotension | 58 (20) |
| Normal saline intravenous bolus | 50 (17) |
| Furosemide | 12 (4) |
| Duration of hospital stay (d): median (range) | 49 (1-480) |
| Acute kidney injury | |
| Stage 1 | 6 (2) |
| Stage 2 | 12 (4) |
| Stage 3 | 16 (5) |
| Mortality | 46 (17) |
A total of 34 infants met the definition of AKI, of whom 13 (38%) were diagnosed using urine output criteria. The calculated overall prevalence of AKI was 11.6% (95%CI: 8.1-15.8). In infants with a birth weight under 1000 g, AKI had a prevalence of 22% (95%CI: 14.6-30.9) and in those over 1000 g it was 5.4% (95%CI: 2.6-9.7). The prevalence of the different stages of AKI by age is shown in Table 2 and Figure 1. All stages were more prevalent with lower birth weight. Furthermore, while the prevalence of all AKI stages was the same in infants over 1000 g, the more severe stages were more prevalent in those under 1000 g.
Table 2.
Stages of acute kidney injury in 34 infants by birth weight n (%)
| AKI stages |
Birth weight |
Total n = 293 | |
| ≥ 1000 g n = 184 | < 1000 g n = 109 | ||
| 1 | 2 (1.0) | 4 (3.7) | 6 (2.0) |
| 2 | 3 (1.6) | 9 (8.2) | 12 (4.1) |
| 3 | 5 (2.7) | 11 (10.1) | 16 (5.4) |
| Total | 10 (5.4) | 24 (22.0) | 34 (11.6) |
AKI: Acute kidney injury.
Figure 1.
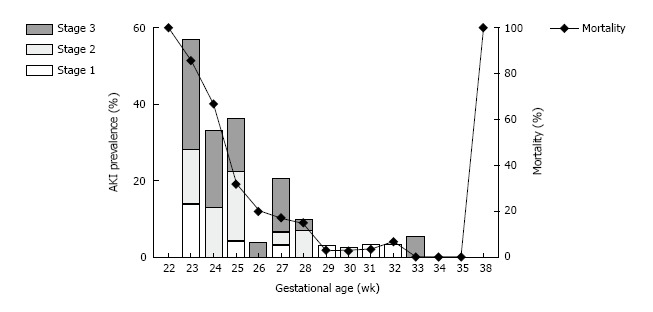
Prevalence of acute kidney injury stages and mortality of all causes (%) by birth weight in 293 low birth weight infants. AKI: Acute kidney injury.
The univariate association of risk factors with AKI is shown in Table 3. Lower birth weight and gestational age, delivery by cesarean section, presence of IVH, NEC, PDA, sepsis, duration of mechanical ventilation, surgery, administration of inotropes, ibuprofen, vancomycin, corticosteroids, normal saline boluses, furosemide, insertion of an umbilical arterial catheter and hypotension were all significantly associated with the development of AKI. However, after adjustment for confounders in a multivariable regression model (Table 3), only NEC remained independently and significantly associated with the development of AKI, with odds ratio of 4.9 (95%CI: 1.9-18.6).
Table 3.
Patients with or without acute kidney injury, n (%) unless stated otherwise
| No AKI n = 259 | Stage 1 AKI n = 6 | Stage 2 AKI n = 12 | Stage 3 AKI n = 16 | Univariate analysis P value | Multivariate analysis4P value | |
| Males | 122 (47) | 4 (67) | 7 (58) | 9 (56) | 0.61 | NS |
| Birth weight (g): mean (SD) | 1130 (267) | 976 (271) | 791 (257) | 850 (253) | < 0.0012 | NS |
| Gestational age (wk): median (range) | 29.0 (22-35) | 28.0 (23-32) | 25.0 (23-30) | 25.5 (23-38) | < 0.0013 | NS |
| Mode of delivery | 0.031 | NS | ||||
| Vaginal delivery | 40 (15) | 1 (17) | 3 (25) | 9 (56) | NS | |
| Cesarean section | 219 (84) | 5 (83) | 9 (75) | 7 (43) | NS | |
| Maternal steroids | 193 (74) | 5 (83) | 8 (67) | 11 (69) | 0.91 | NS |
| Intraventricular hemorrhage | < 0.0011 | NS | ||||
| Grade 1 | 15 (6) | 1 (16) | 0 (0) | 0 (0) | NS | |
| Grade 2 | 8 (3) | 1 (16) | 0 (0) | 1 (6) | NS | |
| Grade 3 | 9 (3) | 1 (16) | 1 (8) | 2 (13) | NS | |
| Grade 4 | 9 (4) | 0 (0) | 1 (8) | 6 (40) | NS | |
| Necrotizing enterocolitis | 16 (6) | 1 (16) | 6 (50) | 7 (43) | < 0.0011 | 0.001 |
| Patent ductus arteriosus | 0.031 | NS | ||||
| Tiny | 29 (11) | 1 (16) | 1 (8) | 3 (18) | NS | |
| Moderate | 32 (12) | 0 (0) | 3 (25) | 4 (25) | NS | |
| Large | 19 (7) | 1 (16) | 3 (25) | 2 (12) | NS | |
| Sepsis | < 0.0011 | NS | ||||
| Clinical sepsis | 45 (17) | 3 (50) | 6 (50) | 7 (43) | NS | |
| Sepsis with normotension | 22 (8) | 1 (16) | 0 (0) | 1 (6) | NS | |
| Sepsis with hypotension | 14 (5) | 1 (16) | 6 (50) | 5 (31) | NS | |
| Duration of mechanical ventilation (d): median (range) | 2 (1-160) | 3.5 (1-29) | 17.5 (7-71) | 13 (2-262) | < 0.0013 | NS |
| Surgery required | 11 (4) | 1 (16) | 4 (33) | 6 (37) | < 0.0011 | NS |
| Inotrope use | 37 (14) | 2 (33) | 8 (66) | 12 (75) | < 0.0011 | NS |
| Ibuprofen use | 51 (19) | 1 (16) | 7 (58) | 4 (25) | 0.011 | NS |
| Vancomycin use | 59 (22) | 3 (50) | 10 (83) | 12 (75) | < 0.0011 | NS |
| Gentamycin use | 173 (66) | 5 (83) | 11 (91) | 14 (87) | 0.081 | NS |
| Steroids use | 24 (9) | 1 (16) | 6 (50) | 7 (43) | < 0.0011 | NS |
| Umbilical arterial catheter use | 129 (49) | 5 (83) | 8 (66) | 16 (100) | < 0.0011 | NS |
| Oliguria | < 0.0011 | NS | ||||
| < 0.5 mL/kg per hour for 6 h | 0 (0) | 0 (0) | 1 (8) | 2 (12) | NS | |
| < 0.3 mL/kg per hour for 24 h | 0 (0) | 1 (16) | 3 (25) | 6 (37) | NS | |
| Hypotension | 35 (13) | 2 (33) | 9 (75) | 12 (75) | < 0.0011 | NS |
| Normal saline intravenous bolus | 28 (10) | 2 (33) | 9 (75) | 11 (68) | < 0.0011 | NS |
| Furosemide | 4 (1) | 1 (16) | 3 (25) | 4 (25) | < 0.0011 | NS |
| Duration of hospital stay in survivors (d): median (range) | 52 (15-280) | 64.5 (53-125) | 74.5 (7-116) | 116 (44-362) | 0.023 | NS |
| Mortality | 27 (10) | 2 (33) | 8 (66) | 9 (56) | < 0.0011 | NS |
| Serum creatinine (µmol/L) on discharge: median (range) | 44 (23) | 64 (56) | 93 (47) | 133 (135) | < 0.0013 | NS |
| Mean blood pressure (mmHg) on discharge: median (range) | 55 (13) | 48 (24) | 38 (13) | 41 (19) | < 0.0013 | NS |
χ2 or Fisher exact test;
Analysis of variance (ANOVA);
Kruskal-Wallis test;
Logistic regression. NS: Not significant; AKI: Acute kidney injury.
Table 4 shows the duration of hospital stay and the mortality of any cause in the infants with AKI. Length of hospital stay was significantly longer in surviving infants with a developed AKI (P = 0.003). Mortality was significantly higher in infants under 1000 g than in heavier neonates and increased significantly in those who developed AKI in both weight groups (Table 4 and Figure 1). After adjusting for confounders in a multivariable regression model, the only factors significantly associated with mortality were the presence of AKI (OR = 4.4, 95%CI: 1.3-14.5, P = 0.01), NEC (OR = 3.1, 95%CI: 0.9-10.0, P = 0.05) and sepsis (OR = 19.5, 95%CI: 2.1-181.4, P = 0.009).
Table 4.
Outcomes, n (%) unless stated otherwise
| No AKI n = 259 | Any stage AKI n = 34 | P value | |
| Length of stay in survivors: median (range) | |||
| BW ≤ 1000 g (n = 108) | 82 (37-280) | 112 (7-362) | 0.32 |
| BW > 1000 g (n = 184) | 40 (15-149) | 53 (35-137) | 0.0032 |
| Mortality of any cause | |||
| BW ≤ 1000 g (n = 108) | 18 (21) | 14 (58) | < 0.0011 |
| BW > 1000 g (n = 184) | 9 (5) | 5 (50) | < 0.0011 |
χ2 or Fisher exact test;
Kruskal-Wallis test. Number of infants in birth weight categories is not identical in all outcomes as some data was missing. AKI: Acute kidney injury; BW: Birth weight.
There was no significant difference in SCr or blood pressure between surviving affected infants and the others at discharge from hospital (Table 3). At one year of age, the mean (SD) GFR of the surviving affected infants was 80.7 (25.6) mL/min per 1.73 m2, with a mean (SD) increase of 69.8 (28.4) mL/min per 1.73 m2 since the diagnosis of AKI, with no child requiring renal replacement therapy. None of the surviving infants with AKI were given follow up appointment with a pediatric nephrologist at the time of discharge.
DISCUSSION
In this study, the prevalence of AKI using the new KDIGO definition was 11.6%. Applying the KDIGO criteria for defining stage one AKI in this cohort of 304 infants was challenging. The lack of measurement and documentation of hourly urine output, associated with the difficulty in having two SCr levels measured 48 h apart made the diagnosis of stage 1 AKI difficult to achieve. This may explain the lower prevalence of AKI in our series when compared to a previous report. Similar to another recent study using the new definition, our results confirmed that smaller infants are more likely to develop AKI stage 2 or 3, with also a higher mortality[23].
Among the risk factors, only NEC was significantly and independently associated with AKI. The development of NEC in an infant should alert the neonatologist to the increased risk of AKI with the need to closely monitor hemodynamics, kidney function and urine output. As the value of hemodynamic assessment in VLBW infants is based on unreliable interpretation of their vital signs, newer biomarkers, such as neutrophil gelatinase-associated lipocalin and serum cystatin C[12,13,24,25], or non-invasive newer techniques such as near-infrared spectroscopy[26] may aid in the early detection of AKI in these children at higher risk.
Although the duration of hospital stay was longer with increasing grades of AKI, the difference was not statistically significant. In infants weighing less than 1000 g, there was no difference between those who developed AKI of any grade and the others. This could be explained by their higher mortality rate, exceeding 58%. However, in surviving infants, hospital stay was significantly longer in neonates who developed AKI than those who did not. All the 19 surviving infants who had AKI in the neonatal period were followed for one year and had GFR in the normal range.
Weaknesses in this study included its retrospective design, with missing data on some infants. The relatively small sample size may have precluded the estimation of the association of AKI with some of the risk factors. In addition, the urine output KDIGO criterion to define AKI was difficult to obtain because the urine output was not documented on an hourly basis, but was only documented by the physicians whenever it exceeded 24 h. Similarly, the other KDIGO criterion to define AKI stage one (increase in SCr by 0.3 mg/dL in the previous 48 h) was not available for all infants as it was not clinically indicated before the onset of AKI.
AKI is common in VLBW infants, with a high mortality rate, and is significantly and independently associated with NEC. Despite the difficulty is recognizing grade one AKI because of the unavailability of some of the data, AKI staging using the KDIGO criteria is a strong predictor of mortality. A longer follow up of surviving VLBW infants with AKI is still required.
ACKNOWLEDGMENTS
We are grateful to the staff of the neonatal intensive care unit for their support in taking care of the infants and allowing us to analyze the data.
COMMENTS
Background
Acute kidney injury (AKI) is defined as a decline in kidney function that includes fluid imbalance and electrolytes disturbances with elevated waste products. It is commonly reported in preterm infants and, recently, the Kidney Disease Improving Global Outcomes (KDIGO) has advocated a simplified definition of neonatal AKI, dividing it into three stages based on changes in serum creatinine and urine output. As more data is needed on the prevalence of that condition and its outcome in very low birth weight (VLBW) infants based on that new definition, the authors report recent experience in a tertiary neonatal intensive care unit. The authors report the prevalence of AKI, its associated risk factors and outcomes, including post-discharge follow up results of serum creatinine and blood pressure.
Research frontiers
Very little has been published on neonatal AKI in the Gulf region and only a limited number of studies in developed countries have tried to evaluate this new definition of AKI, with its validity in predicting the outcome of affected VLBW infants. Long term follow of these infants after discharge is also currently lacking. This study attempts to address these current limitations.
Innovations and breakthroughs
AKI was common in VLBW infants and carries a high mortality rate. It is significantly and independently associated with necrotizing enterocolitis (NEC). The new KDIGO AKI staging criteria strongly predict mortality. Blood pressure (BP) and glomerular filtration rate (GFR) were not different between surviving affected infants and the others upon discharge from hospital and all affected infants had a normal GFR up to one year of age.
Applications
AKI is common in VLBW infants and the new KDIGO definition strongly predicts mortality and long-term outcome. AKI is associated with other neonatal illness, especially NEC. Longer follow up studies of affected infants, including BP, are still required.
Peer-review
This is a very good manuscript facing with the new classification of AKI in infants according KDIGO.
Footnotes
Institutional review board statement: The paper was reviewed by the Al Ain Medical District Human Research Ethics Committee.
Informed consent statement: Institutional review board did not request informed consent, as this is a chart review requires no interaction with patients, but all requirements protect patient confidentiality were fulfilled during data collection process.
Conflict-of-interest statement: None to declare.
Data sharing statement: None.
Manuscript source: Unsolicited manuscript
Specialty type: Urology and nephrology
Country of origin: United Arab Emirates
Peer-review report classification
Grade A (Excellent): 0
Grade B (Very good): B
Grade C (Good): C
Grade D (Fair): 0
Grade E (Poor): 0
Peer-review started: March 20, 2017
First decision: May 8, 2017
Article in press: July 23, 2017
P- Reviewer: Markic D, Salvadori M S- Editor: Ji FF L- Editor: A E- Editor: Lu YJ
Contributor Information
Maisa Al Malla, Department of Paediatrics, Tawam Hospital, P.O. Box 15258, Al Ain, United Arab Emirates. mmalla@seha.ae.
Nisha Viji Varghese, Department of Paediatrics, Tawam Hospital, P.O. Box 15258, Al Ain, United Arab Emirates.
Mustafa AlAbdullatif, Department of Paediatrics, Tawam Hospital, P.O. Box 15258, Al Ain, United Arab Emirates.
Hassib Narchi, Department of Paediatrics, United Arab Emirates University, P.O. Box 15551, Al Ain, United Arab Emirates.
Mohammad Khassawneh, Department of Paediatrics, Tawam Hospital, P.O. Box 15258, Al Ain, United Arab Emirates; Department of paediatrics, Jordan University of Science and Technology, Irbid 22110, Jordan.
References
- 1.Selewski DT, Charlton JR, Jetton JG, Guillet R, Mhanna MJ, Askenazi DJ, Kent AL. Neonatal Acute Kidney Injury. Pediatrics. 2015;136:e463–e473. doi: 10.1542/peds.2014-3819. [DOI] [PubMed] [Google Scholar]
- 2.Saint-Faust M, Boubred F, Simeoni U. Renal development and neonatal adaptation. Am J Perinatol. 2014;31:773–780. doi: 10.1055/s-0033-1361831. [DOI] [PubMed] [Google Scholar]
- 3.Abitbol CL, Seeherunvong W, Galarza MG, Katsoufis C, Francoeur D, Defreitas M, Edwards-Richards A, Master Sankar Raj V, Chandar J, Duara S, et al. Neonatal kidney size and function in preterm infants: what is a true estimate of glomerular filtration rate? J Pediatr. 2014;164:1026–1031.e2. doi: 10.1016/j.jpeds.2014.01.044. [DOI] [PubMed] [Google Scholar]
- 4.Brion LP, Fleischman AR, McCarton C, Schwartz GJ. A simple estimate of glomerular filtration rate in low birth weight infants during the first year of life: noninvasive assessment of body composition and growth. J Pediatr. 1986;109:698–707. doi: 10.1016/s0022-3476(86)80245-1. [DOI] [PubMed] [Google Scholar]
- 5.Askenazi DJ, Ambalavanan N, Goldstein SL. Acute kidney injury in critically ill newborns: what do we know? What do we need to learn? Pediatr Nephrol. 2009;24:265–274. doi: 10.1007/s00467-008-1060-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jetton JG, Askenazi DJ. Acute kidney injury in the neonate. Clin Perinatol. 2014;41:487–502. doi: 10.1016/j.clp.2014.05.001. [DOI] [PubMed] [Google Scholar]
- 7.Auron A, Mhanna MJ. Serum creatinine in very low birth weight infants during their first days of life. J Perinatol. 2006;26:755–760. doi: 10.1038/sj.jp.7211604. [DOI] [PubMed] [Google Scholar]
- 8.Alkandari O, Eddington KA, Hyder A, Gauvin F, Ducruet T, Gottesman R, Phan V, Zappitelli M. Acute kidney injury is an independent risk factor for pediatric intensive care unit mortality, longer length of stay and prolonged mechanical ventilation in critically ill children: a two-center retrospective cohort study. Crit Care. 2011;15:R146. doi: 10.1186/cc10269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Blinder JJ, Goldstein SL, Lee VV, Baycroft A, Fraser CD, Nelson D, Jefferies JL. Congenital heart surgery in infants: effects of acute kidney injury on outcomes. J Thorac Cardiovasc Surg. 2012;143:368–374. doi: 10.1016/j.jtcvs.2011.06.021. [DOI] [PubMed] [Google Scholar]
- 10.Selewski DT, Jordan BK, Askenazi DJ, Dechert RE, Sarkar S. Acute kidney injury in asphyxiated newborns treated with therapeutic hypothermia. J Pediatr. 2013;162:725–729.e1. doi: 10.1016/j.jpeds.2012.10.002. [DOI] [PubMed] [Google Scholar]
- 11.Askenazi D, Patil NR, Ambalavanan N, Balena-Borneman J, Lozano DJ, Ramani M, Collins M, Griffin RL. Acute kidney injury is associated with bronchopulmonary dysplasia/mortality in premature infants. Pediatr Nephrol. 2015;30:1511–1518. doi: 10.1007/s00467-015-3087-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Viswanathan S, Manyam B, Azhibekov T, Mhanna MJ. Risk factors associated with acute kidney injury in extremely low birth weight (ELBW) infants. Pediatr Nephrol. 2012;27:303–311. doi: 10.1007/s00467-011-1977-8. [DOI] [PubMed] [Google Scholar]
- 13.Carmody JB, Swanson JR, Rhone ET, Charlton JR. Recognition and reporting of AKI in very low birth weight infants. Clin J Am Soc Nephrol. 2014;9:2036–2043. doi: 10.2215/CJN.05190514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Koralkar R, Ambalavanan N, Levitan EB, McGwin G, Goldstein S, Askenazi D. Acute kidney injury reduces survival in very low birth weight infants. Pediatr Res. 2011;69:354–358. doi: 10.1203/PDR.0b013e31820b95ca. [DOI] [PubMed] [Google Scholar]
- 15.Cataldi L, Leone R, Moretti U, De Mitri B, Fanos V, Ruggeri L, Sabatino G, Torcasio F, Zanardo V, Attardo G, et al. Potential risk factors for the development of acute renal failure in preterm newborn infants: a case-control study. Arch Dis Child Fetal Neonatal Ed. 2005;90:F514–F519. doi: 10.1136/adc.2004.060434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Stojanović V, Barišić N, Milanović B, Doronjski A. Acute kidney injury in preterm infants admitted to a neonatal intensive care unit. Pediatr Nephrol. 2014;29:2213–2220. doi: 10.1007/s00467-014-2837-0. [DOI] [PubMed] [Google Scholar]
- 17.Bruel A, Rozé JC, Flamant C, Simeoni U, Roussey-Kesler G, Allain-Launay E. Critical serum creatinine values in very preterm newborns. PLoS One. 2013;8:e84892. doi: 10.1371/journal.pone.0084892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Blatt NB, Srinivasan S, Mottes T, Shanley MM, Shanley TP. Biology of sepsis: its relevance to pediatric nephrology. Pediatr Nephrol. 2014;29:2273–2287. doi: 10.1007/s00467-013-2677-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Group AKIW. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl. 2012;2:1–138. [Google Scholar]
- 20.Mathur NB, Agarwal HS, Maria A. Acute renal failure in neonatal sepsis. Indian J Pediatr. 2006;73:499–502. doi: 10.1007/BF02759894. [DOI] [PubMed] [Google Scholar]
- 21.Gregory KE, Deforge CE, Natale KM, Phillips M, Van Marter LJ. Necrotizing enterocolitis in the premature infant: neonatal nursing assessment, disease pathogenesis, and clinical presentation. Adv Neonatal Care. 2011;11:155–164; quiz 165-166. doi: 10.1097/ANC.0b013e31821baaf4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr. 1978;92:529–534. doi: 10.1016/s0022-3476(78)80282-0. [DOI] [PubMed] [Google Scholar]
- 23.Maqsood S, Fung N, Chowdhary V, Raina R, Mhanna MJ. Outcome of extremely low birth weight infants with a history of neonatal acute kidney injury. Pediatr Nephrol. 2017;32:1035–1043. doi: 10.1007/s00467-017-3582-y. [DOI] [PubMed] [Google Scholar]
- 24.Mishra J, Ma Q, Prada A, Mitsnefes M, Zahedi K, Yang J, Barasch J, Devarajan P. Identification of neutrophil gelatinase-associated lipocalin as a novel early urinary biomarker for ischemic renal injury. J Am Soc Nephrol. 2003;14:2534–2543. doi: 10.1097/01.asn.0000088027.54400.c6. [DOI] [PubMed] [Google Scholar]
- 25.Trof RJ, Di Maggio F, Leemreis J, Groeneveld AB. Biomarkers of acute renal injury and renal failure. Shock. 2006;26:245–253. doi: 10.1097/01.shk.0000225415.5969694.ce. [DOI] [PubMed] [Google Scholar]
- 26.Ruf B, Bonelli V, Balling G, Hörer J, Nagdyman N, Braun SL, Ewert P, Reiter K. Intraoperative renal near-infrared spectroscopy indicates developing acute kidney injury in infants undergoing cardiac surgery with cardiopulmonary bypass: a case-control study. Crit Care. 2015;19:27. doi: 10.1186/s13054-015-0760-9. [DOI] [PMC free article] [PubMed] [Google Scholar]