

Abstract
This study provides support for the hypothesis that treatment response to an initial course of repetitive transcranial magnetic stimulation (rTMS) for depression predicts the magnitude of response to a subsequent course of rTMS in the setting of symptom relapse.
Repetitive transcranial magnetic stimulation (rTMS) has emerged as a safe and effective treatment option for patients with treatment-resistant major depression.1 The treatment course typically includes 4–6 weeks of once-daily sessions, five times per week. Response to treatment is variable, with response rates reported between 45% and 60% and remission rates between 30% and 40%.2,3 The benefits of treatment can be limited in duration. While most patients who respond maintain clinical improvement 12 months later, there is much variability in the duration of response, and the best strategies to sustain the antidepressant effect of rTMS remain undefined.2,4 Given the enormous burden of treatment-resistant depression to both patients and society,5,6 establishing effective, long-term treatment strategies is of the upmost importance.
Continuing rTMS sessions less frequently than during induction has been suggested, in the form of either continuation or maintenance therapy, but evidence-based protocols are still under investigation.7–9 Some studies have shown that multiple sessions a week of rTMS directly following the end of induction can help prevent relapse in responders to induction therapy.8,10 Other studies have shown that, among responders who are not concurrently using antidepressant medications, monthly follow-up rTMS treatments are not effective.9
Among responders to rTMS treatment, one possible alternative to maintenance therapy is to withhold additional rTMS while the clinical benefit is sustained (i.e., watchful waiting) and then to treat with a second course of rTMS if symptomatic relapse occurs. This option has been referred to as reintroduction of rTMS. Typically, this involves treating relapses using a protocol resembling induction, with treatments up to 3–5 times per week for 2–6 weeks.2,4,9,11 When considering reintroduction, it is important to know whether the initial treatment response to rTMS predicts subsequent response. This question has received relatively little investigation to date, though preliminary analyses suggest that a favorable response to induction may predict favorable responses to subsequent courses.2,4,9,11 Here, we test the hypothesis that response to a first treatment course predicts response to reintroduction.
Methods
A retrospective chart review was performed for 225 patients who received rTMS for treatment-resistant depression as a part of the clinical program at the Berenson-Allen Center between 2000 and 2015. We identified all patients with treatment-resistant depression (≥2 failed medication trials) who underwent a standard rTMS treatment course and subsequent reintroduction in the setting of symptom relapse. Reintroduction was defined for the current analysis as ≥3 treatment sessions per week for at least 2 weeks and up to 2 months, or 30 sessions. Only patients with valid pre- and posttreatment Beck Depression Inventory (BDI) data for each course of rTMS were included (Figure 1). Percent change in BDI was used as a metric of response, with treatment response defined as a greater than 50% reduction in BDI scores over the course of treatment and partial response as 25%−50% reduction.12 Normal distribution of continuous variables was verified according to the comparison of mean and median, kurtosis, skewness, and the D'Agostino-Pearson (omnibus K2) test. Correlation coefficients were calculated to evaluate the relationship between antidepressant response to the reintroduction course with other continuous variables, namely response to the initial rTMS course, age, number of reintroduction treatment sessions, days between rTMS courses, and baseline severity of depression at reintroduction. Pearson correlation coefficients were used in all cases except days between rTMS courses, which was the only variable that was not normally distributed, leading to use of the Spearman correlation coefficient. Variables that correlated significantly with antidepressant response to the reintroduction were included in a linear regression model to test for potential predictors of antidepressant response to the reintroduction. For the regression model, data transformations and polynomial models were used to test the best fit, model assumptions were tested by analyses of residuals, and influence diagnostics were conducted using Cook's distance. Antidepressant response was compared between courses using a paired-samples t test and according to gender or response status using independent-samples t tests. Unless otherwise noted, group data are presented in the text as mean±standard error (SE).
Figure 1.
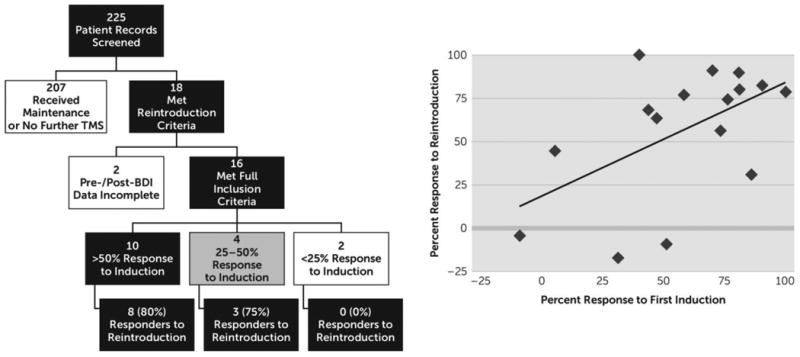
a A total of 225 patient charts were reviewed, with 18 patients meeting reintroduction criteria. Two of these patients were excluded due to lack of adequate Beck Depression Inventory (BDI) data. Of 16 patients identified, 11 had a favorable response to reintroduction (>50% improvement on BDI). All 11 patients that responded to reintroduction had at least a 40% improvement in BDI scores during the initial treatment course. Treatment response, measured according to percent change in BDI, was similar between the first and second course of treatment (57.9±7.7% and 56.5±9.4%, respectively; paired-samples t test, p=0.9), and the values were significantly correlated (r=0.54, p=0.03).
Results
Sixteen patients received reintroduction of rTMS and met all the aforementioned inclusion criteria (Figure 1). In this patient cohort, 37.5% of patients were male, mean age at initial induction was 52.2±2.5 years, mean number of prior medication trials was 5.3±0.6, and mean BDI prior to initial induction was 29.8±3.0. For these 16 patients, the average percent change in BDI across induction was similar to that after reintroduction (57.9±7.7% and 56.5±9.4%, respectively; paired-samples t test, p=0.9) (Figure 1). Ten of 16 (62.5%) patients were responders to the initial rTMS treatment course, and 11 of 16 (68.8%) patients were responders to reintroduction. Eight of the 10 (80%) responders to the initial treatment course were also responders to reintroduction, and the remaining three responders to reintroduction were partial responders to initial induction (Figure 1). Response to the initial rTMS course was the only variable that correlated significantly with response to reintroduction (r=0.54, p<0.04) (Figure 1), with no other variables approaching significance. In fact, response to the initial rTMS course was confirmed as a significant predictor of response to reintroduction in a simple linear regression model (β=0.66, p<0.04; R2=0.29). Responders to reintroduction were also found to have significantly greater response to the initial course compared with those who were nonresponders to reintroduction (69.2±5.9% and 32.9±16.8%, respectively; independent-samples t test, p<0.03).
Discussion
The results presented above support the hypothesis that therapeutic response to an initial course of rTMS for depression is a significant predictor of response to a subsequent course. This finding is consistent with other literature on treatment response, with several authors reporting high response rates to reintroduction in patients who had responded initially.2,4,9,11 Our work, showing that the magnitude of initial antidepressant explains approximately one-third of the magnitude of response to reintroduction, has implications for management of depressed patients with a past favorable response to rTMS. We provide support for an approach involving watchful waiting and reintroduction of TMS when such patients experience a relapse, thus placing rTMS as a viable long-term treatment regimen for treatment-resistant depression. There is also an indication that those who do not respond (BDI change <25%) to initial induction may be less likely to respond to further treatment, but this topic warrants evaluation in larger samples of nonresponders.
The current findings are consistent with the existing literature on the topic of reintroduction. In 2000, Dannon et al.13 reported a case series of four patients who responded to a course of reintroduction to a similar degree relative to the induction course. In 2006, Fitzgerald et al.14 followed 19 responders who received reintroduction, showing that 12 responded (63%) and 17 of 19 had at least a near response (25% improvement). Two years later, Demirtas-Tatlidede et al.11 showed, in a case series of 14 patients, that treatment response to rTMS was reproducible after relapse, with patients receiving reintroduction on average every 5 months. Janicak et al.4 showed, in 2010, that within the first 6 months after induction treatment, 38 of 99 patients experienced symptom worsening, with 32 of 36 (84%) benefitting from reintroduction of TMS. More recently, in a large naturalistic observational study lasting 12 months, Dunner et al.2 showed that, among 98 patients receiving reintroduction in the setting of symptom worsening, those with the best response to induction were the least likely to experience a relapse after reintroduction. Our findings build on the literature summarized above, showing that the best indicator of response to reintroduction is response to induction. Importantly, these findings also give both patients and physicians an understanding that magnitude of response to reintroduction will likely be similar to the initial response.
Patients treated with rTMS tend to have severe, refractory depression. Thus, converting initial therapeutic response into successful long-term management represents an important and still under-investigated topic for the field. Currently, there is no clear consensus on how this should best be accomplished. These findings, along with the literature reviewed above, contribute to this ongoing discussion. Limitations of the study include a relatively small and heterogeneous sample identified retrospectively via chart review. Moreover, though initial response was found to be a significant predictor of reintroduction response, it only accounts for 29% of the variance in scores. Thus, other factors, either not evaluated in this study or requiring a larger sample size to achieve significance, such as gender, age, refractoriness, baseline severity, and comorbid disorders, could also have a significant predictive role.15 However, the current study results reflect the experience of a clinical program and thus have practical relevance. Furthermore, we hope these findings may spur additional prospective research, ideally comparing long-term rTMS treatment strategies, including maintenance rTMS and a combination of watchful waiting and reintroduction therapy upon symptomatic relapse.
Acknowledgments
Funded by the Sidney R. Baer Jr. Foundation (4K12HD027748-24, NIH/NINDS R25NS065743-05) and Harvard Catalyst|The Harvard Clinical and Translational Science Center (NCRR and the NCATS NIH, UL1 RR025758 TR001102 and financial contributions from Harvard University and its affiliated academic healthcare centers).
Footnotes
Previously presented as a poster at the 2016 Annual Meeting of the Clinical TMS Society, May 14, 2016, Atlanta.
The content in this article is solely the responsibility of the authors and does not necessarily represent the official views of Harvard Catalyst, Harvard University and its affiliated academic health care centers, the National Institutes of Health, or the Sidney R. Baer Jr. Foundation.
Dr. Pascual-Leone serves on the scientific advisory boards of Constant Therapy, Neosync, Neuroelectrics, Neuronix, Novavision, Nexstim, and Starlab Neuroscience; and he is listed as the inventor in issued patents and patent applications on the real-time integration of transcranial magnetic stimulation with electroencephalography) and magnetic resonance imaging. All other authors report no financial relationships with commercial interests.
Contributor Information
Michael S. Kelly, Berenson-Allen Center for Noninvasive Brain Stimulation, Division of Cognitive Neurology, Department of Neurology, Harvard Medical School and Beth Israel Deaconess Medical Center, Boston; University of Rochester School of Medicine and Dentistry, University of Rochester Medical Center, Rochester, N.Y.
Albino J. Olibeira-Maia, Berenson-Allen Center for Noninvasive Brain Stimulation, Division of Cognitive Neurology, Department of Neurology, Harvard Medical School and Beth Israel Deaconess Medical Center, Boston; Champalimaud Research and Clinical Centre, Champalimaud Centre for the Unknown, Lisboa, Portugal; Department of Psychiatry and Mental Health, Centro Hospitalar de Lisboa Ocidental, Lisboa, Portugal; NOVA Medical School, Faculdade de Ciências Médicas, Universidade Nova de Lisboa, Lisboa, Portugal.
Margo Bernstein BA, Berenson-Allen Center for Noninvasive Brain Stimulation, Division of Cognitive Neurology, Department of Neurology, Harvard Medical School and Beth Israel Deaconess Medical Center, Boston.
Adam P. Stern, Berenson-Allen Center for Noninvasive Brain Stimulation, Division of Cognitive Neurology, Department of Neurology, Harvard Medical School and Beth Israel Deaconess Medical Center, Boston; Department of Psychiatry at BIDMC.
Daniel Z. Press, Berenson-Allen Center for Noninvasive Brain Stimulation, Division of Cognitive Neurology, Department of Neurology, Harvard Medical School and Beth Israel Deaconess Medical Center, Boston.
Alvaro Pascual-Leone, Berenson-Allen Center for Noninvasive Brain Stimulation, Division of Cognitive Neurology, Department of Neurology, Harvard Medical School and Beth Israel Deaconess Medical Center, Boston.
Aaron D. Boes, Berenson-Allen Center for Noninvasive Brain Stimulation, Division of Cognitive Neurology, Department of Neurology, Harvard Medical School and Beth Israel Deaconess Medical Center, Boston; Noninvasive Brain Stimulation Clinical Program, Departments of Pediatrics and Neurology, University of Iowa Hospitals and Clinics, Iowa City, Iowa.
References
- 1.Gaynes BN, Lloyd SW, Lux L, et al. Repetitive transcranial magnetic stimulation for treatment-resistant depression: a systematic review and meta-analysis. J Clin Psychiatry. 2014;75:477–489. doi: 10.4088/JCP.13r08815. quiz 489. [DOI] [PubMed] [Google Scholar]
- 2.Dunner DL, Aaronson ST, Sackeim HA, et al. A multisite, naturalistic, observational study of transcranial magnetic stimulation for patients with pharmacoresistant major depressive disorder: durability of benefit over a 1-year follow-up period. J Clin Psychiatry. 2014;75:1394–1401. doi: 10.4088/JCP.13m08977. [DOI] [PubMed] [Google Scholar]
- 3.Carpenter LL, Janicak PG, Aaronson ST, et al. Transcranial magnetic stimulation (TMS) for major depression: a multisite, naturalistic, observational study of acute treatment outcomes in clinical practice. Depress Anxiety. 2012;29:587–596. doi: 10.1002/da.21969. [DOI] [PubMed] [Google Scholar]
- 4.Janicak PG, Nahas Z, Lisanby SH, et al. Durability of clinical benefit with transcranial magnetic stimulation (TMS) in the treatment of pharmacoresistant major depression: assessment of relapse during a 6-month, multisite, open-label study. Brain Stimulat. 2010;3:187–199. doi: 10.1016/j.brs.2010.07.003. [DOI] [PubMed] [Google Scholar]
- 5.Mrazek DA, Hornberger JC, Altar CA, et al. A review of the clinical, economic, and societal burden of treatment-resistant depression: 1996–2013. Psychiatr Serv. 2014;65:977–987. doi: 10.1176/appi.ps.201300059. [DOI] [PubMed] [Google Scholar]
- 6.Greenberg PE, Fournier AA, Sisitsky T, et al. The economic burden of adults with major depressive disorder in the United States (2005 and 2010) J Clin Psychiatry. 2015;76:155–162. doi: 10.4088/JCP.14m09298. [DOI] [PubMed] [Google Scholar]
- 7.Perera T, George MS, Grammer G, et al. The Clinical TMS Society Consensus Review and Treatment Recommendations for TMS Therapy for Major Depressive Disorder. Brain Stimul. 2016;9:336–346. doi: 10.1016/j.brs.2016.03.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Richieri R, Guedj E, Michel P, et al. Maintenance transcranial magnetic stimulation reduces depression relapse: a propensity-adjusted analysis. J Affect Disord. 2013;151:129–135. doi: 10.1016/j.jad.2013.05.062. [DOI] [PubMed] [Google Scholar]
- 9.Philip NS, Dunner DL, Dowd SM, et al. Can medication free, treatment-resistant, depressed patients who initially respond to TMS be maintained off medications? a prospective, 12-month multisite randomized pilot study. Brain Stimul. 2015;9:251–257. doi: 10.1016/j.brs.2015.11.007. [DOI] [PubMed] [Google Scholar]
- 10.Levkovitz Y, Isserles M, Padberg F, et al. Efficacy and safety of deep transcranial magnetic stimulation for major depression: a prospective multicenter randomized controlled trial. World Psychiatry. 2015;14:64–73. doi: 10.1002/wps.20199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Demirtas-Tatlidede A, Mechanic-Hamilton D, Press DZ, et al. An open-label, prospective study of repetitive transcranial magnetic stimulation (rTMS) in the long-term treatment of refractory depression: reproducibility and duration of the antidepressant effect in medication-free patients. J Clin Psychiatry. 2008;69:930–934. doi: 10.4088/jcp.v69n0607. [DOI] [PubMed] [Google Scholar]
- 12.Hirschfeld RMA, Montgomery SA, Aguglia E, et al. Partial response and nonresponse to antidepressant therapy: current approaches and treatment options. J Clin Psychiatry. 2002;63:826–837. doi: 10.4088/jcp.v63n0913. [DOI] [PubMed] [Google Scholar]
- 13.Dannon PN, Schreiber S, Dolberg OT, et al. Transcranial magnetic stimulation is effective in the treatment of relapse of depression. Int J Psychiatry Clin Pract. 2000;4:223–226. doi: 10.1080/13651500050518118. [DOI] [PubMed] [Google Scholar]
- 14.Fitzgerald PB, Benitez J, de Castella AR, et al. Naturalistic study of the use of transcranial magnetic stimulation in the treatment of depressive relapse. Aust N Z J Psychiatry. 2006;40:764–768. doi: 10.1080/j.1440-1614.2006.01881.x. [DOI] [PubMed] [Google Scholar]
- 15.Lisanby SH, Husain MM, Rosenquist PB, et al. Daily left prefrontal repetitive transcranial magnetic stimulation in the acute treatment of major depression: clinical predictors of outcome in a multisite, randomized controlled clinical trial. Neuropsychopharmacology. 2009;34:522–534. doi: 10.1038/npp.2008.118. [DOI] [PubMed] [Google Scholar]