

Abstract
Surgeons’ mental and physical workloads are major focuses of operating room (OR) ergonomics, and studies on this topic have generally focused on either mental workload or physical workload, ignoring the interaction between them. Previous studies have shown that physically demanding work may affect mental performance and may be accompanied by impaired mental processing and decreased performance. In this study, 14 participants were recruited to perform laparoscopic cholecystectomy (LC) procedures in a virtual simulator. Surface electromyography (sEMG) signals of the bilateral trapezius, bicipital, brachioradialis and flexor carpi ulnaris (FCU) muscles and eye-tracking signals were acquired during the experiment. The results showed that the least square means of muscle activity during the LC phases of surgery in an all-participants mixed effects model were 0.79, 0.81, and 0.98, respectively. The observed muscle activities in the different phases exhibited some similarity, while marked differences were found between the forearm bilateral muscles. Regarding mental workload, significant differences were observed in pupil dilation between the three phases of laparoscopic surgery. The mental and physical workloads of laparoscopic surgeons do not appear to be generally correlated, although a few significant negative correlations were found. This result further indicates that mental fatigue does markedly interfere with surgeons’ operating movements.
Introduction
Surgeons encounter musculoskeletal strain and disorders resulting from long periods of muscle tension and awkward poses1–3. Injuries to surgeons include pain in specific areas of the body, vertebral disk prolapse and carpal tunnel syndrome4,5. These issues are closely related to the mental and physical workloads of surgeons during surgery2. In terms of mental workload, surgeons can suffer from impaired concentration and slow reactions after long operations. Furthermore, job dissatisfaction of surgeons is considered to be significantly associated with burnout6. As muscle fatigue and attention deficit may contribute to failed surgeries, risk monitoring and risk reduction measures should be implemented if a surgeon is experiencing physical or mental overload or fatigue. Surgeons’ mental and physical workloads have been a focus of operating room (OR) ergonomics over the last few decades.
To assess surgeons’ mental and physical workloads, laparoscopic box trainers and virtual reality simulators are usually employed and are comparable in most aspects7,8. Some studies have suggested that virtual simulators may be more reliable and convenient, and peg transfer, ball pick-and-drop, and cutting and suturing are commonly simulated procedures2. Most previous studies have focused on either mental workload or physical workload but have seldom performed comparative analyses9–12. Taking into account psychophysiological causes and related literature, the relationship between the two types of workloads should be considered.
Metrics used to assess surgeon workload include subjective measures of workload, physiological indices of workload, objective performance, and other methods including comprehensive evaluations. Scales and questionnaires, such as the NASA Task Load Index scale13 and the Subjective Workload Assessment Technique scale, have become among the most popular tools, especially for surgical procedures14–16. Various physiological indices, such as heart rate, blood pressure, eye movements, EMG, and EEG signals, etc. refs17,18, change corresponding to changes in workload; heart rate is generally used to evaluate body load, and eye movements, and EEG are generally used to assess mental workload. In particular, EEG can characterize the dynamics of functional coupling among different brain areas across surgeons performing laparoscopic tasks with different approaches19. In addition, workload status can be deduced through tasks and the associated performance. These different workload evaluation methods each have their own advantages, and physiological indices of workload are more prominent in accuracy and objectivity.
A previous study presented an interesting finding that the mental workload of bank staff is significantly correlated with musculoskeletal disorders20. The mental workload of nurses is also associated with musculoskeletal disorders21. This previously reported conclusion is based on different types of work and different work contents, and those surveyed enjoyed certain autonomy while working22,23. In contrast, considering a surgeon’s workload, the equipment used, the working time and the processes are severely restricted during an operation. In addition, surgeons must meet high mental and physical demands, have high operation accuracy, and make accurate judgements and decisions. Mental status is associated with muscle activity in some work situations. Schleifer et al.24 discovered that mental stress results in increased EMG activity of the upper limbs during computer work. With the differential changes in heart period and end-tidal carbon dioxide in differential working conditions, mental stress elicits more psychophysiological activation, and less effects are attributed to the biomechanical demands of work. Furthermore, high mental workload tasks predispose individuals to increased psychological and physiological activation. Mental fatigue also influences muscle endurance, recovery and EMG activity25,26.
The interactive effects of mental and physical workload have received growing attention, and negative correlations between mental workload and physical workload have been reported22. In the foregoing cited study, subjective self-report rating assessment tools, the Borg CR10 Scale and NASA-TLX, were adopted to assess physical and mental workloads, respectively. The dual-task methodology consisted of a physical lifting task (no load, 8%,14% and 20% of body mass) and a mental arithmetic task (no load, addition, subtraction, and multiplication) with a total of 15 combinations of conditions. This approach has also been commonly used in other studies23,24,27. Compared with the interactive effects of mental and physical workloads that have been assessed for different types of tasks, laparoscopic surgeries contain both heavier mental and physical loads.
Results
The calculated muscle activity levels are shown in Tables 1, 2 and 3. Descriptive statistics are shown in Table 1, the fixed effects of the characteristics on the results are given in Table 2, and statistics for the various phases are listed in Table 3. The physical workload patterns during the 3 phases were generally similar, with minor differences between the left and right trapezius muscle and bicipital muscle and large differences in the brachioradialis and FCU. The most significant finding was that the activities of the eight muscles in the AC phase (disinterring the bile duct and the cystic artery) and SC phase (sealing and cutting the bile duct and the cystic artery) were quite similar (mean difference = 0.02, p < 0.05) and significantly lower than the muscle activities in the DI phase (detaching the gallbladder from the hepatic bed and inspecting the hepatic bed) (p = 0.01 and 0.03, respectively). Interestingly, the left brachioradialis %MVC was nearly twice that of the right brachioradialis, and the bilateral FCU exhibited the opposite trend, with the exception of during the DI phase.
Table 1.
Description of four upper extremity muscles. The %MVC values for all combinations are presented as the mean (standard deviation).
| Phase | Trapezius | Bicipital | Brachioradialis | FCU | ||||
|---|---|---|---|---|---|---|---|---|
| Left | Right | Left | Right | Left | Right | Left | Right | |
| AC | 0.88 (0.49) | 1.01 (0.8) | 0.84 (0.56) | 0.68 (0.26) | 1.01 (1.4) | 0.45 (0.25) | 0.55 (0.55) | 0.89 (0.86) |
| SC | 0.83 (0.36) | 0.96 (0.78) | 0.94 (0.66) | 0.77 (0.31) | 1.01 (1.3) | 0.45 (0.23) | 0.53 (0.29) | 0.99 (0.78) |
| DI | 1.12 (0.64) | 1.07 (0.78) | 1.1 (0.65) | 0.94 (0.59) | 1.18 (1.26) | 0.53 (0.38) | 0.99 (0.44) | 0.91 (0.6) |
Table 2.
Fixed effects of characteristics based on results of a mixed model.
| Characteristics | Class | Coefficient | S.E. | D.F. | t-value | P |
|---|---|---|---|---|---|---|
| Muscle | Trapezius | −0.08 | 0.19 | 80.2 | −0.43 | 0.67 |
| Bicipital | −0.53 | 0.19 | 80.2 | −2.75 | 0.01 | |
| Brachioradialis | −0.22 | 0.19 | 80.2 | −1.12 | 0.27 | |
| FCU | ref | — | — | — | — | |
| Location | Left | −0.07 | 0.19 | 80.2 | −0.35 | 0.73 |
| Right | ref | |||||
| Phase | AC | −0.19 | 0.07 | 265 | −2.88 | 0.004 |
| SC | −0.17 | 0.07 | 265 | −2.56 | 0.01 | |
| DI | ref | |||||
| Muscle * location | Trapezius * Left | −0.17 | 0.15 | 265 | −1.13 | 0.26 |
| Bicipital * Left | 0.65 | 0.15 | 265 | 4.3 | <0.001 | |
| Brachioradialis * Left | 0.23 | 0.15 | 265 | 1.53 | 0.13 |
Table 3.
Least square means and multiple comparisons of the LC phases in an all-participants mixed effects model.
| Phase | Least square mean | S.E. | P-value | Multiple comparison | |||||
|---|---|---|---|---|---|---|---|---|---|
| Mean difference | Bonferroni adjustment for P-value | ||||||||
| AC | SC | DI | AC | SC | DI | ||||
| AC | 0.79 | 0.08 | <0.001 | — | −0.02 | −0.19 | — | 1.00 | 0.01 |
| SC | 0.81 | 0.08 | <0.001 | — | — | −0.17 | — | — | 0.03 |
| DI | 0.98 | 0.08 | <0.001 | — | — | — | — | — | — |
Figure 1 demonstrates the change in the participants’ pupil diameter during the 3 LC phases. The extent of pupil dilation during the SC phase (mean = 0.12, median = 0.13) and DI phase (mean = 0.13, median = 0.13) was less than that in the DI phase (mean = 0.05, median = 0.04). Moreover, the pupil diameter increased during each individual phase.
Figure 1.
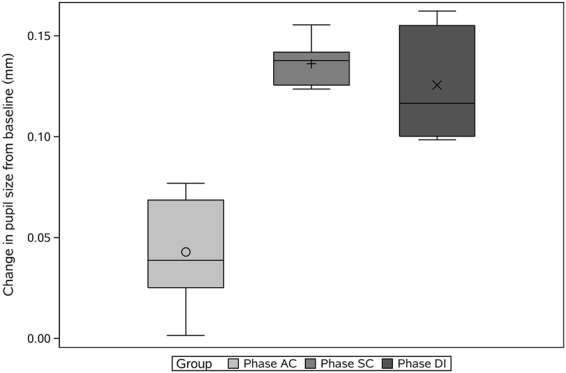
Change in pupil size from baseline during the 3 phases of laparoscopic cholecystectomy surgery.
The results of a correlation analysis between sEMG measurements and eye-tracking is shown in Table 4. We found that the sEMG and eye-tracking measurements during the different phases were uncorrelated. The activities of the left brachioradialis and the left FCU in the SC phase were significantly negatively correlated with mental workload (r = −0.68, p = 0.01 and r = −0.53, p = 0.05).
Table 4.
Correlation analysis between mental and physical workload during the 3 LC phases.
| Muscle | location | AC Phase | SC Phase | DI Phase | |||
|---|---|---|---|---|---|---|---|
| Coefficient | P-value | Coefficient | P-value | Coefficient | P-value | ||
| Trapezius | left | 0.05 | 0.85 | −0.05 | 0.85 | −0.15 | 0.62 |
| right | 0.07 | 0.81 | 0.19 | 0.52 | 0.09 | 0.76 | |
| Bicipital | left | −0.35 | 0.23 | −0.27 | 0.34 | −0.32 | 0.26 |
| right | 0.14 | 0.63 | −0.26 | 0.38 | −0.14 | 0.64 | |
| Brachioradialis | left | −0.33 | 0.25 | −0.68 | 0.01 | −0.37 | 0.19 |
| right | −0.27 | 0.34 | −0.5 | 0.07 | −0.43 | 0.13 | |
| FCU | left | −0.32 | 0.26 | −0.53 | 0.05 | −0.35 | 0.22 |
| right | 0.14 | 0.63 | 0.02 | 0.95 | −0.1 | 0.73 | |
Discussion
Our study is the first to address the significant concern regarding the relationship between the two types of workloads on laparoscopic surgeons. The experimental platform and tasks were carefully considered. An LC surgery was divided into 3 approximately equal phases in terms of the time and process. This partitioning method was effective for our study and is convenient for acquiring and comparing sEMG and eye-tracking signals18.
For evaluating physical workload, similarities in muscle activity among different phases can be determined. This phenomenon can be explained by similar gestures and movements. Notably, we found a difference between the sides of the brachioradialis and the FCU. Fine operations are usually carried out by the dominant hand (i.e., the right hand), and fine movements rely heavily on the wrist and fingers. The left brachioradialis was employed more during usual motions, while the FCU was utilized for finer motions, which reflects muscle movement compensation.
The mean changes in pupil size during the 3 phases are shown in Fig. 1. In this experiment, the pupil was able to characterize mental workload according to expectations. A high mental workload within a short time does not cause mental fatigue and thus does not result in a cumulative effect, which is consistent with the conclusions of other studies28. Other factors influencing pupil size include anxiety, stress, fatigue, and intelligence. In our experimental design, we attempted to eliminate the effects of these factors on pupil size through various methods: allowing the participants to relax, preventing participants from performing tests in a fatigued state, and adjusting lighting brightness of the scene.
Our experimental findings suggest that the mental and physical workloads of the laparoscopic surgeon were non-synchronous and were generally negatively correlated, although insignificant. Mental workload during low-level static work has been verified to adversely affect muscle activity. Laparoscopic surgery involves low-level strength and high-level mental workload. The surgeons’ physical workloads in the AC and SC phases were almost equal and were much lower than the physical workload during the DI phase. In contrast, the surgeons’ mental workload in the AC phase was lower than the mental workload in the SC and DI phase, which corresponded to similar workload levels. The relationship between the workloads can be explained using physiology. Studies of the brain have indicated that mental fatigue and physical fatigue are closely linked. When people are physically fatigued, blood oxygenation in the bilateral prefrontal cortex is reduced, which aggravates mental fatigue29. Muscle activity is directly related to neural activity, as proven by neuroimaging techniques, and the brain possesses a self-adjusting function to maintain physical performance, even when falling into a state of fatigue30–32.
Our experimental results showed that there was no significant negative correlation between the workloads, which is not entirely consistent with previous studies. We attributed this discrepancy to the following reasons: (1) surgical procedures involve both mental and physical workloads, unlike the individual mental and physical tasks employed in previous studies, and the two workloads are not completely independent. Co-existence of the workloads indicates that their relationship is not entirely interactive. (2) We selected a representative group of muscles as research targets but did not include all muscles used during an operation performed by a surgeon, which may result in bias.
Objective evaluations of the workload and ergonomics of laparoscopic surgeons are vital and meaningful. More studies are needed to compensate for the limitations of this study. Physical and mental workload levels are complex and cannot be characterized in a general manner. Multi-means, indices and subjective methods combined with objective techniques will be the most promising approaches going forward33. Workload threshold and ergonomics guidelines should be elaborated to prevent ergonomic problems during laparoscopic surgery.
This experiment was based on a simulation, which holds obvious limitations compared to actual operations. Participants may not be as careful when using a simulator because they may perceive that there will be another chance to repeat the procedure without repercussions. Another limitation of this study was that the LC operation duration was not long enough to induce surgeon fatigue, and therefore, surgeon workloads during a fatigued state could not be evaluated. We plan to study the working status of laparoscopic surgeons and its impact on operation safety and outcomes under different workload conditions in the near future. The concept of a surgeon’s total workload should be established, which would provide a general description of the physician’s fatigue status for quantitative and intuitive monitoring.
Methods
Participants
The procedures of this study were carried out in accordance with approved guidelines. This study was approved by the Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology (IORG No: IORG0003571), and was performed in a simulated operating room with proper lighting conditions and other requirements for an operating environment, according to related standards and manufacturer recommendations. Informed consent was obtained from all participants. In this study, 14 male volunteers were recruited. Four of the participants were laparoscopic surgeons, and the other 10 were predoctoral students. All individuals had laparoscopic surgery experience or training experience and were familiar with the experimental platform prior to the experiment. All participants were right-handed, and they ranged in age from 25 to 35 years (mean age = 28.7, SD = 3.8). The participants’ body mass index (BMI) and elbow height were measured and used as references to adjust the experimental set-up.
Experimental platform and tasks
The experiment was executed in a laparoscopic virtual simulator, which can provide feedback on the operation performance of the participants, including haptic feedback. Statistics of the participants performance on the task were provided when the task was completed.
LC is one of the most common laparoscopic surgeries. LC has been used in many studies as a sample procedure to study the working status of laparoscopic surgeons with respect to OR ergonomics34–36. In previous research, surgical videos, combined with other tools such as rapid upper limb assessment (RULA), have been employed to study physician gestures and stress statics36,37. In contrast to other studies, our study aimed to explore both the physical and mental workloads of laparoscopic surgeons in different LC phases and the correlative relationship between these workloads. All participants were required to complete an LC surgery using the simulator. According to the operation process and the operation simulator’s setting, the LC should be completed via the following five phases: Phase 1: create the pneumoperitoneum and place the trocars; phase 2: based on the anatomy of Calot’s triangle, disinter the bile duct and the cystic artery (AC phase); phase 3: seal and cut the bile duct and the cystic artery (SC phase); phase 4: detach the gallbladder from the hepatic bed and inspect the hepatic bed (DI phase); and phase 5: remove the gallbladder and complete the operation. Phase 1 and phase 5 were executed automatically, and the participants were required to complete the AC, SC and DI phases. We advised the participants to allocate 5 minutes to each of the three phases and to finish the surgery in 15 minutes, if possible. Intervals of approximately 3 minutes were included between the phases to allow the participants’ muscles to relax and to provide feedback.
Workload assessment protocol
Data analysis
An overall 14 × 4 × 2 × 3 (14 participants × 4 muscles × 2 hand sides × 3 phases) analysis of variance was used to analyse the data. A mixed effect model was used for statistical analysis in SAS 9.4, with the significance level set at p = 0.05. Variables with random effects were selected based on the smallest Akaike information criterion (AIC) and the Bayesian information criterion (BIC), with a positive definite G matrix for the intercept, muscles, location and phase.
Eye-tracking data
According to many studies, mental workload can be evaluated by participants’ eye movements, particularly pupil dilatation38–40. The Tobii Glasses 2 Eye Tracker (Tobii Technology, Danderyd, Sweden) was used as an eye-tracking instrument in our study. Before starting the procedure, the participants were equipped with the eye tracker and asked to stare at black dots printed on a paper card for the calibration process. The physiological parameters of the participants’ eyes were recorded during the calibration process.
Laparoscopic surgery requires a high degree of attention, and therefore, eye movement is more able to reflect the physiological state of the surgeon and surgical conditions. Here, pupil size was analysed as the focal index to measure mental workload during operation. In the 1960s, pupil dilation was found to be sensitive to task difficulty and workload41,42. Pupil dilation can be used as a peripheral indicator of brain noradrenergic activity and mental workload in a testing situation. The measurement of pupil diameter has been deemed a promising method for assessing mental workload38,43,44. Task-evoked pupillary responses (TEPRs) have been suggested for exploring the inherent relationship between a task and pupillary dilation44. Generally, larger pupil sizes indicate greater mental workload45–47. In this study, the baseline pupil size (initial diameter) was assessed after the calibration period48. A change in pupil size from baseline, measured as the mean pupil diameter change (MPDC), was observed, consistent with the expected effect.
sEMG data
Physical workload was evaluated by surface myoelectricity, which was captured using a Delsys Trigno Lab sEMG system (Delsys, Inc., Boston, MA) and analysed with standard software. The muscle groups analysed included the bilateral trapezius, biceps, brachioradialis, and FCU. The sEMG sampling frequency was 512 Hz. These data were full-wave rectified and then filtered to obtain a spectrum band ranging from 20 Hz to 250 Hz.
At the beginning of the experimental session, we measured the maximum voluntary contraction (MVC) of each target muscle and normalized the sEMG data to the MVC during data processing49. In this study, we used %MVC, the percentage of MVC, as a measure of muscle workload and characterized the level of muscle contraction per unit time2. For data processing, iEMG was obtained by first integrating the sEMG; the ratio of iEMG to MVC was taken as %MVC2 49.
| 1 |
Conclusions
Observations of surgeons operating during different phases of LC and measurements of their mental and physical workload indicated that the two workloads are non-synchronous, with a general non-significant negative correlation. This study evaluated the workload imposed on surgeons during laparoscopic surgery by physiological (sEMG and eye movement) analysis and objectively demonstrated that while some laparoscopic phases require equal levels of physical work and others do not, significant disparities exist among the mental workloads of those phases. Synthetic and dynamic monitoring of surgeon workload levels is thus highly important in OR ergonomics.
Acknowledgements
No funding bodies played any role in the study design, data collection and analysis, decision to publish, or preparation of this manuscript. The authors would like to thank their colleagues and staff at the Union Hospital of Tongji Medical College, Huazhong University of Science and Technology, China. This study was supported by the National Key Research and Development Program of China (No. 2017YFC0113503) and the National Natural Science Foundation of China (Grant No. 61401242).
Author Contributions
Q.Z. and S.L.L. contributed to the conception and design of the study, and J.Y.Z. wrote the main manuscript text. J.Y.Z. and Q.M.F. reviewed the experiments and analysed the data. J.Y.Z. and J.Q.G. participated in the acquisition of data and statistical analysis. Q.Z., S.L.L. and Q.M.F. reviewed the manuscript.
Competing Interests
The authors declare that they have no competing interests.
Footnotes
A correction to this article is available online at https://doi.org/10.1038/s41598-018-23759-8.
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Wichert A, et al. Improvement of the ergonomic situation in the integrated operating room for laparoscopic operations. Int. Congr. Ser. 2004;1268:842–846. doi: 10.1016/j.ics.2004.03.092. [DOI] [Google Scholar]
- 2.Lee G, Lee T, Dexter D, Klein R, Park A. Methodological infrastructure in surgical ergonomics: a review of tasks, models, and measurement systems. Surg. Innov. 2007;14:153–167. doi: 10.1177/1553350607307956. [DOI] [PubMed] [Google Scholar]
- 3.Szeto GP, et al. Work-related musculoskeletal symptoms in surgeons. J. Occup. Rehabil. 2009;19:175–184. doi: 10.1007/s10926-009-9176-1. [DOI] [PubMed] [Google Scholar]
- 4.Park A. Patients benefit while surgeons suffer: an impending epidemic. J. Am. Coll. Surg. 2010;210:306–313. doi: 10.1016/j.jamcollsurg.2009.10.017. [DOI] [PubMed] [Google Scholar]
- 5.Cass GKS, Vyas S, Akande V. Prolonged laparoscopic surgery is associated with an increased risk of vertebral disc prolapse. J. Obstet. Gynaecol. 2014;34:74–78. doi: 10.3109/01443615.2013.831048. [DOI] [PubMed] [Google Scholar]
- 6.van Wulfften Palthe OD, et al. Among musculoskeletal surgeons, job dissatisfaction is associated with burnout. Clin. Orthop. Relat. Res. 2016;474:1857–1863. doi: 10.1007/s11999-016-4848-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lee GI, et al. Comparative assessment of physical and cognitive ergonomics associated with robotic and traditional laparoscopic surgeries. Surg. Endosc. 2014;28:456–465. doi: 10.1007/s00464-013-3213-z. [DOI] [PubMed] [Google Scholar]
- 8.Zhang A, Hunerbein M, Dai Y, Schlag PM, Beller S. Construct validity testing of a laparoscopic surgery simulator (Lap Mentor): evaluation of surgical skill with a virtual laparoscopic training simulator. Surg. Endosc. 2008;22:1440–1444. doi: 10.1007/s00464-007-9625-x. [DOI] [PubMed] [Google Scholar]
- 9.Zheng B, et al. Quantifying mental workloads of surgeons performing natural orifice transluminal endoscopic surgery (NOTES) procedures. Surg. Endosc. 2012;26:1352–1358. doi: 10.1007/s00464-011-2038-x. [DOI] [PubMed] [Google Scholar]
- 10.Eatough EM, Way JD, Chang CH. Understanding the link between psychosocial work stressors and work-related musculoskeletal complaints. Appl. Ergon. 2012;43:554–563. doi: 10.1016/j.apergo.2011.08.009. [DOI] [PubMed] [Google Scholar]
- 11.Hubert N, et al. Ergonomic assessment of the surgeon’s physical workload during standard and robotic assisted laparoscopic procedures. Int. J. Med. Robot. 2013;9:142–147. doi: 10.1002/rcs.1489. [DOI] [PubMed] [Google Scholar]
- 12.Lee G, Sutton E, Clanton T, Park A. Higher physical workload risks with NOTES versus laparoscopy: a quantitative ergonomic assessment. Surg. Endosc. 2011;25:1585–1593. doi: 10.1007/s00464-010-1443-x. [DOI] [PubMed] [Google Scholar]
- 13.Zheng B, et al. Workload assessment of surgeons: correlation between NASA TLX and blinks. Surg. Endosc. 2012;26:2746–2750. doi: 10.1007/s00464-012-2268-6. [DOI] [PubMed] [Google Scholar]
- 14.Klein M, Andersen LP, Alamili M, Gogenur I, Rosenberg J. Psychological and physical stress in surgeons operating in a standard or modern operating room. Surg. Laparosc. Endosc. Percutan. Tech. 2010;20:237–242. doi: 10.1097/SLE.0b013e3181ed851d. [DOI] [PubMed] [Google Scholar]
- 15.Andersen LP, Klein M, Gogenur I, Rosenberg J. Psychological and physical stress among experienced and inexperienced surgeons during laparoscopic cholecystectomy. Surg. Laparosc. Endosc. Percutan. Tech. 2012;22:73–78. doi: 10.1097/SLE.0b013e3182420acf. [DOI] [PubMed] [Google Scholar]
- 16.Feng QM, Liu SL, Yang L, Xie MX, Zhang Q. The prevalence of and risk factors associated with musculoskeletal disorders among sonographers in central China: a cross-sectional study. PLoS One. 2016;11:e0163903. doi: 10.1371/journal.pone.0163903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Backs RW, Walrath LC. Eye-movement and pupillary response indexes of mental workload during visual-search of symbolic displays. Appl. Ergon. 1992;23:243–254. doi: 10.1016/0003-6870(92)90152-L. [DOI] [PubMed] [Google Scholar]
- 18.Bodala IP, Li J, Thakor NV, Al-Nashash H. EEG and eye tracking demonstrate vigilance enhancement with challenge integration. Front. Hum. Neurosci. 2016;10:273. doi: 10.3389/fnhum.2016.00273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bocci T, et al. How does a surgeon’s brain buzz? An EEG coherence study on the interaction between humans and robot. Behav. Brain Funct. 2013;9:14. doi: 10.1186/1744-9081-9-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Darvishi E, Maleki A, Giahi O, Akbarzadeh A. Subjective mental workload and its correlation with musculoskeletal disorders in bank staff. J. Manip. Physiol. Ther. 2016;39:420–426. doi: 10.1016/j.jmpt.2016.05.003. [DOI] [PubMed] [Google Scholar]
- 21.Yeung SS, Genaidy A, Deddens J, Sauter S. The relationship between protective and risk characteristics of acting and experienced workload, and musculoskeletal disorder cases among nurses. J. Saf. Res. 2005;36:85–95. doi: 10.1016/j.jsr.2004.12.002. [DOI] [PubMed] [Google Scholar]
- 22.DiDomenico A, Nussbaum MA. Interactive effects of physical and mental workload on subjective workload assessment. Int. J. Ind. Ergon. 2008;38:977–983. doi: 10.1016/j.ergon.2008.01.012. [DOI] [Google Scholar]
- 23.Mehta RK, Agnew MJ. Subjective evaluation of physical and mental workload interactions across different muscle groups. J. Occup. Environ. Hyg. 2015;12:62–68. doi: 10.1080/15459624.2014.942455. [DOI] [PubMed] [Google Scholar]
- 24.Schleifer LM, et al. Mental stress and trapezius muscle activation under psychomotor challenge: a focus on EMG gaps during computer work. Psychophysiology. 2008;45:356–365. doi: 10.1111/j.1469-8986.2008.00645.x. [DOI] [PubMed] [Google Scholar]
- 25.Mehta RK, Agnew MJ. Effects of concurrent physical and mental demands for a short duration static task. Int. J. Ind. Ergon. 2011;41:488–493. doi: 10.1016/j.ergon.2011.04.005. [DOI] [Google Scholar]
- 26.Mehta RK, Agnew MJ. Influence of mental workload on muscle endurance, fatigue, and recovery during intermittent static work. Euro. J. Appl. Physiol. 2012;112:2891–2902. doi: 10.1007/s00421-011-2264-x. [DOI] [PubMed] [Google Scholar]
- 27.Mehta RK, Nussbaum MA, Agnew MJ. Muscle- and task-dependent responses to concurrent physical and mental workload during intermittent static work. Ergonomics. 2012;55:1166–1179. doi: 10.1080/00140139.2012.703695. [DOI] [PubMed] [Google Scholar]
- 28.Jansen RJ, Sawyer BD, van Egmond R, de Ridder H, Hancock PA. Hysteresis in mental workload and task performance: the influence of demand transitions and task prioritization. Hum. Factors. 2016;58:1143–1157. doi: 10.1177/0018720816669271. [DOI] [PubMed] [Google Scholar]
- 29.Mehta RK, Parasuraman R. Effects of mental fatigue on the development of physical fatigue: a neuroergonomic approach. Hum. Factors. 2013;56:645–656. doi: 10.1177/0018720813507279. [DOI] [PubMed] [Google Scholar]
- 30.Liu JZ, et al. Shifting of activation center in the brain during muscle fatigue: an explanation of minimal central fatigue? Neuroimage. 2007;35:299–307. doi: 10.1016/j.neuroimage.2006.09.050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Siemionow V, Yue GH, Ranganathan VK, Liu JZ, Sahgal V. Relationship between motor activity-related cortical potential and voluntary muscle activation. Exp. Brain Res. 2000;133:303–311. doi: 10.1007/s002210000382. [DOI] [PubMed] [Google Scholar]
- 32.Tanaka M, Ishii A, Watanabe Y. Physical fatigue increases neural activation during eyes-closed state: a magnetoencephalography study. Behav. Brain Funct. 2015;11:35. doi: 10.1186/s12993-015-0079-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Ishii A, Tanaka M, Watanabe Y. Neural mechanisms to predict subjective level of fatigue in the future: a magnetoencephalography study. Sci. Rep. 2016;6:25097. doi: 10.1038/srep25097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Abbas Z, et al. A comparative clinical evaluation of laparoscopic cholecystectomy with single and multiport access. J. Evol. Med. Dent. Sci. 2015;4:13547–13555. doi: 10.14260/jemds/2015/1938. [DOI] [Google Scholar]
- 35.Dhumane P, et al. Clinical evaluation of an internal adjustable retractor in laparoscopic cholecystectomy. Surg. Innov. 2014;21:234–239. doi: 10.1177/1553350613517945. [DOI] [PubMed] [Google Scholar]
- 36.Silvennoinen M, Antikainen T, Mecklin J-P. Video-assisted surgery: suggestions for failure prevention in laparoscopic cholecystectomy. Cogn. Technol. Work. 2014;17:145–155. doi: 10.1007/s10111-014-0317-8. [DOI] [Google Scholar]
- 37.Vereczkei A, et al. Ergonomic assessment of the static stress confronted by surgeons during laparoscopic cholecystectomy. Surg. Endosc. 2004;18:1118–1122. doi: 10.1007/s00464-003-9157-y. [DOI] [PubMed] [Google Scholar]
- 38.Granholm E, Steinhauer SR. Pupillometric measures of cognitive and emotional processes. Int. J. Psychophysiol. 2004;52:1–6. doi: 10.1016/j.ijpsycho.2003.12.001. [DOI] [PubMed] [Google Scholar]
- 39.Erol Barkana D, Acik A, Duru DG, Duru AD. Improvement of design of a surgical interface using an eye tracking device. Theor. Biol. Med. Model. 2014;11(Suppl 1):S4. doi: 10.1186/1742-4682-11-S1-S4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Smink DS, et al. Utilization of a cognitive task analysis for laparoscopic appendectomy to identify differentiated intraoperative teaching objectives. Am. J. Surg. 2012;203:540–545. doi: 10.1016/j.amjsurg.2011.11.002. [DOI] [PubMed] [Google Scholar]
- 41.Bradshaw JL. Pupil size and problem solving. Quart. J. Exp. Psychol. 1968;20:116–122. doi: 10.1080/14640746808400139. [DOI] [PubMed] [Google Scholar]
- 42.Ahern, S. K. Activation and intelligence: pupillometric correlates of individual differences in cognitive abilities. (ProQuest Information & Learning, 1978).
- 43.Laeng B, Sirois S, Gredeback G. Pupillometry: a window to the preconscious? Perspect. Psychol. Sci. 2012;7:18–27. doi: 10.1177/1745691611427305. [DOI] [PubMed] [Google Scholar]
- 44.Marquart G, de Winter J. Workload assessment for mental arithmetic tasks using the task-evoked pupillary response. Peer J. Comput. Sci. 2015;1:e16. doi: 10.7717/peerj-cs.16. [DOI] [Google Scholar]
- 45.Gable, T. M., Kun, A. L., Walker, B. N. & Winton, R. J. Comparing heart rate and pupil size as objective measures of workload in the driving context. Proceedings of the 7th International Conference on Automotive User Interfaces and Interactive Vehicular Applications (Automotiveui ‘15), doi:10.1145/2809730.2809745, 20–25 (2015).
- 46.Reiner M, Gelfeld TM. Estimating mental workload through event-related fluctuations of pupil area during a task in a virtual world. Int. J. Psychophysiol. 2014;93:38–44. doi: 10.1016/j.ijpsycho.2013.11.002. [DOI] [PubMed] [Google Scholar]
- 47.Liu, Z., Xing, B., Zhou, Q. & Zhang, X. The experiment research of pupil change for the evaluation of mental workload in HCI International 2016 - posters’ extended abstracts, pt. I (ed. Stephanidis, C.) 220–225 (2016).
- 48.Klingner, J. Measuring cognitive load during visual tasks by combining pupillometry and eye tracking. (Stanford University, 2010).
- 49.Zihni AM, Ohu I, Cavallo JA, Cho S, Awad MM. Ergonomic analysis of robot-assisted and traditional laparoscopic procedures. Surg. Endosc. 2014;28:3379–3384. doi: 10.1007/s00464-014-3604-9. [DOI] [PubMed] [Google Scholar]