

Abstract
Objective:
In permanent dentition, different rotary systems are used for canal cleaning and shaping. Rotary instrumentation in pediatric dentistry is an emerging concept. A very few studies have compared the efficiency of rotary instrumentation for canal preparation in primary teeth. Hence, this study was performed to compare the obturation quality and instrumentation time of two rotary files systems – Protaper, Mtwo with hand files in primary molars.
Materials and Methods:
Forty-five primary mandibular molars were randomly allotted to one of the three groups. Instrumentation was done using K-files in Group 1; Protaper in Group 2; and Mtwo in Group 3. Instrumentation time was recorded. The canal filling quality was assessed as underfill, optimal fill, and overfill. Statistical analysis was done using Chi-square, ANOVA, and post hoc Tukey test.
Results:
No significant difference was observed in the quality of obturation among three groups. Intergroup comparison of the instrumentation time showed a statistically significant difference between the three groups.
Conclusion:
The use of rotary instrumentation in primary teeth results in marked reduction in the instrumentation time and improves the quality of obturation.
Keywords: Primary teeth, pulpectomy, randomized controlled trial, rotary instrumentation
INTRODUCTION
Pulpectomy is the choice of treating symptomatic decayed primary teeth and is a challenging and time-consuming procedure in pediatric dentistry.[1] An efficient chemomechanical preparation is essential for effective canal disinfection and thereby contributes to the success of the endodontic procedure.[2] Conventionally, hand files are used for cleaning and shaping and are time-consuming.[3] The length of the appointment is strongly associated with the child's behavior.[4] Removal of organic debris is the primary goal of canal preparation in primary teeth.[5] Use of rotary instrumentation for pulpectomy is an emerging practice in pediatric dentistry. The canals of the permanent teeth are prepared rapidly and uniformly with NiTi files resulting in superior obturation.[6,7] Rotary instrumentation in primary teeth was advocated for its ability to provide conical-shaped canals and reduced the instrumentation time.[3,8,9,10,11]
An in vitro study comparing the canal cleaning capacity of hand files, Mtwo and ProTaper showed no significant differences.[5] Another in vitro study compared the cleaning capacity and instrumentation time of K-files and Mtwo and concluded that there was no significant difference in cleaning capacity, but reduced instrumentation time with the use of Mtwo rotary system was evident.[12] There are no in vivo studies in the literature comparing the manual instrumentation with Mtwo rotary system for pulpectomy in primary teeth.
Hence, the aim of this study was to comparatively evaluate the quality of obturation and instrumentation time using hand files, Protaper, and Mtwo rotary systems in primary molars.
MATERIALS AND METHODS
The randomized controlled trial was carried out in the Department of Pediatric and Preventive Dentistry in a Dental College from July to November 2016. The trial design was approved by the Institutional Review Board (STP/SDMDS2015PED42). The informed consent was obtained from the parents of the children participated in the study.
A total of 45 children aged 4–8 years requiring pulpectomy in any one of the primary mandibular molars were randomly allotted to one of the three groups where instrumentation was done using: Group 1: manual K-files; Group 2: proTaper rotary system; Group 3: Mtwo rotary system. Computer-generated randomization sequence was generated by a person, not involved in the study. The sample size was calculated from a previous in vivo study with 95% power using G Power analysis.[13] The selection of the children was based on the following criteria: (a) vital or nonvital mandibular primary molars without sinus tract, (b) absence of internal or external pathologic root resorption, (c) presence of adequate coronal tooth structure to receive SS crown. The children lacking cooperative ability, children with underlying systemic diseases, and children with special health-care needs were excluded from the study.
All the procedures were done by a single operator. A full mouth examination with intraoral periapical radiographs of the teeth indicated for pulpectomy was taken before the start of the clinical procedure. After confirmation of the diagnosis, local anesthesia was administrated using 2% lignocaine with 1:200,000 adrenaline (LOX* 2% ADRENALINE, Neon Laboratories limited, India). The tooth was isolated using rubber dam (GDC Marketing, India).
Using a round carbide bur in a high-speed handpiece, the superficial caries and roof of the pulp chamber were removed. Coronal pulp amputation was done with spoon excavator. No. 10 size K-file was used to determine the patency of the canals. The working length was determined with radiograph and was kept 1 mm short of the apex. The canal preparation was done using:
Group 1: K-files from size 15 to size 30 in quarter pull turn method.
Group 2: Only S2 ProTaper file was used till the working length using an X-Smart motor.(Dentsply India Pvt. Ltd., Delhi, India)
Group 3: Only Mtwo file of 0.04 taper and 0.25 tip with X-Smart motor till the full working length (Dentsply India Pvt. Ltd., Delhi, India).
During the canal preparation, the instrumentation time was recorded in seconds using a stopwatch by an assistant. The canals were then irrigated with saline and dried using sterile paper points. The obturation was done using calcium hydroxide and iodoform paste by gently pushing with cotton pellets (Metapex, Meta Biomed Co., Ltd., Korea). A postobturation radiograph was taken to assess the quality of obturation. It assessed by another pediatric dentist who was blinded to the type of instrumentation used for canal preparation. The obturation quality was graded as underfill, optimal fill, overfill.
The glass ionomer cement (Shofu, Shofuinc. Japan) was given as the entrance filling. The pulpectomy treated teeth were restored with SS crowns either on the same day or in the next appointment.
The statistical analysis was done using SPSS software version 17.0. (Chicago, SPSS Inc). Chi-square test was used for inter- and intra-group analysis of quality of obturation. ANOVA and post hoc Tukey test were used for the compare the instrumentation time.
RESULTS
A total of 23 girls and 22 boys were participated in the study. The distribution of the participants is tabulated [Table 1]. Of 45 treated primary mandibular molars, 24.4% and 17.8% were mandibular left primary second and first molars, respectively. Mandibular right first and second molars comprised 28.9% each.
Table 1.
Distribution of the participants
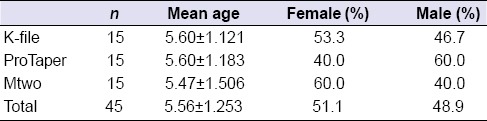
An intergroup comparison was done with respect to the age, gender, and distribution of the teeth using ANOVA and Chi-square test. No statistically significant difference was noted between the groups with respect to the age (P = 0.947), gender (P = 0.537), and distribution of teeth (P = 0.704) indicating that there was an equal distribution of the participants and the teeth between all the three groups.
With respect to quality of obturation among the groups, in Group 1 (K-files): 60% of the mesial canals were optimally filled; 13.3% and 26.7% were under- and over-filled, respectively. In the distal canals, 40% were optimally filled, 26.7% were underfilled, and 33.3% were overfilled.
In Group 2 (Protaper): 73.3% of the mesial canals were optimally filled; 13.3% were under- and over-filled each. 60% of the distal canals were optimally filled; 20% were under- and over-filled each.
In Group 3 (Mtwo): 60% of the mesial canals were optimally filled; 33.3% were under-filled and 6.7% was over-filled. In the distal canals, 53.3% were optimally filled; 26.7% were underfilled, and 20% were overfilled.
Inter- and intra-group comparison of quality of obturation was done using Chi-square test. No statistically significant difference was observed in mesial (P = 0.370) and distal canals (P = 0. 823) between the three groups [Table 2]. Between the mesial and distal canals, there was no significant difference in the teeth instrumented with K-file (P = 0.218). A significant difference was noticed between the mesial and the distal canals of the teeth instrumented with ProTaper (P = 0.036) and Mtwo (P = 0.002). The quality of obturation was superior in mesial canals than the distal canals [Table 3].
Table 2.
Intergroup analysis of quality of obturation
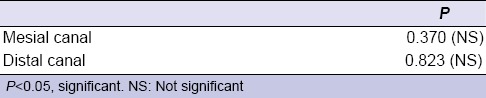
Table 3.
Intragroup analysis of the quality of obturation between mesial and distal canals

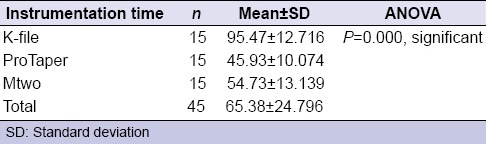
The mean instrumentation time is depicted in Table 4. Intergroup comparison was done using ANOVA and a statistically significant difference was noted between the three groups (P = 0.000) [Table 4].
Table 4.
Instrumentation time of the three groups
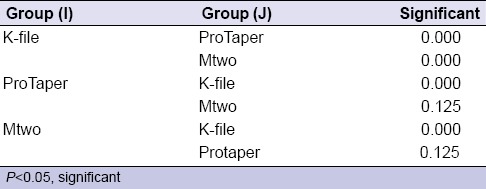
Post hoc Tukey analysis confirmed that there was a significant reduced instrumentation time between the rotary and manual instrumentation [Table 5].
Table 5.
Post hoc test
DISCUSSION
Early loss of primary molars is a serious issue of concern in pediatric dentistry. Pulpectomy should be the treatment option to maintain the integrity of facial tissue. Cleaning and shaping of the root canal is an important step in pulpectomy. The success of an endodontic procedure depends on the proper mechanical debridement and obturation quality.[14] There are many in vitro studies done in primary teeth comparing different rotary instrumentation systems with manual instrumentation.[3,9,10,11] As there are no in vivo study done comparing manual files with ProTaper and Mtwo, this randomized, controlled, single-blinded trial was conducted to evaluate the quality of obturation and instrumentation time using K-file, ProTaper, and Mtwo.
ProTaper files are triangular in cross-section while the Mtwo files have S-shaped cross section. These files get engaged into the walls of the canals, producing smooth and tapered canal walls.[15,16] Nagaratna et al. reported that the increased risk of instrument fracture with rotary instruments is a potential limitation for its use in primary teeth.[17] This is due to the softer and less denser root dentin, thinner and more curved roots with undetectable root tip resorption, and ribbon-shaped root morphology of the primary teeth.[18] There are no clear guidelines for the sequence of using rotary files in primary teeth. Hence, a modified sequence of using only S2 file in ProTaper system and 0.04% taper with 0.25 tip of Mtwo rotary file was selected in this current study. This modified sequence combined with its use in a torque-limited handpiece resulted in no instrument separation within the canals.
With regard to the quality of obturation, there was no statistically significant difference between the groups in both mesial and distal canals. In the study done by Abbas Makarem in 2014 and Tania Ochoa–Romero in 2011, a statistically significant difference was noted in the quality of obturation.[19,20]
Intragroup comparison showed superior obturation of the mesial canals in both rotary groups. The distal canals instrumented with rotary files were over obturated in majority of the cases. This could be due to the anatomy of the root canals. Distal canals are usually straight and wide while the mesial canals are curved and slender.
In the current study, a significant difference in the instrumentation time was noted between the three groups. The reduced instrumentation time was also evident in other studies done with different rotary systems.[13,19] This decrease in the instrumentation time could positively influence the behavior of the child in the dental chair.
Inclusion of only the mandibular molars is considered as the potential confounder in the current study.
CONCLUSION
With the use of rotary instruments for pulpectomy in primary teeth, marked reduction in the instrumentation time has been appreciated resulting in decreased chair side time thereby positively influencing the child's behavior.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Bowen JL, Mathu-Muju KR, Nash DA, Chance KB, Bush HM, Li HF. Pediatric and general dentists’ attitudes toward pulp therapy for primary teeth. Pediatr Dent. 2012;34:210–5. [PubMed] [Google Scholar]
- 2.Endo MS, Ferraz CC, Zaia AA, Almeida JF, Gomes BP. Quantitative and qualitative analysis of micro- organisms in root filled teeth with persistent infection: Monitoring of endodontic retreatment. Eur J Dent. 2013;7:302–9. doi: 10.4103/1305-7456.115414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Silva LA, Leonardo MR, Nelson-Filho P, Tanomaru JM. Comparison of rotary and manual instrumentation techniques on cleaning capacity and instrumentation time in deciduous molars. J Dent Child (Chic) 2004;71:45–7. [PubMed] [Google Scholar]
- 4.Rosa FM, Modesto A, Faraco-Junior IM. Manual and rotary instrumentation techniques for root canal preparation in primary molar. Dentistry. 2014;2:1–5. [Google Scholar]
- 5.Azar MR, Safi L, Nikaein A. Comparison of the cleaning capacity of Mtwo and Pro Taper rotary systems and manual instruments in primary teeth. Dent Res J (Isfahan) 2012;9:146–51. doi: 10.4103/1735-3327.95227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Deplazes P, Peters O, Barbakow F. Comparing apical preparations of root canals shaped by nickel-titanium rotary instruments and nickel-titanium hand instruments. J Endod. 2001;27:196–202. doi: 10.1097/00004770-200103000-00015. [DOI] [PubMed] [Google Scholar]
- 7.Barbizam JV, Fariniuk LF, Marchesan MA, Pecora JD, Sousa-Neto MD. Effectiveness of manual and rotary instrumentation techniques for cleaning flattened root canals. J Endod. 2002;28:365–6. doi: 10.1097/00004770-200205000-00004. [DOI] [PubMed] [Google Scholar]
- 8.Pinheiro SL, Araujo G, Bincelli I, Cunha R, Bueno C. Evaluation of cleaning capacity and instrumentation time of manual, hybrid and rotary instrumentation techniques in primary molars. Int Endod J. 2012;45:379–85. doi: 10.1111/j.1365-2591.2011.01987.x. [DOI] [PubMed] [Google Scholar]
- 9.Barr ES, Kleier DJ, Barr NV. Use of nickel-titanium rotary files for root canal preparation in primary teeth. Pediatr Dent. 2000;22:77–8. [PubMed] [Google Scholar]
- 10.Crespo S, Cortes O, Garcia C, Perez L. Comparison between rotary and manual instrumentation in primary teeth. J Clin Pediatr Dent. 2008;32:295–8. doi: 10.17796/jcpd.32.4.l57l36355u606576. [DOI] [PubMed] [Google Scholar]
- 11.Kuo C, Wang Y, Chang H, Huang G, Lin C, Li U, et al. Application of Ni-Ti rotary files for pulpectomy in primary molars. J Dent Sci. 2006;1:10–5. [Google Scholar]
- 12.Ramezanali F, Afkhami F, Soleimani A, Kharrazifard MJ, Rafiee F. Comparison of cleaning efficacy and instrumentation time in primary molars: Mtwo rotary instruments vs. hand K- files. Iran Endod J. 2015;10:240–3. doi: 10.7508/iej.2015.04.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Vieyra JP, Enriquez FJ. Instrumentation time efficiency of rotary and hand instrumentation performed on vital and necrotic human primary teeth: A Randomized Clinical Trial. Dentistry. 2014;4:1–5. [Google Scholar]
- 14.Tabassum S, Khan FR. Failure of endodontic treatment: The usual suspects. Eur J Dent. 2016;10:144–7. doi: 10.4103/1305-7456.175682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Foschi F, Nucci C, Montebugnoli L, Marchionni S, Breschi L, Malagnino VA, et al. SEM evaluation of canal wall dentine following use of Mtwo and ProTaper NiTi rotary instruments. Int Endod J. 2004;37:832–9. doi: 10.1111/j.1365-2591.2004.00887.x. [DOI] [PubMed] [Google Scholar]
- 16.Malagino VA, Grande NM, Plotino G, Somma F. The MtwoNiTi Rotary System for Root Canal Preparation. [Cited on 2012 Apr 04]. Available from: http://www.vdw-dental.com/pdf/presse/RO0306_59-62_Malagino.pdf .
- 17.Nagaratna PJ, Shashikiran ND, Subbareddy VV. In vitro comparison of NiTi rotary instruments and stainless steel hand instruments in root canal preparations of primary and permanent molar. J Indian Soc Pedod Prev Dent. 2006;24:186–91. doi: 10.4103/0970-4388.28075. [DOI] [PubMed] [Google Scholar]
- 18.Finn SB, editor. Clinical Pedodontics. 4th ed. Philadelphia: Saunders Co; 1973. Morphology of primary teeth; pp. 59–70. [Google Scholar]
- 19.Makarem A, Ravandeh N, Ebrahimi M. Radiographic assessment and chair time of rotary instruments in the pulpectomy of primary second molar teeth: A randomized controlled clinical trial. J Dent Res Dent Clin Dent Prospects. 2014;8:84–9. doi: 10.5681/joddd.2014.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ochoa-Romero T, Mendez-Gonzalez V, Flores-Reyes H, Pozos-Guillen AJ. Comparison between rotary and manual techniques on duration of instrumentation and obturation times in primary teeth. J Clin Pediatr Dent. 2011;35:359–63. doi: 10.17796/jcpd.35.4.8k013k21t39245n8. [DOI] [PubMed] [Google Scholar]