

Dear Editor,
Superficial acral fibromyxoma (SAF) is a rare slow-growing mesenchymal tumor that is commonly located in the periungual and subungual regions of the fingers and toes.1 We report the case of a 71-year-old man, who has been progressing for a year with an asymptomatic lesion in the left hallux, with progressive enlargement. At dermatological examination, there was a smooth and well-delimited surface tumor, fibroelastic consistency, painless to palpation, measuring approximately 3cm, located in the left hallux (Figure 1).
Figure 1.

Smooth, well delimited surface tumor of fibroelastic consistency, painless to palpation, measuring approximately 3cm, located in the left hallux
In view of the clinical picture, the diagnostic hypotheses of eccrine poroma or onychoblastoma were made. Complete surgical excision of the lesion was performed (Figure 2), with a later histopathological study, which demonstrated a well delimited fibromyxoid neoplasm covered by acanthotic epidermis and hyperkeratosis, showing in the dermis elongated, spindle-shaped neoplastic cells without atypia, with a richly vascularized myxoid stroma, consistent with the diagnosis of superficial acral fibromyxoma. An immunohistochemical study with positivity for CD34 and negativity for the markers S100, Desmina, CK 40 and 48, smooth muscle actin and mucin were also performed (Figure 3). Patient remained in periodic follow-up, without recurrence of the lesion after six months of postoperative period. SAF is a rare mesenchymal neoplasm that typically occurs in the digits of middle-aged adult men, more frequent in the chirodactyls, initially described by Fetsch et al. in 2001. It is a tumor characterized clinically by a solitary nodule, sometimes lobulated, of benign behavior, but which can persist or recur if it is excised in an inadequate manner, being recommended the complete excision of the lesion and postoperative follow-up.2,3 Nail bed is involved in 50% of the cases, and can rarely have a history of trauma preceding the onset of the lesion. Less frequent locations have already been described as palmar, calcaneal, ankle and thigh regions. Histopathological study reveals a moderately circumscribed unencapsulated tumor located in the dermis and extending to the subcutaneous tissue. There is proliferation of fibrobasto-like spindle cells embedded in myxoid collagen stroma.
Figure 2.

Surgical removal of the lesion
Figure 3.
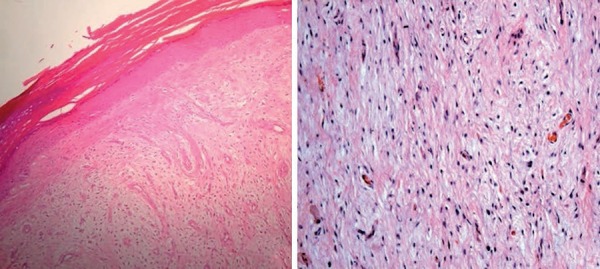
In hematoxylin-eosin staining, a well-delimited fibromyxoid neoplasia covered by acanthotic epidermis and hyperkeratosis was observed. In the dermis, elongated, spindle-shaped neoplastic cells were present, with no atypia with a richly vascularized myxoid stroma. Immunohistochemical study revealed positivity for CD34 (Hematoxylin & eosin X100)
Tumor cells demonstrate immunoreactivity for CD34, CD99, vimetin, and the results of the epithelial membrane antigen are still inconsistent.4 Radiological studies may reveal underlying bone erosions and fine needle cytology shows a cluster of loose spindle cells in the myxoid material. Malignant transformation, although rare, is possible.3,4 Differential diagnosis of SAF should be made with nail/ periungual fibroma, acquired digital fibrokeratoma, low-grade fibromyxoid sarcoma, dermatofibroma, superficial angiomyxoma, and myxoid neurofibroma. Treatment of choice is extensive surgical resection and periodic follow-up after excision is advisable, as recurrence rate may range from 10% to 24%. This recurrence has been associated with incomplete resection.2 Mohs surgery has become a promising alternative due to greater control of the margins, reducing the possibility of recurrence and satisfactorily preserving tissues adjacent to the tumor.5 SAF, although rare, should be included in the differential diagnosis of tumors involving chirodactyls and toes.
Footnotes
Conflict of interests: None.
Study conducted at Alfredo da Matta Foundation (FUAM) - Manaus (AM), Brasil.
Financial support: None.
REFERENCES
- 1.Fetsch JF, Laskin WB, Miettinen M. Superficial acral fibromyxoma: a clinicopathologic and immunohistochemical analysis of 37 cases of a distinctive soft tissue tumor with a predilection for the fingers and toes. Hum Pathol. 2001;32:704–714. doi: 10.1053/hupa.2001.25903. [DOI] [PubMed] [Google Scholar]
- 2.Hollmann TJ, Bovée JV, Fletcher CD. Digital fibromyxoma (superficial acral fibromyxoma): a detailed characterization of 124 cases. Am J Surg Pathol. 2012;36:789–798. doi: 10.1097/PAS.0b013e31824a0b83. [DOI] [PubMed] [Google Scholar]
- 3.Messeguer F, Nagore E, Agustí-Mejias A, Traves V. Superficial acral fibromyxoma: a CD34+ periungual tumor. Actas Dermosifiliogr. Actas Dermosifiliogr. 2012;103:67–69. doi: 10.1016/j.adengl.2011.03.018. [DOI] [PubMed] [Google Scholar]
- 4.Ramya C, Nayak C, Tambe S. Superficial Acral Fibromyxoma. Indian J Dermatol. 2016;61:457–459. doi: 10.4103/0019-5154.185734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hankinson A, Holmes T, Pierson J. Superficial Acral Fibromyxoma (Digital Fibromyxoma): A Novel Treatment Approach Using Mohs Micrographic Surgery for a Recurrence-Prone Digital Tumor. Dermatol Surg. 2016;42:897–899. doi: 10.1097/DSS.0000000000000735. [DOI] [PubMed] [Google Scholar]