

Abstract
Background:
Poor adherence to antidiabetic medications leads to a higher rate of hospital admissions and adverse health outcomes in type 2 diabetes mellitus patients.
Objective:
This study aims to evaluate whether a pharmacist-led medication therapy management, compared to the usual care, could enhance medication adherence and reduce hospital admission in patients with type 2 diabetes mellitus.
Methods:
A prospective randomized controlled study was conducted in patients with type 2 diabetes mellitus from February 1 to July 30, 2016. Patients in the control group (n=65) received the usual care while patients in the intervention group (n=62) received a personalized pharmacotherapeutic care plan and diabetes education. The two groups were compared by repeated measure ANOVA at 3 and 6-months with medication adherence (using Morisky medication adherence scale) and number of hospital admissions as the main outcome variables.
Results:
A total of 127 patients were included in the study. A marked and statistically significant increase in medication adherence from baseline to 3 and 6 months were noted in the intervention group (increased from 9.2% at baseline to 61% at 6 month) compared with the control group (increased from 13.2% at baseline (to 30.2% at 6 month; p-value<0.01). Furthermore, at the 6-month follow-up, only 23 patients in MTM group with poorly controlled blood glucose levels resulted in hospital admissions compared to 48 patients in non-MTM group, resulting in a 52.1% fewer hospital admissions (p< 0.001).
Conclusions:
The findings of this study implied that pharmacist-led medication therapy management might improve medication adherence and reduce number of hospitalizations in patients with type 2 diabetes mellitus. Hence, policies and guidelines should be in place in order for clinical pharmacists to fully engage in patient care and improve the medication therapy outcomes.
Keywords: Diabetes Mellitus, Type 2, Medication Therapy Management, Medication Adherence, Pharmacists, Treatment Outcome, Patient Education as Topic, Ethiopia
INTRODUCTION
Diabetes mellitus is a chronic devastating disease that, despite recent advances in medical care and management, still precipitates substantial morbidity and long-term complications.1 It is a growing chronic disease with a global prevalence of 415 million, and this figure is expected to be more than 642 million by the year 2040.2 In Ethiopia, the number of patients living with diabetes is increasing in alarming rate with a national prevalence close to 6.5%.3 The high prevalence and the chronic nature of the disease necessitate the need for diabetes disease state management. Many approaches are known to improve diabetes disease control including effective screening, management, regular monitoring and consistent follow up.4 Medication adherence, lifestyle modifications and regular monitoring of blood glucose are some of the factors which contribute to better health outcomes and can be significantly affected by health education and counseling.5,6
It has been known, in the past decades, that medication therapy management is associated with reduced mortality, morbidity and increased health related quality of life.7 Yet, there has been an increase in irrational use of medicines with more than half of medicines prescribed and/or dispensed inappropriately. In addition, more than half of patients fail to adhere to their prescribed medicines.8 Consequently, the healthcare system suffers from a number of health and economic losses.9 In recognition to this problem, there has been a rising interest in interdisciplinary healthcare approach involving all specialties of healthcare providers as an effective way of improving medication adherence and overall health outcomes.10 The role of pharmacists is expanding globally from merely dispensing medications to involvement in different patient care services and disease state management.11,12,13,14 Medication therapy management (MTM), one of the well-established roles of pharmacists, could be used as one of the effective approaches to improve adherence to anti-diabeic medications and health outcomes.7,15 Furthermore, clinical pharmacists, with their pharmacotherapeutic knowledge and patient centered training, are uniquely positioned to educate, elaborate, implement and monitor patients on medication therapies, which ultimately results in better health outcomes.7,16,17,18
Cognizant of the global paradigm shift in pharmaceutical education and practice, Public universities in Ethiopian revised their undergraduate pharmacy curriculum in 2008 to be more patient focused and a limited number of pharmacy schools also started a postgraduate course in clinical pharmacy. Even though there has been an increase in pharmacists’ involvement in patient care in Ethiopia, their full potential and role in clinical practice is yet to be explored.19,20 The present study has been conducted with the objective of evaluating the effectiveness of pharmacists-led MTM service on adherence and hospital admission among patients with type 2 diabetes mellitus who visited the diabetes illness follow-up care clinic of University of Gondar Referral and Teaching Hospital (UoGRTH), Ethiopia.
METHODS
Study design
A single-center, prospective randomized controlled study was conducted to assess the effectiveness of pharmacist-led MTM on improving medication adherence and hospital admission in patients with type 2 diabetes mellitus who visited the diabetes illness follow-up care clinic of UoGRTH from February 1 to July 30, 2016. UoGRTH is located in Gondar town, northwest Ethiopia. It is the only referral center in the area with multiple specialized clinics including pediatrics, surgery, gynecology, psychiatry, HIV care, oncology, outpatient clinics, and a diabetes illness follow-up care clinic, which currently provides service for more than 10, 000 diabetic patients on outpatient level annually. Furthermore, the hospital also offers clinical pharmacy services in various clinical sites including ambulatory care, psychiatry, internal medicine and the drug information center.
After receiving the usual care (defined in “intervention and control” section) by the attending physician, all eligible and consenting patients were provided with an interviewer administered questionnaire so as to complete questions on the socio-demographic and baseline clinical characteristics. Patients were then allocated randomly to either intervention group or control group. Patients assigned to the intervention group received, besides the usual care, MTM services from one clinical pharmacist. This study was approved by the ethical review committee of School of pharmacy, University of Gondar with a reference number of UoG-SoP/0319/2016. Written informed consent from all participants were also gained before commencing the study and patients’ information obtained was kept confidential.
Patient selection
Patients who were at least 18 years of age, with a diagnosis of type 2 diabetes; taking at least one long-term antidiabetic medication for a at least 3 months and having regular visits (every month) to the hospital for follow-up and medication refill were included while patients having medical conditions rendering them mentally incapable to participate (such as uncontrolled psychiatric illness, and loss of consciousness due to acute complications) and patients who were unable to communicate and understand Amharic language were excluded from the study.
Control and intervention
Patients assigned to the control group received the usual care provided in the diabetes clinic. It is a short (3–4 minutes) discussion with the attending physician regarding their diagnosis and the importance of medication adherence for the control of blood sugar level with subsequent appointments. Patients allocated in the intervention group received the usual care followed by MTM, a group of analytical, educational, and monitoring services to optimize therapeutic outcomes15, by the pharmacist immediately after physician consultation. More specifically, the clinical pharmacist utilized a personalized approach and tailored to the specific needs of each patient. The intervention (MTM) took an average time of 45 minutes. The clinical pharmacist reviewed the patient’s medication regimen, provided customized education and training on the proper methods to take their medications including dosage, frequency and special precautions as well as education on health-promoting behaviors such as the role of balanced diet, regular exercise, smoking cessation. The pharmacist also tried to address patients’ concern towards medications use and provided charge-free telephone counselling throughout the study period. The aim of the telephone conversation was to prevent the occurrence of lost to follow up that could reduce the number of patients the will stick to the in person scheduled visit. Study participants were well informed that they can contact anytime if they need any advice regarding their medications and once a phone call received it would then be recorded so as to know any change and anticipate any challenge in the implementation of the study. Finally, all patients were asked to teach back the information to confirm understanding. Two consecutive follow-up visits were scheduled for 3 months and 6 months for each patient. To avoid inter-pharmacist variability, a single clinical pharmacist conducted the baseline and subsequent interventional sessions.
Outcome Measures
The primary outcome measures included the change of the medication adherence from baseline to 3 months and 6 months for the control and intervention groups. Number of all hospital admissions were also recorded during the study period and compared between the two groups. Morisky Medication Adherence Scale (MMAS-8) was utilized for assessing self-reported medication adherence owing to its simplicity, ease of administration and low cost. MMAS-8 is an eight-item adherence measurement tool which has been proven to be reliable for assessment of medication adherence in different patient populations including diabetes mellitus and have a good concurrent and predictive validity.21,22,23,24 MMAS-8 scores can range from zero to eight in integers. Using 6 as a cut-off point, its sensitivity of identifying patients with poor or good adherence was estimated to be 93%.22
Statistical analysis
The data collected were entered into and analyzed using Statistical Package for the Social Sciences (SPSS) software version 21.0 for Windows (SPSS Inc., Chicago, IL). Data were presented as mean (SD) or as percentages within groups. Pearson’s chi-square and student’s sample t-test was employed to compare baseline characteristics of the two groups. Mann–Whitney U-tests were used for non-parametric variables and the differences in the change of Morisky scores among the two groups were analyzed using a repeated-measures ANOVA along with corresponding p-value (p<0.05) as cut off points for determining statistical significance.
RESULTS
Out of 172 eligible patients recruited, 127 of them agreed to participate and 45 excluded (29 declined to participate after a detailed description of the study protocol, 9 patients excluded due to uncontrolled psychiatric disease that hindered them from fully participating in the study and the rest 7 had not been contacted). The detailed flow of patients through the study period is presented in Figure 1.
Figure 1. Flow of participants through the study.
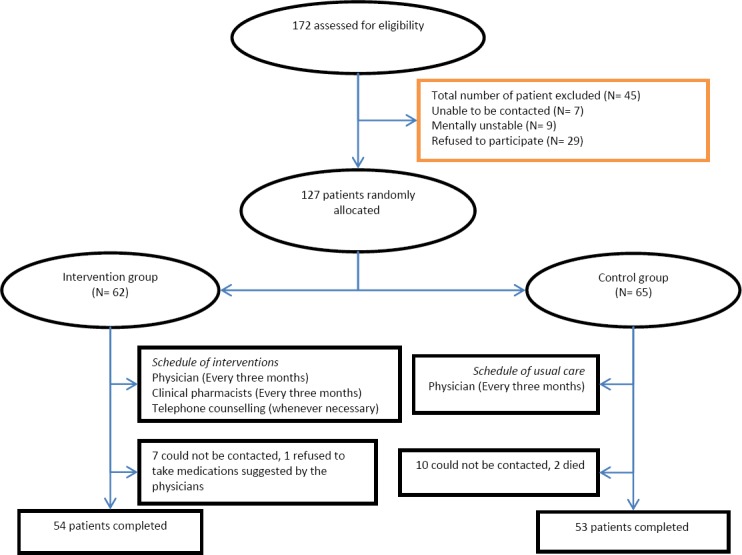
A total of 127 eligible participants were randomly assigned into one of the two groups, with 62 patients allocated to the pharmacist-led MTM group and 65 to the non-MTM (control) group. Majority of patients in our study used metformin with glibenclamide (glyburide) (49.5%) followed by metformin only (40.2%). There were no statistically significant differences between the two groups in demographic and clinical parameters including mean age, gender, and other functional variables (Table 1).
Table 1. Patients demographics and clinical characteristics at baseline.
| Variable | Frequency | p-value | |
|---|---|---|---|
| MTM group (n=54) | Non-MTM group (n=53) | ||
| Age, mean (SD), years | 61.3 (11.4) | 59.8 (13.5) | 0.121 |
| Gender | 0.091 | ||
| Male | 30 (55.5%) | 31 (58.5%) | |
| Female | 24 (44.5%) | 22 (41.5%) | |
| Mean body mass index, kg/m2(SD) | 24.2 (1.8) | 25.3 (2.1) | 0.752 |
| Duration of diabetes (years, SD) | 6.4 (1.9) | 6.2 (2.1) | 0.273 |
| Residence | |||
| Urban | 28 (51.8%) | 26 (49.1%) | |
| Rural | 26 (48.2%) | 27 (50.9%) | |
| Employment status | 0.483 | ||
| Unemployed | 34 (62.9%) | 31 (58.5%) | |
| Employed | 20 (37.1%) | 22(41.5%) | |
| Educational status | 0.064 | ||
| Illiterate (unable to read and write) | 23 (42.6%) | 19 (35.8%) | |
| Primary school | 9 (16.7%) | 13 (24.5%) | |
| Secondary school | 12 (22.2%) | 10 (18.9%) | |
| Collage/university | 8 (14.8%) | 11 (20.8%) | |
| Average monthly income (in USD) | 0.321 | ||
| <75 | 29 (53.7%) | 32 (60.4%) | |
| 75-150 | 18 (33.3%) | 15 (28.3%) | |
| >150 | 7 (13%) | 6 (11.3%) | |
| Antidiabetic medications used | 0.581 | ||
| Metformin | 22 (40.8%) | 21 (39.7%) | |
| Metformin with glibenclamide (glyburide) | 26 (48.1%) | 27 (50.9%) | |
| Insulin | 6 (11.1%) | 5 (9.4%) | |
| Diabetic complications | 0.762 | ||
| Retinopathy | 14 (25.9%) | 11 (20.6%) | |
| Neuropathy | 13 (24.1%) | 15 (28.3%) | |
| Nephropathy | 15 (27.8%) | 10 (18.9%) | |
| Cardiovascular disease | 23 (42.6%) | 27 (50.9%) | |
Abbreviations: MTM: medication therapy management; Non-MTM: Non-medication therapy management
A marked and statistically significant increase in medication adherence from baseline to 3 and 6 months were noted in the MTM group (increased from 9.2% at baseline to 61% at 6 month) than the control or non-MTM group (increased from 13.2% at baseline (to 30.2% at 6 month; p<0.01) (Table 2). A significant difference in Morisky score were also noted between different time points (p<0.001).
Table 2. Difference in level of adherence intervention and control groups at baseline, 3 and 6 months.
| Adherence (Morisky score) | MTM (n=54) | Non-MTM (n=53) | ||||
|---|---|---|---|---|---|---|
| Good | Poor | p-value | Good | Poor | p-value | |
| At baseline | 5 (9.2%) | 49 (90.8%) | <0.001 | 7 (13.2%) | 46 (86.8%) | 0.462 |
| 3 months | 16 (29.6%) | 38 (70.4%) | 0.020 | 11 (20.7%) | 42 (79.3%) | 0.351 |
| 6 months | 33 (61%) | 21 (39%) | <0.001 | 16 (30.2%) | 37 (69.8%) | 0.261 |
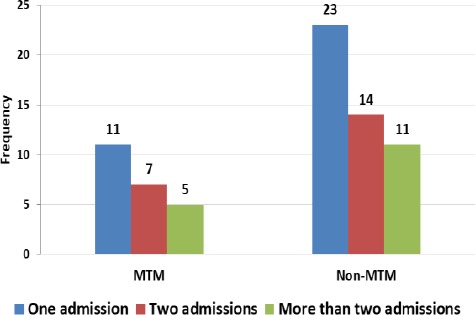
At the 6-month follow-up, only 23 patients in MTM group with poorly controlled blood sugar levels resulted in hospital admissions compared to 48 patients in non-MTM group, resulting in a 52.1% fewer hospital admissions (p<0.001). A higher rate of hospitalization (at least one hospitalization during the study period) was reported in control group (48 out of 53 patients) than intervention group (23 out of 54 patients) (Figure 2).
Figure 2. Number of hospital admissions for patients.
DISCUSSION
The involvement of pharmacists, as part of the interdisciplinary healthcare team, in every step of the medication use process has been shown to improve disease state management and pharmacotherapy, patient adherence and overall health-related quality of life.25 To the best of our knowledge, this is the first study to evaluate the impact of pharmacist-led MTM service on medication compliance and hospital admission in patients with type 2 diabetes in Ethiopia.
In our study, patients in both the intervention and control groups demonstrated poor adherence to anti-diabetic medications and high hospital admission rates at baseline. This could be explained by the relatively low socioeconomic and educational status of patients in our study. A study conducted in Northwest Ethiopia by Abebe et al. identified low educational status and dissatisfaction with the service received at the diabetic clinic as the main predictors of poor adherence to anti-diabetic medications.26 Patients with low socioeconomic and educational status are less likely to access education, and health care services including medication refills on time, which may increase patients’ difficulty in adhering to their treatment regimens.27 Furthermore, it has been shown that non-adherent patients had a higher hospitalization and mortality rate compared to adherent diabetic patients.28
The findings of the present study revealed a marked increase in medication adherence and reduction in hospital admission from baseline to 3 and 6 months in the intervention group than the control group. Our findings are similar to previous studies demonstrating the effect of pharmacist interventions to improve medication adherence.29,30,31 A systematic review of randomized clinical studies conducted by Cutrona et al. to improve medication adherence reported that 5 out of 6 studies that measured a customized pharmacist interventions significantly improved medication adherence by 7% to 27%.32 Another study conducted by Adepu et al. revealed that continuous monthly education for 3 months tended to improve adherence compared to a single educational session.33
Compared to the usual care, patients in the intervention group showed greater reduction in hospital admission. This may be due to the fact that the pharmacist adopted and utilized a pharmaceutical care plan, which involved preventing and resolving a number of medication therapy problems which leads to acute complications and subsequent hospital admissions such as hypoglycemia. A number of similar studies also reported that number of hospital admission and diabetic complication is minimized by pharmacist-led patient counseling and self-care practice training.34,35 Worldwide health care expenditures associated with diabetes including the cost of hospitalizations due to microvascular and macrovascular complications in patients with diabetes mellitus were more than 450 billion USD in 2011, accounting for about 10% of the total healthcare expenditure for adults. Even though there is a difference in the cost of treatment of diabetes and diabetes-related complications in different countries36,37, costs associated with the medications for diabetes disease state management, outpatient medications for diabetes related complications and the hospitalizations remains the main cost drivers in countries like Ethiopia. This is particularly important for developing countries like Ethiopia, where the governments’ annual per capita health care expenditure is less than USD 20 and patients generally can’t afford to pay for the additional costs associated with diabetes related hospitalizations. Such costs could be minimized by reducing the number of hospitalization through extensive pharmaceutical care service, as evidenced by the findings of our study.
Limitations
This study highlights an area of pharmacy practice where there is lack of literature in Ethiopia. The study has also a number of methodological strengths including randomization of patients. Yet, the study has some limitations that should be taken into account while interpreting the results. As study utilized data from a single teaching hospital with patients having easy access to health care facilities, relatively small sample size, and short follow-up period, caution should be exercised when generalizing to other patients with diabetes mellitus. Furthermore, the absence of a gold standard method to measure adherence (we used a self-reported adherence measurement, which is usually associated with recall and social desirability bias) and inability to access HbA1c measurement in our setting complicated assessment of the interventions provided. Even with the above limitations, this study has significant implications for improving the involvement of pharmacists in patient care and health promotion in Ethiopia.
CONCLUSIONS
The findings of the present study implied that a pharmacist-led MTM might improve medication adherence and reduce number of hospitalizations in patients with type 2 diabetes mellitus. Our study adds to the existing literature by demonstrating the positive impact of pharmacist-led MTM on medication adherence. Hence, policies and guidelines should be in place in order for clinical pharmacists to fully engage in patient care and improve the medication therapy outcomes of patients with type 2 diabetes mellitus. Future multicenter, prospective randomized controlled studies recruiting a large number of sample from a diverse population are warranted in order to confirm the generalizability of our results.
ACKNOWLEDGEMENTS
The authors acknowledge the support of the School of Pharmacy, University of Gondar in facilitating the data collection process. We are also grateful to all of the participants of the study.
Footnotes
CONFLICT OF INTEREST
None.
FUNDING
None.
Contributor Information
Daniel A. Erku, Department of Clinical Pharmacy, School of Pharmacy, College of Medicine and Health Sciences, University of Gondar. Gondar (Ethiopia). staymotivated015@gmail.com
Asnakew A. Ayele, Department of Clinical Pharmacy, School of Pharmacy, College of Medicine and Health Sciences, University of Gondar. Gondar (Ethiopia). asnake.21.uog@gmail.com
Abebe B. Mekuria, Department of Pharmacology, School of Pharmacy, College of Medicine and Health Sciences, University of Gondar. Gondar (Ethiopia). abeyohannes21@gmail.com
Sewunet A. Belachew, Department of Clinical Pharmacy, School of Pharmacy, College of Medicine and Health Sciences, University of Gondar. Gondar (Ethiopia). sewunet.admasu@gmail.com
Bisrat Hailemeskel, Associate Professor and Director of Drug Information Services School of Pharmacy, College of Pharmacy, Nursing, and Allied Health Sciences, Howard University. Washington, DC (United States). bhailemeskel@howard.edu.
Henok G. Tegegn, Department of Clinical Pharmacy, School of Pharmacy, College of Medicine and Health Sciences, University of Gondar. Gondar (Ethiopia). heniget@gmail.com
References
- 1.World Health Organization:Global strategy on diet, physical activity and health. Geneva: WHO; 2004. [Google Scholar]
- 2. [accessed 1 Aug 2017];IDF Diabetes Atlas. (Seventh Ed). 2015 Accessed at www.diabetesatlas.org .
- 3.Nshisso LD, Reese A, Gelaye B, Lemma S, Berhane Y, Williams MA. Prevalence of hypertension and diabetes among Ethiopian adults. Diabetes Metab Syndr. 2012;6(1):36–41. doi: 10.1016/j.dsx.2012.05.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Venkartesan R, Devi AS, Parasuraman S, Sriram S. Role of community pharmacist in improving knowledge and glycemic control of type 2 diabetes. Perspect Clin Res. 2012;3(1):26–31. doi: 10.4103/2229-3485.92304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.O'Loughlin J, Masson P, Déry V, Fagnan D. The role of community pharmacists in health education and disease prevention:a survey of their interests and needs in relation to cardiovascular disease. Prev Med. 1999;28(3):324–331. doi: 10.1006/pmed.1998.0436. [DOI] [PubMed] [Google Scholar]
- 6.Paes AHP, Bakker A, Soe-Agnie CJ. Impact of dosage frequency in patient compliance. Diabetes Care. 1997;20(10):1512–1517. doi: 10.2337/diacare.20.10.1512. [DOI] [PubMed] [Google Scholar]
- 7.Lindenmeyer A, Hearnshaw H, Vermeire E, Van Royen P, Wens J, Biot Y. Interventions to improve adherence to medication in people with type 2 diabetes mellitus:a review of the literature on the role of pharmacists. J Clin Pharm Ther. 2006;31(5):409–419. doi: 10.1111/j.1365-2710.2006.00759.x. [DOI] [PubMed] [Google Scholar]
- 8.World Health Organization. Adherence to long-term therapies:evidence for action. Geneva: WHO; 2003. [accessed 1 Aug 2017]. www.who.int/chp/knowledge/publications/adherence_report/en/ [Google Scholar]
- 9.World Health Organization. The Pursuit of Responsible Use of Medicines:Sharing and Learning from Country Experiences. Geneva: WHO; 2012. [Google Scholar]
- 10.Yarnall KSH, Østbye T, Krause KM, Pollak KI, Gradison M, Michener JL. Family Physicians as Team Leaders: ‘Time’ to Share the Care. [accessed 1 Aug 2017];Preventing Chronic Disease. 6(2):A59. www.cdc.gov/pcd/issues/2009/apr/08_0023.htm . [PMC free article] [PubMed] [Google Scholar]
- 11.Dent LA, Harris KJ, Noonan CW. Randomized trial assessing the effectiveness of a pharmacist-delivered program for smoking cessation. Ann Pharmacother. 2009;43(2):194–201. doi: 10.1345/aph.1L556. [DOI] [PubMed] [Google Scholar]
- 12.Gerber RA, Liu G, Mccombs JS. Impact of pharmacist consultations provided to patients with diabetes on healthcare costs in a health maintenance organization. Am J Manag Care. 1998;4(7):991–1000. [PubMed] [Google Scholar]
- 13.Bajorek B, LeMay KS, Magin P, Roberts C, Krass I, Armour CL. Implementation and evaluation of a pharmacist-led hypertension management service in primary care:outcomes and methodological challenges. Pharm Pract (Granada) 2016;14(2):723. doi: 10.18549/PharmPract.2016.02.723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Irons BK, Meyerrose G, Laguardia S, Hazel K, Seifert CF. A collaborative cardiologist-pharmacist care model to improve hypertension management in patients with or at high risk for cardiovascular disease. Pharm Pract (Granada) 2012;10(1):25–32. doi: 10.4321/s1886-36552012000100005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bluml BM. Definition of medication therapy management:development of profession wide consensus. J Am Pharm Assoc (2003) 2005;45(5):566–572. doi: 10.1331/1544345055001274. [DOI] [PubMed] [Google Scholar]
- 16.Sisson E, Kuhn C. Pharmacist roles in the management of patients with type 2 diabetes. J Am Pharm Assoc (2003) 2009;49(Suppl 1):S41–S45. doi: 10.1331/JAPhA.2009.09075. [DOI] [PubMed] [Google Scholar]
- 17.Skowron A, Polak S, Brandys J. The impact of pharmaceutical care on patients with hypertension and their pharmacists. Pharm Pract (Granada) 2011;9(2):110–115. doi: 10.4321/s1886-36552011000200009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Jennings DL, Ragucci KR, Chumney ECG, Wessell AM. Impact of clinical pharmacist intervention on diabetes related quality-of-life in an ambulatory care clinic. Pharm Pract (Granada) 2007;5(4):169–173. doi: 10.4321/s1886-36552007000400005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mekonnen AB, Yesuf EA, Odegard PS, Wega SS. Implementing ward based clinical pharmacy services in an Ethiopian University Hospital. Pharm Pract (Granada) 2013;11(1):51–57. doi: 10.4321/s1886-36552013000100009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Geremew E, Worku F, Tadeg H, Ejigu E, Mekonnen N Building Local Capacity for Clinical Pharmacy Service in Ethiopia through a Holistic In-Service Training Approach. Submitted to the US Agency for International Development by the Systems for Improved Access to Pharmaceuticals and Services (SIAPS) Program. Arlington, VA: Management Sciences for Health; 2014. [Google Scholar]
- 21.Krousel-Wood MA, Muntner P, Islam T, Morisky DE, Webber LS. Barriers to and determinants of medication adherence in hypertension management:perspective of the cohort study of medication adherence among older adults. Med Clin North Am. 2009;93(3):753–769. doi: 10.1016/j.mcna.2009.02.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens (Greenwich) 2008;10(5):348–354. doi: 10.1111/j.1751-7176.2008.07572.x. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 23.Krousel-Wood M, Islam T, Webber LS, Re RN, Morisky DE, Muntner P. New medication adherence scale versus pharmacy fill rates in seniors with hypertension. Am J Manag Care. 2009;15(1):59–66. [PMC free article] [PubMed] [Google Scholar]
- 24.Bruce SP, Acheampong F, Kretchy I. Adherence to oral anti-diabetic drugs among patients attending a Ghanaian teaching hospital. Pharm Pract (Granada) 2015;13(1):533. doi: 10.18549/pharmpract.2015.01.533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Shah A. “Pharmacy Intervention in the Medication Use Process:The Role of Pharmacists in Improving Patient Safety.”. University of Manitoba; Winnipeg, Canada: 2010. [Google Scholar]
- 26.Abebe SM, Berhane Y, Worku A. Barriers to diabetes medication adherence in North West Ethiopia. Springerplus. 2014;3:195. doi: 10.1186/2193-1801-3-195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Seligman HK, Jacobs EA, Lopez A, Tschann J, Fernandez A. Food insecurity and glycemic control among low-income patients with type 2 diabetes. Diabetes Care. 2012;35(2):233–238. doi: 10.2337/dc11-1627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ho PM, Bryson CL, Romfield JS. Medication adherence;its importance in cardiovascular outcome. Circulation. 2009;119(23):3028–3035. doi: 10.1161/CIRCULATIONAHA.108.768986. [DOI] [PubMed] [Google Scholar]
- 29.Kripalani S, Yao X, Haynes RB. Interventions to enhance medication adherence in chronic medical conditions:a systematic review. Arch Intern Med. 2007;167(6):540–550. doi: 10.1001/archinte.167.6.540. [DOI] [PubMed] [Google Scholar]
- 30.Lee JK, Grace KA, Taylor AJ. Effect of a pharmacy care program on medication adherence and persistence, blood pressure, and low density lipoprotein cholesterol:a randomized controlled trial. JAMA. 2006;296(21):2563–2571. doi: 10.1001/jama.296.21.joc60162. [DOI] [PubMed] [Google Scholar]
- 31.Donnelly LA, Morris AD, Evans JM DARTS/MEMO Collaboration. Adherence to insulin and its association with glycaemic control in patients with type 2 diabetes. QJM. 2007;100(6):345–350. doi: 10.1093/qjmed/hcm031. [DOI] [PubMed] [Google Scholar]
- 32.Cutrona SL, Choudhry NK, Fischer MA, Servi A, Liberman JN, Brennan TA, Shrank WH. Modes of delivery for interventions to improve cardiovascular medication adherence:Review. Am J Manag Care. 2010;16(12):929–942. [PMC free article] [PubMed] [Google Scholar]
- 33.Adepu R, Ari SM. Influence of structured patient education on therapeutic outcomes in diabetes and hypertensive patients. Asian J Pharm Clin Res. 2010;3(3):174–178. [Google Scholar]
- 34.Xin C, Xia Z, Jiang C, Lin M, Li G. Effect of pharmaceutical care on medication adherence of patients newly prescribed insulin therapy:a randomized controlled study. Patient Prefer Adherence. 2015;9:797–802. doi: 10.2147/PPA.S84411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Antoine SL, Pieper D, Mathes T, Eikermann M. Improving the adherence of type 2 diabetes mellitus patients with pharmacy care:a systematic review of randomized controlled trials. BMC Endocr Disord. 2014;14:53. doi: 10.1186/1472-6823-14-53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Gordois A, Shuffham P, Shaerer A, Oglesby A. The health care costs of diabetic nephropathy in the United States and the United Kingdom. J Diabetes Complications. 2004;18(1):18–26. doi: 10.1016/S1056-8727(03)00035-7. [DOI] [PubMed] [Google Scholar]
- 37.Doneva M, Valov V, Borisova A-M, Tankova T, Savova A, Manova M, Czech M, Petrova G. Comparative analysis of the cost of insulin treated patients in Bulgaria. Biotechnol Biotechnol Equip. 2013;27(2):3748–3752. doi: 10.5504/BBEQ.2013.0001. [DOI] [Google Scholar]