

Every 10 seconds, a worker is temporarily or permanently disabled and some of them are physicians and surgeons. It is a well-known fact that medical professionals are prone to musculoskeletal disorders (MSDs), with ophthalmologists being particularly at a higher risk.[1,2] Common MSDs in ophthalmologists include disabling back pain, neck pain, numbness in the hands and legs, and carpal tunnel syndrome.[1,2] It may be hard to believe that most work-related disabilities in ophthalmologists are caused by simply doing the routine – performing a slit-lamp examination, using an indirect ophthalmoscope, or even sitting on a surgeon's chair.[1] Although these injuries are chronic in evolution, the effects can be devastating.
Here are some hard facts:
A survey of 325 practicing ophthalmologists in the United Kingdom in 1994 found that 54% had significant back pain, with those longest in practice being worse affected.[3] This number seems to have risen to 64% according to a more recent study.[4] Significantly, 34% reported pain while operating, and 32% had pain while using a slit-lamp
In a survey of 162 ophthalmologists in Iran, 80% reported chronic back pain and 55% had chronic headaches[5]
A survey of American ophthalmologists in 2005 revealed that 52% of the 697 respondents reported neck, upper body, or lower back pain, with 15% having to curtail their work as a consequence.[6] Low back pain was present in 39% of respondents, followed by upper extremity symptoms (33%) and neck pain (33%)
Two-thirds of ophthalmologists in Saudi Arabia had mild to moderate neck and upper back pain[7]
This issue of Indian Journal of Ophthalmology carries the results of a survey among practicing Indian ophthalmologists, which pegs self-reported back pain at a concerning 71%[8]
Vitreoretinal surgeons are specifically at a high risk of developing MSD.[9] As expected, among a large cohort of vitreoretinal surgeons, 55% reported both back and neck pain, and 7% required surgery to relieve their symptoms[1]
Of 130 American ophthalmic plastic surgeons, 73% had pain associated while performing surgery; nine of them had to discontinue operating as consequence.[10]
It is evident that improper work ergonomics leads to disability, poor productivity, and early retirement.[11,12,13,14,15] The National Institute of Occupational Safety and Health has identified four factors influencing the development of MSDs: (1) environmental hazards, (2) human biologic factors, (3) behavioral factors or unhealthy lifestyles, and (4) inadequacies in existing health care.[11] The problem being multifactorial, intervention to minimize the risk must have a layered approach.
Physical strains directly associated with the ophthalmic profession including stress on the shoulders, neck, back, arms, and hands resulting from poor posture during examination and surgery as well as repetitive actions common to the surgical profession are some of the modifiable risk factors. One of the eminently modifiable situations is ergonomic redesigning of our individual work places. Ergonomics is the process of designing or arranging workplaces, products, and systems so that they suit the professionals who use them. This is in sharp contrast to the typical hospital design that assumes that one size fits all.
The American Academy of Ophthalmology recognized the problem early and set up a task force to address the issue. The task force offers an online course encompassing the best practices in work place ergonomics.[12,13,14] Experts have recommended essential work ergonomics to help alleviate MSDs faced by the ophthalmologists [Table 1 and Figs. 1 and 2].[13,14,15] Ergonomic intervention as detailed in Table 1, prophylactic neck and back exercises and timely professional consultation may help alleviate symptoms and maintain better work efficiency.[13,14] In a study of dentists undergoing an ergonomic makeover, a majority of them reported disappearance of their symptoms.[16] In that same study, the mean working hours and work efficiency reportedly improved.
Table 1.
Ergonomics for an ophthalmologist – risk factors and possible solutions
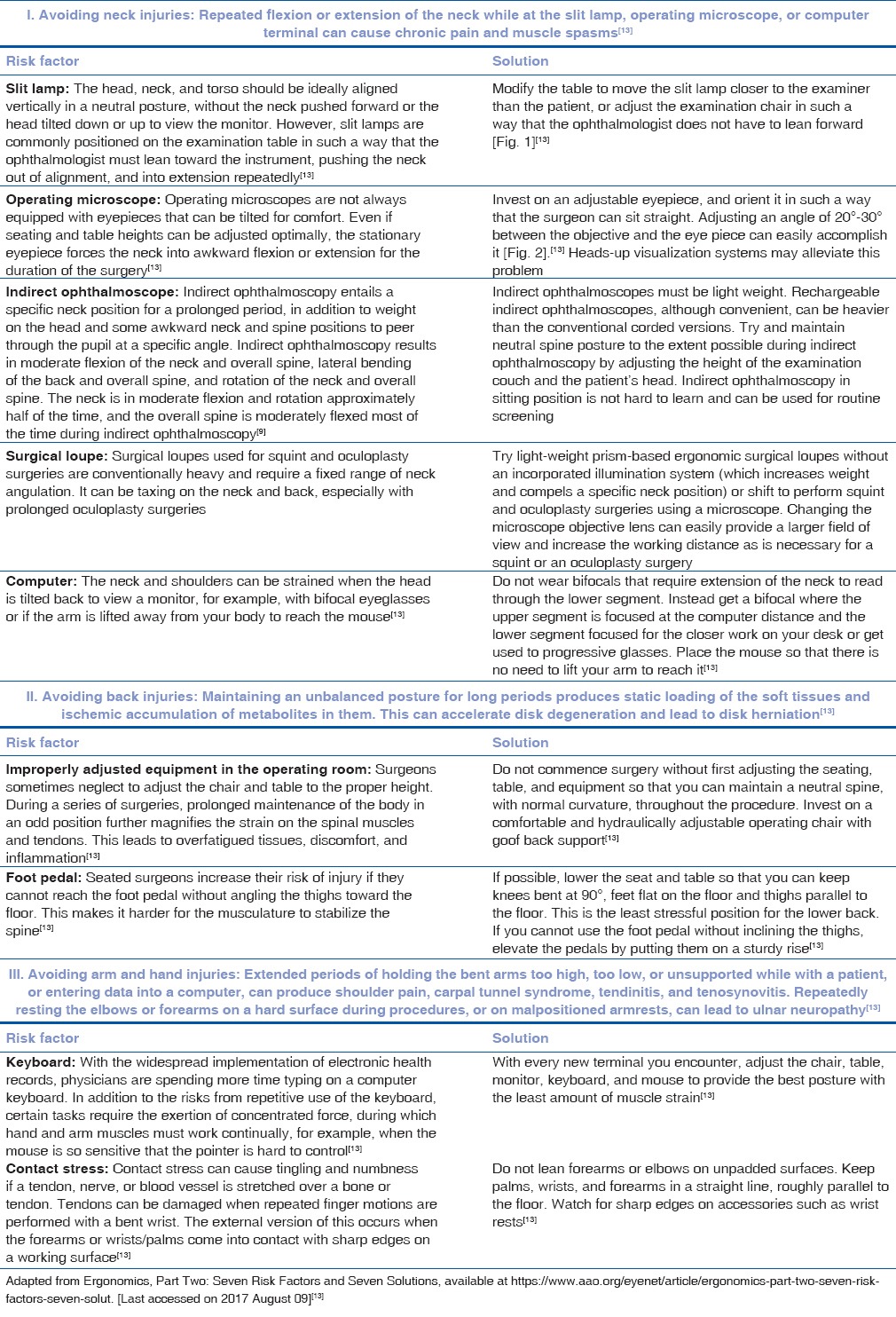
Figure 1.

Posture for slit-lamp evaluation. Ophthalmologist is slumping toward the slit-lamp with the neck extended, thus putting strain on the neck and back (left) – this is a wrong posture. Ophthalmologist has brought the slit-lamp forward and has adjusted the height to sit erect without having to lean forward or change the neck angle (right) – this is an ergonomically appropriate posture. (Adapted from http://www.ophthalmologymanagement.com/issues/2012/january-2012/of-ophthalmologists-aching-backs)[15]
Figure 2.

Posture for operating microscope. Microscope ocular and objective are at a straight line, with the ophthalmologist having to lean forward constantly (left) – this is a wrong posture. If the ocular is moved 20°–25° toward the surgeon and the operating chair height is appropriately adjusted, the surgeon can sit straight (right) – this is an ergonomically appropriate posture. (Adapted from http://www.ophthalmologymanagement.com/issues/2012/january-2012/of-ophthalmologists-aching-backs)[15]
About 50 years ago, Laufman was duly concerned that “only a few surgeons have made the surgical environment their main research interest.”[17,18] The situation has not changed much. Our efforts to create an ergonomic clinic and operating room environment will require paradigm changes in the traditional concepts of design to have customization built into standardized hospital architecture. Instrument manufacturers should be provided with user-driven information to optimize ergonomics and provide adjustability. A greater involvement in this transformation by the ophthalmologists themselves may help accomplish the twin goals of personal well-being and increased efficiency while maintaining patient and staff safety.
References
- 1. [Last accessed on 2017 Aug 09]. Available from: https://www.reviewofophthalmology.com/article/will-ophthalmology-cripple-you .
- 2.Natarajan S, Nair AG. Is ophthalmology becoming a pain in the neck? Indian J Ophthalmol. 2016;64:413–4. doi: 10.4103/0301-4738.187648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Chatterjee A, Ryan WG, Rosen ES. Back pain in ophthalmologists. Eye (Lond) 1994;8(Pt 4):473–4. doi: 10.1038/eye.1994.112. [DOI] [PubMed] [Google Scholar]
- 4.Hyer JN, Lee RM, Chowdhury HR, Smith HB, Dhital A, Khandwala M. National survey of back and neck pain amongst consultant ophthalmologists in the United Kingdom. Int Ophthalmol. 2015;35:769–75. doi: 10.1007/s10792-015-0036-z. [DOI] [PubMed] [Google Scholar]
- 5.Chams H, Mohammadi SF, Moayyeri A. Frequency and assortment of self-report occupational complaints among Iranian ophthalmologists: A preliminary survey. MedGenMed. 2004;6:1. [PMC free article] [PubMed] [Google Scholar]
- 6.Dhimitri KC, McGwin G, Jr, McNeal SF, Lee P, Morse PA, Patterson M, et al. Symptoms of musculoskeletal disorders in ophthalmologists. Am J Ophthalmol. 2005;139:179–81. doi: 10.1016/j.ajo.2004.06.091. [DOI] [PubMed] [Google Scholar]
- 7.Al-Marwani Al-Juhani M, Khandekar R, Al-Harby M, Al-Hassan A, Edward DP. Neck and upper back pain among eye care professionals. Occup Med (Lond) 2015;65:753–7. doi: 10.1093/occmed/kqv132. [DOI] [PubMed] [Google Scholar]
- 8.Venkatesh R, Kumar S. Back pain in ophthalmology: National survey of Indian ophthalmologists. Indian J Ophthalmol. 2017;65:678–82. doi: 10.4103/ijo.IJO_344_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Shaw C, Bourkiza R, Wickham L, Mccarthy I, Mckechnie C. Mechanical exposure of ophthalmic surgeons: A quantitative ergonomic evaluation of indirect ophthalmoscopy and slit-lamp biomicroscopy. Can J Ophthalmol. 2017;52:302–7. doi: 10.1016/j.jcjo.2016.09.011. [DOI] [PubMed] [Google Scholar]
- 10.Sivak-Callcott JA, Diaz SR, Ducatman AM, Rosen CL, Nimbarte AD, Sedgeman JA. A survey study of occupational pain and injury in ophthalmic plastic surgeons. Ophthal Plast Reconstr Surg. 2011;27:28–32. doi: 10.1097/IOP.0b013e3181e99cc8. [DOI] [PubMed] [Google Scholar]
- 11. [Last accessed on 2017 Aug 09]. Available from: https://www.cdc.gov/niosh/index.htm .
- 12. [Last accessed on 2017 Aug 09]. Available from: https://www.aao.org/course/ergonomics-best-practices-course .
- 13. [Last accessed on 2017 Aug 09]. Available from: https://www.aao.org/eyenet/article/ergonomics-part-two-seven-risk-factors-seven-solut .
- 14. [Last accessed on 2017 Aug 09]. Available from: https://www.aao.org/eyenet/article/ergonomics-part-one-is-job-you-love-pain-in-neck .
- 15. [Last accessed on 2017 Aug 09]. Available from: http://www.ophthalmologymanagement.com/issues/2012/january-2012/of-ophthalmologists-aching-backs .
- 16.Droeze EH, Jonsson H. Evaluation of ergonomic interventions to reduce musculoskeletal disorders of dentists in the Netherlands. Work. 2005;25:211–20. [PubMed] [Google Scholar]
- 17.Laufman H. What's wrong with our operating rooms? Am J Surg. 1971;122:332–43. doi: 10.1016/0002-9610(71)90253-4. [DOI] [PubMed] [Google Scholar]
- 18.Berguer R. Surgery and ergonomics. Arch Surg. 1999;134:1011–6. doi: 10.1001/archsurg.134.9.1011. [DOI] [PubMed] [Google Scholar]