

Abstract
Rumination is a well-established vulnerability factor for depression that may exert deleterious effects both independently and in interaction with stress. The current study examined momentary ruminative self-focus (MRS) and stress-reactive rumination (SRR) as predictors of depressive symptoms utilizing a smartphone ecological momentary assessment (EMA) design. 121 undergraduates responded to four text message alerts per day for one week in which they indicated the occurrence of life stress, rumination, and depressed mood. SRR, but not MRS, independently predicted increases in depressive symptoms. MRS interacted with depressive symptoms to predict increases in symptoms at the subsequent timepoint, supporting the deleterious effects of depressive rumination on future mood state. Interactions emerged between stress and both MRS and SRR, such that experiencing higher levels of stressors and rumination at an observation predicted greater increases in depressive symptoms. To our knowledge, this study is the first to demonstrate that state rumination moderates the effect of stress in predicting depressive symptoms using EMA methodology. Results suggest that rumination levels in response to stress vary within individuals and can have an important effect on depressed mood. Findings may have important clinical implications, as lessening individuals’ tendency to engage in rumination following stress may help to alleviate depressive symptoms.
Keywords: rumination, ecological momentary assessment, stress, depression
Major depressive disorder (MDD) is the most common psychiatric disorder, associated with major personal, societal, and economic costs (Birnbaum et al., 2010; Kessler, Merikangas, & Wang, 2007). Rumination, characterized by repetitive, passive thoughts about the symptoms, causes, and future repercussions of one’s depression, is thought to perpetuate depressed mood, as outlined in the response styles theory of depression (Nolen-Hoeksema, 1991). Indeed, a wealth of research has established trait rumination’s role as a major risk factor for MDD that is predictive of the onset, length, and number of depressive episodes experienced (Wisco & Nolen-Hoeksema, 2008). However, the influence of rumination at the state level is less clear. The current study utilized ecological momentary assessment (EMA) methodology to better understand the role of state rumination and stress as predictors of depressive symptoms over time.
Rumination may contribute to depression in interaction with the experience of life stress, in line with the well-supported vulnerability-stress model of depression (Abramson et al., 2002; Hammen, 2005). Indeed, in an influential early study conducted within a nonclinical sample, students scoring higher in initial levels of trait rumination demonstrated greater increases in depressive symptoms following the experience of a major stressor, the 1989 Lomo Prieta earthquake (Nolen-Hoeksema & Morrow, 1991). This relationship also has been supported in nonclinical experimental paradigms, in which individuals who either scored higher on self-report measures of rumination (Feldner, Leen-Feldner, Zvolensky, & Lejuez, 2006) or underwent a rumination induction (Watkins, Moberly, & Moulds, 2008) demonstrated greater increases in depressive symptoms following an in-lab stressor.
An extension of this literature has examined rumination occurring after the experience of stress, referred to as stress-reactive rumination (SRR; Robinson & Alloy, 2003). Individuals engaging in SRR make negative inferences about the events that they have experienced and ruminate about these beliefs, such as that the event’s occurrence was entirely their fault. Those displaying higher trait levels of SRR, as measured by the Stress-Reactive Rumination Scale (SRRS; Robinson & Alloy, 2003), are more likely to experience major depressive disorder over time, suggesting that SRR serves as an important vulnerability for MDD (Alloy et al., 2000; Robinson & Alloy, 2003).
Given that SRR occurs in response to life stress, it is vital to study its frequency following the experience of actual stressors. A daily diary study of undergraduates found that although SRR did not independently predict depressive symptoms, there was a significant positive interaction between SRR and number of stressors per day in predicting same-day depressive symptoms, consistent with a vulnerability-stress framework (Genet & Siemer, 2012). Ecological momentary assessment (EMA) designs, in which the occurrence of rumination and stress are measured multiple times per day, have found that momentary rumination mediated the role of life stress in prospectively predicting depressive symptoms in both nonclinical (Moberly & Watkins, 2008a) and clinical samples (Ruscio et al., 2015). Although neither study found momentary, state-level rumination to moderate the role of stress in predicting depression, such a relationship was reported between trait rumination and daily stress, providing support for response styles theory (Moberly & Watkins, 2008a).
In addition to examining the effect of SRR on depressive symptoms, the degree to which individuals engage in ruminative, self-focused thought irrespective of proximal stressors is also worthy of study. A novel line of research has investigated the relationship between momentary ruminative self-focus (MRS) during periods of rest, in which individuals are not engaged in a specific task and their minds are able to wander, and their subsequent mood symptoms. A nonclinical study of undergraduates found that those who scored higher on a baseline scale of cognitive reactivity and engaged in more ruminative, internally-focused thought during rest, as measured by the Momentary Ruminative Self-focus Inventory (MRSI; Mor, Marchetti, & Koster, 2013) showed increased depressive symptoms (Marchetti, Koster, & De Raedt, 2013). Furthermore, nonclinical EMA studies have found that engaging in negative ruminative self-focus, irrespective of the occurrence of proximal stressors, predicts depressive symptoms both concurrently (Ottaviani et al., 2015; Takano & Tanno, 2010) and prospectively (Moberly & Watkins, 2008b), and has been linked to increased heart rate and decreased autonomic flexibility (Ottaviani et al., 2015). Thus, these findings indicate that momentary rumination is also an important vulnerability factor for depressive symptoms independent of the experience of life stress. Indeed, given extensive research demonstrating the negative effects of ruminating about one’s depression, it is likely that the effects of momentary rumination would be exacerbated when concurrently experiencing down mood (Wisco & Nolen-Hoeksema, 2008). Focused examination of the relationship between current mood state and momentary rumination in predicting subsequent depressive symptoms is needed.
Together, this research emphasizes the need to examine the relationships between rumination, life stress, and depressive symptoms as they occur in real-time utilizing EMA techniques. The use of this methodology is important for several reasons. First, EMA assessment is less likely to fall victim to recall biases in which individuals provide inaccurate retrospective reports of rumination levels or stress. Second, these designs capture stress and ruminative processes in a natural setting, versus in structured laboratory paradigms, which may not generalize to real-world experiences. Third, the use of EMA results in many data points, allowing for examination of temporal relationships as well as providing increased confidence in the reliability of the data (Armey, Schatten, Haradhvala, & Miller, 2015; Shiffman, Stone, & Hufford, 2008; Stone et al., 1998; Wenze & Miller, 2010). Furthermore, it has been demonstrated that rumination levels fluctuate over time and are modestly stable at best, suggesting that trait measures may not accurately capture the phenomenology of this construct (Moberly & Watkins, 2008a; Takano & Tanno, 2011).
Current Study
The current study sought to build on previous findings by utilizing an EMA design to assess the role of both momentary ruminative self-focus irrespective of proximal stressors (e.g., Right now, I am thinking about the possible meaning of the way I feel) and stress-reactive rumination in response to stressor occurrence (e.g., I’m thinking about how the stressful event is all my fault) in predicting depressive symptoms over time. Participants responded to text message alerts on their smartphones four times a day for one week, in which they indicated the occurrence of life stressors, their degree of engagement in SRR directly after event occurrence, and their current mood state and level of momentary ruminative self-focus regardless of whether a stressor was reported. The SRR and MRS measures were derived from the validated SRRS and MRSI questionnaires, respectively. Trait measures of rumination and depression also were collected at a baseline session.
It was hypothesized that observation-level increases in both MRS and SRR relative to individuals’ mean levels would independently predict increases in depressive symptoms, and that individuals with higher mean levels of MRS and SRR across the EMA week would display greater increases in depressive symptoms. In addition, MRS was hypothesized to interact with depressive symptoms at the same timepoint to predict increases in subsequent symptoms, given established deleterious effects of ruminating about one’s depressed mood. Significant interactions were hypothesized to emerge between stressor occurrence and both state-level MRS and SRR in predicting increases in depressive symptoms over time. Finally, in accordance with response styles theory, it was hypothesized that significant interactions would emerge between trait measures of rumination collected at baseline and the experience of stress during the EMA week in predicting prospective increases in depressive symptoms.
The present EMA study is the first to examine both momentary ruminative self-focus and stress-reactive rumination within the same design, and is the first to derive its momentary rumination items directly from the SRRS and MRSI questionnaires in order to best assess these constructs. Furthermore, previous depressive symptoms serve as controls in all analyses, allowing for truly prospective tests of increases in depressive symptoms. It is important to note that previously conducted EMA and daily diary studies either did not control for depressive symptoms at the previous observation (Genet & Siemer, 2012; Moberly & Watkins, 2008a; Takano & Tanno, 2010) or their effects were no longer significant when doing so (Ruscio et al., 2015), precluding interpretations that momentary rumination predicted relative increases in depressive symptoms over time, and thus, highlighting a necessary area of further study.
The current design allows for a thorough examination of rumination’s contribution to temporal changes in depressive symptoms, both independently and in interaction with current mood and stress, during participants’ daily functioning outside of the laboratory. Findings from this research not only will serve to better characterize the nature of ruminative thought patterns, but also will help to identify the ways in which rumination contributes to depressed mood, allowing for more targeted interventions with the ultimate goal of alleviating depressive symptoms.
Method
Participants
One hundred twenty-two undergraduate and graduate students of varied disciplines were recruited from the online study pool of the Temple University psychology department. For inclusion, participants were required to be age 18 or older, fluent in English, and cognitively able to complete all study components. Participants were offered the choice of cash or course credit as compensation for study participation. This study was approved by the Temple University Institutional Review Board and all participants provided informed consent prior to participation. One participant withdrew due to time constraints, resulting in a final sample of 121 participants (Mage = 21.74 years ± 5.21, range: 18 – 50). The sample was 69.4% female and racially and ethnically diverse (54.5% White, 18.2% Black, 14% Asian, 9.1% Hispanic, and 4.2% Biracial).
Measures
Semi-structured diagnostic interview
Schedule of Affective Disorders and Schizophrenia, Lifetime (SADS-L, Endicott & Spitzer, 1978)
The current study utilized the depression module of the expanded version of the SADS-L semi-structured diagnostic interview (exp-SADS-L; see Alloy et al., 2012). This modified version included additional probes to allow for diagnosis of DSM–IV–TR (American Psychiatric Association, 2000) depressive disorders. The depression module of the exp-SADS-L was conducted by student investigators who received extensive training in interview administration, including assigned readings, case vignettes, role-playing, conducting supervised live interviews, and regular case conferencing to achieve consensus regarding diagnostic impressions. Exp-SADS-L interviews administered by researchers trained using this protocol display high interrater reliability with kappas > .80 (Alloy et al., 2000).
Trait-level questionnaires
Stress-Reactive Rumination Scale (SRRS; Robinson & Alloy, 2003)
The SRRS is a 25-item questionnaire assessing the extent to which individuals direct their focus on negative attributions and inferences, hopeless cognitions, and coping and problem-solving strategies following the experience of life stress. Participants rate their degree of focus from 0% (Not focus on this at all) to 100% (Focus on this to a great extent). The current study utilized the 9-item negative attributions and inferences subscale, which has demonstrated good test-retest reliability, internal consistency and validity in predicting major depressive episodes (Robinson & Alloy, 2003). For ease of interpretation, total scores were divided by ten in the current analyses, creating a response range of 0 to 90.
Ruminative Response Scale of the Response Styles Questionnaire (RRS; Nolen-Hoeksema & Morrow, 1991)
The RRS contains 22 items assessing a person’s tendency to think about the symptoms, causes, and consequences of their depressed mood. A subsequent psychometric analysis of the RRS, intended to better isolate the construct of ruminative thought from overall depressive symptomatology, resulted in the removal of 12 items and the creation of reflective and brooding subscales (Treynor, Gonzalez, & Nolen-Hoeksema, 2003). The current study utilized the 5-item brooding subscale (RRS-B), which measures more passive, repetitive cognitions regarding one’s depressed mood and is thought to represent maladaptive rumination. The RRS is internally consistent and moderately correlated with alternative measures of rumination (Nolen-Hoeksema & Morrow, 1991; Siegle, Moore, & Thase, 2004).
Beck Depression Inventory (BDI-II; Beck, Steer, & Brown, 1996)
On a scale of 0 to 3, participants rate the degree to which they experienced symptoms of depression during the past two weeks. The BDI-II is the most widely used self-report measure of depressive symptoms and has demonstrated excellent internal consistency and validity in undergraduates (Dozois, Dobson, & Ahnberg, 1998; Storch, Roberti, & Roth, 2004).
EMA questionnaires
Stress-Reactive Rumination Scale-State (SRRS-S)
The SRRS-S is a modified 5-item version of the SRRS (Robinson & Alloy, 2003) created to measure participants’ responses directly after the experience of stress during the EMA week. It includes one item per component of the negative inferences and attributions domain: Negative Attributions/Stable (Think about how things like this always happen to you), Negative Attributions/Global (Think that the cause of the event will lead to additional stressful events in your life), Negative Attributions/Internal (Think about how the stressful event is all your fault), Negative Inferences/Self (Think about what the occurrence of the event means about you), and Negative Inferences/Future (Think about how the negative event will negatively affect your future). The SRRS rating scale of 0 to 100% was presented as a slider bar on participants’ smartphones. For ease of interpretation, total scores were divided by ten in the current analyses, creating a response range of 0 to 50. The SRRS-S had an α = .81 and was moderately correlated with baseline SRRS (r = .49) and RRS-B (r = .36) scores in this sample.
Momentary Ruminative Self-Focus Inventory-Abbreviated (MRSI-A)
The MRSI is a 6-item questionnaire measuring state-level fluctuations in ruminative self-focus (Mor et al., 2013). Three items were chosen for use during the EMA week, referred to here as the MRSI-A: 1) Right now, I am thinking about how happy or sad I feel, 2) Right now, I wonder why I react the way I do, and 3) Right now, I am thinking about the possible meaning of the way I feel. Participants indicated their degree of rumination at the time of the alert using a fixed 7-point Likert scale, ranging from 1 (Strongly disagree) to 7 (Strongly agree). The MRSI has displayed excellent internal consistency and is moderately correlated with alternative measures of rumination (Mor et al., 2013). The MRSI-A had an α = .85 and was moderately correlated with baseline RRS-B (r = .25) and SRRS (r = .31) scores in this sample.
State Depression Scale (SDS)
The SDS is a 3-item scale in which participants rated their level of depressed mood, anhedonia, and irritability on 7-point Likert scales ranging from 1 (Not at all) to 7 (Very much) at the time of the alert. The SDS is in part modeled after a scale used in a previous EMA study of rumination and depression (Moberly & Watkins, 2008a). The scale was presented as a slider bar on participants’ smartphones. The SDS had an α = .77 and was strongly correlated with baseline BDI scores (r = .50) in this sample.
Procedure
At the Time 1 in-laboratory assessment (T1), participants completed the consenting process, the SADS-L, all trait-level self-report questionnaires (SRRS, RRS, BDI-II), and a briefing on the EMA procedure. Participants completed a sample text message alert sent to their smartphones and reviewed their responses with the researcher to ensure proper EMA functioning and procedure comprehension. Beginning one day following the in-lab assessment, participants received four smartphone alerts per day for seven days during a 12-hour period that they chose based on their anticipated schedule during the EMA week (e.g., 11 AM to 11 PM). Alerts were programmed at random times occurring a minimum of 90 minutes apart within four three-hour periods. Alerts were sent using the online text message reminder service OhDontForget.com and contained a link to a questionnaire on the customizable survey website FluidSurveys.com. Participants were instructed to respond to each alert within 30 minutes of receiving the text message and were informed that they would receive a cash or credit bonus if they completed at least 80% of EMA questionnaires within this window.
At each EMA alert, participants reported if any stressors had occurred since the previous alert within the following categories: school, work, social relationships, money, health, other. Participants were able to indicate up to two events per category. For each event, participants wrote a brief description of the occurrence and completed the SRRS-S. To prevent participants from neglecting to report stressors experienced in order to complete alerts faster, participants reporting no events indicated a neutral or positive event that occurred during the time period and completed an alternate version of the SRRS-S modified for neutral/positive events. This modified version was intended primarily to encourage accurate reporting and scores were not examined in the current study. Participants also completed the MRSI-A and SDS at each alert. In sum, at each alert participants reported event occurrence since the last alert and SRR at the time of the event (TE) and also rated their current level of MRS and depressive symptoms at the time of the alert (TA). One week following EMA completion, participants returned to the laboratory for a follow-up session to complete additional questionnaires and receive compensation.
Statistical Analyses
Hierarchical linear modeling analyses were performed using HLM 7 Hierarchical Linear and Nonlinear Modeling (Raudenbush, Bryk, & Congdon, 2010). EMA observations (Level 1) were nested within individuals (Level 2), in order to differentiate between within-person and between-person variance in predicting depressive symptoms over time.
Momentary ruminative self-focus analyses
HLM analyses tested whether stressor occurrence interacted with MRS at the time of the alert (TA MRSI-A) to predict depressive symptoms at the subsequent alert (TA+1 SDS), controlling for depressive symptoms at the previous alert (TA−1 SDS), in order to capture change in depressive symptoms over time.1 Although participants had the option to report multiple stressors per alert, participants reported only one event at 85% of the alerts (skewness = 1.21). To correct for the non-normality of this distribution, stressor occurrence was dummy coded to indicate either the absence or presence of any stressors at an alert. The Level 1 model can be described as:
SDSti refers to depressive symptoms at observation t (TA+1) for individual i, being predicted by stressor occurrence, rumination, and the interaction between these two variables at observation t (TA) for individual i, controlling for previous alert depressive symptoms (TA−1).
MRSI-A scores were person-mean centered to best capture the effect of fluctuations in rumination relative to individuals’ mean levels during the EMA week; the interaction term was created by multiplying this mean centered variable by the dummy coded stress variable. Time between alerts was not a significant predictor of depressive symptoms, and therefore, was not controlled for in the model. The Level 2 model can be described as:
Aggregated stress and MRSI-A variables were included to account for participants’ average experience of stressors and rumination throughout the EMA week. These scores were controlled for at Level 2 to partition within-person variance, referring to fluctuations in stress and MRSI-A scores from alert to alert within individuals at Level 1, from between-person variance, referring to differences in participants’ average number of stressors and rumination over the EMA week. T1 BDI-II score and SRRS score were controlled for, as they were significant (BDI-II; B = .13, p < .05) and marginally significant (SRRS; B = .03, p < .10) predictors of TA+1 SDS, controlling for TA−1 levels. RRS-B score, age, sex, and history of MDD were not significant predictors and were not controlled for in the model. All Level 2 variables were grand-mean centered. Allowing the slopes of all Level 1 predictors to randomly vary resulted in a significantly improved model fit (χ2(9) = 25.04, p < .01), indicating that the effect of these variables differed between people; therefore these random effects were retained in analyses.
To test the interaction between momentary rumination and current depressive symptoms, the Level 1 interaction of stress and MRSI-A was removed and replaced with an interaction between MRSI-A and concurrent depressive symptoms (TA SDS). The aggregated stress variable was removed from Level 2 and replaced with an aggregated SDS variable. Cross-level analyses were conducted by removing the Level 1 interaction of stress and MRSI-A, and instead including the interaction term derived from the Level 2 variable of interest (SRRS or RRS-B) and Level 1 stress score. Each interaction term was tested separately. The independent effects of all Level 2 variables also were controlled for. These cross-level analyses were run both predicting depressive symptoms at the subsequent timepoint (TA+1 SDS) and the concurrent timepoint (TA SDS), controlling for previous symptoms (TA−1 SDS).
Consistent with previous research and recommendations (Baron & Kenny, 1986; Moberly & Watkins, 2008a) mediation analyses utilized HLM to assess for significant relationships between 1) stress and next alert depressive symptoms, 2) stress and MRSI-A, and 3) MRSI-A and next alert depressive symptoms, controlling for previous depressive symptoms at Level 1 and aggregated stress and MRSI-A scores, T1 BDI, and T1 SRRS at Level 2.
Stress-reactive rumination analyses
These analyses tested the interaction between stress and SRRS-S score in predicting depressive symptoms over time. The SRRS-S was only completed if a participant indicated the occurrence of a stressor; given that there were no SRRS-S data at alerts for which no stress was reported, this interaction could not be tested utilizing the above alert-level procedure with a dummy-coded stress variable. Instead, composite per-day variables were created from all Level 1 measures to allow for variability in number of stressors experienced, as these scores take into account a maximum of four alert responses per day. As SRRS-S refers to rumination at the time of the event (TE) and is reported retrospectively, and SDS score refers to depressive symptoms at the time of alert completion (TA), it was deemed appropriate to predict to SDS on the same day as well as the subsequent day, given temporal difference in these variables. The Level 1 model can be described as:
SDSti refers to depressive symptoms at observation t (TD when predicting to the average of alerts on the same day, TD+1 when predicting to next day), averaged per day for individual i, being predicted by total stress per day, average SRRS-S per day, and the interaction between these two variables at observation t (TD) for individual i, controlling for previous day depressive symptoms (TD−1). Stress and SRRS-S scores were person-mean centered, and the interaction term was derived from these centered values. Time between measurements was not a significant predictor of depressive symptoms and therefore was not controlled for in the model. The Level 2 model can be described as:
T1 BDI-II score and SRRS score were controlled for, as they were significant or marginally significant predictors of TD and TD+1 SDS (Bs > .03, ps < .06), controlling for TD−1 levels. RRS-B score, age, sex, and history of MDD were not significant predictors and were not controlled for in the model. All Level 2 variables were grand-mean centered. Allowing the slopes of all Level 1 predictors to randomly vary did not result in a significantly improved model fit (χ2(9) = 12.22, p > .05); therefore, these random effects were not retained in analyses. The conditional effects (simple slopes) of significant interactions were probed using the protocol set forth by Preacher, Curran, and Bauer (2003).
Mediation analyses utilized HLM to assess for significant relationships between 1) stress and same day/next day depressive symptoms, 2) stress and SRRS-S, and 3) SRRS-S and same day/next day depressive symptoms, controlling for previous depressive symptoms at Level 1 and aggregated stress score, T1 BDI, and T1 SRRS at Level 2.
Results
Preliminary Analyses
Participants completed a total of 2,933 EMA alerts. Five percent of alerts were completed more than 30 minutes after receipt and were removed from analyses, resulting in a total of 2,791 alerts. Participants responded to 82% of alerts on time (23.07 alerts ± 3.78), which is comparable to response rates reported in similar EMA studies (Moberly & Watkins, 2008a; Ruscio et al., 2015). Number of alerts completed did not significantly differ based on age, sex, history of MDD, BDI, SRRS, or RRS-B score. Participants reported experiencing at least one negative event at 46% of completed alerts, with a maximum of five stressors being reported at any one alert. When alerts were summed within days, participants reported experiencing at least one negative event on 78% of the days, with a maximum of seven stressors being reported on any one day. Descriptive statistics for all measures are presented in Table 1. Intraclass correlations (ICCs) indicate that about half of the variance in Level 1 measures (range: 43–52%) existed between individuals, with the remaining variance being within individuals; these values are consistent with previous designs (Genet & Siemer, 2012) and indicate that a hierarchical linear modeling approach is appropriate.
Table 1.
Descriptive Statistics
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |||
|---|---|---|---|---|---|---|---|---|---|
| Trait Measures | 1 T1 Depressive Symptoms (BDI-II) | .48*** | .35*** | .32*** | .34*** | .28** | .50*** | ||
| 2 T1 Brooding Rumination (RRS) | .63*** | .01 | .25** | .36*** | .30** | ||||
| 3 T1 Stress-reactive Rumination (SRRS) | .01 | .31** | .49*** | .33*** | |||||
| EMA Measures | 4 Total # Stressors Endorsed | .15 | .17† | .41*** | |||||
| 5 Momentary Ruminative Self Focus (MRSI-A) | .41*** | .35*** | |||||||
| 6 Stress-reactive Rumination (SRRS-S) | .49*** | ||||||||
| 7 Depressive symptoms (SDS) | |||||||||
|
| |||||||||
| M | 11.88 | 10.48 | 39.83 | 9.46 | 10.01 | 20.56 | 6.05 | ||
| SD | 8.16 | 3.21 | 15.56 | 5.48 | 3.35 | 9.46 | 2.69 | ||
| Range | 0–50 | 5–20 | 5–85 | 0–25 | 3–21 | 0–50 | 3–21 | ||
| Cronbach’s Alpha | .85 | .74 | .82 | .85 | .81 | .77 | |||
| ICC | .52 | .45 | .43 | ||||||
Note. BDI-II = Beck Depression Inventory; RRS = Ruminative Response Scale; SRRS= Stress-Reactive Rumination Scale; MRSI-A= Momentary Ruminative Self-Focus Inventory-Abbreviated; SRRS-S= Stress-Reactive Rumination Scale-State; SDS = State Depression Scale.
There was a significant range in depressive symptoms within the sample as measured by the BDI-II (M = 11.88 ± 8.16). Forty-one percent of the sample met criteria for having experienced at least one major depressive episode (MDE) in their life (n = 50) and 17% (n =21) had a history of multiple MDEs. These rates are consistent with findings from several rigorous longitudinal studies of depression including the Oregon Adolescent Depression Project, which assessed for incidence of a major depressive episode up to age 30 (51% of sample; Rohde, Lewinsohn, Klein, Seeley, & Gau, 2012) and the Dunedin Study, measuring incidence up to age 32 (41% of sample; Moffitt et al., 2010).
Momentary Ruminative Self-Focus Analyses
Experiencing a stressor at a given alert significantly predicted increases in next alert depressive symptoms, controlling for previous alert depressive symptoms (B = .47, p < .01; Table 2); experiencing a greater overall proportion of stressors during the EMA week (aggregated stress) also significantly predicted increases in depressive symptoms over time (B = 3.24, p < .001). The effects of both alert-level fluctuations in ruminative self-focus (MRSI-A) relative to an individual’s mean, as well as average levels of MRSI-A during the EMA week (aggregated MRSI-A) were not significant in predicting increases in depressive symptoms (Bs < .09, ps > .10). Ruminative self-focus significantly interacted with concurrent depressive symptoms to predict increases in depressive symptoms at the next timepoint (B = .01, p < .05).
Table 2.
MRSI-A by Stress Interaction Predicting Next Alert Depressive Symptoms
| Predictor | B | SE |
|---|---|---|
| Alert-Level | ||
| Lagged depressive symptoms (TA−1 SDS) | .14*** | .02 |
| Stress | .47** | .16 |
| Ruminative self-focus (MRSI-A)a | −.02 | .03 |
| Stress X MRSI-A | .10* | .05 |
| Individual-Level | ||
| Intercept | 5.02*** | .21 |
| Aggregated Stressb | 3.24*** | .82 |
| Aggregated MRSI-Ab | .09 | .06 |
| T1 depressive symptoms (BDI-II)b | .07** | .02 |
| T1 rumination (SRRS)b | .02* | .01 |
Note. Analyses include 2,530 alerts. SDS= State Depression Scale, Stress = occurrence of negative life events per alert, dummy-coded, MRSI-A = Momentary Ruminative Self-Focus Inventory-Abbreviated, BDI-II = Beck Depression Inventory-II, SRRS = Stress-Reactive Rumination Scale.
p < .05,
p< .01,
p<.001
= grand-mean centered
= person-mean centered
There was a significant positive interaction between stress and MRSI-A in predicting increases in depressive symptoms at the next alert, controlling for previous alert symptoms (B = .10, p < .05; Table 2), such that engaging in high levels of momentary ruminative self-focus relative to one’s mean at alerts in which a stressor was reported led to significantly greater increases in depressive symptoms at subsequent alerts compared to alerts at which rumination was high but no stressor was endorsed (conditional effect = .77, p < .01; Figure 1). When MRSI-A levels were low relative to individuals’ means, the presence or absence of a stressor did not significantly influence the prediction of subsequent depressive symptoms (conditional effect = .18, p > .10). There also was a significant effect such that, the experience of stress coupled with higher than average MRSI-A levels predicted significantly greater increases in depressive symptoms at subsequent alerts compared to alerts at which a stressor was reported but MRSI-A was low (conditional effect = .08, p < .05). Conversely, differences in relative level of MRSI-A did not significantly affect subsequent depressive symptoms when no stressor was reported (conditional effect = −.02, p > .10). This stress by MRSI-A interaction was significant despite controlling for the independent effect of stress at the alert level and at the aggregated individual level, as well as T1 BDI-II and SRRS scores, all of which also significantly predicted change in depressive symptoms over time.
Figure 1.
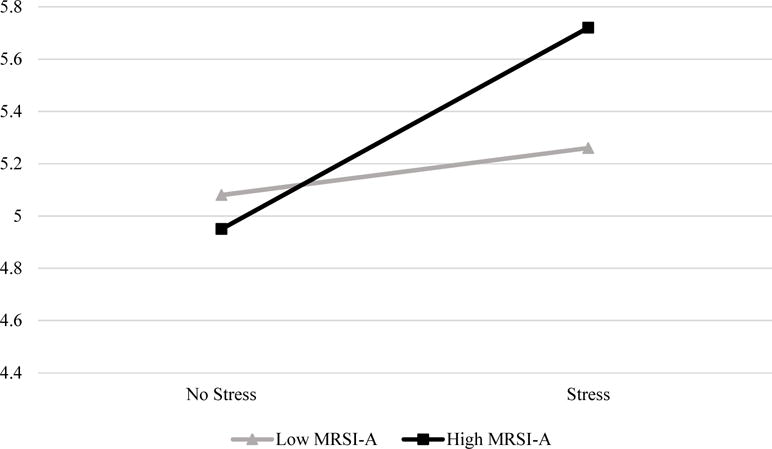
MRSI-A by Stress Interaction Predicting Next Alert Depressive Symptoms
Note. Analyses include 2,530 alerts. Stress= occurrence of any negative life events at a given alert, dummy-coded; MRSI-A = Momentary Ruminative Self-Focus Inventory-Abbreviated; SDS = State Depression Scale. High and low MRSI values ± 1 SD from individual-level mean. Analyses controlled for previous alert depressive symptoms.
There were no significant cross-level interactions between Level 1 stress and trait measures of rumination (T1 SRRS or RRS-B) in predicting concurrent or subsequent depressive symptoms, controlling for previous alert depressive symptoms. As previous EMA research has found rumination to mediate the role of stress in predicting depressive symptoms (Moberly & Watkins, 2008a; Ruscio et al., 2015), the direct and indirect paths were tested for significance to determine if a mediational relationship also existed. Analyses found a significant direct effect of stress on next alert depressive symptoms, controlling for previous symptoms (B = .48, p < .01). Stress also significantly predicted MRSI-A score at the same alert (B = .42, p < .01). However, as reported above, MRSI-A did not significantly predict next alert depressive symptoms, and therefore MRSI-A was not found to mediate the relationship between stress and depressive symptoms.
Stress-Reactive Rumination Analyses
Experiencing greater relative levels of stress per day predicted significant increases in same day depressive symptoms, controlling for previous day symptoms (B = .69, p < .001; Table 3); experiencing a greater overall number of stressors during the EMA week (aggregated stress) also significantly predicted increases in symptoms over time (B = .74, p < .01). The effects of both daily fluctuations in stress-reactive rumination relative to an individual’s mean (SRRS-S; B = .07, p < .001), as well as average levels of SRRS-S during the EMA week (aggregated SRRS-S; B = .10, p < .001) were significant in predicting increases in daily depressive symptoms.
Table 3.
SRRS-S by Stress Interaction Predicting Same Day Depressive Symptoms
| Predictor | B | SE |
|---|---|---|
| Day-Level | ||
| Lagged depressive symptoms (TD−1 SDS) | .25*** | .04 |
| Stressa | .69*** | .12 |
| Rumination (SRRS-S)a | .07*** | .01 |
| Stress X SRRS-S | .04* | .02 |
| Individual-Level | ||
| Intercept | 4.72*** | .31 |
| Aggregated Stressb | .74** | .24 |
| Aggregated SRRS-Sb | .10*** | .02 |
| T1 depressive symptoms (BDI-II)b | .08** | .02 |
| T1 rumination (SRRS)b | .00 | .01 |
Note. Analyses included 505 days. SDS= State Depression Scale, Stress = total negative life events endorsed per day, SRRS-S = Stress-Reactive Rumination Scale-State, BDI-II = Beck Depression Inventory-II, SRRS = Stress-Reactive Rumination Scale.
p < .05,
p< .01,
p<.001
= grand-mean centered
= person-mean centered
There was a significant interaction between SRR and stress in predicting depressive symptoms on the same day controlling for previous day depressive symptoms (B = .04, p < .05; Table 3), such that engaging in high levels of SRR relative to one’s mean led to significantly greater increases in depressive symptoms on days when more stressors were reported (conditional effect = .97, p < .001; Figure 2). Increases in daily stress also predicted greater depressive symptoms even when relative SRR levels were low (conditional effect = .40, p < .05). Furthermore, there was a significant effect such that higher daily stress coupled with higher than average SRR levels predicted significantly greater increases in depressive symptoms compared to high stress days (days where greater numbers of stressors were reported) when SRR levels were low (conditional effect = .10, p < .001). Conversely, differences in relative level of SRR did not significantly affect depressive symptoms on low stress days (conditional effect = −.03, p > .10). This interaction was significant when controlling for the independent effects of stress and SRRS-S at the day level and at the aggregated individual level, as well as T1 BDI-II score, all of which significantly predicted increases in daily depressive symptoms.
Figure 2.
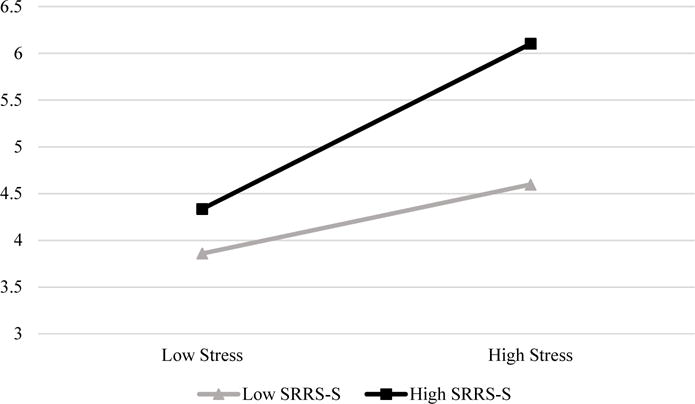
SRRS-S by Stress Interaction Predicting Same Day Depressive Symptoms
Note. Analyses include 505 days. Stress = total negative life events endorsed per day; SRRS-S = Stress-Reactive Rumination Scale-State; SDS = State Depression Scale. High and low values ± 1 SD from individual-level means. Analyses controlled for previous day depressive symptoms.
Mediation analyses found a significant direct effect of stress on same day depressive symptoms, controlling for previous day symptoms (B = .82, p < .001). As reported above, SRR score did significantly predict same day depressive symptoms controlling for previous symptoms. However, stress did not significantly predict same day SRR score (B = −.31, p > .10), and therefore, SRR was not found to mediate the relationship between stress and depressive symptoms.
The interaction between stress and SRRS-S was not significant in predicting depressive symptoms on the subsequent day controlling for previous day depressive symptoms (B = .01, p > .10). With regards to mediation, stressor occurrence was not found to predict next day depressive symptoms controlling for previous symptoms (B = −.08, p > .10), precluding further tests of mediating effects.
Discussion
The current study sought to investigate the role of rumination, both independently and in interaction with stress and current mood state, in predicting relative increases in depressive symptoms utilizing EMA methodology. It was hypothesized that increases in momentary ruminative self-focus (MRS) irrespective of the experience of life stressors, as well as stress-reactive rumination (SRR), would exert independent effects in predicting heightened depressive symptoms over time, and that ruminative self-focus would interact with concurrent depressed mood state to predict increases in symptoms at the subsequent alert. It was further hypothesized that both MRS and SRR would moderate the effect of stress in predicting increases in depressive symptoms. Finally, in line with response styles theory, baseline trait measures of rumination also were expected to interact with the experience of stressors to increase depressive symptoms over time.
The present findings emphasize an important interplay between rumination and stress in contributing to depressed mood. Contrary to hypotheses, MRS did not independently predict increases in depressive symptoms at the next alert, controlling for previous alert symptoms; however, as expected, a positive effect of MRS did emerge in interaction with the experience of stress. In other words, engaging in greater MRS led to higher subsequent depressive symptoms when it occurred at an EMA alert in which a stressor was reported. Furthermore, when individuals engaged in higher levels of MRS relative to their means in response to a stressor, they experienced greater prospective increases in depressive symptoms compared to alerts at which they engaged in lower relative levels of MRS in response to stress. In addition, MRS interacted with concurrent depressive symptoms to predict subsequent increases in symptoms, in accordance with the established deleterious effects of ruminating about one’s down mood (Wisco & Nolen-Hoeksema, 2008). These findings suggest that engaging in introspective thought about one’s feelings is not inherently detrimental, but that MRS becomes maladaptive when occurring following recent stress, or when currently experiencing depressed mood.
Current findings with regards to stress-reactive rumination were in line with hypotheses. Engaging in greater SRR, whether relative to one’s own mean at the alert level or relative to the grand mean at the individual level, exerted a significant independent effect in predicting increases in daily depressive symptoms, controlling for previous day symptoms. SRR also significantly moderated the effect of stress in predicting depressive symptoms. The nature of this interaction was similar to that described with regards to MRS, in that 1) higher levels of SRR relative to an individual’s mean predicted greater depressive symptoms on days when participants reported higher than average numbers of stressors, compared to low stress days, and 2) depressive symptoms were greater on high stress days when participants engaged in more SRR, compared to high stress days during which they did not ruminate as much.
No significant interactions were observed between baseline trait measures of rumination and stressor occurrence during the EMA week in predicting depressive symptoms, in contrast to predictions based on response styles theory (Nolen-Hoeksema, 1991) and previous EMA findings (Moberly & Watkins, 2008a). However, the abovementioned significant interactions between state-level MRS and SRR scores and stress certainly could be viewed as consistent with response styles theory. Although these interactions involved state measures of rumination, these variables were moderately correlated with baseline trait rumination measures (SRRS and RRS-B), suggesting that they may be measuring a separate but closely related facet of ruminative thought. Indeed, such state variables may serve as more accurate measures of individuals’ average cognitive responses to stress compared to trait questionnaires.
To our knowledge, the current study is the first to demonstrate significant positive interactions between rumination and life stress in prospectively predicting depressive symptoms utilizing an EMA design. Whereas previous EMA studies have found rumination to mediate the role of stress in predicting depressed mood (Moberly & Watkins, 2008a; Ruscio et al., 2015), the current work suggests that instead of serving to explain the detrimental effects of stressor occurrence on mood, variability in rumination can indeed change the magnitude of stressor effects, by increasing the potency of life stress as a vulnerability factor for depression. Our results complement findings from a daily diary study of SRR, life stress, and depressive symptoms (Genet & Siemer, 2012), and extend this work by utilizing an EMA design in which variables of interest were measured multiple times per day to increase validity.
Differences in study design and analysis plan may in part account for the lack of an observed mediating effect within the current research as opposed to the abovementioned EMA paradigms. Given that Moberly and Watkins did not control for previous depressive symptoms in their analyses, and Ruscio et al.’s effect lost significance when doing so, these previously reported results are not directly comparable to the current design. This difference in control strategy notwithstanding, it is possible that issues of power may also have contributed to differing results. While the current study included a maximum of 28 observations per participant, the two abovementioned designs involved up to 56 timepoints, which may have influenced the ability to detect a mediating effect.
The current design was strengthened by its assessment of both momentary ruminative self-focus and stress-reactive rumination, utilizing multiple items from validated measures of these constructs, the MRSI and SRRS, neither of which have yet been examined using EMA methodology. By assessing these subtypes of rumination, the differential effects of MRS and SRR were able to be parsed apart; namely, that whereas SRR independently predicted increases in depressive symptoms, engaging in MRS increased symptoms when in response to a stressor or when currently experiencing depressed mood. Although previous research has found that engaging in MRS while at rest is predictive of increases in depressive symptoms (Marchetti et al., 2013), it should be noted that this effect only held among individuals scoring high on a trait measure of cognitive reactivity2. Instead, the current findings demonstrate that engaging in more MRS, whether relative to one’s own mean or relative to the mean of the sample, does not lead to increases in depressive symptomatology when considered independent of stress or down mood. Interestingly, although not a significant effect, the lowest levels of depressive symptoms were seen following alerts at which individuals experienced no stressors but engaged in higher than average MRS (Figure 1), suggesting that focusing on one’s feelings in the absence of a proximal stressor may have beneficial effects on mood. Although such conclusions cannot be drawn from the current findings, the results highlight a potential avenue of future research.
The current findings are strengthened by the study’s analytic strategy. Alert-level rumination variables were centered on individual means in order to assess the effect of relative fluctuations in rumination during the EMA week on depressive symptoms. Analyses also controlled for aggregated alert-level variables at the individual level; this control strategy accounted for overall differences in rumination and stress during the EMA week, to better examine the role of alert-level variation in the prediction of depressive symptoms within each participant. Furthermore, all analyses controlled for previous depressive symptoms, whether at the previous alert or day, in order to truly assess whether depressive symptoms changed over time due to the occurrence of rumination or stress. Past studies either did not control for previous symptoms (Genet & Siemer, 2012; Moberly & Watkins, 2008a; Takano & Tanno, 2010) or their effects were no longer significant when doing so (Ruscio et al., 2015), leading the current findings to serve as the first prospective evidence that rumination, in combination with life stress, increases depressive symptoms over time.
The use of EMA methodology lends multiple strengths to the current findings. Collecting data at several timepoints per day helped to lessen recall biases and increase reliability of the variables of interest. Furthermore, the findings were specific to participants’ actual experience of daily life stressors and rumination occurring outside of a controlled laboratory setting, and captured the effects of relative fluctuations in these levels over time. By utilizing online questionnaires sent to participants’ smartphones that were timestamped upon completion, there was increased confidence that participants were completing EMA alerts within assigned time windows. Furthermore, allowing participants to choose the 12-hour window during which they received alerts maximized the percentage of waking hours assessed and likely benefited overall response rates.
Limitations also should be noted. Although the current EMA design helped decrease the incidence of recall biases, there still exists the possibility of such occurrence, given that participants were asked to retrospectively report on life stress and their degree of SRR since the last alert. However, because the time interval between alerts was only hours rather than days, weeks, or months, recall biases would be expected to be minor compared to non-EMA studies of rumination, stress, and depression. As explained earlier, SRR analyses were conducted by calculating daily averages to allow for variation in life event occurrence, which decreased the number of available data points. In addition, the interaction of SRR and stress was only significant predicting same day, and not next day, depressive symptoms. Although SRR ratings referred to rumination at the time of event occurrence and depressive symptoms referred to mood at time of alert completion, indicating a temporal difference in the variables of interest, our results would have been further strengthened if the interaction term predicted next day symptoms. Although the SADS-L diagnostic measure employed in this study has demonstrated acceptable interrater reliability in previous examinations, this statistic was not calculated within the current design and is therefore a limitation to the research. Finally, despite the wide range of depression scores reported among the current participants, the sample was nonclinical in nature. Assessing such relationships within a clinically depressed sample is an important and much-needed extension of the current work.
The results from this study may have important clinical implications. Specifically, findings of significant interactions between rumination and life stress suggest that ruminative thought is not merely a by-product of experiencing stress, but is instead a response style that exhibits variation both within and between individuals, such that engaging in relatively higher levels leads to greater increases in depressive symptoms. Therefore, it would be important to address individuals’ tendency to engage in rumination directly after the experience of stress, such that decreasing relative levels could potentially reduce the deleterious effects of stressor occurrence on mood. Indeed, trainings intended to decrease levels of abstract, repetitive thought regarding negative information have demonstrated promising preliminary results (Joormann, Hertel, LeMoult, & Gotlib, 2009; Watkins, Baeyens, & Read, 2009). Such designs could benefit from the integration of EMA methodology; for instance, depressed individuals could engage in trainings intended to reduce rumination directly after the experience of stress, after which EMA techniques could monitor relative changes in rumination and depressive symptoms following stressor occurrence during daily functioning. Indeed, EMA is increasingly being employed to track longer-term outcomes following active interventions (Hoorelbeke, Koster, Demeyer, Loeys, & Vanderhasselt, 2016).
The current research sheds light on the role of rumination in response to daily life stressors as a contributor to depressed mood over time. The findings of significant interactions between MRS, SRR and stress suggest that the degree of rumination engaged in following the experience of stress is variable and can lead to greater increases in depressive symptoms when occurring at higher levels relative to individual means. These results have significant clinical implications in that they emphasize the importance of targeting individuals’ momentary response styles to stress in order to help decrease depressive symptoms over time. Future research should continue to capitalize on the many benefits of EMA methodology in order to better understand this relationship and lessen the substantial burden of major depressive disorder.
Rumination interacted with daily stress to predict increased depressive symptoms
First study to find a moderating effect of rumination utilizing EMA methodology
Decreasing rumination following stress may help alleviate depressed mood
Acknowledgments
We are grateful to Angelique Frazier and Matthew Goodman for their significant contributions during the data collection and entry stages, and to Dr. Thomas Olino for his statistical consultation. This work was supported by the National Institute of Mental Health [NIMH NRSA F31 grant 1F31MH106181], the APAGS Scott Mesh Honorary Grant for Research in Psychology, and the APF/COGDOP Charles and Carol Spielberger Scholarship awarded to Samantha Connolly. Lauren Alloy was supported by NIMH R01 grant MH101168.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
These analyses were not also run predicting depressive symptoms at the concurrent alert (TA SDS), given that MRSI-A and SDS scores measured rumination and depressive symptoms occurring at the same time, precluding tests of causality.
Follow-up analyses tested whether significant interactions existed between trait-level rumination (SRRS, RRS-B) at baseline and MRSI scores during the EMA week in predicting depressive symptoms; no significant relationships emerged.
References
- Abramson LY, Alloy LB, Hankin BL, et al. Cognitive vulnerability-stress models of depression in a self-regulatory and psychobiological context. In: Gotlib IH, Hammen CL, editors. Handbook of Depression. New York: Guilford Press; 2002. [Google Scholar]
- Alloy LB, Abramson LY, Hogan ME, Whitehouse WG, Rose DT, Robinson MS, Lapkin JB. The Temple-Wisconsin cognitive vulnerability to depression project: Lifetime history of axis I psychopathology in individuals at high and low cognitive risk for depression. Journal of Abnormal Psychology. 2000;109(3):403–418. [PubMed] [Google Scholar]
- Alloy LB, Bender RE, Whitehouse WG, Wagner CA, Liu RT, Grant DA, Abramson LY. High behavioral approach system (BAS) sensitivity, reward responsiveness, and goal-striving predict first onset of bipolar spectrum disorders: A prospective behavioral high-risk design. Journal of Abnormal Psychology. 2012;121:339–351. doi: 10.1037/a0025877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th. Washington, DC: Author; 2000. text rev. [Google Scholar]
- Armey MF, Schatten HT, Haradhvala N, Miller IW. Ecological momentary assessment (EMA) of depression-related phenomena. Current Opinion in Psychology. 2015;4:21–25. doi: 10.1016/j.copsyc.2015.01.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic and statistical considerations. Journal of Personality and Social Psychology. 1986;51:1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory-II. San Antonio, TX: Psychological Corporation; 1996. [Google Scholar]
- Birnbaum HG, Kessler RC, Kelley D, Ben-Hamadi R, Joish VN, Greenberg PE. Employer burden of mild, moderate, and severe major depressive disorder: Mental health services utilization and costs, and work performance. Depression and Anxiety. 2010;27(1):78–89. doi: 10.1002/da.20580. [DOI] [PubMed] [Google Scholar]
- Dozois DJ, Dobson KS, Ahnberg JL. A psychometric evaluation of the Beck Depression Inventory-II. Psychological Assessment. 1998;10(2):83–89. [Google Scholar]
- Endicott J, Spitzer RA. A diagnostic interview: The Schedule for Affective Disorders and Schizophrenia. Archives of General Psychiatry. 1978;35:837–844. doi: 10.1001/archpsyc.1978.01770310043002. [DOI] [PubMed] [Google Scholar]
- Feldner MT, Leen-Feldner EW, Zvolensky MJ, Lejuez CW. Examining the association between rumination, negative affectivity, and negative affect induced by a paced auditory serial addition task. Journal of Behavior Therapy and Experimental Psychiatry. 2006;37(3):171–187. doi: 10.1016/j.jbtep.2005.06.002. [DOI] [PubMed] [Google Scholar]
- Genet JJ, Siemer M. Rumination moderates the effects of daily events on negative mood: results from a diary study. Emotion (Washington, DC) 2012;12(6):1329–39. doi: 10.1037/a0028070. [DOI] [PubMed] [Google Scholar]
- Hammen C. Stress and depression. Annual Review of Clinical Psychology. 2005;1(1):293–319. doi: 10.1146/annurev.clinpsy.1.102803.143938. [DOI] [PubMed] [Google Scholar]
- Hoorelbeke K, Koster EH, Demeyer I, Loeys T, Vanderhasselt MA. Effects of cognitive control training on the dynamics of (mal) adaptive emotion regulation in daily life. Emotion (Washington, DC) 2016;16(7):945–956. doi: 10.1037/emo0000169. [DOI] [PubMed] [Google Scholar]
- Joormann J, Hertel P, LeMoult J, Gotlib IH. Training intentional forgetting of negative material in depression. Journal of Abnormal Psychology. 2009;118:34–43. doi: 10.1037/a0013794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kessler RC, Merikangas KR, Wang PS. Prevalence, comorbidity, and service utilization for mood disorders in the United States at the beginning of the twenty-first century. Annual Review of Clinical Psychology. 2007:3137–158. doi: 10.1146/annurev.clinpsy.3.022806.091444. [DOI] [PubMed] [Google Scholar]
- Marchetti I, Koster E, De Raedt R. Rest-related dynamics of risk and protective factors for depression: A behavioral study. Clinical Psychological Science. 2013;1(4):443–451. [Google Scholar]
- Moberly NJ, Watkins ER. Ruminative self-focus, negative life events, and negative affect. Behaviour Research and Therapy. 2008a;46(9):1034–1039. doi: 10.1016/j.brat.2008.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moberly NJ, Watkins ER. Ruminative self-focus and negative affect: an experience sampling study. Journal of Abnormal Psychology. 2008b;117(2):314–23. doi: 10.1037/0021-843X.117.2.314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mor N, Marchetti I, Koster EHW. The Momentary Ruminative Self-focus Inventory (MRSI): Validation and Psychometric Evaluation. Manuscript submitted for publication 2013 [Google Scholar]
- Nolen-Hoeksema S. Responses to depression and their effects on the duration of depressive episodes. Journal of Abnormal Psychology. 1991;100(4):569–582. doi: 10.1037//0021-843x.100.4.569. [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S, Morrow J. A prospective study of depression and posttraumatic stress symptoms after a natural disaster: The 1989 Loma Prieta earthquake. Journal of Personality and Social Psychology. 1991;61(1):115–121. doi: 10.1037//0022-3514.61.1.115. [DOI] [PubMed] [Google Scholar]
- Ottaviani C, Medea B, Lonigro A, Tarvainen M, Couyoumdjian A. Cognitive rigidity is mirrored by autonomic inflexibility in daily life perseverative cognition. Biological Psychology. 2015;107:24–30. doi: 10.1016/j.biopsycho.2015.02.011. [DOI] [PubMed] [Google Scholar]
- Preacher KJ, Curran PJ, Bauer DJ. Simple intercepts, simple slopes, and regions of significance in HLM 2-way interactions. 2003 Retrieved from http://www.quantpsy.org/interact/hlm2.htm.
- Raudenbush SW, Bryk AS, Cheong YF, Congdon RT, du Toit M. HLM 7: Hierarchical linear and nonlinear modeling. Chicago, IL: Scientific Software International; 2011. [Google Scholar]
- Robinson MS, Alloy LB. Negative cognitive styles and stress-reactive rumination interact to predict depression: A prospective study. Cognitive Therapy and Research. 2003;27(3):275–291. [Google Scholar]
- Ruscio AM, Gentes EL, Jones JD, Hallion LS, Coleman ES, Swendsen J. Rumination predicts heightened responding to stressful life events in major depressive disorder and generalized anxiety disorder. Journal of Abnormal Psychology. 2015;124(1):17–26. doi: 10.1037/abn0000025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shiffman S, Stone AA, Hufford MR. Ecological Momentary Assessment. Annual Review of Clinical Psychology. 2008;4(1):1–32. doi: 10.1146/annurev.clinpsy.3.022806.091415. [DOI] [PubMed] [Google Scholar]
- Siegle GJ, Moore PM, Thase ME. Rumination: One construct, many features in healthy individuals, depressed individuals, and individuals with lupus. Cognitive Therapy and Research. 2004;28(5):645–668. [Google Scholar]
- Stone AA, Schwartz JE, Neale JM, Shiffman S, Marco CA, Hickcox M, Cruise LJ. A comparison of coping assessed by ecological momentary assessment and retrospective recall. Journal of Personality and Social Psychology. 1998;74(6):1670–1680. doi: 10.1037//0022-3514.74.6.1670. [DOI] [PubMed] [Google Scholar]
- Storch EA, Roberti JW, Roth DA. Factor structure, concurrent validity, and internal consistency of the Beck Depression Inventory-Second Edition in a sample of college students. Depression and Anxiety. 2004;19(3):187–9. doi: 10.1002/da.20002. [DOI] [PubMed] [Google Scholar]
- Takano K, Tanno Y. Concreteness of thinking and self-focus. Consciousness and Cognition. 2010;19(1):419–425. doi: 10.1016/j.concog.2009.11.010. [DOI] [PubMed] [Google Scholar]
- Takano K, Tanno Y. Diurnal variation in rumination. Emotion. 2011;11(5):1046–1058. doi: 10.1037/a0022757. [DOI] [PubMed] [Google Scholar]
- Treynor W, Gonzalez R, Nolen-Hoeksema S. Rumination Reconsidered: A Psychometric Analysis. Cognitive Therapy and Research. 2003;27(3):247–259. [Google Scholar]
- Watkins ER, Baeyens CB, Read R. Concreteness training reduces dysphoria: Proof-of-principle for repeated cognitive bias modification in depression. Journal of Abnormal Psychology. 2009;118(1):55–64. doi: 10.1037/a0013642. [DOI] [PubMed] [Google Scholar]
- Watkins E, Moberly NJ, Moulds ML. Processing mode causally influences emotional reactivity: Distinct effects of abstract versus concrete construal on emotional response. Emotion. 2008;8(3):364–378. doi: 10.1037/1528-3542.8.3.364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wenze SJ, Miller IW. Use of ecological momentary assessment in mood disorders research. Clinical Psychology Review. 2010;30(6):794–804. doi: 10.1016/j.cpr.2010.06.007. [DOI] [PubMed] [Google Scholar]
- Wisco BE, Nolen-Hoeksema S. Ruminative response style. In: Dobson KS, Dozois DA, editors. Risk factors in depression. San Diego, CA US: Elsevier Academic Press; 2008. pp. 221–236. [Google Scholar]