

Abstract
Purpose:
Soft liners act as a cushion between the denture base and the residual ridge. Hence, it is important to study their effect on resorption of mandibular denture bearing area. Therefore, the purpose of this study was to evaluate the influence of soft denture liner on mandibular ridge resorption after 1 year in completely denture wearers.
Materials and Methods:
Twenty-eight completely edentulous patients having age between 45 and 60 years with well-formed ridges in class I jaw relations were selected as per the inclusion and exclusion criterion. Randomization chart was used to enroll participants in experimental and control groups who were given mandibular dentures with and without soft denture liner, respectively. Vertical measurements were made on orthopantomograph and analyzed using Adobe Photoshop 7.0 software at five points, i.e., one at central incisor and two points at right and left first premolars and two in each first molar region.
Results:
On application of repeated measures analysis of variance, both groups showed a significant change in bone height after denture delivery (P < 0.05). Intergroup comparison (Wilcoxon rank sum test) of bone height in different regions at various time intervals showed statistically significant difference in bone levels (P < 0.05) from baseline to 6 months and baseline to 12months (P < 0.01), while the difference was statistically not significant during 6 and 12 months’ period.
Conclusion:
The use of soft denture liner significantly reduces the residual ridge resorption in complete denture wearers as compared to conventional denture wearers (without denture liner) over a period of 1 year.
Keywords: Complete denture, edentulous ridge, residual ridge resorption, soft liner
INTRODUCTION
Residual ridge resorption is a chronic, progressive, irreversible, and disabling disease, and it has probably multifactorial origin.[1] Bone loss varies from patient to patient, but more significant changes occur in the mandibular arch. Tallgren[2] and Atwood and Coy[3] found that the mean ratio of anterior maxillary to anterior mandibular (residual ridge reduction [RRR]) was 1:4. This is because mandibular ridge bears higher functional forces transmitted through the dentures than the maxillary ridge because of its smaller area and less advantageous shape of the lower basal seat.[4]
Residual ridge resorption, especially in the mandible, may affect denture stability and retention.[5,6] Gross resorption of the edentulous mandibular alveolar process over a period of time resulting in excessive loss of the denture bearing ridge and mostly the overlying thin and atrophic mucosa over it makes it more difficult to withstand the masticatory load.[7,8] The mucosa gets impinged between the sharp ridge and the denture resulting in severe pain and discomfort to the patient.[8]
The difficulties encountered in such patients during function can be reduced with the use of either implants or resilient denture liners.[5,6,9] Although implants have been reported as highly effective,[10] they are not a viable solution for all edentulous patients because of unfavorable underlying bone, relevant medical, psychological, and financial constraints.[11] On the other hand, treatment with the resilient denture liners has only few limitations, being the nonsurgical application procedure, and have low treatment cost. The flexibility, resiliency, and the shock absorbency of the resilient denture liner materials help in impact reduction and distribution of masticatory load to the ridge.[12,13,14,15]
The use of soft liners became popular in dentistry because they have many clinical advantages. These materials have the ability to help in healing of the inflamed mucosa,[16,17,18] distribute the functional load in the support area of the prostheses[19,20] and improve their adaptation and retention.[21] According to the literature, due to cushioning effect provided by soft liners, lesser amount of forces are transferred to the underlying bone during various functions as compared to one without soft liners.[13,14,15,22] This leads to a reduction in residual ridge resorption. Although the idea of the resilient liners was introduced several years ago, most of the studies were either laboratory[22] or clinical observations for their efficacy. As intraoral environment is the most precise testing, clinical studies are a must to draw definitive conclusions.[23] Currently, the literature is scanty regarding the evidence of effect resilient liners on residual ridge resorption in complete denture wearers. Therefore, this study was designed to evaluate the effect of soft denture liners on the mandibular ridge resorption in complete denture wearers till 1 year of their application.
MATERIALS AND METHODS
This clinical study was carried out in the Department of Prosthodontics, CDER, All India Institute of Medical Sciences, New Delhi after approval from institutional ethics committee (IESC/T-255/01.06.2012). A total number of 28 completely edentulous patients within the age group of 45–60 years following the inclusion criteria; edentulous patients for the last 6 months, having class I jaw relation, well-developed ridges with firm mucosa and no previous denture experience were selected to participate in the study. Patient suffering with any systemic disorder which may influence bone metabolism and having class II or class III jaw relationship were excluded. Participants were thoroughly informed about the whole procedure, need of follow-up visits, radiographs required, and written informed consent was obtained.
The sample size was calculated based on literature review[24] as two groups, parallel, repeated measures with resorption as the primary outcome variable measured at 6 months’ and 12 months’ postdenture insertion. Keeping in mind the possibility to have dropouts and to achieve 90% power with detectable difference at 95% confidence interval, 14 participants were enrolled in each of the two groups as per stratified (male/female) block randomization which was based on computer-generated numbers given by the statistician.
For participants in experimental group (n = 14, 7 males and 7 females), maxillary dentures were fabricated in heat cured acrylic resin (Travelon, Dentsply India, Mumbai, India) while mandibular denture was lined with heat cured acrylic denture soft liner (Permasoft, Dentsply International, West Philadelphia Street York, PA, USA) at the time of packing. Participants in control group (n = 14, 7 males and 7 females) were provided with conventional maxillary and mandibular complete dentures fabricated in heat cured acrylic resin (without soft liner) [Figure 1]. Bilateral balanced occlusal scheme was given in all the participants. The radiopaque markers were placed over the tooth surfaces in mandibular dentures after dewaxing at five different points (one in central incisor region and one in 1st premolar and 1st molar region on both sides) and secured in position with glue. Then the mold was packed in heat cured acrylic resin. Besides this, in experimental group, wax spacer of uniform two mm thickness was adapted over the mandibular cast and the remaining space was packed with heat cured acrylic resin. Wax spacer was replaced after trial closure with heat cured acrylic soft denture liner and denture was cured using the standard procedure. After processing, dentures were remounted for occlusal adjustment. Following this, dentures were finished, polished, and delivered to the participants.
Figure 1.
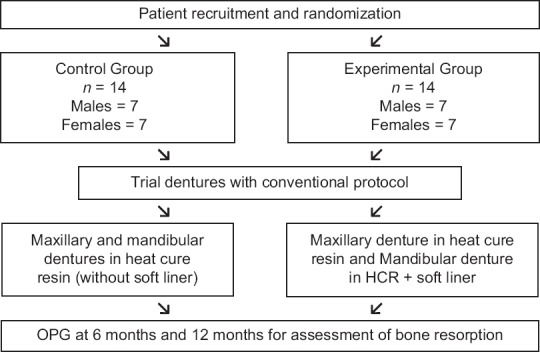
Flow chart of methodology
For each participant, three panoramic radiographs (orthopantomogram [OPG]) were taken to assess the amount of bone resorption; immediately, at 6 months and at 12 months after denture insertion.
To assure the reproducibility between successive films, all the radiographs were taken on same machine (OPG machine details) by a trained radiographer using standard protocol and blinded about the use of soft denture liner. For the measurements, a reference plane was drawn touching the inferior border of the mandible. On this line, 90° tangents were drawn from the lower border of the radiopaque markers in five different regions; 2 in 1st premolar, 2 in 1st molar, and 1 in midline [Figure 2]. The distances from the radiopaque markers to the reference plane were measured with the help of Adobe Photoshop 7.0 (Adobe Systems, San Jose, CA, USA). All the measurements were performed by two independent and blinded examiners to minimize the operator-based bias and error. In case of different values, measurements were verified again.
Figure 2.
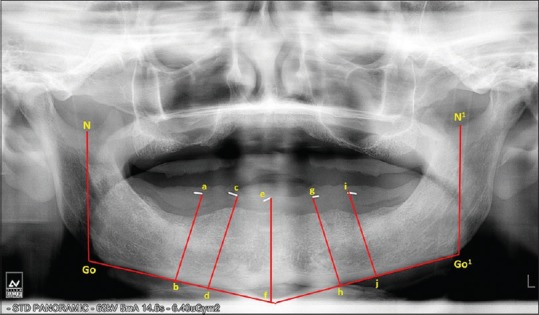
Orthopantomogram showing the measurement of bone height from the radiopaque marker to the reference point at the base of the mandible. Go and Go1 = mandibular right and left gonion, N and N1 = right and left mandibular notch, N-Go and N1-Go1 = fixed reference line, a, c, e, g, i = radiopaque markers
The magnification error for each participant was corrected by measuring the distance from the mandibular notch to the gonion on each radiograph. Measurements recorded immediately after denture insertions were considered as baseline values, and measurements made at 6 months and 12 months were adjusted according to the baseline radiograph.
The following equation represents an example of correction factor:
The values on each side were multiplied by the correction factor. To avoid any horizontal error, right and left sides of mandible were treated as separate and multiplied with respective factors.[24]
The data were analyzed using Statistical Package for Social Sciences (version 19, IBM, Chicago, IL, USA). Quantitative variables were assessed for approximate normality and summarized by mean and standard deviation. Wilcoxon rank-sum test was used to compare nonparametric variables in between the two groups. Within group change in the quantitative variables was assessed by repeated measure two-way analysis of variance followed by post hoc with Bonferroni test. In this study, the confidence interval was set at 95% and P < 0.05 was considered as statistically significant.
RESULTS
A total of 28 (14 male/14 female) participants with mean age of 53.93 ± 4.25 years were rehabilitated with maxillary and mandibular complete dentures. The mean mandibular bone height from radiopaque markers at five different points in the right posterior, anterior and left posterior regions to a reference plane in mandible was measured in both groups over a period of 12 months [Table 1]. The mean change in bone height in right posterior, anterior and left posterior region in control group from baseline to 12 months was 1.4 ± 0.14 mm (4.9%), 1.4 ± 0.2 mm (5.2%), and 1.7 ± 0.05 mm (5.9%) respectively and in experimental group, this was 0.7 ± 0.08 mm (2.3%), 0.6 ± 0.06 mm (2.5%), and 0.9 ± 0.08 mm (3.2%), respectively. Results showed decrease in bone height at all time intervals in both groups, and the change was statistically significant (P < 0.05) [Table 2].
Table 1.
Mean mandibular bone level at five different points from base of the mandible up to the radio-opaque marker at different time intervals (n=14)

Table 2.
Comparison of mean bone level in different regions within the group at different time intervals

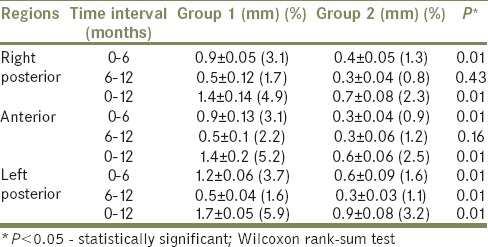
The comparison of bone height between the two groups in different regions at various time intervals showed significant difference in bone levels (P < 0.05) at baseline to 6 months and baseline to 12 months’ period (P < 0.01), while the difference for 6 and 12 months’ period was statistically not significant in right posterior (P = 0.43) and anterior region (P = 0.16) [Table 3].
Table 3.
Comparison of bone loss between the two groups in different regions at various time intervals
DISCUSSION
Resorption of the residual ridge has been estimated with various radiographic techniques such as lateral cephalometric and panoramic radiographs. Panoramic radiography is widely used because an image of both the jaws can be produced on one film with a relatively lesser radiation exposure, and is common in routine examinations, especially for edentulous patients before the construction of complete dentures.[25,26,27] Magnification is one of the major problems with panoramic radiography. Larheim and Svanaes[28] investigated the precision of measurements of mandibular linear dimensions in panoramic radiographs and found that the variability of vertical measurements made from repeated panoramic radiographs is small when patients are properly positioned in the panoramic apparatus. According to Xie et al.,[29] if reference lines and measured points are located in the same vertical plane or in approximately the same plane as the teeth, variations in vertical measurements in the mandible and maxilla are within a small range.
Enlow et al.[30] described the distribution of surface fields of resorption and deposition in all parts of the edentulous mandible and stated that residual ridge resorption is usually more rapid in the premolar and molar region than the anterior region of the mandible, due to the lower position of the reversal line in the posterior region. Hence, it is especially important to record the resorption in anterior and posterior region of the mandible. The results of this study revealed statistically significant rate of RRR at all five reference points of measurement in mandible in all the participants. After 6 months of denture delivery, the bone loss ranged from 0.3 to 1.2 mm as compared to that during 6–12-month period (0.3–0.5 mm) in both groups in all the regions. According to Tallgren[2] and Kovacic et al.,[31] RRR was greater during the first few months after the tooth extraction than later. According to Karaagaçlioglu and Ozkan,[32] duration of edentulousness is one of the most important factor in contributing to the severity of mandibular bone loss. Mandibular resorption rate was greatest in the earlier stages of edentulism and slowed with the longevity of edentulism.[33]
Participants in the experimental group showed 50% lesser bone loss in all the three regions compared to the control group over a period of 12 months. After 1 year period, bone loss in experimental group ranged from 0.3 to 0.9 mm and in control group were 0.5–1.7 mm. Similar results were obtained by Elcharkawi and elMahdy[24] when comparing the bone loss in mandible after 6 months of denture delivery with and without soft liners. Lesser resorption with soft liner may be due to equal distribution of stresses under the denture and lesser amount of force transmitted to underlying bone due to cushioning effect provided by viscoelastic property of soft liners.[13] Thus, the use of the resilient reliner material considerably minimized the stress in the alveolar bone and mucosa.[33,34,35] According to Lima et al.,[34] the thickness of the soft liner plays a significant role in the stress distribution especially in patient with thin mucosa, 2 mm thick soft liner relined denture shows lower stress distribution to bone as compared to denture with no soft liner or soft liner of variable thickness (0.5, 1, 1.5, 2.5 mm). Taguchi et al.[36] stated that acrylic resilient liner material showed a higher viscoelastic behavior than silicone material after applying the stress, and have the ability of stress distribution or stress relaxation.
Contrary to this study, Al-Noori and Said[37] found no significant difference in bone resorption with and without soft liner in complete denture patients. This may be due to difference in the study design, i.e., their subjects were edentulous at least 1 year before denture delivery as compared to the present study in which patients were edentulous for 6 months only.
The main limitation of this study is the short study period. Cushioning effect of soft liner decreases over time; so they have to be replaced repeatedly.[38] Further studies can be carried out to evaluate the effect of different types of soft liner materials on ridge resorption and relining of complete dentures for patients with compromised ridges.
CONCLUSION
The use of complete denture with soft denture liner significantly reduces the residual ridge resorption as compared to the one without denture liner. Although acrylic denture liner bonds chemically to denture base, only problem that arises is the longevity of the denture liner and its long-term maintenance. The risk-benefit ratio should be analyzed before the use of this material.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Atwood DA. Reduction of residual ridges: A major oral disease entity. J Prosthet Dent. 1971;26:266–79. doi: 10.1016/0022-3913(71)90069-2. [DOI] [PubMed] [Google Scholar]
- 2.Tallgren A. The continuing reduction of the residual alveolar ridges in complete denture wearers: A mixed-longitudinal study covering 25 years. J Prosthet Dent. 1972;27:120–32. doi: 10.1016/0022-3913(72)90188-6. [DOI] [PubMed] [Google Scholar]
- 3.Atwood DA, Coy WA. Clinical, cephalometric, and densitometric study of reduction of residual ridges. J Prosthet Dent. 1971;26:280–95. doi: 10.1016/0022-3913(71)90070-9. [DOI] [PubMed] [Google Scholar]
- 4.Tallgren A. Alveolar bone loss in denture wearers as related to facial morphology. Acta Odontol Scand. 1970;28:251–70. doi: 10.3109/00016357009032033. [DOI] [PubMed] [Google Scholar]
- 5.Zarb GA, Schmitt A. The longitudinal clinical effectiveness of osseointegrated dental implants: The Toronto study. Part I: Surgical results. J Prosthet Dent. 1990;63:451–7. doi: 10.1016/0022-3913(90)90237-7. [DOI] [PubMed] [Google Scholar]
- 6.Zarb GA, Schmitt A. The longitudinal clinical effectiveness of osseointegrated dental implants: The Toronto study. Part III: Problems and complications encountered. J Prosthet Dent. 1990;64:185–94. doi: 10.1016/0022-3913(90)90177-e. [DOI] [PubMed] [Google Scholar]
- 7.Reich KM, Huber CD, Lippnig WR, Ulm C, Watzek G, Tangl S. Atrophy of the residual alveolar ridge following tooth loss in an historical population. Oral Dis. 2011;17:33–44. doi: 10.1111/j.1601-0825.2010.01699.x. [DOI] [PubMed] [Google Scholar]
- 8.Meyer RA. Management of denture patients with sharp residual ridges. J Prosthet Dent. 1966;16:431–7. doi: 10.1016/0022-3913(66)90046-1. [DOI] [PubMed] [Google Scholar]
- 9.Zarb GA, Schmitt A. The longitudinal clinical effectiveness of osseointegrated dental implants: The Toronto Study. Part II: The prosthetic results. J Prosthet Dent. 1990;64:53–61. doi: 10.1016/0022-3913(90)90153-4. [DOI] [PubMed] [Google Scholar]
- 10.Feine JS, Carlsson GE, Awad MA, Chehade A, Duncan WJ, Gizani S, et al. The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Gerodontology. 2002;19:3–4. [PubMed] [Google Scholar]
- 11.Hayakawa I, Hirano S, Takahashi Y, Keh ES. Changes in the masticatory function of complete denture wearers after relining the mandibular denture with a soft denture liner. Int J Prosthodont. 2000;13:227–31. [PubMed] [Google Scholar]
- 12.Shim JS, Watts DC. An examination of the stress distribution in a soft-lined acrylic resin mandibular complete denture by finite element analysis. Int J Prosthodont. 2000;13:19–24. [PubMed] [Google Scholar]
- 13.Murata H, Haberham RC, Hamada T, Taguchi N. Setting and stress relaxation behavior of resilient denture liners. J Prosthet Dent. 1998;80:714–22. doi: 10.1016/s0022-3913(98)70060-5. [DOI] [PubMed] [Google Scholar]
- 14.Murata H, Taguchi N, Hamada T, Kawamura M, McCabe JF. Dynamic viscoelasticity of soft liners and masticatory function. J Dent Res. 2002;81:123–8. [PubMed] [Google Scholar]
- 15.Williamson RT. Clinical application of a soft denture liner: A case report. Quintessence Int. 1995;26:413–8. [PubMed] [Google Scholar]
- 16.Bates JF, Smith DC. Evaluation of indirect resilient liners for dentures: Laboratory and clinical tests. J Am Dent Assoc. 1965;70:344–53. doi: 10.14219/jada.archive.1965.0286. [DOI] [PubMed] [Google Scholar]
- 17.Goll G, Smith DE, Plein JB. The effect of denture cleansers on temporary soft liners. J Prosthet Dent. 1983;50:466–72. doi: 10.1016/0022-3913(83)90564-4. [DOI] [PubMed] [Google Scholar]
- 18.Nikawa H, Iwanaga H, Hamada T, Yuhta S. Effects of denture cleansers on direct soft denture lining materials. J Prosthet Dent. 1994;72:657–62. doi: 10.1016/0022-3913(94)90300-x. [DOI] [PubMed] [Google Scholar]
- 19.Sinobad D, Murphy WM, Huggett R, Brooks S. Bond strength and rupture properties of some soft denture liners. J Oral Rehabil. 1992;19:151–60. doi: 10.1111/j.1365-2842.1992.tb01093.x. [DOI] [PubMed] [Google Scholar]
- 20.Aydin AK, Terzioglu H, Akinay AE, Ulubayram K, Hasirci N. Bond strength and failure analysis of lining materials to denture resin. Dent Mater. 1999;15:211–8. doi: 10.1016/s0109-5641(99)00038-x. [DOI] [PubMed] [Google Scholar]
- 21.Eick JD, Craig RG, Peyton FA. Properties of resilient denture liners in simulated mouth conditions. J Prosthet Dent. 1962;12:1043–52. [Google Scholar]
- 22.Surapaneni H, Ariga P, Haribabu R, Ravi Shankar Y, Kumar VH, Attili S. Comparative evaluation of tensile bond strength between silicon soft liners and processed denture base resin conditioned by three modes of surface treatment: An in vitro study. J Indian Prosthodont Soc. 2013;13:274–80. doi: 10.1007/s13191-012-0235-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Rodrigues S, Shenoy V, Shetty T. Resilient liners: A review. J Indian Prosthodont Soc. 2013;13:155–64. doi: 10.1007/s13191-012-0143-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.elCharkawi HG, elMahdy AS. The effect of resilient layer and occlusal reactive complete dentures on the residual alveolar ridge. J Prosthet Dent. 1988;59:598–602. doi: 10.1016/0022-3913(88)90078-9. [DOI] [PubMed] [Google Scholar]
- 25.Xie Q, Wolf J, Ainamo A. Quantitative assessment of vertical heights of maxillary and mandibular bones in panoramic radiographs of elderly dentate and edentulous subjects. Acta Odontol Scand. 1997;55:155–61. doi: 10.3109/00016359709115409. [DOI] [PubMed] [Google Scholar]
- 26.Xie Q, Ainamo A, Tilvis R. Association of residual ridge resorption with systemic factors in home-living elderly subjects. Acta Odontol Scand. 1997;55:299–305. doi: 10.3109/00016359709114968. [DOI] [PubMed] [Google Scholar]
- 27.Saglam AA. The vertical heights of maxillary and mandibular bones in panoramic radiographs of dentate and edentulous subjects. Quintessence Int. 2002;33:433–8. [PubMed] [Google Scholar]
- 28.Larheim TA, Svanaes DB. Reproducibility of rotational panoramic radiography: Mandibular linear dimensions and angles. Am J Orthod Dentofacial Orthop. 1986;90:45–51. doi: 10.1016/0889-5406(86)90026-0. [DOI] [PubMed] [Google Scholar]
- 29.Xie Q, Soikkonen K, Wolf J, Mattila K, Gong M, Ainamo A. Effect of head positioning in panoramic radiography on vertical measurements: An in vitro study. Dentomaxillofac Radiol. 1996;25:61–6. doi: 10.1259/dmfr.25.2.9446974. [DOI] [PubMed] [Google Scholar]
- 30.Enlow DH, Bianco HJ, Eklund S. The remodeling of the edentulous mandible. J Prosthet Dent. 1976;36:685–93. doi: 10.1016/0022-3913(76)90035-4. [DOI] [PubMed] [Google Scholar]
- 31.Kovacic I, Celebic A, Zlataric DK, Petricevic N, Bukovic D, Bitanga P, et al. Decreasing of residual alveolar ridge height in complete denture wearers. A five year follow up study. Coll Antropol. 2010;34:1051–6. [PubMed] [Google Scholar]
- 32.Karaagaçlioglu L, Ozkan P. Changes in mandibular ridge height in relation to aging and length of edentulism period. Int J Prosthodont. 1994;7:368–71. [PubMed] [Google Scholar]
- 33.Parkinson CF. Similarities in resorption patterns of maxillary and mandibular ridges. J Prosthet Dent. 1978;39:598–602. doi: 10.1016/s0022-3913(78)80066-3. [DOI] [PubMed] [Google Scholar]
- 34.Lima JB, Orsi IA, Borie E, Lima JH, Noritomi PY. Analysis of stress on mucosa and basal bone underlying complete dentures with different reliner material thicknesses: A three-dimensional finite element study. J Oral Rehabil. 2013;40:767–73. doi: 10.1111/joor.12086. [DOI] [PubMed] [Google Scholar]
- 35.Kawano F, Ohguri T, Koran III A, Matsumoto N, Ichikawa T. Influence of lining design of three processed soft denture liners on cushioning effect. J Oral Rehabil. 1999;26:962–8. doi: 10.1046/j.1365-2842.1999.00467.x. [DOI] [PubMed] [Google Scholar]
- 36.Taguchi N, Murata H, Hamada T, Hong G. Effect of viscoelastic properties of resilient denture liners on pressures under dentures. J Oral Rehabil. 2001;28:1003–8. doi: 10.1046/j.1365-2842.2001.00770.x. [DOI] [PubMed] [Google Scholar]
- 37.Al-Noori AK, Said GA. The Effect of soft lining materials on mandibular residual ridge resorption for edentulous patient. Al Rafidain Dent J. 2013;13:66–71. [Google Scholar]
- 38.Kimoto S, Kimoto K, Murakami H, Gunji A, Ito N, Kawai Y. Survival analysis of mandibular complete dentures with acrylic-based resilient liners. Gerodontology. 2013;30:187–93. doi: 10.1111/j.1741-2358.2012.00658.x. [DOI] [PubMed] [Google Scholar]