

Abstract
Macular telangiectasia type 2 (Mac Tel 2) also known as idiopathic perifoveal telangiectasia and juxtafoveolar retinal telangiectasis type 2A is an enigmatic disease of unknown etiology. It manifests both neurodegenerative and vasculopathic characteristics.
It manifests itself during the fifth or sixth decades of life. Clinical characteristics include minimally dilated parafoveal capillaries with loss of the retinal transparency in the area involved, absence of lipid exudation, right-angled retinal venules, superficial retinal refractile deposits, hyperplasia of the retinal pigment epithelium (RPE), foveal atrophy and subretinal neovascularization (SRNV). Optical coherence tomography (OCT) images typically demonstrate outer retinal abnormalities and the presence of intra-retinal hyporeflective spaces that are usually not related with retinal thickening or fluorescein leakage. The typical fluorescein angiographic finding is a deep intraretinal hyperfluorescent staining in the temporal parafoveal area. With time this fluorescein hyperfluorescence involves the whole parafoveal area but does not extend to the center of the fovea. Long-term prognosis for central vision is poor, because of the development of SRNV or macular atrophy. Its pathogenesis remains unclear but multi-modality imaging with fluorescein angiography, spectral domain OCT, adaptive optics, confocal blue reflectance, short wave fundus autofluorescence, OCT angiography, and clinicopathological correlations implicate Müller cells. Currently there is no known treatment for this condition.
Keywords: juxtafoveal retinal telangiectasia, macular telangiectasia, Müller cells, parafoveal telangiectasis, perifoveal telangiectasis
1. Introduction
Retinal telangiectasis, characterized by capillary ectasia and incompetence, may occur secondary to branch retinal vein occlusion, diabetic retinopathy, X-ray irradiation, and carotid artery obstruction among several conditions.1 In 1982, Gass and Oya-kawa2 described 27 patients with juxtafoveolar telangiectasis with no apparent specific cause. They named this condition idiopathic juxtafoveolar retinal telangiectasis (IJRT) and classified it into four groups. Group 1 represented a localized form of Coats disease that occurred predominantly in male patients. These eyes were characterized by unilateral parafoveal retinal telangiectasis associated with lipid and serous retinal exudation that was thought to be developmental in origin.2 Men with bilateral symmetric juxtafoveolar telangiectasis affecting the temporal half of the juxtafoveolar areas with minimal intraretinal exudation typified Group 2 eyes. Group 3 eyes comprised both female and male patients who had bilateral parafoveolar telangiectasis with minimal intraretinal exudation. Group 4 eyes included individuals with familial perifoveolar retinal capillary occlusion and optic disc pallor.2 By 1993, Gass and Blodi3 identified 140 patients with this condition and reassessed their classification of IJRT. IJRT was divided into three groups and each group was further subdivided into two subgroups. Eyes in Group 1A most likely represent a form fruste of Coats disease characterized by congenital telangiectasia with lipidic serous exudation that affects mostly male patients in a unilateral pattern. Laser or pharmacologic treatment appears to be effective in preserving or improving vision in these patients.2,4,5 Eyes in Group 1B share the same clinical characteristics as eyes in Group 1A except for the very limited scope of telangiectatic involvement. Group 2A is the most common form of IJRT. These eyes lack lipid exudation and most of the clinical findings are rather subtle. Group 2B was defined as juvenile occult familiar IJRT. This subgroup comprised only two brothers with subtle retinal juxtafoveolar telangiectasis and bilateral subretinal neo-vascularization (SRNV). Group 3 eyes were characterized by bilateral minimal exudation and extensive occlusion of the jux-tafoveolar capillaries. Patients with Group 3A eyes had only ophthalmic manifestations, whereas patients in Group 3B also suffered from a central nervous system vasculopathy.3
Yannuzzi and co-workers6 proposed the most recent and simplified classification of IJRT. They merged Gass Groups 1A and 1B into a single aneurysmal telangiectasis group which they called aneurysmal telangiectasia or idiopathic macular telangiectasia type 1 (Mac Tel 1). Gass and Blodi3 Group 2A was renamed as idiopathic perifoveal telangiectasis, also known as idiopathic macular telan-giectasia type 2 (Mac Tel 2). Mac Tel 2 was further subdivided into a nonproliferative stage characterized by telangiectasia and foveal atrophy; and a proliferative stage characterized by the presence of SRNV.7 Gass and Blodi3 Groups 2B and 3 were discarded because of their rarity. In the accompanying editorial, Chew et al7 endorsed this new classification and encouraged its use. For the purposes of this review, we will refer to IJRT Type 2A as synonymous of idiopathic perifoveal telangiectasis or idiopathic Mac Tel 2.
2. Clinical findings
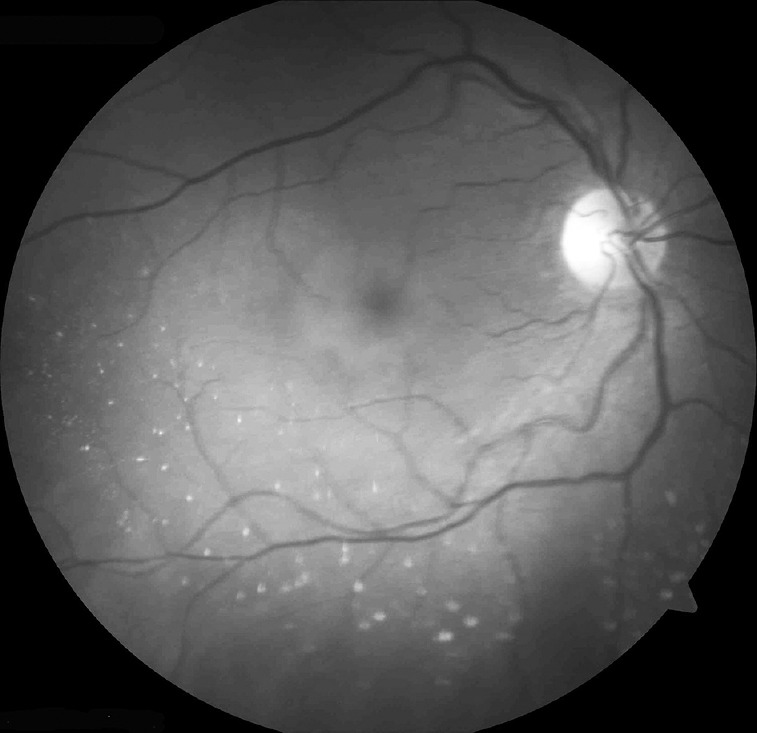
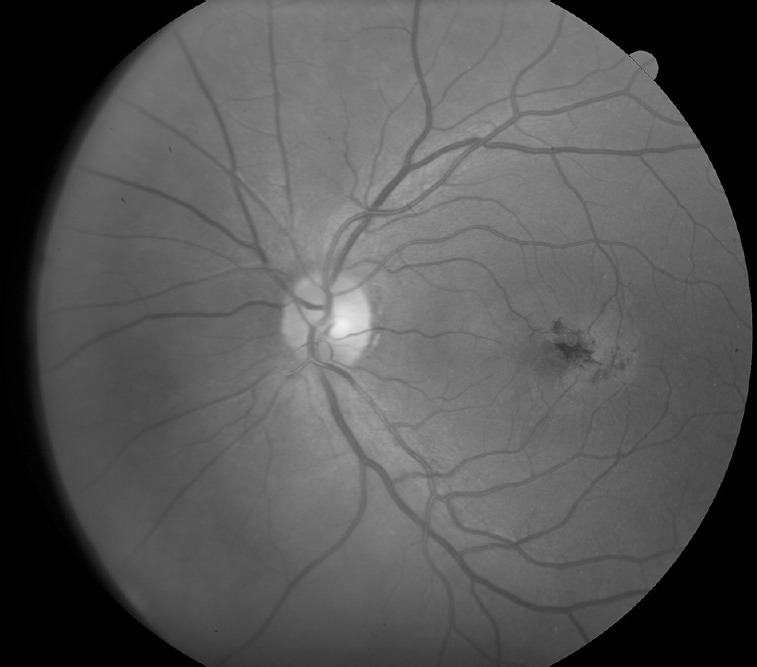
Most patients complain of nonspecific symptoms such as mild blurring of vision, positive scotoma, difficulty in reading, and metamorphopsia.8,9,10,11 Initially the visual acuities are relatively good, in the order of ≥ 20/30.12,13 Gass and Blodi3 have described the biomicroscopic findings in detail. The earliest ophthalmoscopic abnormalities seen in this disease are rather subtle and may be missed easily. Mild grayish discoloration of the retina with loss of retinal transparency temporal to the fovea is one of the earliest clinical abnormalities seen in Mac Tel 2. With disease progression, this loss of retinal transparency surrounds the perifoveal retina in an oval configuration3,6,14 (Fig. 1). This parafoveal graying becomes less intense and more difficult to visualize with continuous light exposure. Following dark adaptation of at least 15 minutes the parafoveal graying reappears.15 At this stage, the juxtafoveolar capillary abnormalities will be absent or barely evident. Fluorescein angiography (FA) is often required to demonstrate them.6,12,14 With time, slightly dilated and blunted retinal venules that extend at right angles into the temporal parafoveolar retina appear. Telangi-ectatic vessels typically are not associated with lipid exudation or hemorrhages.3,13 Multiple, golden, tiny, crystalline, refractile de posits near the inner retinal surface are a common finding occur ring in up to 45% of eyes2,3,14,16 (Fig. 2). The number of these deposits may vary from one to more than twenty. Up to 5% of eyes with Mac Tel 2 will exhibit yellow foveal lesions. These round intraretinal yellow spots measure anywhere between 100 mm and 300 mm in diameter and cause a minimal loss of the foveolar depression. They may be confused with Best disease or an adult form of vitelliform foveomacular dystrophy.3,17,18,19 Focal atrophy of the foveolar retina may develop and lead to a lamellar or even a full thickness macular hole (FTMH).2,3,6,20,21,22,23,24,25,26,27 These areas of foveolar atrophy have a distinct circular margin with central retinal thinning. They do not extend beyond the edges of the capillary free zone.22 The surgical management of eyes with FTMH associated with Mac Tel 2 remains controversial. The findings on OCT might be of prognostic value. If the OCT demonstrates irregular moth eaten edges and there is no evidence of vitreomacular traction, the surgical results will probably be poor.23,25,28 If instead the OCT shows round, edematous edges typical of an idiopathic macular hole then the surgical outcome will be more favorable.26
Fig. 1.
Grayish discoloration of the retina with loss of retinal transparency.
Fig. 2.
Multiple, golden, tiny, crystalline, refractile deposits near the inner retinal surface.
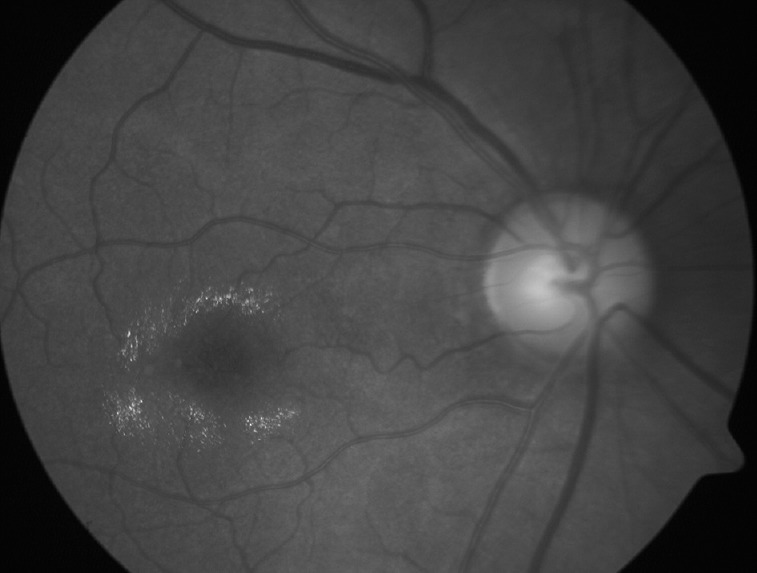
Stellate foci of intraretinal pigmented black plaques composed of hyperplastic retinal pigment epithelium (RPE) cells may develop along the right angled vessels in more advanced cases (Fig. 3). SRNV may develop in the vicinity of these plaques. Once present, SRNV is characterized by a rapid loss of vision, retinochoroidal anastomosis, cystoid macular edema (CME), subretinal hemorrhage, lipid hard exudates, and disciform scarring.6,18 SRNV in Mac Tel 2 may be confused with choroidal neovascularization in age-related macular degeneration (AMD). There are certain features that may help distinguish between both conditions. SRNV in Mac Tel 2 is not usually accompanied by a pigment epithelial detachment.6 The size of SRNV on Mac Tel 2 is also smaller in comparison to AMD.3
Fig. 3.
Intraretinal pigmented black plaque composed of hyperplastic retinal pigment epithelium cells.
3. Multimodality imaging findings
Because the clinical changes in Mac Tel 2 are rather subtle by biomicroscopy, particularly in the earlier stages, ancillary imaging studies are of paramount importance in the diagnosis of this condition.14,29
FA demonstrates dilated ectatic perifoveal capillaries that leak dye in the parafoveal temporal areas. Initially, the early phases of the angiogram show no evidence or barely minimal capillary dilatation. There is mild staining of the temporal outer parafoveal retina in the late phases, which spares the foveal center. As the disease progresses, the telangiectasia extends beyond the temporal parafoveal area and is manifested as a late oval shaped parafoveal hyperfluorescence3 (Fig. 4). The fluorescein leakage is not related to cystic spaces.6 There is a significant reduction in the size of the foveal avascular zone (FAZ) in eyes with Mac Tel 2 in comparison with normal eyes. There have even been two reported cases where the capillaries invaded the fovea and obliterated the FAZ.30,31 SRNV appears to originate from the deep retinal circulation and is characterized by early and late fluorescein leakage.6,32
Fig. 4.
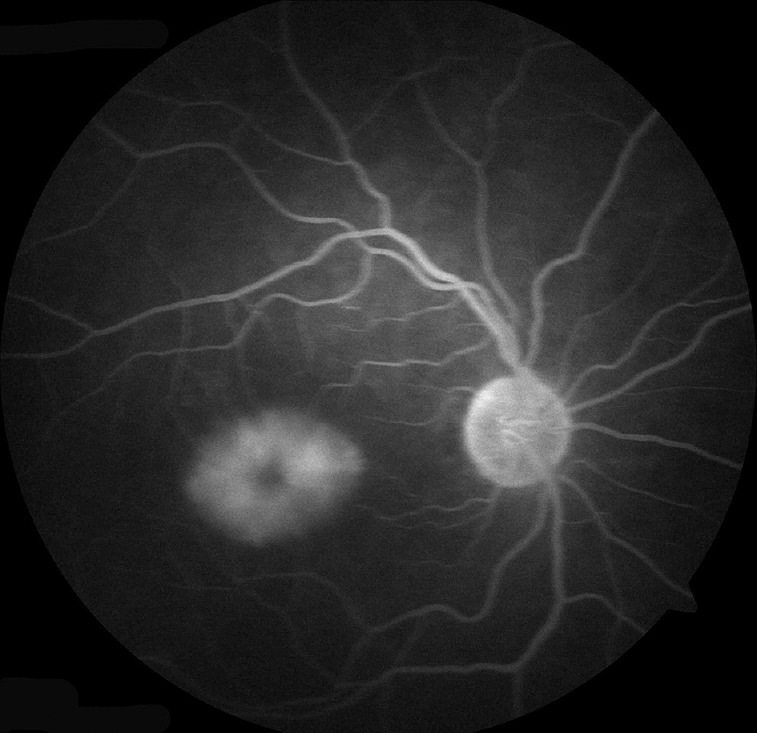
Late fluorescein angiogram frame showing oval shaped parafoveal hyperfluorescence.
OCT has revolutionized our understanding of Mac Tel 2 by demonstrating that there is no correlation between retinal thickening and fluorescein leakage21,33,34 (Fig. 5). Furthermore intraretinal hyporeflective spaces, that have been named as internal limiting membrane drape, cyst, cystoid, or pseudocystoid spaces by different authors, are commonly seen but are usually not related to retinal thickening or fluorescein angiographic leakage21,34,35,36,37,38,39,40,41 (Fig. 6). Interestingly, foveal thickness is decreased in most patients with Mac Tel 2.11,33,34,35,36,37,42 Spectral domain OCT has also documented the presence of outer retina abnormalities1 (Fig. 5).
Fig. 5.
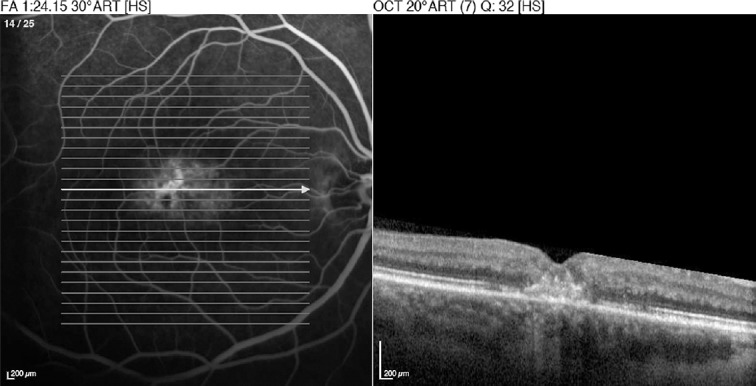
Optical coherence tomography demonstrating no correlation between retinal thickening and fluorescein leakage. Notice the disruption of the outer retina as well.
Fig. 6.

Optical coherence tomography demonstrating intraretinal hyporeflective spaces not related to retinal thickening.
Research prototypes that integrate adaptive optics (AO) with high-resolution spectral domain OCT provide high resolution photoreceptor imaging.43,44,45 AO imaging has shown that eyes with Mac Tel 2 eyes exhibit a lower cone density and disruption of the normal cone mosaic pattern. These abnormalities are even present in areas where the retinal vasculature appears normal.46
One of the earliest changes reported in Mac Tel 2 is an increased short wavelength fundus autofluorescence (SW-FAF) signal in the foveal region47 (Fig. 7). As the disease advances the SW-FAF actually decreases, not only in the central foveal area but also in the parafoveal areas, paralleling the increasing RPE atrophy.48
Fig. 7.
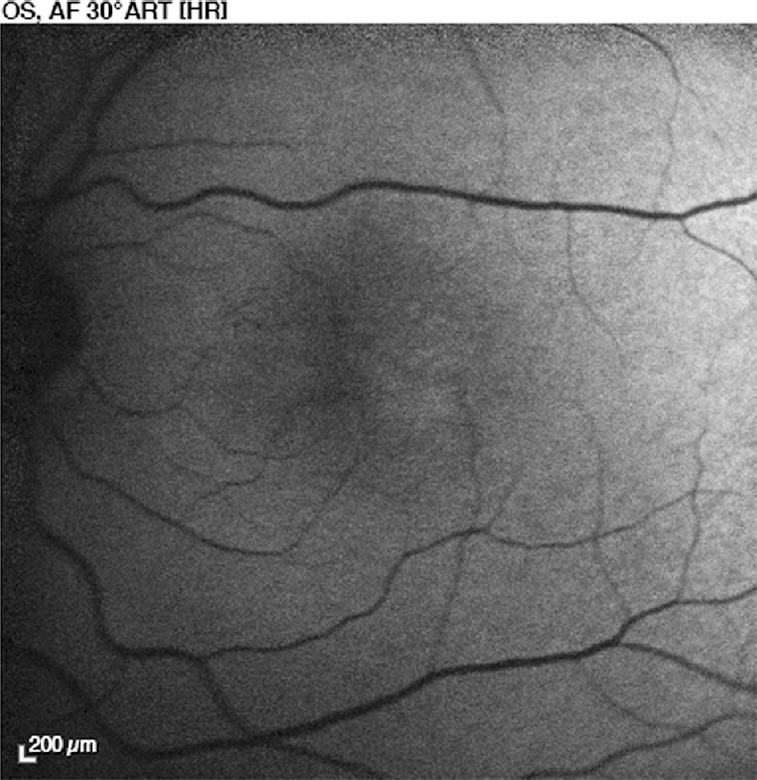
Short wavelength fundus autofluorescence (SW-FAF) imaging of the normal macula is characterized by a central dark area. In Mac Tel 2 there is an increased SWFAF signal in the foveal region.
Confocal reflectance imaging refers to an imaging modality that images the fundus after illuminating it with either a confocal blue light of 488 nm or an infrared light of 820 nm emitted by a scanning laser ophthalmoscope (SLO).27 Confocal blue reflectance (CBR) imaging demonstrated increased reflectance in the majority of patients with fluorescein angiographic evidence for Mac Tel 2.27,40,49 The increased CBR appeared in an oval parafoveal pattern that was slightly larger than the area of late phase fluorescein angiographic hyperfluorescence (Fig. 8).
Fig. 8.
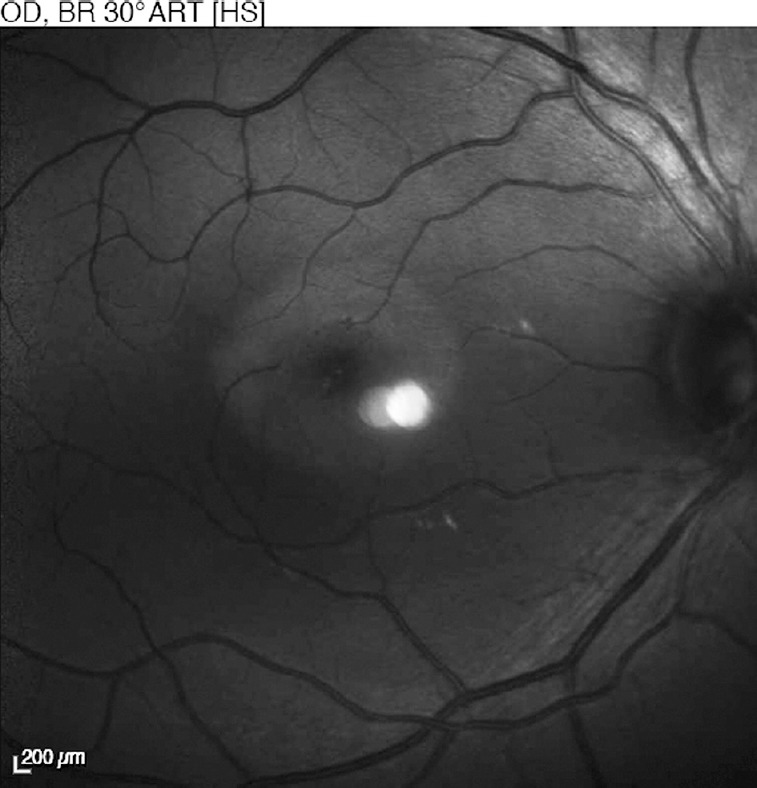
Confocal blue reflectance imaging showing increased reflectance.
OCT angiography demonstrates that the earliest vascular changes in Mac Tel 2 arise in the outer deep capillary plexus.50,51 As the disease progresses, the vascular changes also involve the inner superficial plexus, albeit to a lesser extent than the changes seen in the outer plexus.51 The vessels appear less densely packed, thinner, and in an abnormal arrangement. The normally avascular Henle layer and the outer nuclear layers become the target of a vascular invasion. Anastomosis between plexi and dragging of vessels temporally are also seen by OCT angiography.50
4. Functional testing
Mac Tel 2 has been studied extensively with microperimetry.1 Microperimetric findings show that eyes with Mac Tel 2 despite having a relatively good visual acuity, exhibit severe localized dysfunction next to fixation early in the disease process. Fortunately these scotomata do not appear to progress rapidly. A longitudinal study showed that after 1 year of follow-up, MP1 testing with a 20° central testing grid did not show any differences beyond the normal test–retest variability.52
5. Pathophysiology
The pathogenesis of Mac Tel 2 remains an enigma. Reports of familial and monozygotic twin cases suggest a genetic component despite the absence of established hereditary patterns.3,53,54,55,56,57 Multimodality imaging coupled with clinicopathological studies and the recent discovery of animal models have implicated Müller cells in the disease process.58,59,60
Because Müller cells span the entire retinal thickness, some have suggested that they function as optical fibers that permit light transmission with a minimum of reflection across the retina. Any pathological involvement of Müller cells would interrupt this mechanism causing limited transmission and an increase in retinal reflectance.61 The loss of retinal transparency and acquisition of the grayish discoloration seen clinically may be explained by Müller cell impairment. Jindal et al15 have hypothesized that a photochemical reaction caused by the release of chromophores from the impaired Müller cells is responsible for the changes in intensity in parafoveal graying seen with increasing light exposure and dark adaptation.
The superficial retinal crystalline deposits are thought to be the footplates of degenerated Müller cells and analogous to Rosenthal fibers. Rosenthal fibers are crystalline intracytoplasmic inclusions found in astrocytes of the central nervous system associated to chronic stress conditions.18,21
Even though the fluorescein angiographic findings are similar to the ones found in retinovascular diseases such as DME, there are subtle differences that were recognized by Gass.62 In Mac Tel 2, retinal fluorescein staining occurs prior to capillary dilation. Gass62 speculated that this finding was caused by staining of the extra cellular matrix and intracellular diffusion of the dye into the damaged retinal cells rather than to a breakdown of the blood retinal barrier leading to an increased retinal vascular permeability.62 He then suggested that the primary abnormality of Mac Tel 2 resided in the parafoveal neural cells or in Müller cells rather than the deep outer retinal juxtafoveolar capillaries. He concluded that the retinal vascular abnormalities were a secondary rather than the primary phenomenon.62 AO imaging clearly demonstrates that neural degeneration precedes retinal vascular involvement, lending support to Gass’s hypothesis.46
OCT further differentiates Mac Tel 2 from other retinovascular diseases by documenting the presence of intraretinal hyporewflective spaces that do not correlate with an increased retinal thickness or fluorescein leakage.1,29 These hyporeflective spaces most likely do not represent fluid-filled spaces as seen in CME secondary to retinal vein occlusions or diabetic macular edema (DME). The density of these hyporeflective spaces can be measured and compared to the vitreous density by analyzing the light reflectivity profiles from OCT. In eyes with neurodegenerative conditions such as cone dystrophy, there is less light reflectivity as compared to eyes with exudative conditions such as DME or central serous chorioretinopathy.63 Müller cells play an important role in the structural integrity of the fovea.64 The OCT findings suggest that these hyporeflective spaces may represent cavity formation after photoreceptor and/or Müller cell loss rather than fluid accumulation caused by blood retinal barrier breakdown associated with exudation or inflammation.63
SW-FAF imaging of the normal macula is characterized by a central dark area. Absorption of the blue light by the luteal macular pigments and the RPE melanin are responsible for this finding.65 In Mac Tel 2, an increase of SW-FAF in the foveal region precedes clinical and fluorescein angiographic findings.47 Because histopathological findings show that the RPE is healthy in Mac Tel 2, the increased SW-FAF is most likely the result of macular pigment depletion from the fovea rather than an increased lipofuscin accumulation in the RPE.66,67 The increased CBR may also be explained by a decrease in macular pigment in the parafoveal area. Because the absorption maximum of macular pigment is in the range of blue light at approximately 460 nm, a decrease in macular pigment in the parafoveal area will cause an increased reflection or a decreased absorption of the blue light.27,68 Heterochromatic flicker reflectometry and subtraction autofluorescent imaging at 488 nm and 514 nm confirm the loss of macular pigment optical density (MPOD) in these eyes.47,69,70 Disease severity as documented by late FA leakage mirrors changes in the distribution of the MPOD.70
The human body cannot produce macular pigment; therefore, the macular pigment is entirely of dietary origin. Our bodies can convert lutein into zeaxanthin but not zeaxanthin into lutein.71 Upon ingestion, high-density lipoprotein transports both zeaxanthin and lutein into the bloodstream.72 The specific molecular mechanisms that mediate the selective uptake, concentration, and stabilization of the macular pigment are currently unknown. Macular pigment binding proteins have been immunolocalized to the cone and rod inner segments.73,74,75 Quantification of macular pigment has shown a greater reduction in zeaxanthin compared to lutein in Mac Tel 2 eyes. It is currently unknown if the main problem is retinal failure to convert lutein into zeaxanthin or zeaxanthin accumulation.76 These findings can be attributed to a primary loss of macular pigment secondary to defective transport or storage of macular pigment or a progressive pathological process that damages the anatomic structures that affect macular pigment accumulation.69,70,76 Oral supplementation with 12 mg of lutein and 0.6 mg of zeaxanthin daily for 9 months increased macular pigment in areas where the macular pigment was present at baseline, but did not produce an increase in macular pigment in areas where the macular pigment was previously absent.69
Clinicopathological correlations of eyes with Mac Tel 2 confirm these findings of depleted macular pigment.58,59 Luteal pigment was characteristically absent in these eyes. Immunohistochemical analysis demonstrated the loss of perifoveal Müller cells. Interestingly there was a topographical correlation between areas of macular pigment absence and areas of Müller cell depletion.58 Müller cells may serve as a retinal reservoir for macular pigment but the exact details of how Müller cells affect trafficking, deposition, and storage of the macular pigment are currently unknown.64
Müller cells also help provide nutrition to the surrounding retinal neurons and also play a role in inducing and maintaining the integrity of the blood-retinal barrier. Their processes are intimately related to the retinal blood vessels in the deep outer plexus. By contrast, the retinal blood vessels in the superficial inner plexus are closely related with retinal astrocytes.58,77,78,79 OCT angiography demonstrates prominent vascular abnormalities in the outer deep capillary plexus. Vascular invasion of normally avascular retinal areas such as the subretinal space or the outer nuclear layer may represent a compensatory mechanism for the ischemic insult caused by the vascular abnormalities.
Recently a transgenic mouse model with conditional ablation of Müller cells has been described.60 These animals exhibit photore-ceptor apoptosis, retinal telangiectasis, breakdown of the blood retinal barrier and intraretinal neovascularization. It is hoped that with this model further advancements in our understanding of Mac Tel 2 can be made.
6. Treatment
The main limitation in the treatment of Mac Tel 2 is the lack of knowledge of the basic pathophysiologic mechanisms underlying this condition. FA was the earliest imaging modality used to study this disease. Because the typical angiographic findings suggested the presence of macular edema, it was thought that Mac Tel 2 was a primary retinovascular disease. Therefore, the same treatment modalities used to treat retinovascular diseases, such as macular laser photocoagulation,80 intravitreal triamcinolone,81 photody-namic therapy,82 and intravitreal anti-vascular endothelial growth factor (anti-VEGF) agents,83 were used to treat Mac Tel 2. None of these were particularly beneficial in eyes with nonproliferative Mac Tel 2.1 In some eyes with Mac Tel 2, SRNV will develop. These eyes may benefit from anti-VEGF treatment.1
Several animal models of retinal degenerative diseases have shown that multiple cytokines, neurotrophins, and growth factors such as ciliary neurotrophic factor (CNTF) can rescue photo-receptors.84,85,86 Based on the premise that Mac Tel 2 has a neuro-degenerative component, neuroprotective agents such as CNTF are currently undergoing testing. Delivery of CNTF via encapsulated cell technology (ECT) into the vitreous cavity has overcome a major challenge in retinal CNTF delivery. In ECT, genetically engineered live cells are placed within a semipermeable polymer capsule that is implanted surgically at the pars plana. These cells secrete the therapeutic protein of interest in a continuous fashion directly into the vitreous cavity.87 ECT containing CNTF appears to be safe and well tolerated in eyes with Mac Tel 2 as evidenced by the results of a recently concluded phase 1 trial.88
In summary, Mac Tel 2 is an enigmatic condition characterized by dual neurodegenerative and vasculopathic pathways secondary to Müller cell dysfunction. The exact cause of this dysfunction remains unclear. Currently there is no treatment available to halt or alter the progression of this disease. Although anti-VEGF treatment seems to limit SRNV in the final proliferative stage of the disease, previous stages currently are not treatable.1
Footnotes
Conflicts of interest: Dr Wu has received lecture fees from Bayer Health and Quantel Medical.
Presented in part at the Taiwan Academy of Ophthalmology Spring Meeting, March 31, 2012, Taipei, Taiwan.
References
- 1.Wu L, Evans T, Arevalo JF. Idiopathic macular telangiectasia type 2 (idiopathic juxtafoveolar retinal telangiectasis type 2A, Mac Tel 2) Surv Ophthalmol. 2013;58:536–559. doi: 10.1016/j.survophthal.2012.11.007. [DOI] [PubMed] [Google Scholar]
- 2.Gass JD, Oyakawa RT. Idiopathic juxtafoveolar retinal telangiectasis. Arch Ophthalmol. 1982;100:769–780. doi: 10.1001/archopht.1982.01030030773010. [DOI] [PubMed] [Google Scholar]
- 3.Gass JD, Blodi BA. Idiopathic juxtafoveolar retinal telangiectasis. Update of classification and follow-up study. Ophthalmology. 1993;100:1536–1546. [PubMed] [Google Scholar]
- 4.Chopdar A. Retinal telangiectasis in adults: fluorescein angiographic findings and treatment by argon laser. Br J Ophthalmol. 1978;62:243–250. doi: 10.1136/bjo.62.4.243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lee ST, Friedman SM, Rubin ML. Cystoid macular edema secondary to juxta-foveolar telangiectasis in Coats’ disease. Ophthalmic Surg. 1991;22:218–221. [PubMed] [Google Scholar]
- 6.Yannuzzi LA, Bardal AM, Freund KB, et al. Idiopathic macular telangiectasia. Arch Ophthalmol. 2006;124:450–460. doi: 10.1001/archopht.124.4.450. [DOI] [PubMed] [Google Scholar]
- 7.Chew E, Gillies M, Bird A. Macular telangiectasia: a simplified classification. Arch Ophthalmol. 2006;124:573–574. doi: 10.1001/archopht.124.4.573. [DOI] [PubMed] [Google Scholar]
- 8.Charbel Issa P, Holz FG, Scholl HP. Metamorphopsia in patients with macular telangiectasia type 2. Doc Ophthalmol. 2009;119:133–140. doi: 10.1007/s10633-009-9190-9. [DOI] [PubMed] [Google Scholar]
- 9.Charbel Issa P, Helb HM, Rohrschneider K, et al. Microperimetric assessment of patients with type 2 idiopathic macular telangiectasia. Invest Ophthalmol Vis Sci. 2007;48:3788–3795. doi: 10.1167/iovs.06-1272. [DOI] [PubMed] [Google Scholar]
- 10.Finger RP, Charbel Issa P, Fimmers R, et al. Reading performance is reduced by parafoveal scotomas in patients with macular telangiectasia type 2. Invest Ophthalmol Vis Sci. 2009;50:1366–1370. doi: 10.1167/iovs.08-2032. [DOI] [PubMed] [Google Scholar]
- 11.Charbel Issa P, Helb HM, Holz FG, Scholl HP. Correlation of macular function with retinal thickness in nonproliferative type 2 idiopathic macular telangi-ectasia. Am J Ophthalmol. 2008;145:169–175. doi: 10.1016/j.ajo.2007.08.028. [DOI] [PubMed] [Google Scholar]
- 12.Ryan SJ. Retina. 4th ed. Philadelphia: Elsevier Mosby; 2006. pp. 1409–1415. 3 v. (xxiv, 2654, 64 p.) [Google Scholar]
- 13.Casswell AG, Chaine G, Rush P, Bird AC. Paramacular telangiectasis. Trans Ophthalmol Soc U K. 1986;105:683–692. [PubMed] [Google Scholar]
- 14.Abujamra S, Bonanomi MT, Cresta FB, et al. Idiopathic juxtafoveolar retinal telangiectasis: clinical pattern in 19 cases. Ophthalmologica. 2000;214:406–411. doi: 10.1159/000027534. [DOI] [PubMed] [Google Scholar]
- 15.Jindal A, Choudhury H, Pathengay A, Flynn HW., Jr A novel clinical sign in macular telangiectasia type 2. Ophthalmic Surg Lasers Imaging Retina. 2015;46:134–136. doi: 10.3928/23258160-20150101-26. [DOI] [PubMed] [Google Scholar]
- 16.Moisseiev J, Lewis H, Bartov E, et al. Superficial retinal refractile deposits in juxtafoveal telangiectasis. Am J Ophthalmol. 1990;109:604–605. doi: 10.1016/s0002-9394(14)70699-3. [DOI] [PubMed] [Google Scholar]
- 17.Margalit E, Apte RS, Sadda SR. Idiopathic parafoveal telangiectasis associated with a foveal pseudovitelliform lesion. Br J Ophthalmol. 2002;86:1455–1456. doi: 10.1136/bjo.86.12.1455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Gass JD. Stereoscopic atlas of macular diseases: Diagnosis and treatment. 4th ed. Vol. 1. St. Louis: Mosby; 1997. pp. 504–512. 2 v. [xi, 1061, I19 p., (32) p. of plates] [Google Scholar]
- 19.Diaz-Rodriguez EJ. [Group 2A idiopathic parafoveal telangiectasis] Arch Soc Esp Oftalmol. 2005;80:541–545. doi: 10.4321/s0365-66912005000900010. [DOI] [PubMed] [Google Scholar]
- 20.Patel B, Duvall J, Tullo AB. Lamellar macular hole associated with idiopathic juxtafoveolar telangiectasia. Br J Ophthalmol. 1988;72:550–551. doi: 10.1136/bjo.72.7.550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Cohen SM, Cohen ML, El-Jabali F, Pautler SE. Optical coherence tomography findings in nonproliferative group 2a idiopathic juxtafoveal retinal telangiec-tasis. Retina. 2007;27:59–66. doi: 10.1097/01.iae.0000256663.94734.e1. [DOI] [PubMed] [Google Scholar]
- 22.Olson JL, Mandava N. Macular hole formation associated with idiopathic par-afoveal telangiectasia. Graefes Arch Clin Exp Ophthalmol. 2006;244:411–412. doi: 10.1007/s00417-005-0057-9. [DOI] [PubMed] [Google Scholar]
- 23.Charbel Issa P, Scholl HP, Gaudric A, et al. Macular full-thickness and lamellar holes in association with type 2 idiopathic macular telangiectasia. Eye (Lond) 2009;23:435–441. doi: 10.1038/sj.eye.6703003. [DOI] [PubMed] [Google Scholar]
- 24.Gregori N, Flynn HW., Jr Surgery for full-thickness macular hole in patients with idiopathic macular telangiectasia type 2. Ophthalmic Surg Lasers Imaging. 2010;41 doi: 10.3928/15428877-20100726-10. http://dx.doi.org/10.3928/15428877-20100726-10. [DOI] [PubMed] [Google Scholar]
- 25.Koizumi H, Slakter JS, Spaide RF. Full-thickness macular hole formation in idiopathic parafoveal telangiectasis. Retina. 2007;27:473–476. doi: 10.1097/01.iae.0000246678.93495.2f. [DOI] [PubMed] [Google Scholar]
- 26.Shukla D. Evolution and management of macular hole secondary to type 2 idiopathic macular telangiectasia. Eye (Lond) 2011;25:532–533. doi: 10.1038/eye.2010.233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Charbel Issa P, Berendschot TT, Staurenghi G, et al. Confocal blue reflectance imaging in type 2 idiopathic macular telangiectasia. Invest Ophthalmol Vis Sci. 2008;49:1172–1177. doi: 10.1167/iovs.07-0636. [DOI] [PubMed] [Google Scholar]
- 28.Rishi P, Kothari AR. Parafoveal telangiectasia (PFT) has been associated with changes in macular architecture and macular holes (lamellar and full thick ness) Retina. 2008;28:184–185. doi: 10.1097/IAE.0b013e31815e98c0. author reply 5-6. [DOI] [PubMed] [Google Scholar]
- 29.Wu L. Multimodality imaging in macular telangiectasia 2: A clue to its path-ogenesis. Indian J Ophthalmol. 2015;63:394–398. doi: 10.4103/0301-4738.159864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Mansour AM, Schachat A. Foveal avascular zone in idiopathic juxtafoveolar telangiectasia. Ophthalmologica. 1993;207:9–12. doi: 10.1159/000310399. [DOI] [PubMed] [Google Scholar]
- 31.Koizumi H, Cooney MJ, Leys A, Spaide RF. Centripetal retinal capillary prolif eration in idiopathic parafoveolar telangiectasis. Br J Ophthalmol. 2007;91:1719–1720. doi: 10.1136/bjo.2007.115485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Soheilian M, Tavallali A, Peyman GA. Identification of intraretinal neo-vascularization by high-speed indocyanine green angiography in idiopathic perifoveal telangiectasia. Ophthalmic Surg Lasers Imaging. 2007;38:167–169. doi: 10.3928/15428877-20070301-16. [DOI] [PubMed] [Google Scholar]
- 33.Surguch V, Gamulescu MA, Gabel VP. Optical coherence tomography findings in idiopathic juxtafoveal retinal telangiectasis. Graefes Arch Clin Exp Ophthalmol. 2007;245:783–788. doi: 10.1007/s00417-006-0432-1. [DOI] [PubMed] [Google Scholar]
- 34.Koizumi H, Iida T, Maruko I. Morphologic features of group 2A idiopathic juxtafoveolar retinal telangiectasis in three-dimensional optical coherence tomography. Am J Ophthalmol. 2006;142:340–343. doi: 10.1016/j.ajo.2006.03.021. [DOI] [PubMed] [Google Scholar]
- 35.Paunescu LA, Ko TH, Duker JS, et al. Idiopathic juxtafoveal retinal telangiectasis: new findings by ultrahigh-resolution optical coherence tomography. Ophthalmology. 2006;113:48–57. doi: 10.1016/j.ophtha.2005.08.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Gaudric A, Ducos de Lahitte G, Cohen SY, et al. Optical coherence tomography in group 2A idiopathic juxtafoveolar retinal telangiectasis. Arch Ophthalmol. 2006;124:1410–1419. doi: 10.1001/archopht.124.10.1410. [DOI] [PubMed] [Google Scholar]
- 37.Gupta V, Gupta A, Dogra MR, Agarwal A. Optical coherence tomography in group 2A idiopathic juxtafoveolar telangiectasis. Ophthalmic Surg Lasers Im aging. 2005;36:482–486. [PubMed] [Google Scholar]
- 38.Albini TA, Benz MS, Coffee RE, et al. Optical coherence tomography of idio-pathic juxtafoveolar telangiectasia. Ophthalmic Surg Lasers Imaging. 2006;37:120–128. [PubMed] [Google Scholar]
- 39.Sanchez JG, Garcia RA, Wu L, et al. Optical coherence tomography character istics of group 2A idiopathic parafoveal telangiectasis. Retina. 2007;27:1214–1220. doi: 10.1097/IAE.0b013e318074bc4b. [DOI] [PubMed] [Google Scholar]
- 40.Bottoni F, Eandi CM, Pedenovi S, Staurenghi G. Integrated clinical evaluation of Type 2A idiopathic juxtafoveolar retinal telangiectasis. Retina. 2010;30:317–326. doi: 10.1097/IAE.0b013e3181b9f11e. [DOI] [PubMed] [Google Scholar]
- 41.Fallano KA, Ibrahim M, Nguyen QD, Do DV. Progressive changes from idiopathic macular telangiectasia seen with spectral domain optical coherence tomogra phy. Can J Ophthalmol. 2010;45:649–650. doi: 10.3129/i10-038. [DOI] [PubMed] [Google Scholar]
- 42.Lee HC, Liu M, Ho AC. Idiopathic juxtafoveal telangiectasis in association with celiac sprue. Arch Ophthalmol. 2004;122:411–413. doi: 10.1001/archopht.122.3.411. [DOI] [PubMed] [Google Scholar]
- 43.Liang J, Williams DR, Miller DT. Supernormal vision and high-resolution retinal imaging through adaptive optics. J Opt Soc Am A Opt Image Sci Vis. 1997;14:2884–2892. doi: 10.1364/josaa.14.002884. [DOI] [PubMed] [Google Scholar]
- 44.Povazay B, Hofer B, Torti C, et al. Impact of enhanced resolution, speed and penetration on three-dimensional retinal optical coherence tomography. Opt Express. 2009;17:4134–4150. doi: 10.1364/oe.17.004134. [DOI] [PubMed] [Google Scholar]
- 45.Massamba N, Querques G, Lamory B, et al. In vivo evaluation of photoreceptor mosaic in type 2 idiopathic macular telangiectasia using adaptive optics. Acta Ophthalmol. 2011;89:e601–e603. doi: 10.1111/j.1755-3768.2010.02000.x. [DOI] [PubMed] [Google Scholar]
- 46.Ooto S, Hangai M, Takayama K, et al. High-resolution photoreceptor imaging in idiopathic macular telangiectasia type 2 using adaptive optics scanning laser ophthalmoscopy. Invest Ophthalmol Vis Sci. 2011;52:5541–5550. doi: 10.1167/iovs.11-7251. [DOI] [PubMed] [Google Scholar]
- 47.Wong WT, Forooghian F, Majumdar Z, et al. Fundus autofluorescence in type 2 idiopathic macular telangiectasia: correlation with optical coherence tomog raphy and microperimetry. Am J Ophthalmol. 2009;148:573–583. doi: 10.1016/j.ajo.2009.04.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Clemons TE, Gillies MC, Chew EY, et al. Baseline characteristics of participants in the natural history study of macular telangiectasia (MacTel) MacTel Project Report No. 2. Ophthalmic Epidemiol. 2010;17:66–73. doi: 10.3109/09286580903450361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Charbel Issa P, Finger RP, Helb HM, et al. A new diagnostic approach in patients with type 2 macular telangiectasia: confocal reflectance imaging. Acta Ophthalmol. 2008;86:464–465. doi: 10.1111/j.1600-0420.2007.01041.x. [DOI] [PubMed] [Google Scholar]
- 50.Thorell MR, Zhang Q, Huang Y, et al. Swept-source OCT angiography of macular telangiectasia type 2. Ophthalmic Surg Lasers Imaging Retina. 2014;45:369–380. doi: 10.3928/23258160-20140909-06. [DOI] [PubMed] [Google Scholar]
- 51.Spaide RF, Klancnik JM, Jr, Cooney MJ. Retinal vascular layers in macular tel-angiectasia type 2 imaged by optical coherence tomographic angiography. JAMA Ophthalmol. 2015;133:66–73. doi: 10.1001/jamaophthalmol.2014.3950. [DOI] [PubMed] [Google Scholar]
- 52.Schmitz-Valckenberg S, Ong EE, Rubin GS, et al. Structural and functional changes over time in MacTel patients. Retina. 2009;29:1314–1320. doi: 10.1097/IAE.0b013e3181a4d2f1. [DOI] [PubMed] [Google Scholar]
- 53.Hutton WL, Snyder WB, Fuller D, Vaiser A. Focal parafoveal retinal telangiec-tasis. Arch Ophthalmol. 1978;96:1362–1367. doi: 10.1001/archopht.1978.03910060116003. [DOI] [PubMed] [Google Scholar]
- 54.Menchini U, Virgili G, Bandello F, et al. Bilateral juxtafoveolar telangiectasis in monozygotic twins. Am J Ophthalmol. 2000;129:401–403. doi: 10.1016/s0002-9394(99)00380-3. [DOI] [PubMed] [Google Scholar]
- 55.Siddiqui N, Fekrat S. Group 2A idiopathic juxtafoveolar retinal telangiectasia in monozygotic twins. Am J Ophthalmol. 2005;139:568–570. doi: 10.1016/j.ajo.2004.09.030. [DOI] [PubMed] [Google Scholar]
- 56.Chew EY, Murphy RP, Newsome DA, Fine SL. Parafoveal telangiectasis and diabetic retinopathy. Arch Ophthalmol. 1986;104:71–75. doi: 10.1001/archopht.1986.01050130081025. [DOI] [PubMed] [Google Scholar]
- 57.Putteman A, Toussaint D, Graff E, Verougstraete C. [Idiopathic familial juxta-foveolar retinal telangiectasias] Bull Soc Belge Ophthalmol. 1984;209:81–90. [in French] [PubMed] [Google Scholar]
- 58.Powner MB, Gillies MC, Tretiach M, et al. Perifoveal Müller cell depletion in a case of macular telangiectasia type 2. Ophthalmology. 2010;117:2407–2416. doi: 10.1016/j.ophtha.2010.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Powner MB, Gillies MC, Zhu M, et al. Loss of Müller’s cells and photoreceptors in macular telangiectasia type 2. Ophthalmology. 2013;120:2344–2352. doi: 10.1016/j.ophtha.2013.04.013. [DOI] [PubMed] [Google Scholar]
- 60.Shen W, Fruttiger M, Zhu L, et al. Conditional Müller cell ablation causes in dependent neuronal and vascular pathologies in a novel transgenic model. J Neurosci. 2012;32:15715–15727. doi: 10.1523/JNEUROSCI.2841-12.2012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Franze K, Grosche J, Skatchkov SN, et al. Müller cells are living optical fibers in the vertebrate retina. Proc Natl Acad Sci U S A. 2007;104:8287–8292. doi: 10.1073/pnas.0611180104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Gass JD. Histopathologic study of presumed parafoveal telangiectasis. Retina. 2000;20:226–227. doi: 10.1097/00006982-200002000-00028. [DOI] [PubMed] [Google Scholar]
- 63.Barthelmes D, Sutter FK, Gillies MC. Differential optical densities of intraretinal spaces. Invest Ophthalmol Vis Sci. 2008;49:3529–3534. doi: 10.1167/iovs.07-1320. [DOI] [PubMed] [Google Scholar]
- 64.Gass JD. Müller cell cone, an overlooked part of the anatomy of the fovea centralis: hypotheses concerning its role in the pathogenesis of macular hole and foveomacualr retinoschisis. Arch Ophthalmol. 1999;117:821–823. doi: 10.1001/archopht.117.6.821. [DOI] [PubMed] [Google Scholar]
- 65.Schmitz-Valckenberg S, Holz FG, Bird AC, Spaide RF. Fundus autofluorescence imaging: review and perspectives. Retina. 2008;28:385–409. doi: 10.1097/IAE.0b013e318164a907. [DOI] [PubMed] [Google Scholar]
- 66.Helb HM, Charbel Issa P, Van Der Veen RL, et al. Abnormal macular pigment distribution in type 2 idiopathic macular telangiectasia. Retina. 2008;28:808–816. doi: 10.1097/IAE.0b013e31816d81aa. [DOI] [PubMed] [Google Scholar]
- 67.Schmitz-Valckenberg S, Fan K, Nugent A, et al. Correlation of functional impairment and morphological alterations in patients with group 2A idiopathic juxtafoveal retinal telangiectasia. Arch Ophthalmol. 2008;126:330–335. doi: 10.1001/archopht.126.3.330. [DOI] [PubMed] [Google Scholar]
- 68.Snodderly DM, Brown PK, Delori FC, Auran JD. The macular pigment. I. Absorbance spectra, localization, and discrimination from other yellow pigments in primate retinas. Invest Ophthalmol Vis Sci. 1984;25:660–673. [PubMed] [Google Scholar]
- 69.Zeimer MB, Kromer I, Spital G, et al. Macular telangiectasia: patterns of dis tribution of macular pigment and response to supplementation. Retina. 2010;30:1282–1293. doi: 10.1097/IAE.0b013e3181e096dd. [DOI] [PubMed] [Google Scholar]
- 70.Zeimer MB, Padge B, Heimes B, Pauleikhoff D. Idiopathic macular telangiectasia type 2: distribution of macular pigment and functional investigations. Retina. 2010;30:586–595. doi: 10.1097/IAE.0b013e3181bd2d38. [DOI] [PubMed] [Google Scholar]
- 71.Whitehead AJ, Mares JA, Danis RP. Macular pigment: a review of current knowledge. Arch Ophthalmol. 2006;124:1038–1045. doi: 10.1001/archopht.124.7.1038. [DOI] [PubMed] [Google Scholar]
- 72.Clevidence BA, Bieri JG. Association of carotenoids with human plasma lipo-proteins. Methods Enzymol. 1993;214:33–46. doi: 10.1016/0076-6879(93)14051-j. [DOI] [PubMed] [Google Scholar]
- 73.Yemelyanov AY, Katz NB, Bernstein PS. Ligand-binding characterization of xanthophyll carotenoids to solubilized membrane proteins derived from hu man retina. Exp Eye Res. 2001;72:381–392. doi: 10.1006/exer.2000.0965. [DOI] [PubMed] [Google Scholar]
- 74.Bhosale P, Larson AJ, Frederick JM, et al. Identification and characterization of a Pi isoform of glutathione S-transferase (GSTP1) as a zeaxanthin-binding protein in the macula of the human eye. J Biol Chem. 2004;279:49447–49454. doi: 10.1074/jbc.M405334200. [DOI] [PubMed] [Google Scholar]
- 75.Bhosale P, Li B, Sharifzadeh M, et al. Purification and partial characterization of a lutein-binding protein from human retina. Biochemistry. 2009;48:4798–4807. doi: 10.1021/bi9004478. [DOI] [PubMed] [Google Scholar]
- 76.Charbel Issa P, van der Veen RL, Stijfs A, et al. Quantification of reduced macular pigment optical density in the central retina in macular telangiectasia type 2. Exp Eye Res. 2009;89:25–31. doi: 10.1016/j.exer.2009.02.006. [DOI] [PubMed] [Google Scholar]
- 77.Tout S, Chan-Ling T, Hollander H, Stone J. The role of Müller cells in the for mation of the blood-retinal barrier. Neuroscience. 1993;55:291–301. doi: 10.1016/0306-4522(93)90473-s. [DOI] [PubMed] [Google Scholar]
- 78.Newman E, Reichenbach A. The Müller cell: a functional element of the retina. Trends Neurosci. 1996;19:307–312. doi: 10.1016/0166-2236(96)10040-0. [DOI] [PubMed] [Google Scholar]
- 79.Nishikawa S, Tamai M. Müller cells in the human foveal region. Curr Eye Res. 2001;22:34–41. doi: 10.1076/ceyr.22.1.34.6979. [DOI] [PubMed] [Google Scholar]
- 80.Park DW, Schatz H, McDonald HR, Johnson RN. Grid laser photocoagulation for macular edema in bilateral juxtafoveal telangiectasis. Ophthalmology. 1997;104:1838–1846. doi: 10.1016/s0161-6420(97)30019-0. [DOI] [PubMed] [Google Scholar]
- 81.Wu L, Evans T, Arevalo JF, et al. Long-term effect of intravitreal triamcinolone in the nonproliferative stage of type II idiopathic parafoveal telangiectasia. Retina. 2008;28:314–319. doi: 10.1097/IAE.0b013e31814cf03e. [DOI] [PubMed] [Google Scholar]
- 82.De Lahitte GD, Cohen SY, Gaudric A. Lack of apparent short-term benefitof photodynamic therapy in bilateral, acquired, parafoveal telangiectasis without subretinal neovascularization. Am J Ophthalmol. 2004;138:892–894. doi: 10.1016/j.ajo.2004.06.010. [DOI] [PubMed] [Google Scholar]
- 83.Charbel Issa P, Finger RP, Kruse K, et al. Monthly ranibizumab for non-proliferative macular telangiectasia type 2: A 12-month prospective study. Am J Ophthalmol. 2011;151:876–886. e1. doi: 10.1016/j.ajo.2010.11.019. [DOI] [PubMed] [Google Scholar]
- 84.LaVail MM, Unoki K, Yasumura D, et al. Multiple growth factors, cytokines, and neurotrophins rescue photoreceptors from the damaging effects of constant light. Proc Natl Acad Sci U S A. 1992;89:11249–11253. doi: 10.1073/pnas.89.23.11249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.LaVail MM, Yasumura D, Matthes MT, et al. Protection of mouse photoreceptors by survival factors in retinal degenerations. Invest Ophthalmol Vis Sci. 1998;39:592–602. [PubMed] [Google Scholar]
- 86.Tao W, Wen R, Goddard MB, et al. Encapsulated cell-based delivery of CNTF reduces photoreceptor degeneration in animal models of retinitis pigmentosa. Invest Ophthalmol Vis Sci. 2002;43:3292–3298. [PubMed] [Google Scholar]
- 87.Tao W. Application of encapsulated cell technology for retinal degenerative diseases. Expert Opin Biol Ther. 2006;6:717–726. doi: 10.1517/14712598.6.7.717. [DOI] [PubMed] [Google Scholar]
- 88.Chew EY, Clemons TE, Peto T, et al. Ciliary neurotrophic factor for macular telangiectasia type 2: results from a phase 1 safety trial. Am J Ophthalmol. 2015;159:659–666. e1. doi: 10.1016/j.ajo.2014.12.013. [DOI] [PMC free article] [PubMed] [Google Scholar]