

Abstract
Background/Purpose:
To assess the prevalence of nonstrabismic accommodative and vergence dysfunctions among primary schoolchildren in Hampyeong, a rural area of South Korea.
Methods:
Five hundred and eighty-nine primary schoolchildren, 8–13 years old, were each given a thorough eye examination, including binocular-vision testing, near point of convergence, horizontal phoria measurement by von Graefe, and negative and positive vergence amplitudes with prism bar, to determine any form of accommodative or vergence dysfunctions.
Results:
Of the 589 participants examined, 168 (28.5%) primary schoolchildren presented some form of nonstrabismic accommodative or vergence dysfunctions. The prevalence of accommodative dysfunctions and vergence dysfunctions was 13.2% and 9%, respectively. Convergence insufficiency (10.3%) was more prevalent than convergence excess (1.9%), and accommodative insufficiency (5.3%) was more prevalent than accommodative excess (1.2%).
Conclusion:
This study suggests that nonstrabismic accommodative and vergence dysfunctions are prevalent in the rural area of South Korean primary schoolchildren, and convergence insufficiency was the most prevalent.
Keywords: accommodative dysfunctions, convergence insufficiency, primary schoolchildren, vergence dysfunctions
1. Introduction
More than 80% of perceptual information is oriented and processed through the eyes.1 Therefore, any anomalies in the visual-function system affect children’s cognitive development and educational progress. Vision anomaly is the fourth leading physical disease in the United States and is more common in children.1 The prevalence of nonstrabismic accommodative and vergence dysfunctions shows marked differences depending on the test methods, diagnostic criteria, and characteristics of study populations. But, despite varying statistics, it commonly occurs in schoolchildren.2,3,4,5,6,7,8,9,10 Under the Korean School Health Act, children’s eyesight, such as uncorrected visual acuity and colorvision, is measured during annual school physical examinations. Although decreased visual acuity can be detected during school eye screening, general binocular dys functions, such as blurriness at near workloads, headache, astheno-pia, lacking understanding and concentrating, or repeating the same line, are harder to identify11,12,13 Thus, it is necessary to establish more comprehensive eye and vision examinations mandated in the Korean school system to detect such vision anomalies. In South Korea, the only published population study was conducted in Daegu City, a southeast urban area of South Korea, and according to this study, the prevalence of accommodative and vergence dysfunctions in primary schoolchildren is 35.4% and 34.1%, respectively.14 This study was based on the urban population and socioeconomic diversity, but does not reflect the prevalence of general binocular dysfunctions for the rest of the country. Therefore, this study was conducted to assess the prevalence of general binocular dysfunctions among schoolchildren in a rural area of South Korea.
2. Methods
Hampyeong, with an area of 392 km2, is a small town in South Jeolla province, located in southeast South Korea. Hampyeong was chosen for this study because it is a small rural town in South Jeolla province with a population of 37,998. Also, Hampyeong has a higher population engaged in agriculture than Seoul and Daegu (71%, 0.4%, and 2.9%, respectively). Hampyeong is one of the poorest in education environment. Geographically, Seoul has 559 elementary schools, while Hampyeong has 11 elementary schools and Daegu has 221 primary schools in accordance with their population sizes. Five hundred and eighty-nine participants, 8–13 years old, were recruited from three different primary schools between April 2014 and December 2014. Samples were collected from the schoolchildren who had no history of eye injuries and who were not taking any medications. Also, none of the schoolchildren had any eye diseases, strabismus, or amblyopia that may affect the visual acuity and refractive status.
To detect and properly diagnose accommodation and vergence dysfunctions, it is important to have the following comprehensive tests. The first step was performed by taking a case history that includes full scope of questionnaires about visual symptoms. The second step includes preliminary tests, distance and near visual acuity, distance and near cover test, distance and near point of convergence (fixation stick; Bernell, Mishawaka, USA), distance and near pupillary distance (PD-85; Vitzro, Seoul, South Korea), ocular motility, fusion (Worth 4-dot; Bernell), and stereopsis (Titmus stereo fly; Bernell). Monocular and binocular measurements for distance at 5 m and near visual acuity at 40 cm were determined using an auto chart projector (CCP-3100; Huvitz, Gyeonggi-do, Korea). The third step was assessment of refractive-error examination. Refractive errors were determined by a noncycloplegic autorefractor (HRK-8000A; Huvitz), and subjective refraction was determined using a phoropter (DU-7000; Dongyang, Korea) and auto chart projector (CCP-3100; Huvitz). This was performed by monocular-fogging method with cross cylinder, and followed by binocular balancing to a standard end point of maximum plus for the best visual acuity. The last step was binocular-vision tests. To assess the quality of the general binocular-vision system, the following tests were performed with the subjective refraction in place. The von Graefe technique was used to determine phoria at near and at distance. Positive and negative fusional vergence was measured using the prism-bar method. The accommodative convergence/accommodation ratio was measured using the gradient method. Positive and negative relative accommodation were determined by a phoropter (DU-7000) with auto chart projector (CCP-3100; Huvitz) at 40 cm. Monocular and binocular accommodative facility was measured with a ±2.00 D flipper. The near point of convergence was evaluated by the standard push-up technique. All tests were done three times repeatedly and the average values were analyzed. The results of each of the tests performed were first compared with the norms (Scheiman and Wick15), and then were grouped according to their deviation from the excepted values. The anomalies were than diagnosed following the criteria of Scheiman and Wick,15 which are shown in Tables 1 and 2, where we also have specified the number of signs we used to classify the students under each diagnosis. Participants who revealed symptoms of refractive errors and corrected with prescription glasses were classified as refractive errors, and participants with no symptoms in refraction and binocular tests were classified as normal. All data were entered into a Microsoft Excel database (Microsoft, version 2010). Analyses were conducted, followed by frequencies, percentage, and correlation using SPSS (version 21.0 for Windows; SPSS Inc., Chicago, IL, USA).
Table 1.
Diagnosis criteria for classification of general binocular dysfunctions.
| Convergence insufficiency |
| Symptoms are associated with reading or near tasks |
| Signs need to be present: signs 1–3 & 1 of 4–6 |
| 1 Moderate to high exophoria at near >6Δ |
| 2 Reduced positive fusional vergence at near ≤12/15/4 for blur, break, & recovery (at least 1 of 3) |
| 3 Receded near point of convergence ≥10 cm for break point |
| 4 Low AC/A ratio <3/1 |
| 5 Fails binocular accommodative facility with +2.00 D, ≤2.5 cpm |
| 6 Low NRA ≤1.50 D |
| Basic exophoria |
| Symptoms are associated with distance & near tasks |
| Signs need to be present: signs 1 –2 & 1 of 3–4 |
| 1 Exophoria of approximately equal magnitude at near & distance |
| 2 Reduced positive fusional vergence at distance & near ≤12/15/4 for blur, break, & recovery (at least 1 of 3) |
| 3 Normal AC/A ratio |
| 4 Fails binocular accommodative facility with +2.00 D, ≤2.5 cpm |
| Convergence excess |
| Symptoms are associated with reading or other near tasks |
| Signs need to be present: signs 1 –2 & 1 of 3–4 |
| 1 Significant esophoria at near >2 Δ |
| 2 Reduced negative fusional vergence at near ≤9/17/8 for blur, break, & recovery (at least 1 of 3) |
| 3 High AC/A ratio, >7/1 |
| 4 Fails binocular accommodative facility with +2.00 D, ≤2.5 cpm |
| 5 Low PRA ≤1.25D |
AC/A = accommodative convergence/accommodation ratio; cpm = cycles per minute; NRA = negative relative accommodation; PRA = positive relative accommodation.
Table 2.
Diagnosis criteria for classification of accommodative dysfunctions.
| Accommodative insufficiency |
| Symptoms are associated with reading or other close work |
| Signs need to be present: signs 1–2 & 1 of 3–4 |
| 1 Amplitude of accommodation low for age, push-up accommodative amplitude at least 2 D below Hofstetter’s calculation for minimum amplitude: 15 - 0.25 x age |
| 2 Difficulty clearing -2.00 D with monocular accommodative facility, ≤4.5 cpm |
| 3 Difficulty clearing -2.00 D with binocular accommodative facility, ≤2.5 cpm |
| 4 Low PRA, ≤1.25 D |
| Accommodative infacility |
| Symptoms are associated with reading or other work |
| Signs need to be present: signs 1 –3; 4 may or may not be present |
| 1 Normal amplitude of accommodation |
| 2 Difficulty clearing ±2.00 D with monocular accommodative facility, ≤ 4.5 cpm |
| 3 Difficulty clearing ±2.00 D with binocular accommodative facility, ≤ 2.5 cpm |
| 4 Low PRA & NRA, PRA ≤1.25 D & NRA ≤1.50 D |
| Accommodative excess |
| Symptoms associated with reading or other work |
| Signs need to be present: signs 1–2 & 1 of 3–5 |
| 1 Variable visual acuity findings |
| 2 Variable objective & subjective refraction |
| 3 Difficulty clearing +2.00 D with monocular accommodative facility, ≤4.5 cpm |
| 4 Difficulty clearing +2.00 D with binocular accommodative facility,≤2.5 cpm |
| 5 Low PRA, ≤1.50 D |
AC/A = accommodative convergence/accommodation ratio; cpm = cycles per minute; NRA = negative relative accommodation; PRA = positive relative accommodation.
2.1. Informed consent and ethics approval or procedures
An informed consent was obtained from both the children and their parents after explaining the nature of the tests to be performed, and completed consent forms were obtained from the parents or guardians of all children before the examination. The local administration of the education and school board was contacted to request their cooperation. After securing permission to perform the study, an approval was obtained by the Association of Korean University Ethics Advisory Committee.
3. Results
The prevalence of general binocular dysfunctions is summarized in Table 3. Out of 589 participants, 168 participants (28.5%) presented with accommodative and/or binocular dysfunctions, 289 participants (49%) were classified as normal, and 132 participants (22.4%) were classified as refractive errors. Of the 168 participants with binocular dysfunctions, 53 participants (9.0%) presented with accommodative dysfunctions, 78 participants (13.2%) presented with vergence dysfunctions, and 37 participants (6.3%) had com bined accommodative and vergence dysfunctions.
Table 3.
Prevalence of general binocular and accommodative dysfunctions.
| Classification | N | % |
|---|---|---|
| Accommodative dysfunctions | 53 | 9.0 |
| Accommodative insufficiency | 31 | 5.3 |
| Accommodative infacility | 15 | 2.5 |
| Accommodative excess | 7 | 1.2 |
| Binocular dysfunctions | 78 | 13.2 |
| Convergence insufficiency | 61 | 10.3 |
| Basic exophoria | 6 | 1.0 |
| Convergence excess | 11 | 1.9 |
| AD combination with BD | 37 | 6.3 |
| Convergence insufficiency with accommodative insufficiency | 23 | 3.9 |
| Convergenceinsufficiencywithaccommodative excess | 6 | 1.0 |
| Convergence excess with accommodative insufficiency | 8 | 1.4 |
| Refractive errors | 132 | 22.4 |
| Normal | 289 | 49 |
| Total | 589 | 100 |
AD = accommodative dysfunctions; BD = binocular dysfunctions.
In terms of accommodative dysfunctions, there was a higher incidence of accommodative insufficiency (5.3%) than accommodative infacility (2.5%) and accommodative excess (1.2%). For vergence dysfunctions, the convergence insufficiency was the most prevalent (10.3%) compared to the convergence excess (1.9%) and the basic exophoria (1.0%). Of 37 participants, 23 (3.9%) had combined accommodative insufficiency with convergence insufficiency, and it was more prevalent than the accommodative-excess-and-convergence-insufficiency combination and the accommodative-insufficiency-and-convergence-excess combination.
Table 4 shows the analysis of the prevalence of binocular dysfunctions in seven studies. Besides the authors of the studies, the sample populations, and the number of participants, the prevalence rates of binocular dysfunctions were compared and analyzed. Most of the previous studies showed that accommodative dysfunctions were more prevalent than vergence dysfunctions, excluding the study of Lara et al.16 The highest prevalence of accommodative dysfunctions was presented in the study of Shin et al14 and Garcia et al,17 whereas the highest prevalence of vergence dysfunctions was presented in the study of Shin et al.14 The prevalence rates of accommodative dysfunctions and vergence dysfunctions were higher in Shin et al14 and Garcia et al,17 studies, respectively. This is because, in Shin et al14 and Garcia et al,17 the total participants included only those with binocular dysfunctions, whereas in other studies, the total participants include those with normal, refractive error, and general binocular dysfunctions.
Table 4.
The prevalence of dysfunction in our study (for 168 participants) compared to other studies.
| Study | Age (y) | N | % | ||
|---|---|---|---|---|---|
| AD with BD | AD | BD | |||
| Lara et al16 (2001) | 10–35 | 265 | 22.3 | 9.4 | 12.9 |
| Hokoda21 (1985) | <35 | 119 | 21.0 | 16.8 | 4.2 |
| Montés-Micó19 (2001) | 18–38 | 1679 | 56.3 | 34.6 | 21.7 |
| Porcar & Martinez-Palomera20 (1997) | 19–25 | 65 | 32.3 | 17.0 | 15.3 |
| Scheiman et al18 (1996) | 6 mo–18 y | 2030 | 19.7 | 5.4 | 14.3 |
| Garcia et al17 (2002) | 13–35 | 69 | 72.4 | 44.9 | 27.5 |
| Shin et al14 (2009) | 9–13 | 82 | 69.5 | 35.4 | 34.1 |
| Present study | 8–13 | 168 | 28.5 | 12.0 | 16.5 |
AD = accommodative dysfunctions; BD = binocular dysfunctions.
Fig. 1 shows the Pearson correlation of age, and vergence dys functions indicate that the strength of association between the variables is very high (r = 0.890), and that the correlation coefficient is very highly significantly different from p < 0.05. Also, 79% (0.8902) of the variation in age is explained by vergence dysfunctions (Fig. 2). There is an association between accommodative dysfunctions and vergence dysfunctions that is a strength of correlation (r = 0.969) and that can be highly statistically significant (p < 0.01). The 94% (0.9692) of the accommodative dysfunctions is explained by vergence dysfunctions. However, there was no association between age and accommodative dysfunctions (Fig. 3).
Fig. 1.
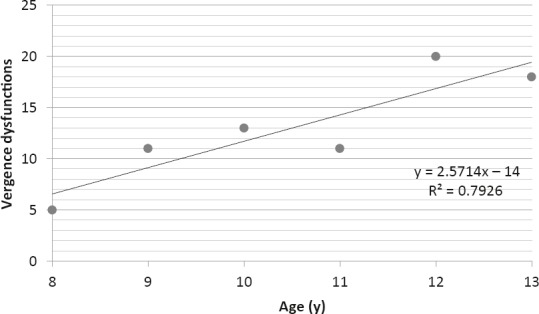
The correlation of age with vergence dysfunctions.
Fig. 2.
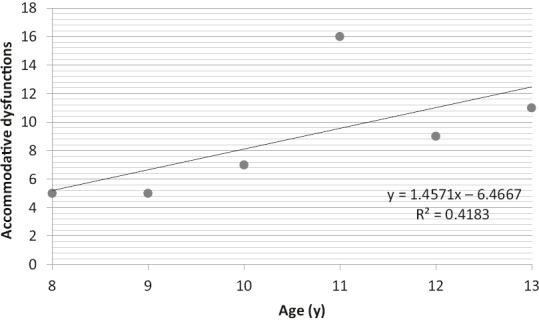
The correlation of age with accommodative dysfunctions.
Fig. 3.
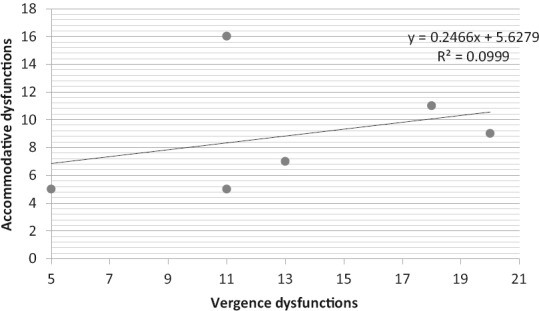
The correlation of vergence dysfunctions with accommodative dysfunctions.
4. Discussion
Nonstrabismic accommodative and vergence dysfunctions are prevalent vision anomalies, which are encountered frequently in a clinical setting. Many studies on the prevalence of accommodative and vergence dysfunctions were done with various diagnostic criteria, special characteristics of the populations, and the study area.16,17,18,19,20 The present study was conducted based on the case history and classification of general binocular dysfunctions according to the data in the literature, although major differences especially, convergence insufficiency (10.3%) was more prevalent than accommodative insufficiency (5.3%).
We used the same diagnostic criteria as in the studies of Lara et al16 and Porcar and Martinez-Palomera.20 However, the prevalence of general binocular dysfunctions was different because of the characteristics of the study participants. In Porcar and Martinez-Palomera’s20 study, the participants were optometry-school stu dents who were required to do a significant amount of near workloads. Thus, Porcar and Martinez-Palomera’s20 study presented higher prevalence of accommodative and vergence dys functions (17% and 15.3%, respectively) than Lara et al’s16 study, in which their participants were not a student group.
There are studies with participant groups of primary-school students. According to Shin et al,14 the prevalence of accommodative dysfunctions was 35.4% and the prevalence of vergence dys functions was 34.1% among the 9–13-year-old primary-school students. In Shin et al’s14 study of 114 children, 82 children (71.9%) were symptomatic with general binocular dysfunctions, and the prevalence rate was significantly high. Interestingly, both Shin et al’s14 study and our study were done in South Korea, but Shin et al’s14 study was based on an urban area (Daegu City), whereas our study was based on a rural area (Hampyeong). Although our study sample size was approximately two times larger than Shin et al’s,14 their prevalence rate of general binocular dysfunctions was significantly higher than ours. Because children from an urban area spend more time in study and less time in outdoor activities, their required near workloads were higher, and this can lead to a significantly high prevalence rate of binocular dysfunctions. Even though our study sample was larger, the prevalence rate of general binocular dysfunctions was relatively lower.
In our study, the prevalence of general binocular dysfunctions was distinguished from other studies. Numerous study results agreed that accommodative dysfunctions were more prevalent than vergence dysfunctions,14,17,19,20,21 whereas in the present study, the prevalence of vergence dysfunctions was higher. For example, in Hokoda’s21 study, the prevalence of accommodative dysfunctions was significantly higher than that of vergence dysfunctions, particularly accommodative insufficiency was the most prevalent. In this particular study, 42.9% of the patients had jobs with near workloads, and 39.5% of the patients were students with near workloads. Therefore, near workloads can play a role in increased binocular dysfunctions. In addition, in Montés-Micé‘s19 study with a significant number of participants, accommodative dysfunctions were more prevalent than vergence dysfunctions. However, in our study, vergence dysfunctions were more prevalent than accommodative dysfunctions; particularly, convergence insufficiency was the most prevalent, followed by accommodative insufficiency (10.3% and 5.3%, respectively). In addition, the prevalence of the combination of convergence insufficiency with accommodative insufficiency was significant (3.9%). Similar to our results, in Shin et al’s14 study, convergence insufficiency was the most prevalent, followed by accommodative insufficiency (28% and 18.3%, respectively). Our study, as well as Shin et al’s14 and Hokoda’s21 studies, presents the relationship between general binocular dysfunctions and amount of near workloads.
In this study, vergence dysfunctions, particularly convergence insufficiency, were the most prevalent, because the participants of the study were primary schoolchildren who are required an extensive amount of near workloads during studying and learning. Recent studies22,23,24,25,26,27,28,29 agreed with our results. These findings suggest that, in schoolchildren, it is important to give a thorough eye examination, including tests for binocular vision, to detect general binocular dysfunctions. Also, it is necessary to have a thorough eye examination to find an appropriate treatment plan for symptomatic participants to improve their vision efficiency and daily lives. Although, in our study, the prevalence of general binocular dysfunctions among primary schoolchildren was limitedly focused, it would be useful to study the relationship prevalence of general binocular dysfunctions and academic achievement in a rural area of South Korea in future studies.
Nonstrabismic accommodative and vergence dysfunctions commonly occur among primary schoolchildren. The prevalence of general binocular dysfunctions in a rural area among Korean schoolchildren was 28.5%. We have also shown a high percentage of vergence dysfunctions compared to accommodative dysfunctions, with convergence insufficiency (10.3%) and accommodative insufficiency (5.3%) being the most prevalent dysfunctions. Therefore, accommodative and vergence insufficiency are more common dysfunctions in the rural area of South Korea. Understanding the prevalence of general binocular dysfunctions in Korean school children would be useful who are interesting the prevalence of general binocular dysfunctions. Future studies should compare general binocular dysfunctions in Korean populations of all ages in order to gain a better understanding of their prevalence.
Footnotes
Conflicts of interest: None of the authors have a conflict of interest about the paper. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
- 1.Borsting E, Rouse MW, Deland PN, et al. Association of symptoms and convergence and accommodative insufficiency in school-age children. Optometry. 2003;74:25–34. [PubMed] [Google Scholar]
- 2.Scheiman M, Mitchell GL, Cotter S. A randomized clinical trial of treatments for convergence insufficiency in children. Arch Ophthalmol. 2005;123:14–24. doi: 10.1001/archopht.123.1.14. [DOI] [PubMed] [Google Scholar]
- 3.Borsting E, Rouse MW, Deland P. Prospective comparison of convergence insufficiency and normal binocular children on CIRS symptom surveys. Convergence Insufficiency and Reading Study (CIRS) group. Optom Vis Sci. 1999;76:221–228. doi: 10.1097/00006324-199904000-00025. [DOI] [PubMed] [Google Scholar]
- 4.Borsting EJ, Rouse MW, Mitchell GL. Validity and reliability of the revised convergence insufficiency symptom survey in children aged 9 to 18 years. Optom Vis Sci. 2003;80:832–838. doi: 10.1097/00006324-200312000-00014. [DOI] [PubMed] [Google Scholar]
- 5.Atzmon D, Nemet P, Ishay A, Karni E. A randomized prospective masked and matched comparative study of orthoptic treatment versus conventional reading tutoring treatment for reading disabilities in 62 children. Binocul Vis Eye Muscle Surg. 1993;8:91–106. [Google Scholar]
- 6.Marran LF, De Land PN, Nguyen AL. Accommodative insufficiency is the pri mary source of symptoms in children diagnosed with convergence insufficiency. Optom Vis Sci. 2006;83:281–289. doi: 10.1097/01.opx.0000216097.78951.7b. [DOI] [PubMed] [Google Scholar]
- 7.Daum KM. Accommodative dysfunction. Doc Ophthalmol. 1983;55:177–198. doi: 10.1007/BF00140808. [DOI] [PubMed] [Google Scholar]
- 8.Rouse MW. Management of binocular anomalies: efficacy of vision therapy in the treatment of accommodative deficiencies. Am J Optom Physiol Opt. 1987;64:415–420. [PubMed] [Google Scholar]
- 9.Hennessey D, Iosue RA, Rouse MW. Relation of symptoms to accommoda tive infacility of school-aged children. Am J Optom Physiol Opt. 1984;61:177–183. doi: 10.1097/00006324-198403000-00005. [DOI] [PubMed] [Google Scholar]
- 10.Sterner B, Abrahamsson M, Sjostrom A. The effects of accommodative facility training on a group of children with impaired relative accommodation–a comparison between dioptric treatment and sham treatment. Ophthalmic Physiol Opt. 2001;21:470–476. doi: 10.1046/j.1475-1313.2001.00615.x. [DOI] [PubMed] [Google Scholar]
- 11.Cacho-Martinez P, Garcia-Munoz A, Ruiz-Cantero MT. Do we really know the prevalence of accommodative and nonstrabismic binocular dysfunctions. J Optom? 2010;3:185–197. [Google Scholar]
- 12.Dusek WA, Pierscionek BK, McClelland JF. An evaluation of clinical treatment of convergence insufficiency for children with reading difficulties. BMC Oph-thalmol. 2011;11:11–21. doi: 10.1186/1471-2415-11-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Barnhardt C, Cotter SA, Mitchell GL, Scheirman M, Kulp MT CITT Study Group. Symptoms in children with convergence insufficiency: before and after treatment. Optom Vis Sci. 2012;89:1512–1520. doi: 10.1097/OPX.0b013e318269c8f9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Shin HS, Park SC, Park CM. Relationship between accommodative and vergence dysfunctions and academic achievement for primary school children. Ophthalmic Physiol Opt. 2009;2:615–624. doi: 10.1111/j.1475-1313.2009.00684.x. [DOI] [PubMed] [Google Scholar]
- 15.Scheiman M, Wick B. Clinical Management of Binocular Vision: Heterophoric, Accommodative and Eye Movement Disorders Chapter 1. third edition. Philadelphia, PA: Lippincott Williams & Wilkins; 2002. pp. 3–52. [Google Scholar]
- 16.Lara F, Cacho P, Garcia A, Megias R. General binocular disorders: prevalence in a clinic population. Ophthalmic Physiol Opt. 2001;21:70–74. doi: 10.1046/j.1475-1313.2001.00540.x. [DOI] [PubMed] [Google Scholar]
- 17.Garcia A, Cacho-Martinez P, Lara F. Evaluating relative accommodations in general binocular dysfunctions. Optom Vis Sci. 2002;79:779–787. doi: 10.1097/00006324-200212000-00010. [DOI] [PubMed] [Google Scholar]
- 18.Scheiman M, Gallaway M, Coulter R, et al. Prevalence of vision and ocular disease conditions in a clinical pediatric population. J Am Optom Assoc. 1996;67:193–202. [PubMed] [Google Scholar]
- 19.Montés-Micé R. Prevalence of general dysfunctions in binocular vision. Ann Ophthalmol. 2001;33:205–208. [Google Scholar]
- 20.Porcar E, Martinez-Palomera A. Prevalence of general binocular dysfunctions in a population of university students. Optom Vis Sci. 1997;74:111–113. doi: 10.1097/00006324-199702000-00023. [DOI] [PubMed] [Google Scholar]
- 21.Hokoda SC. General binocular dysfunctions in an urban optometry clinic. JAm Optom Assoc. 1985;56:560–562. [PubMed] [Google Scholar]
- 22.Hoseini-Yazdi SH, Yekta A, Nouri H, Heravian J, Ostadimoghaddam H, Khabazkhoob M. Frequency of convergence and accommodative disorders in a clinical population of Mashhad, Iran. Strabismus. 2015;23:22–29. doi: 10.3109/09273972.2014.1002622. [DOI] [PubMed] [Google Scholar]
- 23.Borsting E, Mitchell GL, Kulp MT, et al. Improvement in academic behaviors following successful treatment of convergence insufficiency. Optom Vis Sci. 2012;89:12–18. doi: 10.1097/OPX.0b013e318238ffc3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Pang U, Teitelbaum B, Krall J. Factors associated with base-in prism treatment outcomes for convergence insufficiency in symptomatic presbyopes. Clin Exp Optom. 2012;95:192–197. doi: 10.1111/j.1444-0938.2011.00693.x. [DOI] [PubMed] [Google Scholar]
- 25.Scheiman M, Cotter S, Kulp MT, et al. Treatment of accommodative dysfunction in children: results from a randomized clinical trial. Optom Vis Sci. 2011;88:1343–1352. doi: 10.1097/OPX.0b013e31822f4d7c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Rogers DL, Serna A, McGregor ML, Golden RP, Bremer DL, Rogers GL. Treatment of symptomatic convergence insufficiency with a home-based computer orthoptic exercise program. J A APOS. 2011;15:140–143. doi: 10.1016/j.jaapos.2010.11.023. [DOI] [PubMed] [Google Scholar]
- 27.Alvarez TL, Vicci VR, Alkan Y, et al. Vision therapy in adults with convergence insufficiency: clinical and functional magnetic resonance imaging measures. Optom Vis Sci. 2010;87:985–1002. doi: 10.1097/OPX.0b013e3181fef1aa. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Scheiman M, Kulp MT, Cotter S, et al. Vision therapy/orthoptics for symp tomatic convergence insufficiency in children: treatment kinetics. Optom Vis Sci. 2010;87:593–603. doi: 10.1097/OPX.0b013e3181e61bad. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Shin HS, Park SC, Maples WC. Effectiveness of vision therapy for convergence dysfunctions and long-term stability after vision therapy. Ophthalmic Physiol Opt. 2011;31:180–189. doi: 10.1111/j.1475-1313.2011.00821.x. [DOI] [PubMed] [Google Scholar]