

Abstract
Background:
Anterior shoulder instability can be a disabling condition for the young athlete; however, the best surgical treatment remains controversial. Traditionally, anterior shoulder instability was treated with open stabilization. More recently, arthroscopic repair of the Bankart injury with suture anchor fixation has become an accepted technique.
Hypothesis:
No systematic reviews have compared the rate of return to play following arthroscopic Bankart repair with suture anchor fixation with the Bristow-Latarjet procedure and open stabilization. We hypothesized that the rate of return to play will be similar regardless of surgical technique.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
We performed a systematic review and meta-analysis focused on return to play following shoulder stabilization. Inclusion criteria included studies in English that reported on rate of return to play and clinical outcomes following primary arthroscopic Bankart repair with suture anchors, the Latarjet procedure, or open stabilization. Statistical analyses included Student t tests and analyses of variance.
Results:
Sixteen papers reporting on 1036 patients were included. A total of 545 patients underwent arthroscopic Bankart repair with suture anchors, 353 with the Latarjet procedure, and 138 with open repair. No significant difference was found in patient demographic data among the studies. Patients returned to sport at the same level of play (preinjury level) more consistently following arthroscopic Bankart repair (71%) or the Latarjet procedure (73%) than open stabilization (66%) (P < .05). Return to play at any level and postoperative Rowe scores were not significantly different among studies. Recurrent dislocation was significantly less following the Latarjet procedure (3.5%) than after arthroscopic Bankart repair (6.6%) or open stabilization (6.7%) (P < .05).
Conclusion:
This systematic review demonstrates a greater rate of return to play at the preinjury level following arthroscopic Bankart repair and the Latarjet procedure than open stabilization. Despite this difference, >65% of all treated athletes returned to sport at their preinjury levels, with other outcome measures being similar among the treatment groups. Therefore, arthroscopic Bankart repair, the Latarjet procedure, and open stabilization remain good surgical options in the treatment of the athlete with anterior shoulder instability.
Keywords: return to play, return to sport, shoulder stabilization, Bankart, Latarjet
Anterior shoulder instability can be a disabling condition for the young athlete. Treatment of the athlete with shoulder instability continues to evolve and remains a topic of debate in the literature. The ultimate goal of many of these patients, especially younger ones, is to return to the activities and sports in which they were participating prior to injury.
Unidirectional anterior instability is most commonly caused by sequelae of traumatic anterior shoulder dislocation, which can tear the anterior labrum and cause injury to the anterior capsule and/or glenoid.21 Anterior shoulder instability, particularly in older individuals, can oftentimes be satisfactorily treated nonoperatively through physical therapy and activity modification.20 However, for cases of recurrent dislocations among younger patients, for patients participating in collision/contact sports, or for those patients otherwise at risk for ongoing instability, surgery is typically indicated to prevent continued instability.2,20,29
Although open stabilization has been regarded as the gold standard in the surgical management of anterior shoulder instability, arthroscopic repair of the Bankart injury with suture anchor fixation (arthroscopic Bankart procedure) has become an accepted and primary treatment option.20 Owens et al24 highlighted the increasing utilization of arthroscopic techniques in the treatment of shoulder instability, with a nearly 20% increase in arthroscopic procedures over a 5-year period. Open stabilization involves direct open repair of the injury to the capsule. Another popular procedure, the Bristow-Latarjet procedure, involves transfer of the coracoid process to the anterior rim of the glenoid to act as a bone block preventing anterior translation and subsequent dislocation of the humeral head from the glenoid.2,18,19 This improves the inherent stability of the glenohumeral joint because of the increased excursion required to dislocate, and it provides an anteroinferior soft tissue sling.27 The arthroscopic Bankart repair improves stability by directly tightening the anterior capsule as well as repairing the anterior labrum into a so-called anteroinferior bumper.33
In the literature to date, there are data suggesting that arthroscopic and open techniques, including open capsular repair and reconstruction and the Latarjet procedure for addressing anterior shoulder instability, are safe and effective, with few complications and low rates of recurrent instability regardless of the technique.5,23 The focus of the current literature comparing these techniques, however, has largely been to investigate any difference in rates of redislocation or need for revision surgery. To our knowledge, no systematic reviews have examined the rate of return to play following arthroscopic Bankart repair with suture anchor fixation as compared with open stabilization and the Latarjet procedure. Given the many smaller series evaluating these techniques, this study is ideal for a systematic review to provide additional clinical information to surgeons and patients. It was our aim to describe rates of return to sport in the arthroscopic and open variants of surgical correction of anterior shoulder instability. We describe return to the same and lower level of play, as well as time to return to play. Our hypothesis was that there would be no difference in rates of return to play among these 3 common surgical techniques.
Methods
A systematic review and meta-analysis of the literature were performed following the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-analyses).22 A protocol was established stating the goal of the review as well as the search strategies.
Search Strategy
An electronic search of the literature was performed in MEDLINE via PubMed, Scopus, Embase, and the Cochrane Library of Systematic Reviews. Searches included the keywords “return to play/sport,” “shoulder stabilization,” “Bankart repair,” “Latarjet,” and “open stabilization.” The final search was performed on November 1, 2016. The references were checked for each article, and a manual search of related articles was performed.
Selection Criteria
Inclusion criteria were studies in the English language (levels of evidence 1-4) that evaluated return to sport and clinical outcomes after treatment of traumatic shoulder instability. Surgical treatments included primary arthroscopic capsule-labral repair (the arthroscopic Bankart procedure) with suture anchors, primary Latarjet procedure, and primary open stabilization (open capsular repair or the open Bankart procedure). Exclusion criteria were reviews of the literature, expert opinions, nonclinical studies, case reports, and clinical studies that did not assess return to play. Associated lesions (superior labral anterior-posterior lesions, rotator cuff tears) were not exclusion criteria. Two authors selected the abstracts and then analyzed them separately. When the abstract seemed pertinent, the article was analyzed.
Data Extraction and Synthesis
Data extraction was performed according to a standardized form developed prior to data search. It included (1) characteristics of the study (design, year, number of patients, and level of evidence), (2) characteristics of the study participants (age, sex, level of sport, sports played, dominant shoulder), (3) characteristics of pathology (number of times dislocated, dislocation during sport), (4) treatment technique (arthroscopic Bankart repair with suture anchors, Latarjet procedure, or open stabilization), and (5) clinical outcome measures (rate of return to sport at preinjury level or lower, time to return to play, Rowe scores).
Data were analyzed with PSPP (GNU Project) statistical data software. The main judgment criterion was whether a study participant was able to return to sport following surgery. Subgroup analysis was also performed assessing whether the participant was able to return to preinjury level of sport, as well as time to return to sport. Redislocation rate following surgery was analyzed. Rowe score was also analyzed as a self-reported clinical outcome measure.
Bivariate data were analyzed with a Student t test, while 1-way analysis of variance (ANOVA) was used to analyze differences among the means of the 3 repair techniques. P = .05 was considered statistically significant in all tests.
Results
Initial search, including studies reporting on outcomes following surgical stabilization, yielded 1756 studies (Figure 1). Sixty-three of these records reported on return to play following surgical stabilization. After removal of duplicate studies, 47 studies remained for abstract review. An additional 26 studies were found to be nonpertinent and were thus removed following abstract review. The remaining 21 studies underwent full study review. Five studies were removed, leaving 16 papers remaining for inclusion in quantitative and qualitative synthesis (Table 1).
Figure 1.
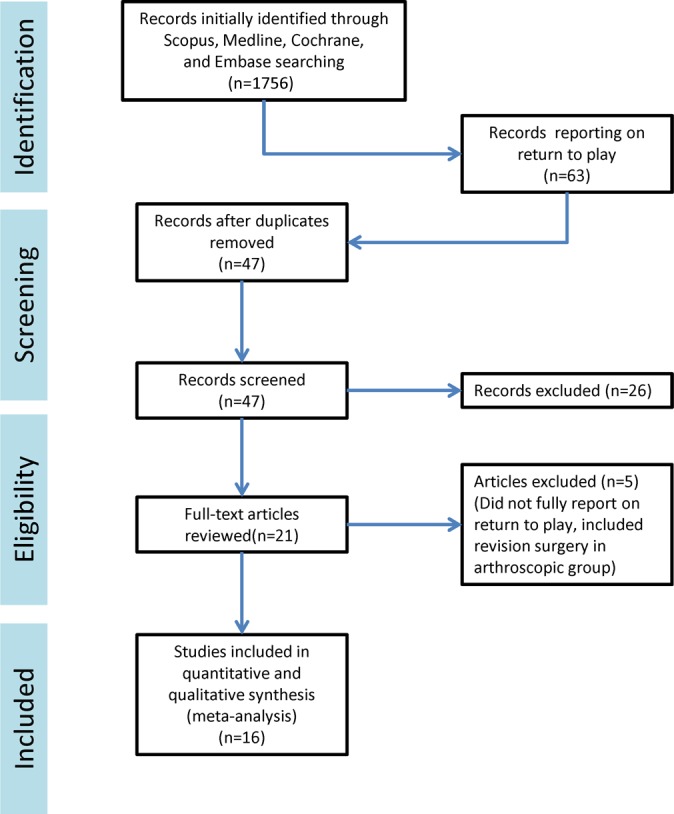
Systematic review flowchart.
TABLE 1.
Studies Meeting Inclusion Criteria for Meta-analysisa
| Study Name | First Author | Year | LOE | No. of Patients | Male | Female | |
|---|---|---|---|---|---|---|---|
| Open repair | |||||||
| “Neer Modification of Open Bankart Procedure: What Are the Rates of Recurrent Instability, Functional Outcome, and Arthritis?” | Boileau7 | 2012 | 4 | 64 | 46 | 18 | |
| “Long-term Results With Bankart Procedure: A 26-Year Follow-up Study of 50 Cases” | Fabre11 | 2010 | 4 | 49 | 46 | 3 | |
| “Modified Bankart Procedure for Recurrent Anterior Dislocation and Subluxation of the Shoulder in Athletes” | Takeda30 | 1998 | 4 | 25 | 21 | 4 | |
| Latarjet procedure | |||||||
| “Arthroscopic Bankart Repair Versus Open Bristow-Latarjet for Shoulder Instability: A Matched-Pair Multicenter Study Focused on Return to Sport” | Blonna5 | 2016 | 3 | 30 | 26 | 4 | |
| “The Open Latarjet Procedure Is More Reliable in Terms of Shoulder Stability Than Arthroscopic Bankart Repair” | Bessiere3 | 2014 | 3 | 93 | 89 | 4 | |
| “Anterior Shoulder Stabilization by Bristow-Latarjet Procedure in Athletes: Return-to-Sport and Functional Outcomes at Minimum 2-Year Follow-up” | Beranger2 | 2016 | 4 | 47 | 46 | 1 | |
| “Evaluation of Functional Outcomes and Complications Following Modified Latarjet Reconstruction in Athletes With Anterior Shoulder Instability” | Colegate-Stone9 | 2015 | 4 | 56 | 50 | 6 | |
| “Bristow-Latarjet Repairs for Anterior Instability of the Shoulder: Clinical and Radiographic Results at Mean 8.2 Years Follow-up” | Dossim10 | 2008 | 4 | 93 | 84 | 9 | |
| “The Latarjet-Patte Procedure for Recurrent Anterior Shoulder Instability in Contact Athletes” | Joshi16 | 2015 | 4 | 34 | 34 | 0 | |
| ASA repair | |||||||
| “Arthroscopic Bankart Repair Versus Open Bristow-Latarjet for Shoulder Instability: A Matched-Pair Multicenter Study Focused on Return to Sport” | Blonna5 | 2016 | 3 | 30 | 26 | 4 | |
| “The Open Latarjet Procedure Is More Reliable in Terms of Shoulder Stability Than Arthroscopic Bankart Repair” | Bessiere3 | 2014 | 3 | 93 | 85 | 8 | |
| “Arthroscopic Bankart Shoulder Stabilization in Athletes: Return to Sports and Functional Outcomes” | Gerometta12 | 2016 | 4 | 46 | 36 | 10 | |
| “Return to Sport Following Arthroscopic Anterior Shoulder Stabilization: High Outcome Scores Despite Moderate Rate of Return to Play” | Kraeutler17 | 2013 | 4 | 35 | NR | NR | |
| “Return to Play After Shoulder Instability Surgery in National Collegiate Athletic Association Division I Intercollegiate Football” Athletes | Robins28 | 2017 | 4 | 153 | 153 | 0 | |
| “Sporting Activity After Arthroscopic Bankart Repair for Chronic Glenohumeral Instability” | Plath26 | 2015 | 4 | 66 | 46 | 20 | |
| “Mid-term Results of Arthroscopic Bankart Repair: A Review of 31 Cases” | Tordjman32 | 2016 | 4 | 30 | 17 | 13 | |
| “Arthroscopic Suture Anchor Fixation of Bony Bankart Lesions: Clinical Outcome, Magnetic Resonance Imaging Results, and Return to Sports” | Plath25 | 2015 | 4 | 45 | 36 | 9 | |
| “Shoulder Sport-Specific Impairments After Arthroscopic Bankart Repair: A Prospective Longitudinal Assessment” | Stein29 | 2011 | 3 | 47 | 39 | 8 | |
aASA, arthroscopic suture anchor; LOE, level of evidence; NR, not reported.
Sixteen papers were reviewed, including 1036 patients. Nine studies were identified that described return to sport after arthroscopic shoulder stabilization. These studies included a total of 545 patients (438 male, 72 female, 35 not reported). Mean age at surgery was 27.6 years. Length of follow-up was highly variable, ranging from 32 to 82 months. A majority of the patients (58%) underwent arthroscopic Bankart repair in the lateral decubitus position. Six studies were identified that described return to sport after the Latarjet procedure. These studies included a total of 353 patients (329 male, 24 female). Mean age at surgery was 26.5 years. Three studies were identified that described return to sport after open shoulder stabilization procedure. These studies included a total of 138 patients (113 male, 25 female) and 150 shoulders. Mean age at time of surgery was 24 years. Length of follow-up was again variable among the studies, with a range from 6 months to 28 years. No significant difference was found among the demographics of these groups (Table 2).
TABLE 2.
Demographic Data
| Arthroscopic Suture Anchor Repair | Latarjet | Open Repair | |
|---|---|---|---|
| Male, No. (%) | 438 (80) | 329 (93) | 113 (82) |
| Age at time of surgery, y, mean | 28 | 26.5 | 24 |
| Dominant shoulder, % | 57 | 50.20 | 46.60 |
| Previous dislocations, No., mean | 9 | 20 | 19 |
A 1-way ANOVA was conducted to compare the return-to-sport rate at the preinjury level among patients who underwent Latarjet stabilization, open repair, and arthroscopic suture anchor stabilization. Patients returned to their desired sport at the same level of play (preinjury level) more consistently following arthroscopic Bankart repair with suture anchors (71%) or the Latarjet procedure (73%) than those treated with open stabilization (66%) (P < .05). Arthroscopic and Latarjet procedures were found to be associated with a higher rate of return to play at the same level when compared with open stabilization (P < .05) (Table 3). However, return to sport at any level was not significantly different among the groups. The time to return to sport was longer following arthroscopic Bankart repair with suture anchors (8 months on average in 2 studies reporting 81 patient outcomes) versus Latarjet and open stabilization (6 months each—3 Latarjet studies reporting 137 patients and 3 open studies reporting 138 patients) (P < .05).
TABLE 3.
Rate of Return to Sporta
| Arthroscopic Suture Anchor Repair | Latarjet Procedure | Open Repair | |
|---|---|---|---|
| Same level, No. (%) | 387 (71) | 258 (73) | 97 (66) |
| Any level, % | 90.5 | NR | 89 |
| Time to return, mo, mean | 6.1 | 5.3 | 8.2 |
aSignificant differences are denoted in bold (P < .05). NR, not reported.
The Rowe score was the most commonly reported patient outcome measure among the papers evaluated. All 3 open stabilization studies reported Rowe scores, and the mean score was 86 postoperatively. Three arthroscopic suture anchor studies (185 patients) reported postoperative Rowe scores; the mean score was 79.5. Two Latarjet studies (127 patients) reported postoperative Rowe scores; the mean score was 82.0. These scores were not found to be statistically different per ANOVA with post hoc analysis.
Recurrent dislocation rates were reported in 7 arthroscopic suture anchor studies (545 shoulders), 5 Latarjet studies (353 shoulders), and all 3 open repair (148 shoulders). ANOVA testing was performed on these results, as well as post hoc analysis. Recurrent dislocation was significantly less likely after Latarjet stabilization (3.5%) as compared with arthroscopic Bankart repair (6.6%) and open stabilization (6.7%) (P < .05).
Discussion
This systematic review and meta-analysis demonstrated no statistically significant difference in rate of return to play following arthroscopic Bankart repair, Latarjet procedure, and open stabilization. No differences were found among the groups when analysis included patients returning to all levels of sport, including lower level than that prior to injury. Rowe scores were not statistically significant different among the 3 treatment options analyzed. The Latarjet procedure demonstrated a lower overall redislocation rate in comparison with arthroscopic Bankart repair utilizing suture anchors and open stabilization.
As surgical stabilization is becoming a more commonly performed procedure for the young active patient with a history of traumatic glenohumeral dislocation,24 the rate of return to play is an increasingly important outcome measure. Arthroscopic Bankart repair has become the treatment of choice for many surgeons in the setting of minimal glenoid bone loss.1,13,15,23,32 Despite this fact, the current literature demonstrates wide variation with regard to the comparison of arthroscopic stabilization with open stabilization.3–5,8 Few studies have compared the Latarjet procedure with arthroscopic Bankart repair with suture anchors, and no studies to date have analyzed the rates of return to play among the 3 most common stabilization procedures, possibly owing to the fact that there are different indications for each procedure for many surgeons.
Arthroscopic Bankart repair has demonstrated an excellent rate of return to sport to the preinjury athletic level.14,31–33 Blonna and colleagues,5 for example, demonstrated a 90% return to preinjury level among their 30 patients who underwent arthroscopic Bankart repair. A 94% rate of return to play at all levels was reported by Gerometta et al12 following arthroscopic stabilization in 46 athletes. Some studies have suggested that the Latarjet procedure has a higher rate of return to play for contact athletes (eg, rugby and hockey).14 Open stabilization was the gold standard treatment prior to the development of arthroscopic techniques. Fabre and colleagues11 demonstrated outstanding long-term results following open stabilization, with an 82% return to the same level of sport. More recent studies, however, have demonstrated less enthusiastic results. Our meta-analysis demonstrated no difference in the rate of return to play with all techniques, especially at any level of sport.
Several outcome measures are typically reported in studies of anterior stabilization surgery, including Rowe score, 12-Item Short Form Survey scores, and American Shoulder and Elbow Surgeons scores. Our systematic review demonstrated wide variation in outcome scores reported. Most athletes define surgical success as ability to return to sport at the preinjury level, with partial success being defined as return to some level of sport.5,6,29 This holds especially true at the higher levels of competition. For these reasons, we focused our study on the rate of return to play as well as the redislocation rate. Although some scores have been validated (eg, Subjective Shoulder Value–Sport),6 the variation in outcome measures makes it difficult to compare among multiple studies.
Redislocation rates were similar among the 3 procedures assessed in our study, with the Latarjet procedure slightly outperforming arthroscopic suture anchor and open stabilization. This is consistent with most of the currently published literature,20,23 although wide variation in postoperative redislocation rates exists. Tordjman and colleagues32 reported a redislocation rate of 16% following arthroscopic stabilization, while other studies reported much lower incidence of recurrent instability.12,25 Despite these similar dislocation rates, the rate of return to play at the preinjury level was lower among those patients who underwent open stabilization. This suggests that other factors, such as shoulder stiffness and loss of motion or strength with open stabilization, may play a role in return to sport, especially at the collegiate or professional level. These factors should continue to be examined in the future.
Given its excellent rate of return to play, especially at a high level of competition with limited complications, arthroscopic Bankart procedure should be considered an option for athletes with recurrent shoulder instability. The Latarjet procedure and open stabilization remain options for the modern-day athlete.
Limitations of this study include the inherent limitations of a systematic review and meta-analysis, including multiple and inconsistent outcome measures reported in the individual studies. Furthermore, the type of sport involved was inconsistently reported in the included studies. The major strength of this study is the large number of patients included, especially for arthroscopic Bankart repair utilizing only suture anchor fixation. Also, this is the first study to date to compare rates of return to play among the 3 most prevalent stabilization procedures. Our outcomes are consistent with published data but elucidate the rate of return to play as well as time to return with current techniques.
Conclusion
This systematic review demonstrated no overall difference in the rate of return to play, as well as patient-reported outcomes, following arthroscopic Bankart repair, the Latarjet procedure, and open stabilization. Despite this difference, >65% of all treated athletes returned to sport at their preinjury levels, with other outcome measures being similar among the treatment groups. Therefore, arthroscopic Bankart repair, the Latarjet procedure, and open stabilization remain good surgical options in the treatment of the athlete with anterior shoulder instability.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
References
- 1. Bacilla P, Field LD, Savoie FH., 3rd Arthroscopic Bankart repair in a high demand patient population. Arthroscopy. 1997;13:51–60. [DOI] [PubMed] [Google Scholar]
- 2. Beranger JS, Klouche S, Bauer T, Demoures T, Hardy P. Anterior shoulder stabilization by Bristow-Latarjet procedure in athletes: return-to-sport and functional outcomes at minimum 2-year follow-up. Eur J Orthop Surg Traumatol. 2016;26:277–282. [DOI] [PubMed] [Google Scholar]
- 3. Bessiere C, Trojani C, Carles M, Mehta SS, Boileau P. The open Latarjet procedure is more reliable in terms of shoulder stability than arthroscopic bankart repair. Clin Orthop Relat Res. 2014;472:2345–2351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Bessiere C, Trojani C, Pelegri C, Carles M, Boileau P. Coracoid bone block versus arthroscopic Bankart repair: a comparative paired study with 5-year follow-up. Orthop Traumatol Surg Res. 2013;99:123–130. [DOI] [PubMed] [Google Scholar]
- 5. Blonna D, Bellato E, Caranzano F, Assom M, Rossi R, Castoldi F. Arthroscopic Bankart repair versus open Bristow-Latarjet for shoulder instability: a matched-pair multicenter study focused on return to sport. Am J Sports Med. 2016;44:3198–3205. [DOI] [PubMed] [Google Scholar]
- 6. Blonna D, Bellato E, Caranzano F, et al. Validity and reliability of the SPORTS score for shoulder instability. Joints. 2014;2:59–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Boileau P, Fourati E, Bicknell R. Neer modification of open Bankart procedure: what are the rates of recurrent instability, functional outcome, and arthritis? Clin Orthop Relat Res. 2012;470:2554–2260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Cole BJ, Warner JJ. Arthroscopic versus open Bankart repair for traumatic anterior shoulder instability. Clin Sports Med. 2000;19:19–48. [DOI] [PubMed] [Google Scholar]
- 9. Colegate-Stone TJ, van der Watt C, de Beer JF. Evaluation of functional outcomes and complications following modified Latarjet reconstruction in athletes with anterior shoulder instability. Shoulder Elbow. 2015;7:168–173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Dossim A, Abalo A, Dosseh E, Songne B, Ayite A, Gnandi-Pio F. Bristow-Latarjet repairs for anterior instability of the shoulder: clinical and radiographic results at mean 8.2 years follow-up [in French]. Chir Main. 2008;27:26–30. [DOI] [PubMed] [Google Scholar]
- 11. Fabre T, Abi-Chahla ML, Billaud A, Geneste M, Durandeau A. Long-term results with Bankart procedure: a 26-year follow-up study of 50 cases. J Shoulder Elbow Surg. 2010;19:318–323. [DOI] [PubMed] [Google Scholar]
- 12. Gerometta A, Rosso C, Klouche S, Hardy P. Arthroscopic Bankart shoulder stabilization in athletes: return to sports and functional outcomes. Knee Surg Sports Traumatol Arthrosc. 2016;24:1877–1883. [DOI] [PubMed] [Google Scholar]
- 13. Harris JD, Gupta AK, Mall NA, et al. Long-term outcomes after Bankart shoulder stabilization. Arthroscopy. 2013;29:920–933. [DOI] [PubMed] [Google Scholar]
- 14. Hovelius L, Vikerfors O, Olofsson A, Svensson O, Rahme H. Bristow-Latarjet and Bankart: a comparative study of shoulder stabilization in 185 shoulders during a seventeen-year follow-up. J Shoulder Elbow Surg. 2011;20:1095–1101. [DOI] [PubMed] [Google Scholar]
- 15. Hovelius LK, Sandstrom BC, Rosmark DL, Saebo M, Sundgren KH, Malmqvist BG. Long-term results with the Bankart and Bristow-Latarjet procedures: recurrent shoulder instability and arthropathy. J Shoulder Elbow Surg. 2001;10:445–452. [DOI] [PubMed] [Google Scholar]
- 16. Joshi MA, Young AA, Balestro JC, Walch G. The Latarjet-Patte procedure for recurrent anterior shoulder instability in contact athletes. Orthop Clin North Am. 2015;46:105–111. [DOI] [PubMed] [Google Scholar]
- 17. Kraeutler JA, Aberlee N II, Long C, McCarty E. Return to sport following arthroscopic anterior shoulder stabilization: high outcome scores despite moderate rate of return to play. Orthop J Sports Med. 2013;1(suppl 4):2325967113S00098. [Google Scholar]
- 18. Lafosse L, Boyle S. Arthroscopic Latarjet procedure. J Shoulder Elbow Surg. 2010;19:2–12. [DOI] [PubMed] [Google Scholar]
- 19. Latarjet M. Technic of coracoid preglenoid arthroereisis in the treatment of recurrent dislocation of the shoulder [in French]. Lyon Chir. 1958;54:604–607. [PubMed] [Google Scholar]
- 20. Levy DM, Cole BJ, Bach BR., Jr History of surgical intervention of anterior shoulder instability. J Shoulder Elbow Surg. 2016;25:e139–e150. [DOI] [PubMed] [Google Scholar]
- 21. Lippitt S, Matsen F. Mechanisms of glenohumeral joint stability. Clin Orthop Relat Res. 1993;(291):20–28. [PubMed] [Google Scholar]
- 22. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010;8:336–341. [DOI] [PubMed] [Google Scholar]
- 23. Owens BD, Cameron KL, Peck KY, et al. Arthroscopic versus open stabilization for anterior shoulder subluxations. Orthop J Sports Med. 2015;3(1):23259 67115571084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Owens BD, Harrast JJ, Hurwitz SR, Thompson TL, Wolf JM. Surgical trends in Bankart repair: an analysis of data from the American Board of Orthopaedic Surgery certification examination. Am J Sports Med. 2011;39:1865–1869. [DOI] [PubMed] [Google Scholar]
- 25. Plath JE, Feucht MJ, Bangoj R, et al. Arthroscopic suture anchor fixation of bony Bankart lesions: clinical outcome, magnetic resonance imaging results, and return to sports. Arthroscopy. 2015;31:1472–1481. [DOI] [PubMed] [Google Scholar]
- 26. Plath JE, Feucht MJ, Saier T, et al. Sporting activity after arthroscopic Bankart repair for chronic glenohumeral instability. Arthroscopy. 2015;31:1996–2003. [DOI] [PubMed] [Google Scholar]
- 27. Pogorzelski J, Beitzel K, Imhoff AB, Braun S. The mini-open Latarjet procedure for treatment of recurrent anterior instability of the shoulder [in German]. Oper Orthop Traumatol. 2016;28:408–417. [DOI] [PubMed] [Google Scholar]
- 28. Robins RJ, Daruwalla JH, Gamradt SC, et al. Return to play after shoulder instability surgery in National Collegiate Athletic Association Division I intercollegiate football athletes. Am J Sports Med. 2017;45:2329–2335. [DOI] [PubMed] [Google Scholar]
- 29. Stein T, Linke RD, Buckup J, et al. Shoulder sport-specific impairments after arthroscopic Bankart repair: a prospective longitudinal assessment. Am J Sports Med. 2011;39:2404–2414. [DOI] [PubMed] [Google Scholar]
- 30. Takeda H, Watarai K, Ganev GG, Oguro K, Higashi A, Tateishi A. Modified Bankart procedure for recurrent anterior dislocation and subluxation of the shoulder in athletes. Int Orthop. 1998;22:361–365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Thomazeau H, Courage O, Barth J, et al. Can we improve the indication for Bankart arthroscopic repair? A preliminary clinical study using the ISIS score. Orthop Traumatol Surg Res. 2010;96:S77–S83. [DOI] [PubMed] [Google Scholar]
- 32. Tordjman D, Vidal C, Fontes D. Mid-term results of arthroscopic Bankart repair: a review of 31 cases. Orthop Traumatol Surg Res. 2016;102:541–548. [DOI] [PubMed] [Google Scholar]
- 33. Zhu M, Young SW, Pinto C, Poon PC. Functional outcome and the structural integrity of arthroscopic Bankart repair: a prospective trial. Shoulder Elbow. 2015;7:85–93. [DOI] [PMC free article] [PubMed] [Google Scholar]