

Abstract
Aim:
This study aims to compare visual outcomes and complications of iris-fixated (claw) intraocular lens (IFIOL) implantation with those of posterior chamber intraocular lens (PCIOL) implantation in children with traumatic cataract.
Settings and design:
Retrospective observational clinical audit.
Materials and methods:
A total of 50 pediatric traumatic cataract cases that underwent lens removal and IOL implantation (IFIOL or PCIOL) with or without corneal or corneoscleral tear repair between January 2009 and December 2013 were analyzed. After meeting the eligibility criteria, their pre- and postoperative visual outcomes and complication rates were recorded. Data were analyzed descriptively.
Results:
Out of 50 children, IFIOL and PCIOL implantations were performed in one eye of each of 25 children. Their mean age was 11 ± 4 years (range 4–18 years). Primary (cataract removal with lens implantation) and secondary (corneal tear repair followed by cataract removal with lens implantation) procedures were performed in 19 (76%) and six (24%) children in the IFIOL group and in 21 (84%) and four (16%) children in the PCIOL group, respectively. There was an improvement in best corrected visual acuity postimplantation in both the IFIOL and the PCIOL group, and no significant difference in the logarithm of the minimum angle of resolution of best corrected visual acuity was observed between the two groups over 36 months. Only three eyes in the IFIOL group developed complications: one eye developed secondary glaucoma, one disenclavation of IOL haptic, and one cystoid macular edema.
Conclusion:
Both IFIOL and PCIOL implantations have good visual outcomes and minimal postoperative complications; therefore, IFIOL can be used as an alternative to PCIOL in children with traumatic cataract with inadequate capsular support.
Keywords: complications, iris claw, posterior chamber intraocular lens, traumatic cataract, visual outcome
1. Introduction
Ocular trauma, the leading cause of pediatric cataracts, is characterized by simple corneal abrasion, lid laceration, iritis, hyphema, lens injury, vitreous hemorrhage, retinal detachment, traumatic optic neuropathy, orbit fracture, and ruptured globes.1,2
Optical rehabilitation of traumatic cataract (Figure 1) with inadequate capsular support is a major therapeutic challenge. Successful rehabilitation depends on the choice of intraocular lens (IOL) design and surgical procedure.3 Literature describes that an IOL can be placed in the anterior chamber (ACIOL), fixed to the anterior or posterior surface of iris (IFIOL), or sutured to the sclera (SFIOL).4 Placement of an IOL in the capsular bag has become the accepted method of treatment for children undergoing cataract surgery.5 The IOL can be placed in the capsular bag if either the anterior or the posterior capsule is intact, or sufficient amount of capsule is present.6 Several surgical procedures have been used to correct traumatic cataract, aphakia, or ectopia lentis, including flexible open-loop ACIOL,7 iris-fixated posterior chamber IOL (PCIOL),8 iris-claw ACIOL,9 retropupillary iris-fixated IOL,10 scleralfixated PCIOL,9 and fibrin glue-assisted PCIOL.11 However, controversies still exist over the efficacy and safety of different IOL implantation procedures in cases of inadequate or no capsular support.12
Figure 1.
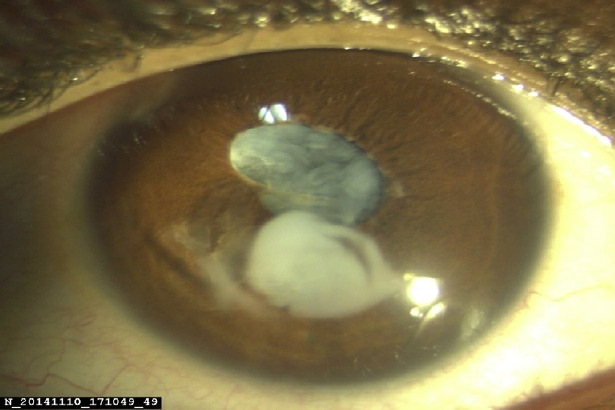
Traumatic cataract.
ACIOLs are infrequently used in children due to high risk of corneal decompensation, pseudophakic bullous keratopathy, iris atrophy, pupil ectopia, secondary glaucoma, severe uveitis, and hyphema.13,14,15 IFIOLs are fixated to the anterior surface of the iris in the anterior chamber or to the posterior surface of the iris, offering several advantages such as low-risk method of surgery, stability enhancement, less tilting of the lens, and reduced glare phenomenon.16,17 SFIOL implantation is a well-tolerated method for correction of traumatic cataract; however, the surgery is technically more difficult and associated with surgical complications such as suture breakage with IOL subluxation and retinal detachment.4,9,12,18
Some literatures discuss the comparison of IFIOL implantation with PCIOL implantation. Some studies have favored IFIOL over PCIOL in terms of better visual outcomes,9,19 and some studies have shown comparable visual outcomes.20 However, little evidence is yet available regarding the visual outcomes and complication profiles of both (IFIOL and PCIOL) implantations. Hence, the present study was planned to evaluate the visual outcome and complication rate following IFIOL and PCIOL implantations in Indian pediatric traumatic cataract cases with or without adequate capsular support.
2. Materials and methods
This was a retrospective, observational clinical audit of 50 children with traumatic cataract who attended the outpatient department (Sankara Eye Hospital, Shimoga, India) between January 2009 and December 2013. The study was in compliance with the principles of the Declaration of Helsinki 2000. Twenty-five case records with traumatic cataract, inadequate capsular support, and IFIOL implantation, and a similar number of case records with adequate capsular support and PCIOL implantation were included in the analysis, after obtaining consent from all parents. Corneal/corneoscleral tear, when present, was repaired, and cataract surgery was performed by anterior (limbal) approach with IOL implantation as a primary/secondary procedure. A procedure was said to be primary if cataract removal with lens implantation was performed as the first procedure and secondary if corneal tear repair was carried out first, followed by cataract removal with lens implantation as a second procedure. Children with retinal detachment, vitreous hemorrhage, and posterior (pars plana) approach for cataract removal and IOL implantation were excluded from the study.
Choice of the procedure was decided intraoperatively/preoperatively and was dependent on the status of capsular support. IFIOL implantation was considered as the procedure of choice in large posterior capsular tear cases. A single surgeon performed all the 50 surgeries.
Prior to surgery, complete clinical examination of the traumatic cataract eye was performed, whereby the nature and duration of injury, visual acuity [uncorrected visual acuity and best corrected visual acuity (BCVA)] using logarithm of the minimum angle of resolution (logMAR) charts,21 anterior segment (slit lamp) and posterior segment (indirect ophthalmoscope or B scan) findings, and intraocular pressure (IOP) were noted. Keratometric values (automated keratorefractometer) and axial length (A scan) of fellow normal eye was used for IOL power calculation in cases with a corneal scar in the affected eye. For IOL power implantation, Dahan and Drusedau’s22 guidelines were used with slight modification, where all children aged < 2 years were undercorrected by 20%, aged 2–5 years by 10%, aged 5–8 years by 5%, and aged 8–10 years by 2.5%, and children aged >10 years were made emmetropic.
In both groups, corneal/corneoscleral tear, when present, was repaired first under general anesthesia using 10-0 nylon interrupted sutures. Cataract surgery, anterior vitrectomy, and IOL implantation were performed as a primary or secondary procedure. IFIOL (model no.: PIC 5590, or PIC 5580; Excel Optics (P) Ltd., Chennai, India (Joint venture with: American Ophthalmic Laboratories, LLC, 193- Rock Ridge Road, Millersville, MD 21108, U.S.A); overall length: 9 mm or 8 mm; biconvex optic size: 5 mm or 5.5 mm; estimated A constant: 117; Figure 2A) was implanted in cases with inadequate capsular support. The IOL was inserted into the anterior chamber. Optic was held using a pair of lens forceps; one haptic was tilted down and pushed under the iris gently. A fine rod was passed through the paracentesis on the same side; once the haptic was behind the iris (retrofixated), the haptic was tilted up to produce an indent on the iris and the iris was enclaved into the haptic claw with a gentle push of the rod. Haptic enclavation was then performed on the other side. In cases with adequate capsular support (either anterior or posterior capsular support, or both), a 12.5-mm or 13-mm PCIOL was implanted either in the capsular bag or in the sulcus.
Figure 2.
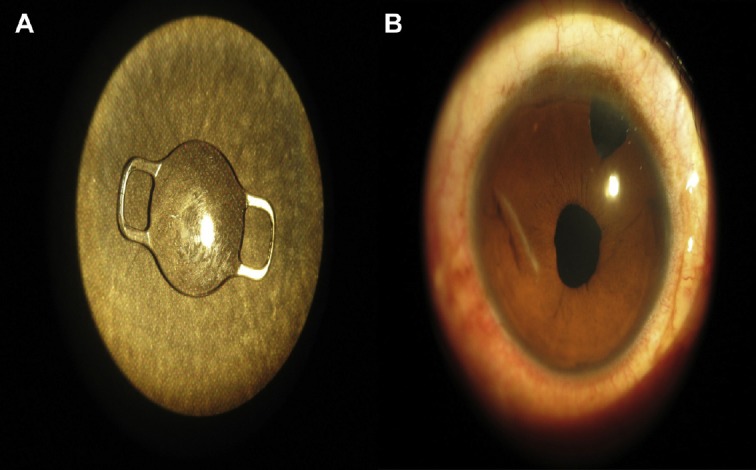
(A) IFIOL (claw): overall length: 9 mm or 8 mm; optic size 5 mm or 5.5 mm; A constant: 117. (B) Postoperative round pupil. IFIOL = iris-fixated intraocular lens.
Topical antibiotics and steroids were instilled and tapered over 3 months. Patients were prescribed oral steroids (1 mg/kg) for 7–10 days, and homatropine and antiglaucoma medicines for 1 month. The postoperative vision, IOP, IOL status, and posterior segment complications were noted at each follow-up visit.
2.1. Statistical analyses
Data were analyzed using SAS 9.2, SPSS 15.0, Stata 10.1, MedCalc 9.0.1, Systat 12.0, and R environment version 2.11.1. Descriptive and inferential statistical analyses were used to analyze the data. Fisher test was used to analyze visual acuity in both groups.
3. Results
The mean age in the IFIOL group was 10.76 ± 3.98 years and in the PCIOL group 11 ± 4.14 years (range 4–18 years). In each group, 44% (11/25) of children were in the age range of 6–10 years. There was male preponderance in both groups, 84% in the IFIOL group and 88% in the PCIOL group. In the IFIOL group, 64% of children had left eye trauma, and in the PCIOL group, 64% had right eye trauma. The most common nature of eye injury was that caused by a stick in both groups (IFIOL: 56%; PCIOL: 48%). More than 60% of children in both groups had an axial length of 22–24 mm and were implanted with an IOL with power between 20.1 D and 24 D (Table 1). The most common diagnosis at presentation was traumatic mature cataract with closed globe injury (IFIOL: 44%; PCIOL: 56%), followed by traumatic mature cataract with open globe injury (IFIOL: 24%; PCIOL: 20%) and traumatic absorbed cataract with closed globe injury (IFIOL: 20%; PCIOL: 16%) (Table 2).
Table 1.
Patient characteristics at baseline.
| Category | IFIOL (n = 25),n(%) | PCIOL (n = 25),n(%) |
|---|---|---|
| Age (y) | ||
| 1–5 | 3 (12.0) | 2 (8.0) |
| 6–10 | 11 (44.0) | 11 (44.0) |
| 11–15 | 7 (28.0) | 6 (24.0) |
| 16–20 | 4 (16.0) | 6 (24.0) |
| Sex | ||
| Female | 4 (16.0) | 4 (16.0) |
| Male | 21 (84.0) | 21 (84.0) |
| Eye involvement | ||
| Left | 16 (64.0) | 9 (36.0) |
| Right | 9 (36.0) | 16 (64.0) |
| Trauma nature | ||
| Stick | 14 (56.0) | 12 (48.0) |
| Pencil | 2 (8.0) | 0 |
| Ball | 1 (4.0) | 1 (4.0) |
| Bat | 1 (4.0) | 0 |
| Coconut shell | 1 (4.0) | 0 |
| Fall | 1 (4.0) | 1 (4.0) |
| Fire cracker | 0 | 1 (4.0) |
| Iron rod | 1 (4.0) | 0 |
| Needle | 0 (0) | 1 (4.0) |
| Peacock peck | 1 (4.0) | 0 |
| Pen | 1 (4.0) | 3 (12.0) |
| Road traffic accident | 1 (4.0) | 0 |
| Stone | 0 | 1 (4.0) |
| Thorn | 0 | 3 (12.0) |
| Welding bar | 1 (4.0) | 0 |
| Wire | 0 | 1 (4.0) |
| Wood | 0 | 1 (4.0) |
| Axial length (mm) | ||
| 21–22 | 5 (20.0) | 5 (20.0) |
| 22–24 | 17 (68.0) | 17 (68.0) |
| 24–26 | 3 (12.0) | 3 (12.0) |
| IOL power (D) | ||
| <18 | 3 (12.0) | 4 (16.0) |
| 18–20 | 6 (24.0) | 3 (12.0) |
| 20.1–24 | 15 (60.0) | 17 (68.0) |
| >24 | 1 (4.0) | 1 (4.0) |
IFIOL = iris-fixated intraocular lens; PCIOL = posterior chamber intraocular lens.
Table 2.
Diagnosis at presentation.
| Lens | IFIOL (n = 25), n(%) | PCIOL (n = 25), n(%) | |
|---|---|---|---|
| Traumatic cataract with open globe injury | |||
| Mature cataract | 6 (24.0) | 5 (20.0) | |
| Subluxated lens | 1 (4.0) | 0 | |
| Traumatic cataract with close globe injury | |||
| Absorbed cataract | 5 (20.0) | 4(16.0) | |
| Mature cataract | 11 (44.0) | 14 (56.0) | |
| Rosette cataract | 0 | 1 (4.0) | |
| Subluxated lens | 2 (8.0) | 1 (4.0) | |
IFIOL = iris-fixated intraocular lens; PCIOL = posterior chamber intraocular lens.
Of the 50 children, 40 (80%) underwent IOL implantation by the primary procedure, where IFIOL was implanted in 19 (47.5%) and PCIOL in 21 (52.5%) children. The remaining 10 (20%) children underwent IOL implantation by a secondary procedure, where IFIOL was implanted in six (60%) and PCIOL in four (40%) children. The IOL was placed in the sulcus in 17 (68%) and in the capsular bag in eight (32%) of the children in the PCIOL group. Forty-two (84%) [IFIOL: 20 (80%); PCIOL: 22 (88%)] children underwent patching of the nonoperated eye following surgery. The majority of children in both groups [IFIOL: 23 (92%); PCIOL: 24 (96%)] had normal fundus. A myopic tessellated fundus was observed in one (4%) child in each group and, optic atrophy was observed in one (4%) child of the IFIOL group (Table 3). After surgery, the duration of follow-up visits to the ophthalmologist varied from 9 months to 36 months. In the IFIOL group, 36% of the children were followed up for 18 months and the mean follow-up period was 16.44 ± 7.41 months, and in the PCIOL group, 36% were followed up for 12 months and the mean follow-up period was 15.36 ± 7.42 months.
Table 3.
Treatment approach.
| Type | IFIOL (n = 25),n(%) | PCIOL (n = 25),n(%) |
|---|---|---|
| Primary procedure | ||
| Cataract removal + lens implantation | 19 (76.0) | 21 (84.0) |
| Corneal tear repair | 6 (24.0) | 4(16.0) |
| Secondary procedure | ||
| Nil | 19 (76.0) | 21 (84.0) |
| Cataract removal + lens implantation | 6 (24.0) | 4(16.0) |
| Treatment | ||
| Posterior iris fixation | 25 (100.0) | 0 |
| Bag | 0 | 8 (32.0) |
| Sulcus | 0 | 17 (68.0) |
| Patching | ||
| No | 5 (20.0) | 3 (12.0) |
| Yes | 20 (80.0) | 22 (88.0) |
| Fundus examination | ||
| Normal | 23 (92.0) | 24 (96.0) |
| Myopic | 1 (4.0) | 1 (4.0) |
| Optic atrophy | 1 (4.0) | 0 |
| IOP (mmHg) measurement | ||
| ≤20 | 24 (96.0) | 25 (100.0) |
| >20 | 1 (4.0) | 0 |
IFIOL = iris-fixated intraocular lens; IOP = intraocular pressure; PCIOL = posterior chamber intraocular lens.
The preoperative BCVA in both groups was worse than logMAR 1.0. In the IFIOL group, 32% were able to see hand movement (HM), 24% had counting finger (CF) ability, and 44% had perception of light (PL); in the PCIOL group, 52% were able to see HM, 8% had CF ability, and 40% had PL. There was an improvement in uncorrected visual acuity and BCVA at 1 month, 3 months, and the last follow up postoperatively. However, the values were comparable between these two groups. At the last follow up, the proportion of children with BCVA (0–0.2 logMAR) was comparable between these two groups (64% vs. 56%; p > 0.05). There was a marked decline in the proportion of children with HM, CF, and PL at 1 month, 3 months, and the last follow up in both groups. One eye (4%) in the IFIOL group had PL at 1 month, 3 months, and 36 months. One eye (4%) in the PCIOL had HM at 1 month, 3 months, and 36 months. One eye (4%) in both groups had CF at 1 month and 3 months (Table 4).
Table 4.
Pre- and postoperative BCVA.
| Category | Preoperative | No. of Children (%) | % Change | |||
|---|---|---|---|---|---|---|
| UCVA 1 mo | BCVA 1 mo | BCVA 3 mo | BCVA 36 mo | |||
| IFIOL (n = 25) | ||||||
| 0–0.2 | 0 | 2 (8.0) | 4 (16.0) | 4 (16.0) | 16 (64.0) | +64.0 |
| 0.3–0.6 | 0 | 11 (44.0) | 12 (48.0) | 14 (56.0) | 6 (24.0) | +24.0 |
| 0.7–1.0 | 0 | 10 (40.0) | 7 (28.0) | 5 (20.0) | 2 (8.0) | +8.0 |
| HM | 8 (32.0) | 0 | 0 | 0 | 0 | –32.0 |
| CF | 6 (24.0) | 1 (4.0) | 1 (4.0) | 1 (4.0) | 0 | –24.0 |
| PL+ | 11 (44.0) | 1 (4.0) | 1 (4.0) | 1 (4.0) | 1 (4) | –40.0 |
| PCIOL (n = 25) | ||||||
| 0–0.2 | 0 | 0 | 2 (8.0) | 3 (12.0) | 14 (56.0) | +56.0 |
| 0.3–0.6 | 0 | 15 (60.0) | 16 (64.0) | 15 (60.0) | 7 (28.0) | +28.0 |
| 0.7–1.0 | 0 | 8 (32.0) | 5 (20.0) | 5 (20.0) | 3 (12.0) | +12.0 |
| HM | 13 (52.0) | 1 (4.0) | 1 (4.0) | 1 (4.0) | 1 (4.0) | –48.0 |
| CF | 2 (8.0) | 1 (4.0) | 1 (4.0) | 1 (4.0) | 0 | –8.0 |
| p | 0.344 | 0.825 | 0.809 | >0.99 | >0.99 | — |
Fisher test was used to analyze visual acuity in both groups.
BCVA = best corrected visual acuity; CF = counting finger; HM = hand movement; IFIOL = iris-fixated intraocular lens; PCIOL = posterior chamber intraocular lens; PL = perception of light; UCVA = uncorrected visual acuity
The common complications in both groups were posterior synechiae, pigment dispersion, pupillary capture, and irregular pupil. Posterior synechiae was the most frequent postoperative complication observed in the PCIOL group (28%), in particular where the IOL was placed in the sulcus, followed by pigment dispersion (24%) and pupillary capture (12%) (Figure 3). In the IFIOL group, pigment dispersion was the most frequent postoperative complication observed in 24% of patients, which was similar to that observed in the PCIOL group.
Figure 3.
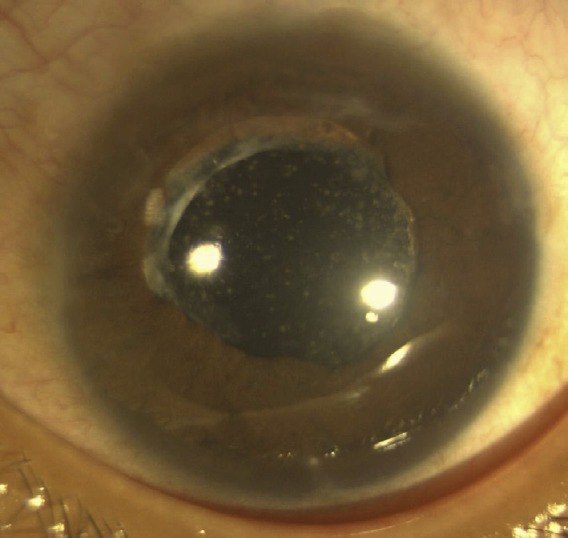
PCIOL: pigment dispersion, pupillary capture, posterior synechiae. PCIOL = posterior chamber intraocular lens.
None of the 50 eyes had infection, secondary glaucoma, or retinal problems except for three eyes of the IFIOL group, where one eye underwent re-enclavation of one of the claws following spontaneous disenclavation at 1 month, the second eye had cystoid macular edema (CME) that resolved by 3 months, and the third eye had IOP >20 mmHg (24 mmHg) 1 month after IOL implantation and was well controlled with antiglaucoma medicines within 3 months (Table 3).
In the IFIOL group, only one eye had a horizontally oval pupil, while the remaining 24 eyes had a round pupil (Figure 2B) post-operatively. Pigment dispersion (Figure 4) on the lens surface in four eyes (16%) and iris atrophy at the site of enclavation (Figure 4) at 6 months in one eye (4%) were also noted postoperatively.
Figure 4.
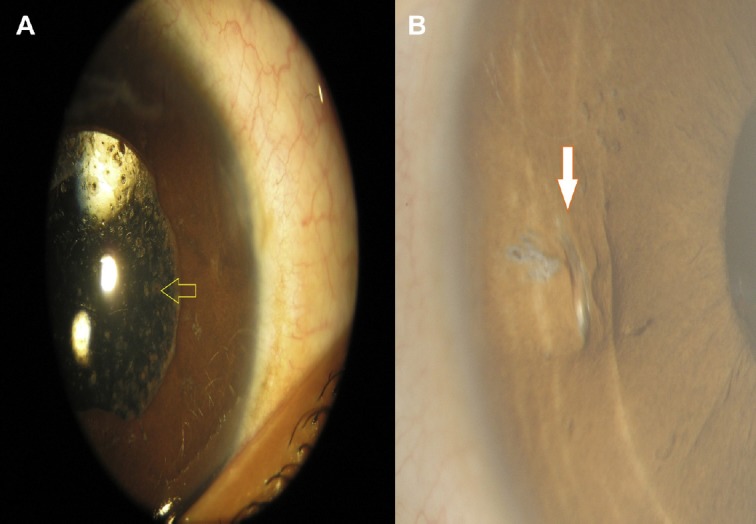
IFIOL: (A) pigment dispersion; (B) iris atrophy. IFIOL = iris-fixated intraocular lens.
4. Discussion
Traumatic cataract is an important cause of monocular blindness in children.3 IOL implantation has been recommended as the treatment of choice for traumatic cataract cases and offers benefits such as infrequent hospital visits, reduced need of supervision by the ophthalmologist due to the availability of refined surgical procedures, and better instruments and suture materials.4,5,8,10,23 IFIOL and SFIOL have been popular choices of IOLs for implantation in the absence of adequate capsule support.20
In our study, the majority (80%) of children had IOL implantation by the primary procedure, and a comparable proportion of children underwent IFIOL or PCIOL implantation. Previous literature has reported a positive role of patching of the nonoperated eye after IOL implantation in improving visual outcomes.24 In our study, out of 50 children, 42 (84%) underwent patching.
None of the 50 eyes had BCVA < 1 logMAR before surgery, but after implantation of either lens, the mean postoperative BCVA improved over time; however, no significant difference was observed in postoperative BCVA between the two groups. Our results were in line with the previous literature wherein visual acuity increased postimplantation of IFIOL and SFIOL lenses, but no statistical difference in logMAR BCVA was reported between the two groups over 6 months.20 Other studies have also shown improved visual outcomes after implantation of iris-claw IOL25 and trans-scleral-fixated IOL.26
Elevated IOP is a common complication of IOL implantation.27 In the present study, all the eyes had IOP ≤ 20 mm except for one eye in the IFIOL group, which had elevated IOP of >24 mmHg 1 month postimplantation; this may be attributed to pre-existing trauma or postoperative inflammation.
CME and retinal detachment are two common complications of IOL implantation. CME develops after disruption of blood–retinal barrier, leading to accumulation of excess fluid within the macula, thereby making its prophylaxis extremely important in cataract patients.28 We observed CME and re-enclavation of dislocated IOL in one eye each in the IFIOL group, indicating a low incidence of postoperative complications. Our results were in concordance with previous literature where a low incidence (4.1–4.8%) of postoperative complications was reported.29,30
Both IFIOL and PCIOL have good visual outcomes and are associated with minimal postoperative complications. Hence, IFIOL can be used as an alternative to other IOLs in children with traumatic cataracts where the capsular support is inadequate.
Acknowledgments
The authors thank the management of Sankara Eye Hospital and its staff—Dr S. Mahesha Bhat, Mr K.P. Suresh (statistician), Mr Praveen K, Dr Somashekhar SP, Dr Hariprasad Vokuda, Dr Mubashir Parkar, and Mrs Geetha H.
Footnotes
Conflicts of interest: The authors declare that they have no conflicts of interest.
Part of the data and figures that has been used in the analysis of this article (children with traumatic pediatric cataract managed with cataract removal and irisfixated lens) has been submitted to and is in the process of getting published in the Middle East African Journal of Ophthalmology [V. Kavitha, Preethi Balasubramanian, Mallikarjun M. Heralgi. Posterior iris fixated intraocular lens for pediatric traumatic cataract. MEAJO_115_15R9. (Brief communication)].
References
- 1.Burstein ES, Lazzaro DR. Traumatic ruptured globe eye injuries in a large urban center. Clin Ophthalmol. 2013;7:485–488. doi: 10.2147/OPTH.S42050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Guzel M, Erenler AK, Niyaz L, Baydin A. Management of traumatic eye injuries in the emergency department. OA Emerg Med. 2014;2:2. [Google Scholar]
- 3.Dakshayani R. Analysis of visual prognosis after surgery in traumatic cataract. J Evid Based Med Healthc. 2014;1:1029–1046. [Google Scholar]
- 4.Rao GS. Scleral fixated intraocular lens implantation in pediatric age group—an overview. All India Ophthalmic Conference Proceedings (Retina/Vitreous Session-III) 2010:626–629. [Google Scholar]
- 5.Wilson ME. Anterior lens capsule management in pediatric cataract surgery. Trans Am Ophthalmol Soc. 2004;102:391–422. [PMC free article] [PubMed] [Google Scholar]
- 6.Krachmer JH, Mannis MJ, Holland EJ. Cornea. 2nd ed. Philadelphia, PA: Mosby; 2005. [Google Scholar]
- 7.Evereklioglu C, Er H, Bekir NA, Borazan M, Zorlu F. Comparison of secondary implantation of flexible open-loop anterior chamber and scleral-fixated posterior chamber intraocular lenses. J Cataract Refract Surg. 2003;29:301–308. doi: 10.1016/s0886-3350(02)01526-2. [DOI] [PubMed] [Google Scholar]
- 8.Yen KG, Reddy AK, Weikert MP, Song Y, Hamill MB. Iris fixated posterior chamber intraocular lenses in children. Am J Ophthalmol. 2009;147:121–126. doi: 10.1016/j.ajo.2008.07.038. [DOI] [PubMed] [Google Scholar]
- 9.Farrahi F, Feghhi M, Haghi F, Kasiri A, Afkari A, Latifi M. Iris claw versus scleral fixation intraocular lens implantation during pars plana vitrectomy. J Ophthalmic Vis Res. 2012;7:118–124. [PMC free article] [PubMed] [Google Scholar]
- 10.Bhandari V, Reddy JK, Karandikar S, Mishra I. Retro-pupillary iris fixated intraocular lens in pediatric subluxated lens. J Clin Ophthalmol Res. 2013;1:151–154. [Google Scholar]
- 11.Agarwal A, Kumar DA, Jacob S, Baid C, Agarwal A, Srinivasan S. Fibrin glue-assisted sutureless posterior chamber intraocular lens implantation in eyes with deficient posterior capsules. J Cataract Refract Surg. 2008;34:1433–1438. doi: 10.1016/j.jcrs.2008.04.040. [DOI] [PubMed] [Google Scholar]
- 12.Ahmad M, Naeem M, Iqbal S, Khan S. Visual outcome and complications of anterior chamber intraocular lens versus scleral fixated intraocular lens. Pak J Ophthalmol. 2012;28:206–210. [Google Scholar]
- 13.Epley KD, Shainberg MJ, Lueder GT, Tychsen L. Pediatric secondary lens implantation in the absence of capsular support. J AAPOS. 2001;5:301–306. doi: 10.1067/mpa.2001.117567. [DOI] [PubMed] [Google Scholar]
- 14.Morrison D, Sternberg P, Donaue S. Anterior chamber intraocu ar ens (ACIOL) placement after pars planalensectomy in pediatric Marfan syndrome. JAAPOS. 2005;9:240–242. doi: 10.1016/j.jaapos.2005.02.004. [DOI] [PubMed] [Google Scholar]
- 15.Condon GP, Masket S, Kranemann C, Crandall AS, Ahmed II. Small-incision iris fixation of foldable intraocular lenses in the absence of capsule support. Ophthalmology. 2007;114:1311–1318. doi: 10.1016/j.ophtha.2007.04.018. [DOI] [PubMed] [Google Scholar]
- 16.Koss MJ, Kohnen T. Intraocular architecture of secondary implanted anterior chamber iris-claw lenses in aphakic eyes evaluated with anterior segment optical coherence tomography. Br J Ophthalmol. 2009;93:1301–1306. doi: 10.1136/bjo.2008.148726. [DOI] [PubMed] [Google Scholar]
- 17.Lett KS, Chaudhuri PR. Visual outcomes following Artisan aphakia iris claw lens implantation. Eye. 2011;25:73–76. doi: 10.1038/eye.2010.146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Asadi R, Kheirkhah A. Long-term results of scleral fixation of posterior chamber intraocular lenses in children. Ophthalmology. 2008;115:67–72. doi: 10.1016/j.ophtha.2007.02.018. [DOI] [PubMed] [Google Scholar]
- 19.Zheng D, Wan P, Liang J, Song T, Liu Y. Comparison of clinical outcomes between iris-fixated anterior chamber intraocular lenses and scleral-fixated posterior chamber intraocular lenses in Marfan syndrome with lens subluxa-tion. Clin Exp Ophthalmol. 2012;40:268–274. doi: 10.1111/j.1442-9071.2011.02612.x. [DOI] [PubMed] [Google Scholar]
- 20.Mahajan AR, Datti NP. Comparison of iris claw lens and scleral fixated intraocular lens in terms of visual outcome and complications. J Clin Biomed Sci. 2014;4:357–360. [Google Scholar]
- 21.Grosvenor T, Theodore P. Primary Care Optometry. 5th ed. St. Louis, MO: Elsevier; 2007. pp. 174–175. [Google Scholar]
- 22.Dahan E, Drusedau MU. Choice of lens and dioptric power in pediatric pseu-dophakia. J Cataract Refract Surg. 1997;23:618–623. doi: 10.1016/s0886-3350(97)80043-0. [DOI] [PubMed] [Google Scholar]
- 23.Kaipu S, Gudala KK, Chandrasekhar G, Pathapati RM, Buchineni M, Manikala S. Visual outcome and change in refraction after paediatric cataract surgery. J Evid Based Med Healthc. 2015;2:71–80. [Google Scholar]
- 24.Hemo Y, BenEzra D. Traumatic cataracts in young children. Correction ofaphakia by intraocular lens implantation. Ophthalmic Paediatr Genet. 1987;8:203–207. doi: 10.3109/13816818709031471. [DOI] [PubMed] [Google Scholar]
- 25.Gonnermann J, Klamann MK, Maier AK, et al. Visual outcome and complications after posterior iris-claw aphakic intraocular lens implantation. JCataract Refract Surg. 2012;38:2139–2143. doi: 10.1016/j.jcrs.2012.07.035. [DOI] [PubMed] [Google Scholar]
- 26.Buckley EG. 3 strategies for managing traumatic cataract in children. Ophthalmology Times. 2013. [Accessed June 2015]. Available at: http://ophthalmologytimes.modernmedicine.com/ophthalmologytimes/content/tags/cataract-surgery/3-strategiesmanaging-traumatic-cataract-children?page=full .
- 27.Agrawal S, Verma A. Coloured diaphragm scleral fixated IOL in patients with traumatic aniridia and cataract. IJRTSAT. 2013;7:36–39. [Google Scholar]
- 28.Jaffe NS, Clayman HM, Jaffe MS. Cystoid macular edema after intracapsular and extracapsular cataract extraction with and without an intraocular lens. Ophthalmology. 1982;89:25–29. doi: 10.1016/s0161-6420(82)34855-1. [DOI] [PubMed] [Google Scholar]
- 29.Mohr A, Hengerer F, Eckardt C. Retropupillary fixation of iris claw lens in aphakia. 1 year outcome of a new implantation technique. Ophthalmologe. 2002;99:580–583. doi: 10.1007/s00347-001-0563-z. [In German] [DOI] [PubMed] [Google Scholar]
- 30.Wolter-Roessler M, Kuchle M. Correction of aphakia with retroiridally fixated IOL. Klin Monbl Augenheilkd. 2008;225:1041–1044. doi: 10.1055/s-2008-1027721. [In German] [DOI] [PubMed] [Google Scholar]