

Abstract
Background
In the United States today, 16 million children are growing up poor. Few studies report multiple environmental factors associated with poverty during the first year of life and effects on infant development.
Objectives
To evaluate maternal, home, and neighborhood environment of Low and Higher Socioeconomic Status (SES) infants from birth to 1 year; to evaluate impact of SES and environment on infant developmental outcome at 1 year.
Methods
Low (n=30) and Higher SES (n=30) African American mothers and their healthy term gestation female infants were prospectively compared for environmental characteristics and infant developmental outcome. Environment-Maternal: Wechsler Adult Intelligence Scale-IV (WAIS-IV); Beck Depression Inventory (BDI-II); Perceived Stress Scale (PSS); Parenting Stress Index (PSI-4); Social Support Scale (SSS); Home: Home Observation Measurement of the Environment (HOME); Household Food Insecurity (HFI); Neighborhood: Concentrated Neighborhood Disadvantage (CND). Infant Outcome-Bayley Scales of Infant Development Third Edition (BSID-III); Preschool Language Scale (PLS-5).
Results
Environmental risk was greater for Low compared to Higher SES: lower WAIS-IV (p< 0.001); higher PSI-4 Total (p=0.003); lower HOME Total and 3 subscales (p<0.002); higher HFI (p=0.012); and higher CND (p=0.027). Low SES infant outcomes differed from Higher SES: lower BSID-III Cognitive Composite (p=0.005), PLS-5 Total Language (p ≤ 0.017), and Auditory Comprehension (p ≤ 0.008). In regressions, after controlling for SES, effects of environmental factors were not found.
Conclusions
By age one, Low SES infants had been exposed to greater environmental disadvantage, and already exhibited poorer developmental functioning than Higher SES infants. These findings suggest support for families and children from impoverished circumstances cannot begin too early.
Key Terms: Poverty, Low Socioeconomic Status, Infant Development, Birth Cohort, Environmental factors
INTRODUCTION
It is not news that poverty exerts deleterious effects on child outcome. Seminal studies show lower family income is associated with poorer cognitive performance and academic achievement, with persistent poverty having a greater effect than transient poverty.1 Evaluations of preschool age and older children show a pattern of developmental delay followed by increased likelihood of deficits in school readiness, and academic gaps that widen over time.2 In the United States, the impact of these adverse effects is enormous: 16 million children (one in five) now are living below the federal poverty line of $24,230 for a family of four.3 All of these children are at risk for a compromised future, with over 40% of those growing up in poverty remaining in poverty as adults.4
Risk factors associated with poverty status can be grouped by various domains, including caregiver, home, and community/neighborhood. Ecobiodevelopmental models that integrate these domains of child experience have been applied to the study of human health and disease.5 While socioecomonic status provides a broad indication of level of contextual risk, maternal, home and neighborhood level characteristics provide additional insight regarding contextual variation within SES groups. Viewing development through such an ecological lens enriches conceptualization of the influence of risk associated with poverty.
The majority of investigations of poverty’s effects, including evaluations of environmental risk factors, have been conducted in children older than 2 years of age.5 Despite knowledge regarding sensitivity to the environment and rapid learning that occurs during infancy, few reports examine effects of environmental factors at this young age.2,6 Because it is likely that poverty begins to impact outcome at the earliest stages of development, even prenatally,7 comprehensive evaluation of environmental factors affecting infants is needed to more fully understand contexts that shape development of children growing up poor.
In an ongoing study of the effects of low SES on infant outcome our objectives were twofold: 1) to evaluate maternal, home, and neighborhood environment of Low and Higher Socioeconomic Status (SES) infants from birth to 1 year; and 2) to evaluate impact of SES and environment on infant developmental outcome at 1 year. We hypothesized that disadvantage, present from birth onward, would affect infant outcome by age one year.
METHODS
Participants
Infants for this report were participants in a longitudinal study of the effects of poverty on developmental and neural outcome in the first year of life. Sixty American-born African American mothers and their infants were enrolled. Mothers were excluded if they had significant medical, psychiatric or obstetric problems, had a history of drug use, or did not speak English. Maternal chart review included screening for history of drug or alcohol problems and other maternal markers associated with increased risk for infant developmental delay including risk for Fetal Alcohol Syndrome. Eligible infants were healthy, female, term (between 38 and 42 weeks gestation), appropriate size for gestation, and with 5-minute Apgar ≥ 8. By study design, 30 were of Low SES and 30 of Higher SES. SES groups were determined using the 2013 U.S. Census Bureau federal income-to-needs (ITN) ratios for families. Low SES was defined as annual household income at or below the federal poverty line (for a family of four the poverty line was $23,550 at the time of project initiation) with both parents having no more than a high school education. Higher SES families had ITN of greater than the poverty line and both parents had at least a high school diploma. While “poverty” has been defined in a number of ways, to include combinations of income, insurance status, education, and job category, we used ITN as our primary group identifier as it has a precise definition and takes into account household size.
Measures
At time of enrollment mothers completed demographic questionnaires. Natal data, acquired by maternal and infant chart review, included infant growth parameters, size for gestational age, and Apgar score. During infants’ first year of life, maternal, home, and neighborhood factors, known to be associated with child outcomes in older children, were evaluated. The timing of assessments was determined based on overall study design, respondent burden at various time points, stability of measures such as Maternal IQ, and time period reflected in caregiver responses.
Maternal characteristics
Maternal cognitive function was assessed at the study center by a psychologist masked to group status when infants were 7 months of age using the Vocabulary and Matrix Reasoning subtests from the Wechsler Adult Intelligence Scale - Fourth Edition (WAIS-IV). 8 Maternal cognitive function is of particular interest as it likely influences child outcome through both genetic and environmental pathways.9 Maternal psychosocial function was assessed in one-on-one sessions at time of the 7 or 12-month follow-up visits. The Beck Depression Inventory - Second Edition (BDI-II), designed to measure maternal symptoms of depression experienced over the last 2 weeks, was completed at the 12-month visit.10 The Perceived Stress Scale (PSS), designed to measure the degree to which situations are appraised as stressful over the past 30 days, was completed at the 12-month visit. The Parenting Stress Index-4th Edition (PSI-4),11 evaluating three domains that contribute to stress (child characteristics, parental characteristics, and life stress), was completed at the 7-month visit. Social support experienced by mothers over the last six months was evaluated at the 12-month visit utilizing the Social Support Scales. 12
Household and neighborhood factors
Approximately 2 months prior to the 12 month developmental evaluation, trained research assistants visited infants’ homes to evaluate the quality of the home environment using the Infant/Toddler Home Observation Measurement of the Environment Inventory (HOME). The HOME consists of six subscales (Table 2)13 that measure the quality and quantity of stimulation and support available to a child in the home environment. Timing of this assessment was chosen to provide measurement prior to developmental testing and capitalize on the higher predictive power of HOME scores at later ages. Household food insecurity over the past 12 months was assessed at the 12-month visit using the US Household Food Security Module.14 A Concentrated Neighborhood Disadvantage (CND) factor score,15 derived from US census data for each participant’s home address at time of enrollment, was computed using principal component analysis of six items (Table 2) from the 2000 U.S. census data. The 52 participants lived in 43 census tracts. Six measures were employed: percentage of individuals below the poverty line, unemployed, receiving public assistance, African Americans, children under the age of 18, and female-headed households. Principal components analysis confirmed a single factor of concentrated disadvantage which accounted for 69.9% of the total variance in the six variables. Factor loadings, which ranged from 0.66 to 0.92, were used to create a continuous, regression-weighted factor score for concentrated disadvantage.
Table 2.
Environment: Maternal, Home and Neighborhood Factors
| Low SES n=27 |
Higher SES n=25 |
p-value | |
|---|---|---|---|
| Maternal Factors | |||
|
| |||
| Maternal† WAIS-IV Subtests | |||
| Vocabulary Scaled scorea | 6.2 ± 1.8b | 9.8 ± 3.4 | <0.001 |
| High Risk Category* | 16 (59.3%)c | 3 (12.5%) | 0.001d |
| Matrix Reasoning Scaled score | 7.9 ± 2.8 | 11.8 ± 2.3 | <0.001 |
| High Risk Category | 10 (37.0%) | 1 (4.2%) | 0.004 |
|
| |||
| Beck Depression Inventory-II (BDI-II) | 10.4 ± 9.8 | 10.4 ± 8.7 | 0.99 |
| High Risk Category | 4 (14.8%) | 3 (12.0%) | 0.77 |
|
| |||
| Perceived Stress Scale (PSS) | 16.4 ± 7.6 | 14.4 ± 9.2 | 0.40 |
| High Risk Category | 8 (29.6%) | 6 (24.0%) | 0.65 |
|
| |||
| Parenting Stress Index-4 (PSI-4) | |||
| Total Stress T-score | 49.6 ± 5.0 | 45.2 ± 5.3 | 0.003 |
| Child T-score | 49.8 ± 5.5 | 46.0 ± 4.8 | 0.01 |
| Parent T-score | 49.4 ± 5.5 | 45.1 ± 7.0 | 0.02 |
| Life Stress T-score | 48.4 ± 10.9 | 49.5 ± 9.3 | 0.71 |
| High Risk Category | 8 (29.6%) | 6 (24.0%) | 0.65 |
|
| |||
| Social Support score | 7.6±2.4 | 8.5±2.1 | 0.17 |
| High Risk Category | 8 (29.6%) | 7 (28.0%) | 0.89 |
|
| |||
| Home Factors | |||
|
| |||
| Home Observation Measurement of the Environment (HOME) | |||
| Age at time of Home Visit | 11.2 ± 0.57 | 10.9 ± 0.57 | 0.094 |
| Total score | 32.6 ± 3.6b | 38.2 ± 3.2 | <0.001 |
| HOME subscales | |||
| Emotional and Verbal Responsivity of Parent | 8.8 ± 1.9 | 9.4 ± 1.0 | 0.21 |
| Acceptance of Child’s Behavior | 6.0 ± 1.3 | 6.3 ± 1.0 | 0.28 |
| Organization of Physical & Temporal Environment | 4.7 ± 1.0 | 5.4 ± 0.6 | 0.002 |
| Provision of Appropriate Play Materials | 6.3 ± 1.7 | 8.1 ± 1.1 | <0.001 |
| Parent Involvement with Child | 3.1 ± 1.2 | 5.2 ± 1.1 | <0.001 |
| Opportunities for Variety in Daily Stimulation | 3.2 ± 1.1 | 3.8 ± 1.0 | 0.056 |
| High Risk Category* | 9 (33.3%)c | 1 (4.0%) | 0.007d |
|
| |||
| Food Insecurity Index (HFI) | |||
| High Risk Category | 18 (66.7%) | 8 (32.0%) | 0.012 |
|
| |||
| Neighborhood Factors | |||
|
| |||
| Concentrated Neighborhood Disadvantage (CND) | |||
| Concentrated Disadvantage Factor Score | 0.32± 0.80 | −0.27 ± 1.0 | 0.027 |
| % Below povertye | 30.7 ± 11.6 | 25.8 ± 10.0 | 0.11 |
| % Receiving public assistance | 13.3 ± 6.8 | 10.3 ± 6.5 | 0.12 |
| % Female-only hshld w/minor children | 37.9 ± 8.6 | 31.1 ± 11.1 | 0.016 |
| % Unemployed | 7.8 ± 2.7 | 6.4 ± 3.2 | 0.093 |
| % Under 18 | 30.4 ± 5.4 | 26.9 ± 7.8 | 0.062 |
| % African American | 82.4±21.4 | 70.5±31.7 | 0.12 |
| High Risk Category | 10 (37.0%) | 5 (20.0%) | 0.018 |
Higher SES scores (n=25) include one father.
WAIS-IV subtests scaled score mean 10 and standard deviation 3;
Mean ± SD;
n (%);
Pearson Chi-Square;
Percent of families in the census tract.
High Risk Categories were determined for environmental factors as follows: WAIS-IV subtest scores >1 SD below normative mean of 10; BDI-II Total score in moderate or severe range; PSS score ≥ 75th percentile; PSI-4 Life Stress score ≥ 75th percentile; Social Support ≤ 25th percentile; HOME Total score >1 SD below sample mean; HFI category of food insecure; CND≥ 75th Percentile. Number and percent show proportion of sample in high risk category for each factor.
Infant developmental outcome
Infant developmental functioning was assessed at 12 months of age utilizing the Bayley Scales of Infant Development III (BSID-III) and the Preschool Language Scale - 5th Edition (PLS-5). The BSID-III provides measurement of cognitive, language, and motor development and has a high degree of reliability, test-retest stability, and interrater agreement.16 The PLS-5 is a standardized measure of language function for children ranging in age from newborn to 7 years, 11 months and is commonly used in studies of language development in at-risk children.6 It provides Total Language, Auditory Comprehension, and Expressive Communication scores.17
This study was carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki) and informed consent was obtained from caregivers at time of enrollment. The privacy rights of participants were maintained at all times.
Statistical Analyses
Bivariate comparisons of scores for the Low and Higher SES groups were conducted for environmental factor variables and the outcome variables using t-tests and Chi Square tests. Pearson correlations were used to test relationships between outcomes and environmental factors.
We utilized multiple linear regression to determine if maternal, home, and neighborhood factors accounted for variance in outcomes after controlling for SES group. SES group was entered in step 1 of each model examined. In Model 1, environmental factors were entered in step 2, after controlling for SES. In Model 2, maternal cognitive function, a factor of particular interest, was evaluated in step 2 (after controlling for SES). With the exception of maternal cognitive function, if environmental factors showed no relationship with outcomes in Pearson correlations (p>0.10) they were not examined in regression analysis.
SES groups were compared for elevated risk for each environmental factor. High or low risk for each factor was determined using: 1) established categorical definitions of risk; 2) scores that corresponded to one standard deviation above or below the sample mean; or 3) scores in the bottom or top quartile of the sample distribution. Scores in the high risk range were assigned a value of 1 (High Risk Category: Table 2), and scores in the low risk range were assigned a value of 0. In addition to examining risk for each factor, cumulative risk scores for each participant were obtained by summing the nine risk category values, resulting in a score ranging from 0–9.5 The impact of cumulative risk on infant outcome was evaluated utilizing this variable in regression analyses controlling for SES status.
Our study was powered at 80%, with Type I error rate of 0.05, to detect a difference of 0.8 × standard deviation (SD) in outcome variables. Choice of a single sex, single race/ethnicity cohort preserved power through elimination of the need to control for these two confounders in analyses. Data were analyzed in SPSS (version 22).
RESULTS
Of the 60 participants enrolled at birth, fifty-two completed the 12-month follow up visit, 27 Low SES and 25 Higher SES. Of those not participating at the 12-month visit, 5 withdrew, 2 were not evaluated at 12 months, and 1 was lost to follow-up. The 8 who were not evaluated at 12 months were similar to those who were evaluated in maternal and infant characteristics (all p≥0.15), except for gestational age (39.4±0.9 and 40.3±1.2 wks, respectively, p=0.023).
Cohort Characteristics
By study design all Low SES infants were from homes with ITN at or below the poverty line. Higher SES infants were from families with ITN above the poverty line. Thirty seven percent of Low SES mothers had a high school diploma and the remaining 63% had not graduated from high school. Twenty percent of Higher SES mothers had only a high school diploma while the remaining 80% had some degree of higher education. Low SES mothers were younger than Higher SES mothers at time of delivery. Low and Higher SES infants were similar in birth parameters (Table 1).
Table 1.
Cohort Characteristics at Time of Enrollment
| Low SES | Higher SES | p-value | |
|---|---|---|---|
| Income-to-Needs | |||
| At or below poverty line | 27 (100%)a | 0 | -- |
| Above poverty line | 0 | 25 (100%) | -- |
| 100–199% of poverty line | - | 15(60%) | -- |
| ≥200% of poverty line | - | 10(40%) | -- |
|
| |||
| Education | |||
| Less than high school | 17 (63%) | 0 | |
| High school/GED | 10 (37%) | 5 (20%) | |
| Some college | 0 | 6 (24%) | |
| Two-year college degree | 0 | 8 (32%) | |
| Four-year college degree | 0 | 3 (12%) | |
| Graduate school | 0 | 3 (12%) | |
|
| |||
| Maternal age at delivery, yr. | 24.6 ± 5.1b | 28.5 ± 5.9 | 0.015 |
|
| |||
| Infant gestational age (wks) | 39.3 ± 0.9 | 39.6 ± 0.9 | 0.25 |
| Birth weight (kg) | 3.2 ± 0.3 | 3.4 ± 0.4 | 0.10 |
| Head circumference (cm) | 33.4 ± 1.4 | 34.1 ± 1.6 | 0.14 |
n (%),
Mean ± SD
Environmental Factors by Low and Higher SES
Low SES mothers scored significantly lower than Higher SES mothers on both the Vocabulary and Matrix Reasoning subtests of the WAIS-IV (p≤ 0.001)(Table 2). For the Vocabulary subtest, 59% of Low SES mothers scored more than one standard deviation below the mean, compared with 12% of the Higher SES mothers. On Matrix Reasoning, 37% of Low SES mothers scored more than one standard deviation below the mean compared with 4% of Higher SES mothers. On measures of social emotional functioning, the BDI-II scores were similar between groups (p=0.99), as were scores on the PSS (p=0.40). PSI-4 scores for the Low SES group were higher than those for the Higher SES group on the PSI-4 Total, Child and Parent Stress scales (p≤0.02) but similar for the PSI-4 Life Stress scale (p=0.71). Social Support was similar between the two groups (p=0.17). Assessment of household environment showed the HOME Total score to be lower in the Low SES group (p<0.001) with significant differences in three of six HOME subscales (p≤0.002). Levels of Food Insecurity and Concentrated Neighborhood Disadvantage were significantly higher for the Low SES group (p=0.012, p=0.027, respectively).
Environmental Risk Status
Percentage of Low SES infants in the High Risk Category for environmental factors was greater than Higher SES infants for eight of the nine factors and reached statistical significance in five of the nine factors (Table 2).
Comparison of Cognitive and Language Outcomes by Low and Higher SES
Five of six outcome scores were lower in Low SES group compared with Higher SES (Table 3). Of these, three were statistically lower: BSID-III Cognitive Composite (p=0.005), PLS-5 Total Language (p=0.017) and PLS-5 Auditory Comprehension (p=0.008). Overall, scores for the BSID-III Cognitive Composite were in the High Average range for the Higher SES group and in the Average range for the Low SES group. All other scores for both groups were in the Average range except PLS-5 Expressive Communication score that was in the Low Average range for Low SES infants.
Table 3.
Infant Developmental Outcome at Age 12 Months
| Low SES n=27 |
Higher SES n=25 |
p value | |
|---|---|---|---|
| Age at Testing (months) | 12.9 ± 0.5a | 12.9 ± 0.6 | .59 |
|
| |||
| Bayley Scales of Infant Development - III | |||
| Cognitive Composite | 107.2 ± 10.8 | 115.8 ± 10.4 | .005 |
| Language Composite | 97.6 ± 6.9 | 97.4 ± 8.9 | .93 |
| Motor Composite | 102.4 ± 12.1 | 107.9 ± 12.0 | .10 |
|
| |||
| Preschool Language Scale -5 | |||
| Total Language | 90.7 ± 6.4 | 94.8 ± 5.4 | .017 |
| Auditory Comprehension | 95.2 ± 6.3 | 99.0 ± 3.1 | .008 |
| Expressive Communication | 87.6 ± 8.0 | 91.6 ± 8.9 | .10 |
Mean ± SD
Regressions on Cognitive and Language Outcomes at age 12-Months
In regression models, SES effects were found for the BSID-III Cognitive Composite score and the PLS-5 Language Total and Auditory Comprehension Composite scores (all p<0.018) (Data not shown). SES effects remained significant (p≤0.040) after Maternal Vocabulary and Matrix Reasoning scores were added in model 2. When controlling for SES, no effects on outcomes were shown for maternal cognitive function (all p≥0.40) or environmental factors (all p≥0.16), including HOME subscales (all p≥0.052, data not shown). BSID-III Language Composite score and the PLS-5 Expressive Communication score (p>0.11) were not influenced by SES. (Table 4)
Table 4.
Multiple Regression Analyses on Developmental Outcome
| Model 1 | Model 2b | |||
|---|---|---|---|---|
| B(SE) | β(p-value) | B(SE) | β(p-value) | |
| BSID-III Cognitive Composite Score | ||||
| SES Groupa | 8.54(2.96) | 0.38(0.006) | 9.80(4.08) | .44(0.020) |
| Vocabulary | 0.037(0.62) | 0.011(0.95) | ||
| Matrix Reasoning | −0.39(0.60) | −0.11(0.52) | ||
|
| ||||
| BSID-III Language Composite Score | ||||
| SES Group | −0.68(2.24) | −0.044(0.76) | −1.50(3.04) | −0.097(0.62) |
| Vocabulary | 0.30(0.45) | 0.12(0.51) | ||
| Matrix Reasoning | 0.06(0.46) | 0.025(0.90) | ||
| PSI: Life Stress | −0.19(0.11) | −0.25(1.0) | ||
| Food Insecurity | −1.44(1.11) | −0.20(0.20) | ||
|
| ||||
| PLS-5 Language Composite Score | ||||
| SES Group | 2.15(2.15) | 0.17(0.32) | 4.89(2.31) | 0.40(0.040) |
| Vocabulary | −0.008(0.34) | −0.004(0.98) | ||
| Matrix Reasoning | −0.19(0.35) | −.0.99(0.59) | ||
| HOME Total | 0.35(0.25) | 0.25(0.16) | ||
|
| ||||
| PLS Auditory Comprehension Score | ||||
| SES Group | 2.15(1.87) | 0.20(0.26) | 5.42(1.94) | 0.51(.007) |
| Vocabulary | −0.24 (.28) | −0.14(0.40) | ||
| Matrix Reasoning | −0.17 (.30) | −0.10(.57) | ||
| HOME Total | 0.24(0.21) | 0.19(0.27) | ||
| Food Insecurity | −0.87(0.68) | −0.17(0.21) | ||
|
| ||||
| PLS Expressive Communication Score | ||||
| SES Group | 1.55(3.09) | 0.091 (0.62) | 3.84 (3.30) | 0.225 (0.25) |
| Vocabulary | 0.22(.49) | 0.083(0.65) | ||
| Matrix Reasoning | −0.18(.50) | −0.066(0.73) | ||
| Home Total | 0.43(0.36) | 0.22(0.24) | ||
SES group status variable used in the regression was coded as follows: Low SES group =0 and Higher SES group =1. Results for step 2 are shown.
Evaluated in step 2 of Model 2 as Maternal Cognitive function was a variable of particular interest.
Environmental factor variables were included in step 2 of models if p-value for Pearson correlation with outcome was less than or equal to 0.10.
Cumulative Risk and Infant Developmental Outcome
The boxplot shown in Figure 1 illustrates the comparison of the distribution of cumulative risk scores for SES groups which ranged from 0 to 8. Low SES infants differed from Higher SES infants in mean scores for cumulative risk (3.4 ± 1.8 versus 1.6 ± 1.4, p<0.001). In regression analyses cumulative risk was not associated with any measured outcome (all p≥0.11).
Figure 1.
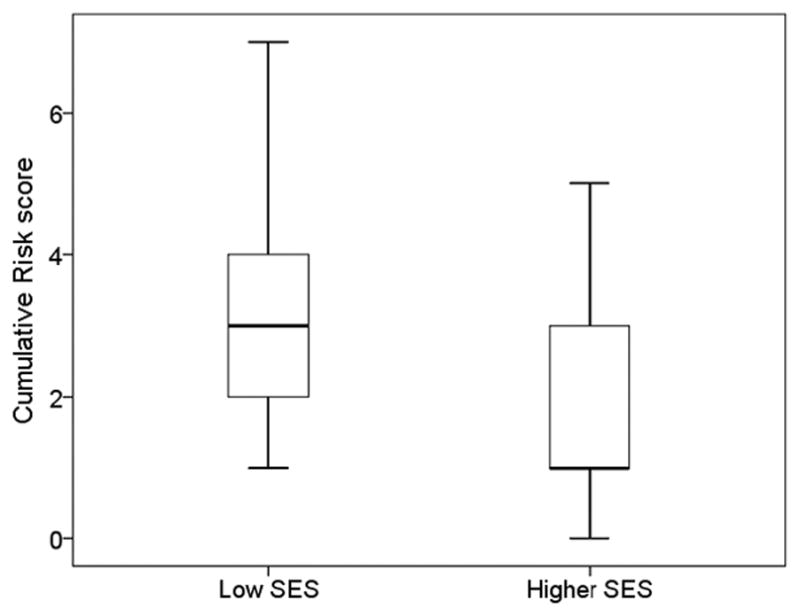
Cumulative Risk Score by SES Group
Legend: Boxplots show 25th, 50th and 75th percentiles for Cumulative Risk by SES group. The Cumulative Risk score is higher in Low SES compared to Higher SES infants (p<0.001).
DISCUSSION
In this investigation, by age one year, Low SES infants had been exposed to greater environmental disadvantage and were exhibiting poorer developmental function than Higher SES infants. Although this may not be surprising given the permanence of many elements of disadvantage, to our knowledge this study is the first to report on the maternal, home, and neighborhood environment during infancy, and to evaluate relationships with performance on standardized tests of infant development at age one year. Even at this early age, Low SES infants already were performing more poorly than Higher SES infants. This innovative set of results inform as most investigations of relationships between poverty and child outcome do not utilize a birth cohort of healthy term infants, are conducted at ages beyond infancy, do not include environmental data collected in the first year of life, and have not evaluated developmental outcome as early as one year of age.
Our goal was to explore effects of poverty in infancy and, if present, identify specific environmental factors influencing developmental outcome. By age 12 months the BSID-III Cognitive Composite and PLS-5 Total Language and Auditory Comprehension scores of the Low SES cohort were statistically significantly lower than scores of Higher SES. The mean BSID-III Cognitive Composite scores for both groups were within or above the average range, but the 8-point difference between Low and Higher SES was equivalent to at least a half standard deviation difference in outcome with a medium effect size of 0.57. These relative differences show the Low SES group is experiencing an early developmental disadvantage. As reported by others, this early divergence portends a more significant decline in cognitive development at later ages.
On the PLS-5, the Low SES mean scores also were within average range but were significantly lower than Higher SES on both Total Language and Auditory Comprehension. Effect sizes were 0.27 and 0.25, respectively. These results extend an earlier finding in this cohort showing Low SES infants performed less well than Higher SES (p≤ 0.012) on language assessments at age 7 months.18 Other investigations in young subjects have found differences in language performance related to SES status, although at ages beyond infancy. Wild19 found poorer language outcomes in prior preterm infants at age 22 months with Medicaid-type insurance compared with those with private insurance. Hoff 20 reported influence of SES, defined by parental education, on early vocabulary development via maternal speech in two-year-olds. As cited in Hurt 2016,6 researchers utilizing the Hollingshead Index to define SES, found more advanced vocabulary and language processing in children from high versus low SES at 18 months.
Although results from the current investigation showed significant differences between Low and Higher SES on the PLS Total Language and Auditory Comprehension scores, groups did not differ on the BSID Language Composite. One possible explanation for this discrepancy relates to item differences in the BSID-III and PLS-5 language scales. For example, items evaluating play are included in PLS-5 Auditory Comprehension and BSID-III Cognitive scales but not the BSID-III Language scale. In this regard, groups differed on PLS-5 relational play, observed in 64% of Low SES infants versus 96% of Higher SES infants (p=0.011, Fisher’s Exact Test). A second possibility may be related to differences between the standardization samples of the two tests: PLS-5 matches 2008 census data whereas the standardization sample for the BSID-III matches 2000 census data.16,17
Cognitive and language differences at this early age are particularly striking because the designated Higher SES group is actually relatively low SES. The National Center for Children in Poverty defines “poor” as families below the federal poverty threshold and “near poor” being between 100% and 199% of the federal poverty threshold. “Poor” and “near poor” taken together are considered “low income”.21 All cohort families in the Low SES group, by project design, were in the “poor” category. Sixty percent of the families in the Higher SES group met the “near poor” criterion with only 40 percent being above “low income” (Table 1). Thus, our ability to detect differences between the two groups, low and relatively higher SES, likely is an underestimation of differences that would be found between low SES and a true, higher SES group that consisted of only families above “low income”.
We evaluated environmental influences on outcome utilizing two approaches, regressions using individual risk factors, and a cumulative risk factor. In regressions controlling for SES no significant association between environmental factors and outcome were shown. These analyses, however, did show a marginal association between the Provision of Appropriate Play Materials HOME subscale and the PLS-5 Language Total and Auditory Comprehension scores (p<0.052) (Data not shown.) This finding, while marginal, is consistent with other studies showing similar relationships in older children. This subscale of the HOME Inventory is a measure of the presence or absence of toys and equipment available to the child and appropriate for their age. Lower scores on this scale may reflect several conditions in the home: insufficient financial resources for acquisition of such items, lack of knowledge regarding child development, and/or a less child-centered approach to household organization. The relation between this subscale and outcome is consistent with the importance of interventions targeting parenting practices and education regarding child development.22 Further, the relation is compatible with conceptualization of SES effects as a financial resource deficit, a finding raising the possibility that monetary resources could effect a difference in developmental outcome.23
Low SES demonstrated elevated risk in eight of the nine environment factors evaluated when compared with Higher SES (Table 2); of these, five reached statistical significance. Mean scores for cumulative risk, too, were higher in Low SES when compared with Higher SES. Although these results indicate early environmental disadvantage at age 1 year for children of lower SES, the cumulative risk score was not associated with BSID-III or PLS-5 scores. Previous investigations of effects of cumulative risk report relationships between number of risk factors and deleterious effects on child outcomes.5 The lack of effect of cumulative risk across all outcomes in our cohort may be due, in part, to our eligibility criteria. We enrolled only African American participants in both Low and Higher SES groups, thus eliminating race as a potential risk factor for compromised outcome.2,5 Based on study design, we also excluded other risk factors commonly linked to SES disparity and associated with deleterious effects on child outcome such as medical risk, teen motherhood, substance use, and significant psychological issues. 5 Further, another possibility for lack of effect of cumulative risk on outcome may relate to our method of assigning risk status: high-risk status for four of the nine factors examined was based on the distribution of our sample, not validated using external indicators of risk.
No discussion of factors affecting infant outcome would be complete without mention of genetic influence. Clearly our Low SES mothers’ verbal and matrix reasoning scores were low. Whether these scores reflect genetic influence or are themselves a product of environmental influence cannot be determined in our study. Moreover, we cannot determine the potential importance of genetic influence as compared to environmental influences on the infants in our cohort. In this regard, however, studies of older twin subjects have shown that environmental factors account for 60% of the variation in cognitive outcome of low SES children with genetic influence being negligible,24 a finding supported by similar investigations.25 Further, in the investigation reported here, maternal intelligence was not related to infant outcome.
The early divergence in developmental outcomes reported here, coupled with the anticipated decline in cognitive performance of children being raised in poverty, strongly underscores the importance of early intervention. The current emphasis on universal Pre-K is laudable, but these interventions may occur well after foundational developmental and neural patterns are in place.26 Programs that focus on younger ages, such as Early Head Start and Zero to Three, are directed at reducing the impact of SES disparities at very young ages.27 In a recent report, however, fewer than 4% of children eligible for Early Head Start were served.28 Relevant to providing intervention for the very young and their parents is our finding that developmental scores of Low SES infants, while diverging from Higher SES scores, actually were in the average range at one year of age. This finding suggests a window of opportunity for interventions to ameliorate or obviate the anticipated decline in developmental outcome of children growing up poor.3
Limitations
There are at least 4 limitations to this study. First, cohort size is a concern. By way of explanation, cohort size was constrained by the initial project goal to determine the neural effects of poverty through MRIs obtained at 1 and 12 months of age, a labor intensive and expensive endeavor.29 Second, to evaluate a homogeneous and healthy cohort for imaging purposes, we enrolled only American-born African American mothers and their female babies to avoid confounding by various race/ethnicities and sex in a small cohort. Our decision to enroll only female infants was both to reduce confounding by sex and to avoid bias associated with increased developmental risk in males at early ages.30 Third, our sample size may have affected our ability to detect combined effects of SES and environmental factors. In larger samples we anticipate that such associations could be detected. Last, our study was conducted in an inner-city setting that limits generalizations to other impoverished populations, such as the rural poor. Regardless of these limitations, the early divergence of developmental performance in our cohort, coupled with the well-established downward trajectory of cognitive outcome in older children growing up poor, suggests that the effects of poverty are present at very young ages.
CONCLUSION
Environmental disadvantages, maternal, home, and neighborhood, are present in abundance in the first year of life of children growing up poor. By age one year Low SES infants perform less well on cognitive and language evaluations than Higher SES infants. These findings suggest support for families and children from impoverished circumstances cannot begin too early. Findings reported here, from an urban, single sex and race/ethnicity cohort, need to be replicated in larger, more diverse cohorts in different locales.
Acknowledgments
All phases of this study were supported by NIH/NICHD: R21HD072461. The NIH/NICHD had no role in study design; collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
Footnotes
The authors have nothing to disclose.
CONFLICT OF INTEREST STATEMENT
Each author of this manuscript declares that she has no actual or potential conflict of interest including any financial, personal or other relationships with other people or organizations within that could inappropriately influence (bias) their work.
References
- 1.Brooks-Gunn J, Duncan GJ. The effects of poverty on children. Future Child. 1997;7(2):55–71. [PubMed] [Google Scholar]
- 2.Halle T, Forry N, Hair E, et al. Disparities in Early Learning and Development: Lessons from the Early Childhood Longitudinal Study – Birth cohort (ECLS-B) Washington, DC: Child Trends; Jun, 2009. [Google Scholar]
- 3.AAP Council on Community Pediatrics. Poverty and Child Health in the United States. Pediatr. 2016;137(4):e20160339. doi: 10.1542/peds.2016-0339. [DOI] [PubMed] [Google Scholar]
- 4.Urahn SK, Currier E, Elliott D, et al. Pursuing the American Dream: Economic Mobility Across Generations. The Pew Charitable Trusts; Jul, 2012. [Google Scholar]
- 5.Evans GW, Li D, Whipple SS. Cumulative risk and child development. Psychol Bull. 2013;139(6):1342–1396. doi: 10.1037/a0031808. [DOI] [PubMed] [Google Scholar]
- 6.Hurt H, Betancourt LM. Effect of socioeconomic status disparity on child language and neural outcome: how early is early? Pediatr Res. 2016;79(1–2):148–158. doi: 10.1038/pr.2015.202. [DOI] [PubMed] [Google Scholar]
- 7.Hackman DA, Farah MJ, Meaney MJ. Socioeconomic status and the brain: mechanistic insights from human and animal research. Nat Rev Neurosci. 2010;11(9):651–659. doi: 10.1038/nrn2897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wechsler D. Wechsler Adult Intelligence Scale -Fourth Edition. San Antonio, TX: Pearson; 2008. [Google Scholar]
- 9.Huston AC, McLoyd VC, Garcia Coll C. Poverty and Behavior: The Case for Multiple Methods and Levels of Analysis. Dev Rev. 1997;17(3):376–393. [Google Scholar]
- 10.Beck AT, Steer RA, Brown GK. Beck Depression Inventory II Manual. 2. San Antonio, TX: The Psychological Corporation; 1996. [Google Scholar]
- 11.Abidin R. PSI-4 Professional Manual. Lutz FL: Psychological Assessment Resources; 2012. [Google Scholar]
- 12.Dunst CJ, Trivette CM, Cross AH. Mediating influences of social support: personal, family, and child outcomes. Am J Ment Defic. 1986;90(4):403–417. [PubMed] [Google Scholar]
- 13.Caldwell BM, Bradley RH. Home Observation for Measurement of the Environment (HOME) Little Rock, AR: University of Arkansas at Little Rock; 1984. [Google Scholar]
- 14.Rose-Jacobs R, Black MM, Casey PH, et al. Household Food Insecurity: Associations With At-Risk Infant and Toddler Development. Pediatr. 2008;121(1):65–72. doi: 10.1542/peds.2006-3717. [DOI] [PubMed] [Google Scholar]
- 15.Sampson RJ, Sharkey P, Raudenbush SW. Durable effects of concentrated disadvantage on verbal ability among African-American children. Proc Natl Acad Sci U S A. 2008;105(3):845–852. doi: 10.1073/pnas.0710189104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bayley N. Bayley Scales of Infant and Toddler Development: Technical manual. 3. San Antonio TX: Harcourt Assessment; 2006. [Google Scholar]
- 17.Zimmerman IL, Steiner VG, Pond RE. Preschool Language Scales, Fifth Edition (PLS-5) San Antonio, TX: Pearson Clinical Assessment Group; 2011. [Google Scholar]
- 18.Betancourt LM, Brodsky NL, Hurt H. Socioeconomic (SES) differences in language are evident in female infants at 7months of age. Early Hum Dev. 2015 doi: 10.1016/j.earlhumdev.2015.08.002. [DOI] [PubMed] [Google Scholar]
- 19.Wild KT, Betancourt LM, Brodsky NL, et al. The effect of socioeconomic status on the language outcome of preterm infants at toddler age. Early Hum Dev. 2013;89(9):743–746. doi: 10.1016/j.earlhumdev.2013.05.008. [DOI] [PubMed] [Google Scholar]
- 20.Hoff E. The specificity of environmental influence: socioeconomic status affects early vocabulary development via maternal speech. Child Dev. 2003;74:1368–1378. doi: 10.1111/1467-8624.00612. [DOI] [PubMed] [Google Scholar]
- 21.Jiang Y, Ekono M, Skinner C. Basic Facts About Low-Income Children: Children under 6 Years. New York, NY: 2013. [Google Scholar]
- 22.Raikes H, Green BL, Atwater J, et al. Involvement in Early Head Start home visiting services: Demographic predictors and relations to child and parent outcomes. Early Childhood Res Q. 2006;21(1):2–24. [Google Scholar]
- 23.Noble KG, Houston SM, Brito NH, et al. Family income, parental education and brain structure in children and adolescents. Nat Neurosci. 2015;18(5):773–778. doi: 10.1038/nn.3983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Turkheimer E, Haley A, Waldron M, et al. Socioeconomic status modifies heritability of IQ in young children. Psychol Sci. 2003;14(6):623–628. doi: 10.1046/j.0956-7976.2003.psci_1475.x. [DOI] [PubMed] [Google Scholar]
- 25.Tucker-Drob EM, Rhemtulla M, Harden KP, et al. Emergence of a Gene × socioeconomic status interaction on infant mental ability between 10 months and 2 years. Psychol Sci. 2011;22(1):125–133. doi: 10.1177/0956797610392926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Johnson MH, Mareschal D. Cognitive and perceptual development during infancy. Curr Opin Neurobiol. 2001;11(2):213–218. doi: 10.1016/s0959-4388(00)00199-9. [DOI] [PubMed] [Google Scholar]
- 27.Zero to Three. [Accessed August 4, 2015];Infants and Toddlers in Early Head Start. 2009 http://www.zerotothree.org/public-policy/policy-toolkit/ehssinglesmar5.pdf.
- 28.Schmit S, Matthews H, Smith S, et al. Investing in Young Children: A Fact Sheet on Early Care and Education Participation, Access, and Quality. Vol. 2013 New York, NY: Nov, 2013. [Google Scholar]
- 29.Betancourt LM, Avants B, Farah MJ, et al. Effect of socioeconomic status (SES) disparity on neural development in female African-American infants at age 1 month. Dev Sci. 2016;19(6):947–956. doi: 10.1111/desc.12344. [DOI] [PubMed] [Google Scholar]
- 30.Ozcaliskan S, Goldin-Meadow S. Sex differences in language first appear in gesture. Dev Sci. 2010;13(5):752–760. doi: 10.1111/j.1467-7687.2009.00933.x. [DOI] [PMC free article] [PubMed] [Google Scholar]