

Abstract
Rationale:
Kaposiform hemangioendothelioma (KHE) is an aggressive vascular tumor, mainly occurring in infants and young children and previously reported cases were mainly cutaneous or visceral form. Intestinal kaposiform hemangioma was first reported in 2012. Intestinal type KHE showed better prognosis if the lesion was limited in the gastrointestinal tract and coagulopathy was not accompanied. Since the number of reported cases is small, further study for treatment options and prognosis need to be done.
Patient concerns:
We described the case of a 1-month-old female who had abdominal distention and bilious vomiting.
Diagnoses:
She was suspected as intestinal obstruction after diagnostic work up.
Interventions:
Surgical exploration was performed and jejunal obstruction with a mass was identified. Small bowel segmental resection and anastomosis was performed.
Outcomes:
The patient discharged with symptom free. Through the pathological examination, the mass was identified as intestinal type KHE.
Lessons:
Intestinal KHE can cause bowel obstruction and be managed successfully with complete surgical resection. More cases should be reported and further evaluation for treatment options and prognosis evaluation is necessary.
Keywords: gastrointestinal tracts, kaposiform hemangioendothelioma, Kasabach–Merritt syndrome
1. Introduction
Kaposiform hemangioendothelioma (KHE) is rare vascular neoplasm mainly occurs in infants and young children.[1] KHE is an aggressive vascular proliferation that has common features to both capillary hemangioma and Kaposi sarcoma[2] and is a biologically borderline malignant tumor due to its rapid infiltrative growth.[3] These lesions are characterized by irregular tumor nodules which are composed of spindle-shaped endothelial cells with abundant eosinophilic cytoplasm that form cresenteric vascular spaces and fragmented red cells.[4]
Since 1993, when KHE was first defined by Zuckerberg et al, less than 183 cases have been reported in English-language literature.[5] Most of them are cutaneous or visceral forms and intestinal KHE is very rare.[3] Intestinal KHE was first reported in 2012 in a 3-year-old boy found in jejunum. To our knowledge, this is the 4th case and the youngest patient of KHE in the gastrointestinal tract.[1,3,5]
2. Case report
A 1 month-old female infant with body weight around 3.5 kg presented to emergency room due to projectile bilious vomiting for 11 days. She was born as a full-term baby without perinatal problems. On the 19th day after birth, she had abdominal distention with nonbilious vomiting, and the vomitus had changed to projectile and bilious pattern.
When admitted, initial vital sign and laboratory tests such as complete blood count, liver function tests, and C-reactive protein were normal. An infant gram showed diffuse dilatation of bowel loops (Fig. 1). Abdominal ultrasonography showed diffuse dilatation of proximal small bowel accompanied by inflammatory change of bowel loops which suggests possible partial small bowel obstruction at the level of distal jejunum to proximal ileum (Fig. 2).
Figure 1.

Infantogram of the patient showing small bowel distension.
Figure 2.

Ultrasonographic findings showing segmental wall thickening of the small bowel (arrows) and dilatation of the upstream small bowel (arrow heads).
Surgical exploration was performed on the next day, and a 4.0 × 2.5 cm-sized reddish spongious solid mass lesion on small bowel wall, 60 cm distal from Treitz ligament, was identified with extension to nearby mesentery (Fig. 3). Proximal small bowel from the lesion was markedly dilated with distal bowel collapse. Jejunal segmental resection including the mass lesion and end-to-end jejuno-jejunal anastomosis was done. On postoperative 6th day, the patient started diet and discharged on postoperative 13th day without any complications.
Figure 3.

Operative finding. Markedly dilated proximal small bowel with solid mass lesion on small bowel wall.
On pathologic report, the excised tumor measured as 4.0 × 2.5 × 1.0 cm, and infiltrated from submucosa to subserosa. In the gross findings, the luminal surface was hypertrophic and spongious, and looked like hemangioma (Fig. 4A). A poorly circumscribed and infiltrative mass which consists of irregular vascular lobules that extends from submucosa to subserosa was observed in the microscopic findings. In higher magnification, monomorphic spindle-shaped endothelial cells that adjacent slit like vessels formed glomeruloid clusters which are typical in KHE. Some fragmented red cells and fibrin thrombi were also present (Fig. 4B).
Figure 4.
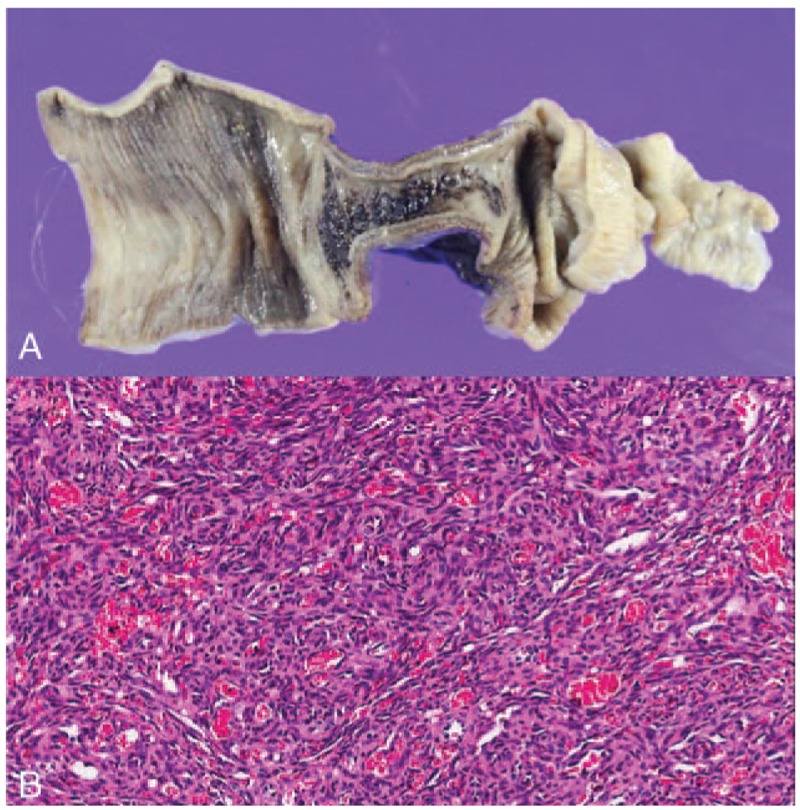
(A) Gross finding. 4.0 × 2.5 × 1.0 cm sized mass infiltrating submucosa to subserosa and hypertrophied luminal surface, (B) microscopic findings in high magnification, and irregular spindle-shaped endothelial cells forming glomeruloid clusters.
To confirm the diagnosis, imunohistochemical study was performed. The tumor was positive for cluster of differentiation 31 and friend leukemia integration 1 transcription factor (FLI-1), and was negative for glucose transporter 1 and human herpesvirus 8. Morphometric analysis revealed that 19.62% of tumor cells were positive for Ki-67 staining (Fig. 5). Thus, this tumor was pathologically diagnosed as KHE.
Figure 5.

Imunohistochemical study: positive for (A) CD31, (B) FLI-1, and (C) Ki-67 staining, and negative for (D) GLUT-1. CD31 = cluster of differentiation 31, FLI-1 = friend leukemia integration 1, GLUT-1 = glucose transporter 1.
3. Discussion
Since 1993 when the KHE was first defined by Zuckerberg et al, 183 cases of KHE have been reported.[5] Among these cases, cutaneous form was most common, followed by retroperitoneal or mediastinal form, and there were no reports about intestinal KHE until 2012.[1,2] Only 4 cases of intestinal KHE including our patient, 2 in small bowel, 1 in cecum, and 1 in multiple gastrointestinal tract, have been reported since then (Table 1).
Table 1.
Reported intestinal kaposiform hemangioendothelioma.

Three of these patients except Kajiwara et al's case showed vomiting as the main symptom, and the lesions originated from gastrointestinal tract. They had complete surgical excision and were all alive. Kajiwara et al reported a case of multiorgan involvement of KHE including mediastinum, para-aortic lesion, and retroperitoneum infiltrating into multiple gastrointestinal tract without definite identifiable site of origin. Anemia and bloody stool were main symptoms, and after combination therapy with vincristine and propranolol, tumor reduction was observed.
To date, the therapeutic options for KHE have been limited by lack of knowledge on the disease entity due to the rarity of this neoplasm.[6] If it is possible, surgical excision is the most successful therapeutic option.[7]
Excision of skin and soft tissue KHE was curative in 4 patients described by Zuckerberg et al.[7] When cutaneous lesion is widely dispersed on extremities with infiltrating into deeper tissues, it cannot be surgically resected completely. In these circumstances, applying chemotherapeutic agents such as vincristine can be effective.[8,9] Rapamycin is applied more recently for treating cutaneous KHE, because it is efficient in the treatment of lymphangiogenic disease and acts as mechanistic target of rapamycin inhibitor in the treatment of vascular anomalies.[10] If the lesion is associated with Kasabach–Merritt syndrome (KMS), aggressive medical treatment such as ticlopidine[8] and embolization could be followed after surgical resection.[9]
Therapeutic guidelines for intestinal KHE have not been well established even more than other forms. So far, if there were no evidence of KMS, surgical excision becomes the 1st-line treatment in the resectable tumors, and the reported 4 cases of intestinal KHE in Table 1 were treated mainly with surgical excision except Kajiwara et al's one.
Prognosis of KHE is affected by 2 factors, locations of lesion and presence of KMS. Recently reported cutaneous KHE patients are all cured and alive even with KMS for 1 to 3-year follow-up.[9] Mediastinal and retroperitoneal KHE tend to infiltrate into deeper soft tissue to make large extensive unresectable lesions.[2] They are accompanied by KMS in high frequencies to present with poor prognoses.[2]
Reported intestinal type KHE, even though the number of listed cases are small, has no relation with KMS so far if the lesion is limited in gastrointestinal tract only.[4] These findings made us to expect intestinal KHE might have better prognosis than other forms of KHE. Of course, more cases should be reported, and further evaluation for treatment options and prognosis evaluation is necessary.
Footnotes
Abbreviations: KHE = kaposiform hemangioendothelioma, KMS = Kasabach–Merritt syndrome.
Comment: Study approval from institutional review board of Seoul National University Hospital was waived due to the nature of this study, a case report.
The authors have no funding and conflicts of interest to disclose.
References
- [1].Kurian JJ, Kishore R, John TJ, et al. A rare case of kaposiform hemangioendothelioma presenting as intussusception in a 4-month-old child without Kasabach–Merrit syndrome: a case report. J Indian Assoc Pediatr Surg 2014;19:233–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Iwami D, Shimaoka S, Mochizuki I, et al. Kaposiform hemangioendothelioma of the mediastinum in a 7-month-old boy: a case report. J Pediatr Surg 2006;41:1486–8. [DOI] [PubMed] [Google Scholar]
- [3].Kajiwara R, Yokosuka T, Sasaki K, et al. Kaposiform hemangioendothelioma infiltrates the gut wall: a rare case report. J Pediatr Hematol/Oncol 2014;36:657–8. [DOI] [PubMed] [Google Scholar]
- [4].Nakaya T, Morita K, Kurata A, et al. Multifocal kaposiform hemangioendothelioma in multiple visceral organs: an autopsy of 9-day-old female baby. Hum Pathol 2014;45:1773–7. [DOI] [PubMed] [Google Scholar]
- [5].Odgaard HS, Christensen MK, Gade J. [Kaposiform haemangioendothelioma in the small intestine of a three year-old boy]. Ugeskrift Laeger 2012;174:1679–80. [PubMed] [Google Scholar]
- [6].Fernandez Y, Bernabeu-Wittel M, Garcia-Morillo JS. Kaposiform hemangioendothelioma. Eur J Intern Med 2009;20:106–13. [DOI] [PubMed] [Google Scholar]
- [7].Vin-Christian K, McCalmont TH, Frieden IJ. Kaposiform hemangioendothelioma. An aggressive, locally invasive vascular tumor that can mimic hemangioma of infancy. Arch Dermatol 1997;133:1573–8. [DOI] [PubMed] [Google Scholar]
- [8].Barabash-Neila R, Garcia-Rodriguez E, Bernabeu-Wittel J, et al. Kaposiform hemangioendothelioma with Kasabach–Merritt phenomenon: successful treatment with vincristine and ticlopidine. Indian J Pediatr 2012;79:1386–7. [DOI] [PubMed] [Google Scholar]
- [9].Shen W, Cui J, Chen J, et al. Treating kaposiform hemangioendothelioma with Kasabach–Merritt phenomenon by intralesional injection of absolute ethanol. J Craniofac Surg 2014;25:2188–91. [DOI] [PubMed] [Google Scholar]
- [10].Kai L, Wang Z, Yao W, et al. Sirolimus, a promising treatment for refractory Kaposiform hemangioendothelioma. J Cancer Res Clin Oncol 2014;140:471–6. [DOI] [PubMed] [Google Scholar]