

Abstract
The aim of this study is to investigate the incidence and pattern of traumatic fractures (TFs) as a result of falls in a population of children and adolescents (≤18 years old) in China.
This was a cross-sectional study. We retrospectively reviewed 1412 patients who were children and adolescents with TFs as a result of falls admitted to our university-affiliated hospitals in China from 2001 to 2010. Etiologies included high fall (height ≥2) and low fall (height <2 m). The incidence and pattern were summarized with respect to different age groups, year of admission, etiologies, genders, and the neurological function.
This study enrolled 1054 males (74.6%) and 358 females (25.4%) aged 10.8 ± 4.7 years. The etiologies were low fall (1059, 75.0%) and high fall (353, 25.0%). There were 2073 fractures in total and 92 patients (6.5%) presented with multiple fractures. The most common fracture sites were upper extremity fractures in 814 patients (57.6%) and lower extremity fractures in 383 patients (27.1%), followed by craniofacial fractures in 233 patients (16.5%). A total of 231 (16.4%) patients suffered a nerve injury. The frequencies of early and late complications/associated injuries were 19.5% (n = 275) and 9.2% (n = 130). The frequencies of emergency admission, nerve injury, spinal fracture, lower extremity fractures, craniofacial fracture, sternum and rib fracture, and early complications/ASOIs were significantly larger in high fall than low fall (all P <.001, respectively). The frequencies of medical insurance rate (P = .042) and upper extremity fractures (P <.001) were significantly larger in low fall than high fall. The frequencies of spinal fracture (P = .039), lower extremity fractures (P = .048), and craniofacial fracture (P = .041) were significantly larger in female than the male patients. The frequency of upper extremity fractures (P <.001) and the mean age (P <.001) was significantly larger in male than female patients. The frequencies of emergency admission, high fall, spinal fracture, and craniofacial fracture were significantly larger in patients with nerve injury than other patients without nerve injury (all P <.001, respectively).
Low falls and upper extremity fractures were the most common etiologies and sites, respectively. High fall, spinal fracture and craniofacial fracture were risk factors for nerve injury. Therefore, we should focus on patients who were caused by high fall and presented with spinal and craniofacial fracture to determine the presence of a nerve injury so that we can provide early, timely diagnosis and targeted treatment to children.
Keywords: adolescent, children, fall, fracture, nerve injury
1. Introduction
Falls are one of the main causes of trauma-related hospitalizations and client to emergency departments among the 0- to 18-year-old children.[1–8] In high-income countries, injuries due to falls are the 14th leading cause of disability-adjusted life years for all age groups combined.[9] In developing countries, falls accounted for 25% to 52% of all treated child injuries in hospitals.[10] Falls can result in serious consequences for children, including fractures, permanent neurological impairment, death, and serious lifetime cognitive and physical disabilities.[11–16] Fractures are common among all the pediatric injuries and they comprise 10% to 25%.[17,18] Some studies have shown an increasing incidence of pediatric fractures at specific sites.[19–22] However, population-based data on overall pattern and epidemiological trends of traumatic fractures (TFs) resulting from falls in children and adolescents are scarce.
Although fractures due to falls account for a small proportion of injuries among children, many of them are preventable by modifying the environment and strengthening the education. We believe that the changes of incidence are partly explained by children's activity patterns. Further investigations may help to identify preventive measures to reduce the incidence of TFs involving falls. So the pattern and epidemiologic trends of TFs resulting from falls and the related nerve injury is important for prevention and education. In the present study, we reviewed a multicenter database of falls in a population of children and adolescents ≤18 years of age that happened over a 10-year period between 2001 and 2010 in China. The incidence and pattern were summarized with respect to the different age groups, year of admission, etiologies, genders, and the neurological function to provide information on this important childhood public health problem in China.
2. Materials and methods
2.1. Study population
We retrospectively reviewed 2502 children and adolescents (≤18 years old) who presented with fractures between January 2001 and December 2010 and who were admitted to our university-affiliated hospitals, and among which 1412 patients had TFs that resulted from falls (Fig. 1). The patients included all children and adolescents who presented with TFs admitted as inpatients and patients treated as outpatients in the emergency clinic were not included because electronic medical records about emergency patients are not available. Our study population represented referrals from other hospitals and it also included an unselected group of patients. Chongqing Municipality is a city located in southwest China. The data were collected from Third Military Medical University-affiliated hospitals, which are the 2 largest public tertiary hospitals located in the Shapingba District. The Shapingba District is a core district located in the northwest region of Chongqing. We searched the ID numbers of all patients (≤18 years old) presented with fractures in the medical records system, and then the medical records were reviewed and assessed by 2 independent doctors who had not participated in treating any patients according to the ID numbers to extract the data such as etiology, gender, age, ASIA score, fracture sites, and nerve injury. We made definitive diagnoses of TFs in patients using x-rays, computed tomography (CT), and magnetic resonance imaging (MRI). Etiologies included high fall (height ≥2) and low fall (height <2 m). The American Spinal Cord Injury Association (ASIA) scoring standard was used to assess spinal cord injury. The traumatic brain injuries (TBIs) were divided into closed craniocerebral injury (CCI) and open craniocerebral injury (OCI). CCI includes cerebral concussion, cerebral contusion and laceration, and brainstem injury. Multiple fractures meant fractures happen in >1 part such as spine, upper limbs, lower limbs, craniofacial part, and sternum/rib. The study protocol and this manuscript were approved by the committee on ethics and the institutional review board of our institution.
Figure 1.
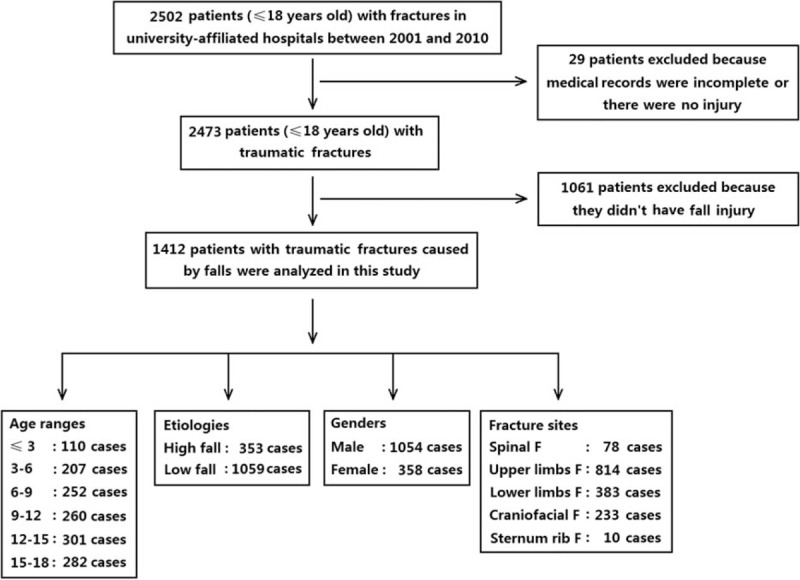
Patient flow diagram.
2.2. Statistical analysis
All statistical analyses were performed using SPSS version 22.0 (SPSS, Inc, Chicago, IL). Pearson χ2 tests were conducted for assessing differences in age, sex distribution, and clinical characteristics between the 2 groups. The continuous variables such as current age were expressed as mean ± standard deviation (SD) and differences between 2 groups were evaluated using independent samples t-test because the data were normally distributed.
3. Results
3.1. Demographic features and general characteristics
The study included 1412 patients (1054 males and 358 females) with a mean age of 10.8 ± 4.7 years and a sex ratio of 2.9:1. The most common etiology was low fall (1059, 75.0%) and the other was high fall (353, 25.0%). There were 2073 fractures in total and 92 patients (6.5%) presented with multiple fractures. The most common fracture sites were upper extremity fractures in 814 patients (57.6%) and lower extremity fractures in 383 patients (27.1%), followed by craniofacial fractures in 233 patients (16.5%). Among the patients who presented with upper extremity fractures, humeral fractures were seen in 414 cases (29.3%), radial fractures in 272 cases (19.3%), ulnar fractures in 232 cases (16.4%), fractures of the clavicle in 69 cases (4.9%), metacarpal fractures in 14 cases (1.0%), and phalangeal fracture in 3 cases (0.2%). Among the patients who presented with lower extremity fractures, femoral fractures were seen in 175 cases (12.4%), tibia fractures in 136 cases (9.6%), fibular fractures in 69 cases (4.9%), calcaneal fractures in 28 cases (2.0%), pelvic fractures in 23 cases (1.6%), patellar fractures in 19 cases (1.3%), and talar fractures in 10 cases (0.7%). Among the patients who presented with craniofacial fractures, parietal fractures were seen in 51 cases (3.6%), temporal fractures in 50 cases (3.5%), occipital fractures in 48 cases (3.3%), basilar skull fractures in 43 cases (3.0%), and frontal fractures in 34 cases (2.4%). There were mandible fractures in 49 cases (3.5%), nasal fractures in 14 cases (1.0%), maxillary fractures in 10 cases (0.7%), orbital fractures in 10 cases (0.7%), and zygomatic fractures in 6 cases (0.4%).
A total of 231 (16.4%) patients suffered a nerve injury. Among the patients who presented with a nerve injury, brain injury were seen in 137 cases (9.7%), spinal cord injury in 27 cases (1.9%), cranial nerve injury in 7 cases (0.5%), and spinal nerve injury, in 67 cases (4.7%). A total of 275 (19.5%) patients presented with early complications/associated injuries (ASOIs) and 130 patients (9.2%) presented with late complications/ASOIs. Early complications/ASOIs included nerve injury (n = 231), hemorrhagic shock (n = 7), lung injury (n = 26), splenic injury (n = 3), osteofascial compartment syndrome (n = 6), renal injury (n = 6), retroperitoneal hematoma (n = 6), liver injury (n = 4), and cardiac injury (n = 1). Late complications/associated injuries included infection (n = 30), decubitus ulcers (n = 2), fracture malunion (n = 78), fracture nonunion (n = 13), traumatic arthritis (n = 1), myositis ossificans (n = 5), and death (n = 3).
The incidences had a little seasonal variation and an obvious time variation, with peaks in autumn (28.4%) and 16 to 20 post meridiem (PM) (32.7%). The seasonal distribution map showed that autumn accounted for 28.4%, summer accounted for 27.3%, spring accounted for 23.5%, and winter accounted for 20.8%. The time distribution map showed that 16 to 20 accounted for 32.7%, 12 to 16 accounted for 30.3%, 8 to 12 accounted for 19.3%, 20 to 24 accounted for 10.4%, and other time accounted for 7.3% (Fig. 2).
Figure 2.
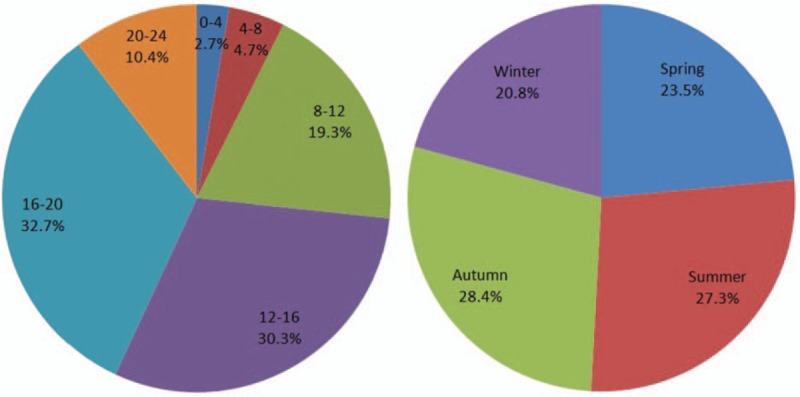
Time and season distribution.
3.2. Characteristics respect to different age groups
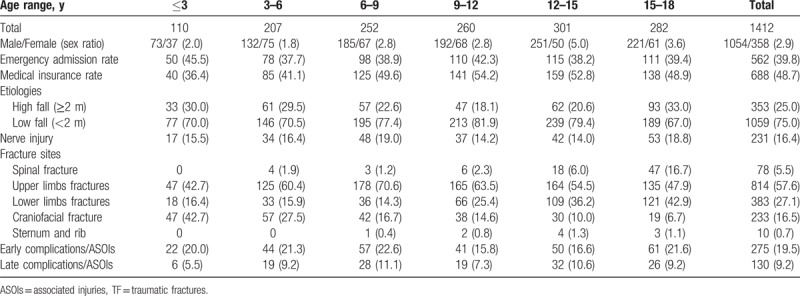
The most common age group was the 12 to 15 year age group (301, 21.3% of all patients) and the patients in the age group had the largest sex ratio of 5.0. The patients in the 4 to 6 year age group had the lowest sex ratio of 1.8. The frequency of emergency admission was the highest in the ≤3 year age group (45.5%) and lowest in the 3 to 6 year age group (37.7%). The frequency of medical insurance was low in the ≤3 year age group (36.4%) and highest in the 13 to 15 year age group (52.8%). The frequency of spine fractures was significantly higher in the 15 to 18 year age group (n = 47, 16.7%) than the other groups (all P <.001). The frequency of upper extremity fracture was significantly higher in 6 to 9 year age group (n = 178, 70.6%) than the other groups (all P <.05) except for 9 to 12 year age group. The frequency of lower extremity fractures was significantly higher in 15 to 18 year age group (n = 121, 42.9%) than the other groups (all P <.001) except for 12 to 15 year age group. The frequency of craniofacial fracture was significantly higher in the ≤3 year age group (n = 47, 42.7%) than the other groups (all P <.01) (Table 1).
Table 1.
Characteristics of 1412 TFs resulting from falls according to different age range groups.
3.3. Characteristics respect to different year of admission, etiologies, and gender
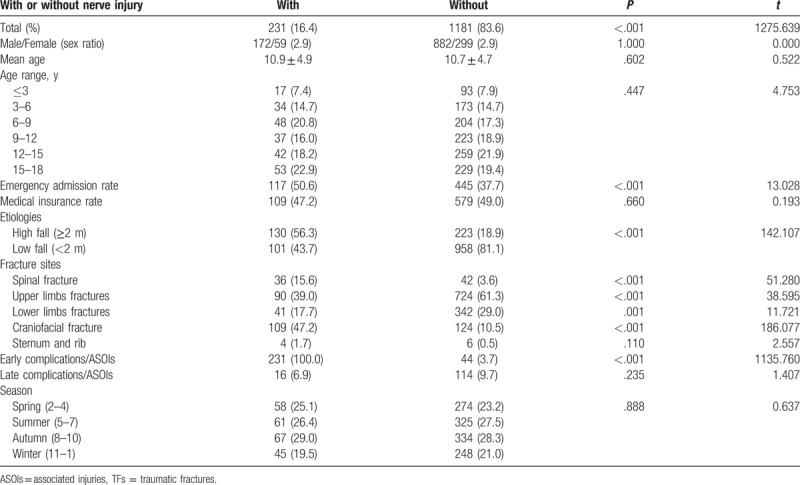
The overall annual incidence of children and adolescent fractures was (1316.1 ± 597.4) cases per 1,000,000 hospital admission per 2 years. Annual incidence rates increased exponentially with year of admission from 322.1 to 1474.2 cases per 1,000,000 hospital admission per 2 years. The frequency of emergency admission was gradually increased from 26.3% to 41.2% with the year of admission. The frequency of medical insurance was significantly increased from 26.3% to 66.8% (P <.001) with the year of admission (Table 2). The frequencies of emergency admission, nerve injury, spinal fracture, lower extremity fractures, craniofacial fracture, sternum and rib fracture, and early complications/ASOIs were significantly larger in high fall than low fall (all P <.001, respectively). The frequencies of medical insurance (P = .042) and upper extremity fractures (P <.001) were significantly larger in low fall than high fall (Table 3). The frequencies of spinal fracture (P = .039), lower extremity fractures (P = .048), and craniofacial fracture (P = .041) were significantly larger in female than the male patients. The frequency of upper extremity fractures (P <.001) and mean age (P <.001) was significantly larger in male than female patients (Table 4). Patients with nerve injury presented with significantly larger frequencies of emergency admission, high fall, spinal fracture, and craniofacial fractures (all P <.001, respectively) than the other patients without nerve injury (Table 5).
Table 2.
Characteristics of 1412 TFs resulting from falls according to different year of admission.
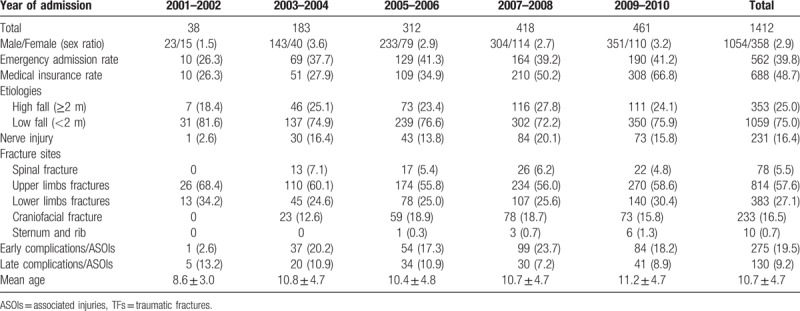
Table 3.
Characteristics of 1412 TFs resulting from falls according to different etiologies.
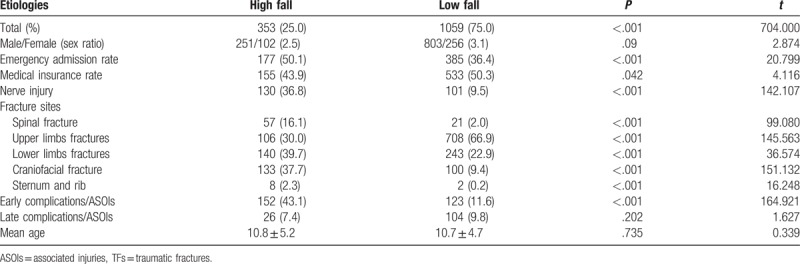
Table 4.
Characteristics of 1412 TFs resulting from falls according to different genders.
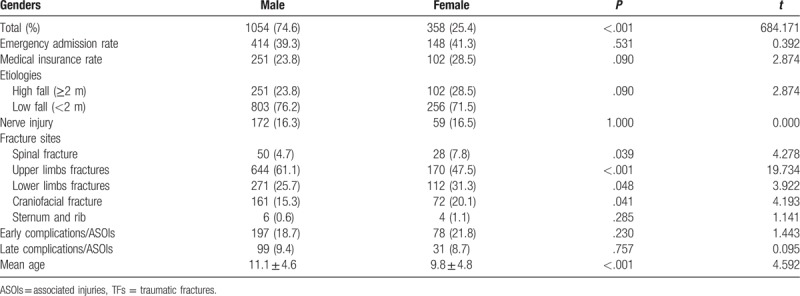
Table 5.
Characteristics of 1412 TFs resulting from falls according to nerve injury.
4. Discussion
China is a rapidly developing country undergoing significant economic expansion. Chongqing Municipality is a city of 31,442,300 located in southwest China, and the rural population accounted for 61.7% in 2009. The rural residents account for mean 55.1% and 56.9% in Chongqing. So we think that these 2 particular hospitals which were the 2 biggest public tertiary hospitals located in Shapingba District in Chongqing can represent a typical urban/rural setting in China. Fractures are a common problem in children and adolescent, rates are higher among boys than girls with a sex ratio of 2.9 in the study, and the results are in concordance with previous published data.[23] Male incidence rates peak later than those among females, the results were consistent with previous study.[24] The patients in the 15 to 18 year age group had the highest frequency of spinal fracture and complications/ associated injuries. The combinations of extrinsic and intrinsic factors which vary with age are the causes of fractures.[21] The incidences had a little seasonal variation and an obvious time variation, with peaks in autumn (28.4%) and 16 to 20 PM (32.7%). The results were partly consistent with previous study.[25] We believe the pattern of TFs among the children and adolescent is partly explained by children's activity patterns and whether the time is rush hour or dismissal time. Also, the number of patients treated for fall-related fractures increased with age and a higher incidence of injuries among children happened during the autumn and summer months. Although fractures due to falls account for a small proportion of injuries among children, resulting in serious injury including death, many of them are preventable by modifying the environment and strengthening the education including increasing public awareness and caregiver education. Consideration should also be given to legislative strategies that have shown success in other cities and states.[24,26–30]
The most common fracture sites were upper extremity fractures (57.6%) and lower extremity fractures (27.1%), followed by craniofacial fracture (16.5%). The results were consistent with previous study which showed that most of the fractures (73%) involved upper and lower extremities (22%).[29] Most studies showed that forearm fracture was the most common diagnosis,[30] but the fractures in the studies were caused by all etiologies, not only fractures caused by fall. High fall presented with significantly larger frequencies of spinal fracture, lower extremity fractures, and craniofacial fracture than low fall, but on the contrary, in the frequency of upper extremity fractures. So, we can see that spinal fracture, lower extremity fractures, and craniofacial fracture most common happen in high fall which with greater violence, upper extremity fractures most common happen in low fall during which people are used to contacting the ground with hands to support their bodies. In the present study, the number of patients presented with TFs increased with age from 110 to 282. Frequencies of spine fractures in the 15 to 18 year age group and craniofacial fracture in the ≤3 year age group were significantly higher than the other groups. So, we should focus on patients in the 15 to 18 year age group whether there are spine fractures and in the ≤3 year age group whether there are craniofacial fractures when they come to the hospitals. Frequencies of spinal fracture, lower extremity fractures and craniofacial fracture were significantly larger in female than male patients. The frequency of upper extremity fractures and mean age was significantly larger in male than the female patients. So, we can see that the pattern of fractures among the patients caused by falls has its own characteristics according to different etiologies, age groups, and genders, so targeted intervention methods should be taken to decrease the incidence and burden of falls.
In our study population, the frequencies of nerve injury, early complications/ASOIs, and late complications/ASOIs were 16.4%, 19.5%, and 9.2%, respectively. The patients in the 6 to 9 and 15 to 18 year age groups had the highest frequency of nerve injury (19.0% and 18.8%, respectively). Patients with nerve injury presented with significantly larger than the other patients without nerve injury in the emergency admission rate, frequency of high fall, spinal fracture, and craniofacial fractures. Falls can result in serious consequences for children, including fractures, permanent neurological impairment, death, and serious lifetime cognitive and physical disabilities.[11–17] Therefore, focusing on risk factors such as high fall, spinal fracture, and craniofacial fractures and modes of prevention is important; prevention and education play an important role in decreasing children's disabilities. The 3 most common early complications/ASOIs were nerve injury (16.4%) and lung injury (1.8%). The most common late complications were fracture malunion (5.5%) and infection (2.1%). The frequency of early complications/ASOIs was significantly larger in high fall than low fall. The timely discovery and correction of uncontrolled hemorrhagic shock, timely treatment of pulmonary contusion, and prevention and treatment of infections are all important for the treatment of TFs among the patients who are children or adolescents.
This study has several limitations. First, it was limited by the retrospective study design and by the small sample size. Second, the patients included all children and adolescent patients admitted as inpatients and patients treated as outpatients in the emergency clinic were not included because electronic medical records about emergency patients are not available. Third, there may be selection bias because this study includes patients who were referred to our teaching hospitals. Although there were several limitations, but our study was the most recent study to show the incidence and pattern of child and adolescent TFs as a result of falls in China. It provided initial information on this important childhood public health problem. Injury should be attributed to poor awareness of the injured children, their parents, and teachers, who should pay more attention to injury prevention and take some relevant measures for causes of injury in school children.[30] Results of the study showed that incidence of injury could be effectively controlled after we know more about the causes of injury and take effective measures.[30] In the near future, other researchers will take multicenter study including many cities to show more comprehensive information according to our study, all investigations may help to identify preventive measures to reduce the incidence of fractures involving falls among child and adolescent.
5. Conclusions
Low fall and upper extremity fractures were the most common etiologies and sites, respectively. High fall, spinal fracture, and craniofacial fracture were risk factors for nerve injury. Therefore, we should focus on patients who were caused by high fall and presented with spinal and craniofacial fracture to determine the presence of a nerve injury so that we can provide early, timely diagnosis and targeted treatment to children.
Footnotes
Abbreviations: ASIA = American Spinal Cord Injury Association, ASOIs = associated injuries, CCI = closed craniocerebral injury, CT = computed tomography, MRI = magnetic resonance imaging, OCI = open craniocerebral injury, TBIs = traumatic brain injuries, TFs = traumatic fractures.
HW and HY contributed equally to this work.
WHW and YHL: conceived the study, collected the data, participated in the analysis of samples, drafted the manuscript, and performed the statistical analysis. ZY, LCQ, LJ, and OL: conceived the study and participated in its design, coordination, and drafting. ZYW and SGL: participated in the analysis and interpretation of samples. WHW, HJD, CY, and XLB: participated in the review, revision, coordination, and drafting of the manuscript and performed the analysis with constructive discussions.
Funding: This work was supported by the Foundation of the State Key Laboratory of Robotics (2017-O01), the Foundation of the State Key Laboratory of Materials Processing and Die & Mould Technology (P2018-011), the Open Project Program of the State Key Laboratory of CAD&CG (A1718), the Liaoning Province Doctor Startup Fund (201601389), and the Research Foundation about Clinical Diagnosis and Treatment of Anaemia for Young Physician (LIM-SS-16001).
The authors have no conflicts of interest to disclose.
References
- [1].Pickett W, Streight S, Simpson K, et al. Injuries experienced by infant children: a population-based epidemiological analysis. Pediatrics 2003;111:e365–70. [DOI] [PubMed] [Google Scholar]
- [2].Macgregor DM. Accident and emergency attendances by children under the age of 1 year as a result of injury. Emerg Med J 2003;20:21–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Lehman D, Schonfeld N. Falls from heights: a problem not just in the northeast. Pediatrics 1993;92:121–4. [PubMed] [Google Scholar]
- [4].Benoit R, Watts DD, Dwyer K, et al. Windows 99: a source of suburban pediatric trauma. J Trauma 2000;49:477–81. discussion 481-482. [DOI] [PubMed] [Google Scholar]
- [5].Keogh S, Gray JS, Kirk CJ, et al. Children falling from a height in London. Inj Prev 1996;2:188–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Ong ME, Ooi SB, Manning PG. A review of 2,517 childhood injuries seen in a Singapore emergency department in 1999—mechanisms and injury prevention suggestions. Singapore Med J 2003;44:12–9. [PubMed] [Google Scholar]
- [7].Lallier M, Bouchard S, St-Vil D, et al. Falls from heights among children: a retrospective review. J Pediatr Surg 1999;34:1060–3. [DOI] [PubMed] [Google Scholar]
- [8].Mirdad T. Fractures of the neck of femur in children: an experience at the Aseer Central Hospital, Abha, Saudi Arabia. Injury 2002;33:823–7. [DOI] [PubMed] [Google Scholar]
- [9].Krug EG, Sharma GK, Lozano R. The global burden of injuries. Am J Public Health 2000;90:523–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Bartlett SN. The problem of children's injuries in low-income countries: a review. Health Policy Plan 2002;17:1–3. [DOI] [PubMed] [Google Scholar]
- [11].Vish NL, Powell EC, Wiltsek D, et al. Pediatric window falls: not just a problem for children in high rises. Inj Prev 2005;11:300–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Stone KE, Lanphear BP, Pomerantz WJ, et al. Childhood injuries and deaths due to falls from windows. J Urban Health 2000;77:26–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Mathis RD, Levine SH, Phifer S. An analysis of accidental free falls from a height: the 'spring break’ syndrome. J Trauma 1993;34:123–6. [DOI] [PubMed] [Google Scholar]
- [14].Musemeche CA, Barthel M, Cosentino C, et al. Pediatric falls from heights. J Trauma 1991;31:1347–9. [DOI] [PubMed] [Google Scholar]
- [15].Williams RA. Injuries in infants and small children resulting from witnessed and corroboincidenced free falls. J Trauma 1991;31:1350–2. [DOI] [PubMed] [Google Scholar]
- [16].Kim KA, Wang MY, Griffith PM, et al. Analysis of pediatric head injury from falls. Neurosurg Focus 2000;8:e3. [DOI] [PubMed] [Google Scholar]
- [17].Jones G, Cooley HM. Symptomatic fracture incidence in those under 50 years of age in southern Tasmania. J Paediatr Child Health 2002;38:278–83. [DOI] [PubMed] [Google Scholar]
- [18].Mattila V, Parkkari J, Kannus P, et al. Occurrence and risk factors of unintentional injuries among 12- to 18-year-old Finns–a survey of 8219 adolescents. Eur J Epidemiol 2004;19:437–44. [DOI] [PubMed] [Google Scholar]
- [19].Hagino H, Yamamoto K, Ohshiro H, et al. Increasing incidence of distal radius fractures in Japanese children and adolescents. J Orthop Sci 2000;5:356–60. [DOI] [PubMed] [Google Scholar]
- [20].Khosla S, Melton LJ, 3rd, Dekutoski MB, et al. Incidence of childhood distal forearm fractures over 30 years: a population-based study. JAMA 2003;290:1479–85. [DOI] [PubMed] [Google Scholar]
- [21].Hedström EM, Svensson O, Bergström U, et al. Epidemiology of fractures in children and adolescents. Acta Orthop 2010;81:148–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Jerrhag D, Englund M, Petersson I, et al. Increasing wrist fracture rates in children may have major implications for future adult fracture burden. Acta Orthop 2016;87:296–300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Pressley JC, Barlow B. Child and adolescent injury as a result of falls from buildings and structures. Inj Prev 2005;11:267–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Cooper C, Dennison EM, Leufkens HG, et al. Epidemiology of childhood fractures in Britain: a study using the general practice research database. J Bone Miner Res 2004;19:1976–81. [DOI] [PubMed] [Google Scholar]
- [25].Durkin MS1, Laraque D, Lubman I, et al. Epidemiology and prevention of traffic injuries to urban children and adolescents. Pediatrics 1999;103:e74. [DOI] [PubMed] [Google Scholar]
- [26].Istre GR, McCoy MA, Stowe M, et al. Childhood injuries due to falls from apartment balconies and windows. Inj Prev 2003;9:349–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Harris VA, Rochette LM, Smith GA. Pediatric injuries attributable to falls from windows in the United States in 1990–2008. Pediatrics 2011;128:455–62. [DOI] [PubMed] [Google Scholar]
- [28].Mäyränpää MK, Mäkitie O, Kallio PE. Decreasing incidence and changing pattern of childhood fractures: a population-based study. J Bone Miner Res 2010;25:2752–9. [DOI] [PubMed] [Google Scholar]
- [29].Howard A, Rothman L, McKeag AM, et al. Children in side-impact motor vehicle crashes: seating positions and injury mechanisms. J Trauma 2004;56:1276–85. [DOI] [PubMed] [Google Scholar]
- [30].Li LP, Wang S, Huang G, et al. A survey on injury incidence in school children in Shantou City, China. Biomed Environ Sci 2003;16:180–6. [PubMed] [Google Scholar]