

Abstract
A 60-year-old woman under treatment with letrozole for metastatic breast cancer underwent 18F-FDG PET-CT for restaging. A new widespread intense splenic FDG uptake without nodular lesions and multiple FDG-avid mediastinal and abdominal nodes were observed. Based on these findings, a nodal and transbronchial lung biopsy was performed. Histological results were compatible with sarcoidosis. The patient began steroid treatment and 6 weeks after a PET-CT showed normalisation of both splenic and nodal uptake. In our case, 18F-FDG PET-CT has been useful in detecting a rare case of splenic sarcoidosis without typical nodular lesions on CT images, impacting the patient’s treatment and prognosis.
Keywords: 18F-FDG, positron emission tomography, spleen sarcoidosis, breast cancer
Introduction
Sarcoidosis is a benign systemic granulomatous disorder of unknown aetiology. The condition usually involves the lungs and mediastinal or hilar nodes [1]. One of the most frequent extra-thoracic manifestations is peripheral lymph node involvement, found in 8–15% of patients [2–4].
Blank et al. reported breast and cervical cancer and B-cell lymphoma as the most common malignancies in patients with sarcoidosis [1].
A retrospective report of 12 cases and a literature review showed that sarcoidosis frequently affects patients with breast cancer (32.3%) and must be considered in the differential diagnosis of the disease [5].
Case report
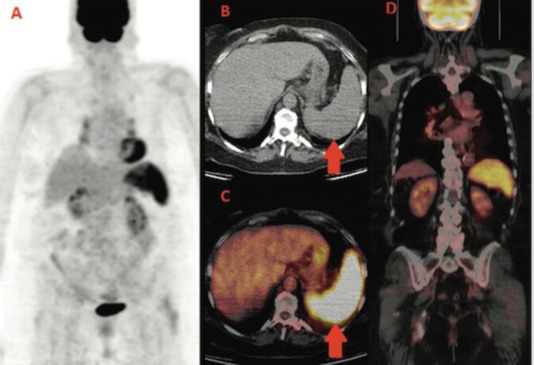
We report the case of a 60-year-old woman diagnosed with left breast cancer in 2006. The histology showed an oestrogen (ER) and progesteron (PgR) receptor positive, HER2 negative, invasive lobular carcinoma, with some palpable left axillary nodes. The staging CT scan showed multiple mediastinal and abdominal lymph nodes. The patient was asymptomatic. Considering her breast cancer as metastatic, she received surgery on the primary tumour and axillary nodes but no radiation treatment and started palliative letrozole. The breast cancer’s stage was established as pT1c N3 M1. She was followed with clinical, biochemical evaluations and an annual CT scan that always showed stable disease. In the late 2013, for the first time, a 18F-FDG PET-CT was performed for disease status assessment. Images were acquired one hour after intravenous injection of 240 MBq (6.5 mCi) of 18F-FDG according to the body mass index. Maximum-intensity projection PET image (A), axial CT (B), and fused PET/CT images (C,D) (Figure 1) showed intense and diffuse tracer uptake in the spleen (red arrow), which had an homogeneous parenchymal structure without focal nodular lesions and, in mediastinal field, multiple FDG avid bilateral hilar lymph nodes characterised by greater lymph node enlargement on the right side.
Figure 1. First F-FDG performed; intense and diffuse tracer uptake in the spleen and hilar lymph nodes.
Based on the 18F-FDG PET-CT findings, a transbronchial lung and lymph node biopsy were performed. Histological features were compatible with sarcoidosis showing noncaseating granuloma between the mucinous bronchial glands (A) and submucosal granuloma consisting of a nodular cluster of epithelioid and giant cells (B) (Figure 2).
Figure 2. Histological features showing non-caseating granuloma between the mucinous bronchial glands (A) and submucosal granuloma consisting of a nodular cluster of epithelioid and giant cells (B).

A control PET-CT performed after 6 weeks of prednisone showed a rapid decrease of FDG uptake in both nodes and spleen (images E,F,G,H) (Figure 3).
Figure 3. PET-CT after treatment that shows a rapid decrease of FDG uptake.

During all this time period, the patient had never been symptomatic for any respiratory or abdominal complaints.
Re-evaluating the clinical history of this patient, we concluded breast cancer was not metastatic at diagnosis and she could have received a curative multidisciplinary treatment upfront.
Discussion
Examples of sarcoidosis or sarcoid-like reactions associated with malignancy have already been reported in the literature, in many cases as bilateral mediastinal lymph node involvement and sometimes as organ infiltration characterised by typical granulomas and/or nodular lesions [6–9]. The frequency of sarcoidosis in cancer patients is 4.4% higher than in the general population [10]. Cases of sarcoidosis mimicking metastatic breast cancer have already been described [11, 12]. There are several possible chronological associations between breast cancer and sarcoidosis. As previously reported, the two diseases may develop in tandem, or breast cancer may induce a sarcoidosis-like granulomatous response [13, 14].
The frequency of splenic involvement in sarcoidosis has been reported to be 10–50%, depending on whether it is detected on physical examination (5–14%), by a radiological test (33–53%), or a tissue biopsy (24–59%) [15].
A previous case report described a spleen sarcoidosis highlighted by 18F-FDG PET-CT and associated with 1,25-dihydroxyvitamin D [1,25(OH)2D]-mediated hypercalcemia [16]. In our case, 18F-FDG PET-CT has been crucial in detecting a spleen sarcoidosis without classical focal nodular lesions, therefore previously misdiagnosed as advanced breast cancer. The splenic and lymph node complete response after steroids has allowed a quick disease down staging. The patient was considered disease-free and PET-positive lymph nodes as false positive. This case underlines that the hybrid imaging can discover sarcoidosis and sarcoid-like reactions before and more specifically than conventional imaging [17]. The functional impairment highlighted by PET-CT may anticipate morphological alterations and therefore provide useful information for correct staging and early and appropriate therapeutic decisions. On the other hand, sarcoidosis is one of the known pitfalls in PET imaging, frequently causing false-positive results; expertise and knowledge are therefore key for a correct imaging interpretation.
Conclusions
This clinical case emphasises the clinical utility of always performing biopsies of suspicious lesions, as reaffirmed by the third ESO-ESMO international consensus for advanced breast cancer [18] and shows that PET-CT can help in detecting unusual parenchymal sarcoidosis localisations.
References
- 1.Blank N, Lorenz HM, Ho AD, et al. Sarcoidosis and the occurrence of malignant diseases. Rheumatol Int. 2014;34:1433–1439. doi: 10.1007/s00296-014-2983-5. [DOI] [PubMed] [Google Scholar]
- 2.Baughman RP, Teirstein AS, Judson MA, et al. on behalf of Case Control Etiologic Study of Sarcoidosis (ACCESS) research group Clinical characteristics of patients in a case control study of sarcoidosis. Am J Respir Crit Care Med. 2001;164:1885–1889. doi: 10.1164/ajrccm.164.10.2104046. [DOI] [PubMed] [Google Scholar]
- 3.Rizzato G. Extrapulmonary presentation of sarcoidosis. Curr Opin Pulm Med. 2001;7:295–297. doi: 10.1097/00063198-200109000-00008. [DOI] [PubMed] [Google Scholar]
- 4.Rizzato G, Palmieri G, Agrati AM, et al. The organ-specific extrapulmonary presentation of sarcoidosis: a frequent occurrence but a challenge to an early diagnosis A 3-year-long prospective observational study. Sarcoidosis Vasc Diffuse Lung Dis. 2004;21:119–126. [PubMed] [Google Scholar]
- 5.Grados A, Ebbo M, Bernit E, et al. Medicine. Vol. 94. Baltimore: 2015. Sarcoidosis occurring after solid cancer: a nonfortuitous association: report of 12 cases and review of the literature; p. e928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hunt BM, Vallières E, Buduhan G, et al. Sarcoidosis as a benign cause of lymphadenopathy in cancer patients. Am J Surg. 2009;197(5):629–32. doi: 10.1016/j.amjsurg.2009.01.004. [DOI] [PubMed] [Google Scholar]
- 7.DeFilippis EM, Arleo EK. New diagnosis of sarcoidosis during treatment for breast cancer, with radiologic-pathologic correlation. Clin Imaging. 2013;37(4):762–6. doi: 10.1016/j.clinimag.2012.10.002. [DOI] [PubMed] [Google Scholar]
- 8.Butt S, Alzebdeh R, Kable TD, et al. Non-caseating granulomas in patients after the diagnosis of cancer: clinical characteristics and outcome. Sarcoidosis Vasc Diffuse Lung Dis. 2011;28(1):44–9. [PubMed] [Google Scholar]
- 9.Ito T, Okada T, Murayama K, et al. Two cases of sarcoidosis discovered accidentally by positron emission tomography in patients with breast cancer. Breast J. 2010;16(5):561–3. doi: 10.1111/j.1524-4741.2010.00961.x. [DOI] [PubMed] [Google Scholar]
- 10.Smith IC, Ogston KN, Whitford P, et al. Staging of the axilla in breast cancer: accurate in vivo assessment using positron emission tomography with 2-(fluorine-18)-fluoro-2-deoxy-D-glucose. Ann Surg. 1998;228(2):220–7. doi: 10.1097/00000658-199808000-00012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Zivin S1, David O, Lu Y. Sarcoidosis mimicking metastatic breast cancer on FDG PET/CT. Intern Med. 2014;53(21):2555–6. doi: 10.2169/internalmedicine.53.3333. [DOI] [PubMed] [Google Scholar]
- 12.Tolaney SM1, Colson YL, Gill RR, et al. Sarcoidosis mimicking metastatic breast cancer. Clin Breast Cancer. 2007;7(10):804–10. doi: 10.3816/CBC.2007.n.044. [DOI] [PubMed] [Google Scholar]
- 13.Martella S1, Lohsiriwat V, Barbalho DM, et al. Sarcoid-like reaction in breast cancer: a long-term follow-up series of eight patients. Surg Today. 2012;42(3):259–63. doi: 10.1007/s00595-011-0084-6. [DOI] [PubMed] [Google Scholar]
- 14.Ojeda H, Sardi A, Totoonchie A. Sarcoidosis of the breast: implications for the general surgeon. Am Surg. 2000;66:1144–1148. [PubMed] [Google Scholar]
- 15.Judson MA. Extrapulmonary sarcoidosis. Semin Respir Crit Care Med. 2007;28(1):83–101. doi: 10.1055/s-2007-970335. [DOI] [PubMed] [Google Scholar]
- 16.Dennis BA, Jajosky RP, Harper RJ. Splenic sarcoidosis without focal nodularity: a case of 1,25-dihydroxyvitamin D-mediated hypercalcemia localized with FDG PET/CT. Endocr Pract. 2014;20(2):28–33. doi: 10.4158/EP13240.CR. [DOI] [PubMed] [Google Scholar]
- 17.Kurata A, Takayama N, Terado Y, et al. Sarcoidal granulomas in the spleen associated with multiple carcinomas. Sarcoidosis Vasc Diffuse Lung Dis. 2010;27(2):153–159. [PubMed] [Google Scholar]
- 18.Cardoso F, Costa E, Senkus E, et al. 3rd ESO-ESMO International Consensus Guidelines for Advanced Breast Cancer (ABC 3) Ann Oncol. 2017;28(1):16–33. doi: 10.1093/annonc/mdx036. [DOI] [PMC free article] [PubMed] [Google Scholar]