

Abstract
Background:
Cancer is one of the leading causes of death throughout the world. Analyzing the incidence of cancer by site, sex and age is essential to detect the burden of cancer. Throughout the twelve hospital based cancer registries of Nepal, a total of 29,802 cancer cases with known age, were registered from January 1st 2010 to 2013 December 31st. The purpose of this retrospective study is to present the incidence of all cancer sites in both males and females for this period.
Materials and Methods:
This paper reviews data from all the hospital based cancer registries over a four-year period. This retrospective study has illustrated the number of cases, frequencies and crude incidence of all cancers by sex and site. For statistical analysis, SPSS (version 23.0) and Microsoft Excel 2010 were used.
Results:
Over the four-year period from January 1st 2010 to 2013 December 31st the major cancer in males was identified as follows: lung cancer (17.5%) followed by stomach cancer (7.6 %) and larynx cancer (5.4%). Among females, for the same four-year period, the three common cancers were identified as cervix (18.9 %) followed by breast (15.6 %) and lung (10.2%).
Conclusion:
This retrospective study concluded that cancer is being increased by calendar years both in males and females however, the incidence of cancer is higher in females compared to males. .
Keywords: Cancer , male and female , site , incidence , Nepal.
Introduction
Population based cancer registry is currently unavailable in Nepal although there are twelve hospital based cancer registries (B P Koirala Memorial Cancer hospital, Bhaktapur Cancer Hospital, Bir hospital, TU Teaching Hospital, Kanti Children Hospital, BP Koirala Institute of Health Science and Manipal Teaching Hospital, Shree Birendra Hospital, Civil Service Hospital, Patan Hospital, Paropakar Maternity and Women Hospital and Nepalgunj Teaching Hospital) operating throughout this country [ 1 ]. The first hospital-based cancer registry was established in 2003 with the aid of the World Health Organization. Documents were previously issued which highlighted the problem of cancer cases in Nepal [ 2, 3, 4, 5 ], however, owing to the lack of community based cancer registries, we have taken the population (denominator) from the census and cases from the hospital. This study primarily relies on the analysis of data from all the cancer registries in Nepal between 2010-2013 inclusive. In so doing, it has demonstrated the reality that hospital based study remains incomplete due to a lack of data because many people either remain incapable to visit hospitals or they are unaware of cancer. For any meaningful progress especially the reduction of cancers generally, it is imperative to secure the establishment of population based cancer registry in Nepal. The output of this study suggests there is an urgent necessity for cancer epidemiologists, statisticians as well as concerned stakeholders to invest in a preventative program to control and thereby prevent the increasing trend of cancers in Nepal.
Methodology
Data of cancer cases was collected from all the hospital based cancer registries of Nepal between 1st January 2010 to 31st December 2013. All double/multiple entry cases were excluded by cross checking each patients name, sex, address and hospital registered number. We analyzed 13789 male cases and 16013 female cases which have known age. The collected data was entered in Excel Sheet with respect to age, sex, years and site. The population growth rate from 2001 to 2011 published in population monograph of Nepal volume 1 and the Census population of 2011 was used to estimate the 2010, 2012 and 2013 population of Nepal [ 6 ]. Cancer cases were categorized as per International Classification of Disease for Oncology (ICD-10) published by the International Agency for Research on Cancer/ World Health Organization (IARC/WHO). The crude incidence rate of cancer (per 100,000) in males and females of all sites are calculated. For statistical analysis, SPSS (version 23.0) and Microsoft Excel 2010 were used.
Results
Lung cancer has the highest incidence (4.6) in males followed by stomach cancer (2.0) and larynx cancer (1.4) per 100,000 population from 2010 to 2013. Similarly, cervical cancer has the highest incidence (5.5) per 100,000 population in females followed by breast cancer (4.6) and lung cancer (3.0) over the same four-year period. The crude incidence of female cancer cases (29.2) per 100,000 population is higher than the crude incidence of male cancer cases (26.5) (Table 2).
Table 2.
Table 2. Distribution of cancer site in males and females in Nepal from 2010 to 2013.
| Male | Female | ||||||
| (Per 100,000) | (Per 100,000) | Site | |||||
| ICD-10 | cases | Fre (%) | Crude rate | cases | Fre (%) | Crude rate | |
| C00 | 70 | 0,5 | 0,1 | 24 | 0,1 | 0,0 | Lip |
| C01 | 26 | 0,2 | 0,1 | 6 | 0,0 | 0,0 | Base of Tongue |
| C02 | 348 | 2,5 | 0,7 | 184 | 1,1 | 0,3 | Other and unspecified parts of tongue |
| C03 | 75 | 0,5 | 0,1 | 29 | 0,2 | 0,1 | Gum |
| C04 | 60 | 0,4 | 0,1 | 16 | 0,1 | 0,0 | Floor of mouth |
| C05 | 57 | 0,4 | 0,1 | 38 | 0,2 | 0,1 | Palate |
| C06 | 472 | 3,4 | 0,9 | 161 | 1,0 | 0,3 | Other and unspecified parts of mouth |
| C07 | 92 | 0,7 | 0,2 | 53 | 0,3 | 0,1 | Parotid gland |
| C08 | 60 | 0,4 | 0,1 | 48 | 0,3 | 0,1 | Other and unspecified major salivary gland |
| C09 | 93 | 0,7 | 0,2 | 36 | 0,2 | 0,1 | Tonsil |
| C10 | 90 | 0,7 | 0,2 | 34 | 0,2 | 0,1 | Oropharynx |
| C11 | 173 | 1,3 | 0,3 | 93 | 0,6 | 0,2 | Nasopharynx |
| C12 | 259 | 1,9 | 0,5 | 39 | 0,2 | 0,1 | Pyriform sinus |
| C13 | 44 | 0,3 | 0,1 | 11 | 0,1 | 0,0 | Hypopharynx |
| C14 | 54 | 0,4 | 0,1 | 16 | 0,1 | 0,0 | Other and ill-defined sites in lip oral cavity and mouth |
| C15 | 362 | 2,6 | 0,7 | 233 | 1,5 | 0,4 | Esophagus |
| C16 | 1047 | 7,6 | 2 | 640 | 4,0 | 1,2 | Stomach |
| C17 | 53 | 0,4 | 0,1 | 44 | 0,3 | 0,1 | Small intestine |
| C18 | 347 | 2,5 | 0,7 | 277 | 1,7 | 0,5 | Colon |
| C19 | 21 | 0,2 | 0 | 13 | 0,1 | 0,0 | Rectosegmoidjucnction |
| C20 | 396 | 2,9 | 0,8 | 338 | 2,1 | 0,6 | Rectum |
| C21 | 40 | 0,3 | 0,1 | 27 | 0,2 | 0,0 | Anus and anal canal |
| C22 | 367 | 2,7 | 0,7 | 283 | 1,8 | 0,5 | Liver |
| C23 | 292 | 2,1 | 0,6 | 577 | 3,6 | 1,1 | Gall bladder |
| C24 | 66 | 0,5 | 0,1 | 73 | 0,5 | 0,1 | Other and unspecified billary tract |
| C25 | 158 | 1,1 | 0,3 | 129 | 0,8 | 0,2 | Pancreas |
| C26 | 15 | 0,1 | 0 | 6 | 0,0 | 0,0 | Ill defined digestive organs |
| C30 | 85 | 0,6 | 0,2 | 75 | 0,5 | 0,1 | Nasal cavity and middle ear |
| C31 | 74 | 0,5 | 0,1 | 73 | 0,5 | 0,1 | Accessory sinus |
| C32 | 741 | 5,4 | 1,4 | 243 | 1,5 | 0,4 | Larynx |
| C33 | 5 | 0 | 0 | 1 | 0,0 | 0,0 | Trachea |
| C34 | 2414 | 17,5 | 4,6 | 1634 | 10,2 | 3,0 | Bronchus and lung |
| C37 | 29 | 0,2 | 0,1 | 12 | 0,1 | 0,0 | Thymus |
| C38 | 34 | 0,2 | 0,1 | 20 | 0,1 | 0,0 | Heart, mediastinum and pleura |
| C39 | 2 | 0 | 0 | 2 | 0,0 | 0,0 | Ill defined respiratory system |
| C40 | 167 | 1,2 | 0,3 | 107 | 0,7 | 0,2 | Bones joint and articular cartilage |
| C41 | 173 | 1,3 | 0,3 | 133 | 0,8 | 0,2 | Other and unspecified bones joints and articular cartilage |
| C42 | 0 | 0 | 0 | 2 | 0,0 | 0,0 | Spleen |
| C43 | 94 | 0,7 | 0,2 | 71 | 0,4 | 0,1 | Skin melanoma |
| C44 | 113 | 0,8 | 0,2 | 107 | 0,7 | 0,2 | Skin other |
| C47 | 7 | 0,1 | 0 | 13 | 0,1 | 0,0 | Perepheral nerves and autonomic nervous system |
| C48 | 36 | 0,3 | 0,1 | 21 | 0,1 | 0,0 | Peritoneum and retroperitoneum |
| C49 | 241 | 1,7 | 0,5 | 188 | 1,2 | 0,3 | Connective subcutaneous and other soft tissue |
| C50 | 71 | 0,5 | 0,1 | 2505 | 15,6 | 4,6 | Breast |
| C51 | 0 | 0 | 0 | 107 | 0,7 | 0,2 | Vulva |
| C52 | 0 | 0 | 0 | 98 | 0,6 | 0,2 | Vagina |
| C53 | 0 | 0 | 0 | 3033 | 18,9 | 5,5 | Cervix uteri |
| C54 | 0 | 0 | 0 | 214 | 1,3 | 0,4 | Endometrium |
| C55 | 0 | 0 | 0 | 46 | 0,3 | 0,1 | Uterus |
| C56 | 0 | 0 | 0 | 1035 | 6,5 | 1,9 | Ovary |
| C57 | 0 | 0 | 0 | 118 | 0,7 | 0,2 | Other and unspecified female genital organs |
| C58 | 0 | 0 | 0 | 1 | 0,0 | 0,0 | Placenta |
| C60 | 230 | 1,7 | 0,4 | 0 | 0,0 | 0,0 | Penis |
| C61 | 248 | 1,8 | 0,5 | 0 | 0,0 | 0,0 | Prostate gland |
| C62 | 89 | 0,6 | 0,2 | 0 | 0,0 | 0,0 | Testis |
| C63 | 48 | 0,3 | 0,1 | 0 | 0,0 | 0,0 | Other and unspecified male genital organs |
| C64 | 182 | 1,3 | 0,4 | 113 | 0,7 | 0,2 | Kidney |
| C65 | 2 | 0 | 0 | 2 | 0,0 | 0,0 | Renal Pelvis |
| C66 | 2 | 0 | 0 | 0 | 0,0 | 0,0 | Ureter |
| C67 | 657 | 4,8 | 1,3 | 227 | 1,4 | 0,4 | Bladder |
| C68 | 12 | 0,1 | 0 | 10 | 0,1 | 0,0 | Other unspecified urinary organs |
| C69 | 93 | 0,7 | 0,2 | 100 | 0,6 | 0,2 | Eye and adexa |
| C70 | 24 | 0,2 | 0 | 39 | 0,2 | 0,1 | Meninges |
| C71 | 390 | 2,8 | 0,8 | 283 | 1,8 | 0,5 | Brain |
| C72 | 21 | 0,2 | 0 | 15 | 0,1 | 0,0 | Spinal cord and other parts of CNS |
| C73 | 154 | 1,1 | 0,3 | 487 | 3,0 | 0,9 | Thyroid |
| C74 | 6 | 0 | 0 | 5 | 0,0 | 0,0 | Adrenal gland |
| C75 | 13 | 0,1 | 0 | 10 | 0,1 | 0,0 | Other endocrine and related |
| C76 | 376 | 2,7 | 0,7 | 296 | 1,8 | 0,5 | Other and ill-defined sites |
| C77 | 61 | 0,4 | 0,1 | 38 | 0,2 | 0,1 | Lymph nodes |
| C80 | 227 | 1,6 | 0,4 | 189 | 1,2 | 0,3 | Unknown Primary site |
| C81 | 187 | 1,4 | 0,4 | 81 | 0,5 | 0,1 | Hodgkin's disease |
| C83 | 9 | 0,1 | 0 | 9 | 0,1 | 0,0 | Diffuse non hodgkin lymphoma |
| C85 | 470 | 3,4 | 0,9 | 276 | 1,7 | 0,5 | Non hodgkin lymphoma |
| C90 | 98 | 0,7 | 0,2 | 76 | 0,5 | 0,1 | Multiple myeloma |
| C91 | 323 | 2,3 | 0,6 | 172 | 1,1 | 0,3 | Leukemia/lymphoid |
| C92 | 350 | 2,5 | 0,7 | 237 | 1,5 | 0,4 | Leukemia/myeloid |
| C94 | 0 | 0 | 0 | 0 | 0,0 | 0,0 | Other leukemia |
| C95 | 94 | 0,7 | 0,2 | 61 | 0,4 | 0,1 | Leukemia unspecified |
| TOTAL | 13789 | 100 | 26,5 | 16013 | 100,0 | 29,2 | |
Cancer both in males and females is increasing by calendar years(Table 1) The incidence of three major cancers in males and females over the four-year period has been demonstrated in figure 1 and figure 2 respectively
Table 1.
Table 1. Summary of cancer cases and incidence per 1, 00,000 people in Nepal from 2010 to 2013.
| Years | Total male cases | Total Female cases | Male crude incidence per 100,000 | Female crude incidence per 100,000 |
| 2010 | 3192 | 3581 | 24.8 | 27.8 |
| 2011 | 3295 | 3793 | 26.6 | 27.5 |
| 2012 | 3291 | 3921 | 25.2 | 28 |
| 2013 | 4011 | 4718 | 30.4 | 33.3 |
Figure 1.
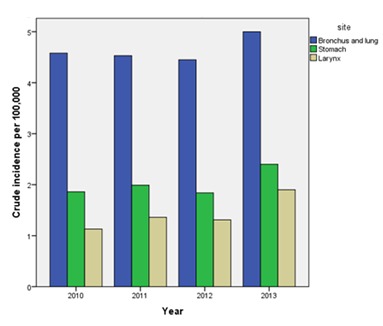
Figure 1: Crude incidence of three major cancers in males from 2010 to 2013.
Figure 2.
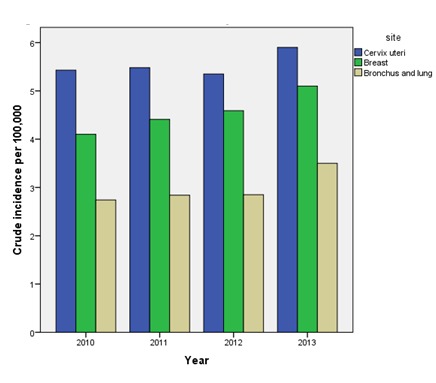
Figure 2: Crude incidence of three major cancers in females from 2010 to 2013
Discussion:
This study was undertaken in Nepal between 2010-2013 and presents the detail of cancer incidence by gender, sites and calendar years. Trends show that the cancer incidence is increasing every year especially for females. This is possibly due to increasing activities of screening programs in different areas of the country [ 7 ] and the support from the International Agency for Research on Cancer (IARC) for early detection and prevention of cervix and breast cancer [ 8 ]. Due to an increasing number of cancer diagnostic centers in Nepal, many people now also come forward to report the cancer cases which could be another possible cause for the growth of new cases of cancer in Nepal [ 9 ].
As a result of our studies we have found that bronchus and lung cancer is the most common cancer in males and the third common cancer in females. The crude incidence rate of lung cancer is 4.6 per 100,000 populations in Nepal while it was 4.45 in 2012 [ 5 ]. The following mitigating factors may have an effect on this trend: lower education, unmarried individuals and Rai/Limbu/Magar ethnicity [ 10 ], household air pollution and tobacco consumption [ 11, 12 ], and not enough medical health education [ 13 ]. For young people in western Nepal; smoking was a serious issue [ 14 ] and the risk factor leading to lung cancer [ 15 ]. The crude incidence rate of lung cancer is 3.0 per 100,000 populations in Nepal while it was 2.85 in previous years [ 5 ].
Cervical uteri cancer is the most common type of cancer in females. The crude incidence rate of cervical uteri is 5.5 per 100,000 population in Nepal while it was 5.35 in 2012 [ 5 ]. Women do not have enough information regarding the human papillomavirus (HPV), cervical cancer and HPV vaccine [ 16 ], or concept of pap smear test [ 17 ]. Using the HPV16/18 vaccines, almost 80% of cervical cancer in Nepal could be prevented [ 18 ].
Breast cancer is the second most common cancer in females with more than a quarter occurring in young females. The more aggressive biological features of tumors were found in this at-risk group therefore we conclude that breast cancer prevention programs are essential to reduce this trend [ 19 ]. The crude incidence rate of breast cancer is (4.6) per 100,000 populations in Nepal while it was 4.59 in 2012 [ 5 ].
Ovarian cancer is the fourth most common cancer in females over this four-year period. The incidence of ovarian cancer is (1.9) per 100,000 populations while it was (1.70) in 2012 ( [ 5 ].
Stomach cancer is the second most common cancer in males while it is the fifth common cancer in females for the same period. The crude incidence rate of stomach cancer in males is (2.0) per 100,000 populations in Nepal, while it was 1.84 in 2012 [ 5 ].
Analyzing the data from B P Koirala Memorial Cancer Hospital, out of 7212 (7.3%) presented as stomach cancer [ 3 ]. Similarly, another study in 2005 reported out of 4397 cases (7.5%) represented male stomach cancer rates while the corresponding percentage of females was (4.1%) [ 2 ]. In female, the incidence of stomach cancer was 1.2 per 100,000 population over the four year period while it was 1.06 in 2012 [ 5 ]. Stomach cancer incidence rated men almost two times higher as compared to women although there is a worldwide variation in trend [ 15 ].
Larynx cancer was the third most common cancer in males over the four-year period 2010 - 2013. The crude incidence rate of larynx cancer is (1.4) per 100,000 populations, while it was 1.0 in 2012 [ 5 ]. Out of 7212 cases in 2012 (5.2%) were the larynx cases [ 3 ]. Similarly, another study in 2005 reported out of 4397 cases, 3.7% presented as larynx cancer in males while the corresponding percentage in females was 1.3% cases [ 2 ].
Ovarian cancer (1.9 per 100,000 populations) is the fourth most common cancer in females while gall bladder (1.1 per 100,000 population) represents the fifth most common cancer in Nepal throughout the four-year period 2010 - 2013. Bladder cancer (1.3 per 100,000 population) is the fourth most common cancer in males while cancer of other and unspecified parts of mouth is the fifth most common cancer in Nepal for the same period.
In conclusion cancer incidence in Nepal is growing at a higher rate for both males and females. The most common cancers in males are bronchus and lung, stomach and larynx while in females cervical uteri, breast, bronchus and lung are the most common cancers.
What is already known on this topic:
A couple of studies had been conducted to demonstrate the incidence of cancer in Nepal which had only focused the single calendar year.
What this study adds:
This study is different from the previous studies in Nepal because it has clearly presented the cancer incidence of all sites over the recent four years. Furthermore, this study also performed the incidence of three major cancers in males and females from 2010 to 2013.
Acknowledgments
The author would like to thank Dr Søren Nymand Lophaven , Sakrish Poudel, Dr Bal Ram Dhakal (University of Cambridge, UK), Shirish Poudel, Dr David Hurman. (Consultant of Aberdeen Royal Infirmary Hospital, Scotland ), Ramesh Kanta Poudel, Nirmal Duwadi (Lecture at Nepal Medical College), Ex Bhuminanda Poudel, Tulashi Devi Poudel, Shanta Poudel Tiwari, Sharan Hari Tiwari, Dev Kumar Basel, Dr Bishwa Ram Poudel ( Consultant BPKMCH), Dr Nirmal Lamichhane ( Consultant Chitwan Medical College), Divya Basel, Shikcha Sharma, Dr Bishnu Kandel, Keshav Dhungana, Dr Dong Pang, Jaya Tamang, Pratap Gurung, Suresh Adhikari, Shalik Ram Acharya, Krishna Hari Bhushal, Krishna Prasad Sapkota, Ravi lal Kharel, Bal Krishna Pandey,Rakcha Acharya, Sabita Sharma, Sadikcha Sharma, Ambika Poudel, Aayush Poudel, Bishnu Adhikari, Sumana Sharma, Bhawani Poudel, Resham Lal Sharma, Sharda Poudel, Babu Ram Khanal, Ravi Lal Kharel, Saroj Acharya, Dr Sunil Shah, Dr Ramesh Bhandari, Dr Ganga Sapkota, Dr Bijaya Chandra Acharya and Dr Ak Narayan Poudel for their contribution towards this research.
References
- 1. National Cancer Registry Programme Report of Hospital Based National Cancer Registry. B.P. Koirala Memorial Cancer Hospital cancer prevention, control and research department. 2013; : 1 - 91. [Google Scholar]
- 2. Pradhananga KK, Baral M, Shresta BM. Multi-institution Hospital-based Cancer Incidence Data for Nepal - An Initial Report. Asian Pac J Cancer Prev. 2009. ; 10 : 259 - 62. PMid: [PubMed] [Google Scholar]
- 3. Pun CB, Pradhananga KK, Siwakoti B, et al. Malignant Neoplasm Burden in Nepal- Data from the seven major cancer service hospitals for 2012. Asian Pac J Cancer Prev. 2015. ; 16 (18): 8659 - 63. https://doi.org/10.7314/APJCP.2015.16.18.8659 PMid: [DOI] [PubMed] [Google Scholar]
- 4. Poudel KK, Huang Z, Neupane PR. Trend of cancer incidence in Nepal from 2003 to 2012. Asian Pac J Cancer Prev. 2016. ; 17 (4): 2171 - 75. https://doi.org/10.7314/APJCP.2016.17.4.2171 PMid: [DOI] [PubMed] [Google Scholar]
- 5. Poudel KK, Huang Z, Neupane PR. Age specific incidence of five major cancers in Nepal. Nepal Journal of Epidemiology. 2016. ; 6 (2): 565 - 73. https://doi.org/10.3126/nje.v6i2.15163 PMid: PMCid: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Population Monograph of Nepal. Population Dynamics, Government of Nepal, National Planning Commission Secretariat, Central Bureau of Statistics. 2014;; I. [Google Scholar]
- 7.Report of NNCTR. [Cited 2017 January 10]. Available on: https://www.globalgiving.org/pfil/6686/ projdoc.pdf.
- 8. Sankaranarayanan R, Sauvaget C, Ramada K.et al. Clinical trials of cancer screening in the developing world and their impact on cancer healthcare. Ann Oncol . 2011. ; 22 : 21 - 8. https://doi.org/10.1093/annonc/mdr422 PMid: [DOI] [PubMed] [Google Scholar]
- 9. Annual Report B.P. Koirala Memorial Cancer Hospital. 2015; 1 - 88. [Google Scholar]
- 10. Hashibe M, Siwakoti B, Wei M. Socioeconomic status and lung cancer risk in Nepal. Asian Pac J Cancer Prev. 2010; 11 : 1083 - 8. [PubMed] [Google Scholar]
- 11. Raspanti GA, Hashibe M, Siwakoti B, et al. Ethnic variation in consumption of traditional tobacco products and lung cancer risk in Nepal. Asian Pac J Cancer Prev. 2015. ; 16 : 5721 - 26. https://doi.org/10.7314/APJCP.2015.16.14.5721 PMid: [DOI] [PubMed] [Google Scholar]
- 12. Raspanti GA, Hashibe M, Siwakoti B, et al. Household air pollution and lung cancer risk among never smokers in Nepal. Environmental Research. 2016. ; 147 : 141 - 45. https://doi.org/10.1016/j.envres.2016.02.008 PMid: [DOI] [PubMed] [Google Scholar]
- 13. Khatiwada P, Kayastha SR, Panta P.et al. Understanding of tobacco and lung cancer among medical students in Kathmandu University School of Medical Sciences (KUSMS). Kathmandu Univ Med J. 2012. ; 10 : 60 - 5. [DOI] [PubMed] [Google Scholar]
- 14. Binu VS, Subba SH, Menezes RG.et al. Smoking among Nepali Youth - Prevalence and Predictors 2010. Asian Pac J Cancer Prev . 2010. ; 11 : 221 - 26. PMid: [PubMed] [Google Scholar]
- 15. Torre LA, Bray F, Siegel RL.et al. Cancer Statistics. Cancer J Clin . 2015. ; 65 : 87 - 108. https://doi.org/10.3322/caac.21262 PMid: [DOI] [PubMed] [Google Scholar]
- 16. Johnson DC, Bhatta MP, Gurung S, et al. Knowledge and awareness of human papillomavirus (HPV), cervical cancer and HPV vaccine among women in two distinct Nepali communities. Asian Pac J Cancer Prev. 2014. ; 15 : 8287 - 93. https://doi.org/10.7314/APJCP.2014.15.19.8287 PMid: [DOI] [PubMed] [Google Scholar]
- 17. Ranabhat S, Tiwari M, Dhungana G, Shrestha R. Association of knowledge, attitude and demographic variables with cervical Pap smear practice in Nepal. Asian Pac J Cancer Prev. 2014. ; 15 : 8905 - 10. https://doi.org/10.7314/APJCP.2014.15.20.8905 PMid: [DOI] [PubMed] [Google Scholar]
- 18. Sherpa ATL, Clifford GM, Vaccarella S.et al. Human papillomavirus infection in women with and without cervical cancer in Nepal. Cancer Causes Control . 2010. ; 21 : 323 - 30. https://doi.org/10.1007/s10552-009-9467-z PMid: [DOI] [PubMed] [Google Scholar]
- 19. Thapa B, Singh Y, Sayami P.et al. Breast cancer in young women from a low risk population in Nepal. Asian Pac J Cancer Prev. 2013. ; 14 : 5095 - 9. https://doi.org/10.7314/APJCP.2013.14.9.5095 PMid: [DOI] [PubMed] [Google Scholar]