

Abstract
In past years, policies and regulations required hospitals to implement advanced capabilities of certified electronic health records (EHRs) in order to receive financial incentives. This has led to accelerated implementation of health information technologies (HIT) in health care settings. However, measures commonly used to evaluate the success of HIT implementation, such as HIT adoption, technology acceptance, and clinical quality, fail to account for complex sociotechnical variability across contexts and the different trajectories within organizations because of different implementation plans and timelines. We propose a new focus, HIT adaptation, to illuminate factors that facilitate or hinder the connection between use of the EHR and improved quality of care as well as to explore the trajectory of changes in the HIT implementation journey as it is impacted by frequent system upgrades and optimizations. Future research should develop instruments to evaluate the progress of HIT adaptation in both its longitudinal design and its focus on adaptation progress rather than on one cross-sectional outcome, allowing for more generalizability and knowledge transfer.
Keywords: health information technology, adaptation, adoption, acceptance
Introduction
Health information technology (HIT) is defined as “the application of information processing involving both computer hardware and software that deals with the storage, retrieval, sharing, and use of health care information, data, and knowledge for communication and decision making” [1]. During the past 10 years in the United States, several policies, such as the Health Information Technology for Economic and Clinical Health Act, have led to accelerated HIT adoption and implementation in health care settings, especially implementation of electronic health record (EHR) systems [2,3]. In addition, the Centers for Medicare and Medicaid Services established the EHR incentive program to promote the development of a robust HIT infrastructure, and as part of that effort, released Meaningful Use (MU) criteria in 2010. These criteria require hospitals to implement advanced capabilities of certified EHRs by certain dates in order to receive financial incentives. Other efforts focused on the creation of regional extension centers to facilitate the transition to EHR use through training. MU criteria consist of 3 stages [4]: stage 1, begun in 2011, has a focus on data capture and sharing; stage 2, begun in 2014, aims to improve clinical processes with health information exchange, ePrescription, and patient access; and stage 3, in 2017, was recently replaced by Advanced Care Information [5,6] due to criticism of the MU program [7,8].
Hospitals have been rapidly responding to these new policies and incentives with large-scale implementations of EHRs during the past few years. Adopting new technology requires the redesign of individual and collective workflows and results in changes in both organizational structure and process [9-13]. Yet rapid adoption may hinder the interoperability of the EHR system [14,15]. To facilitate appropriate adoption and use, upgrades, redesign, and optimization are needed, including both minor and major changes in EHR infrastructures, functions, interfaces, and workflows. Further, recent studies have shown that there is a close relationship between the speed of adoption and patient safety concerns of clinicians, both across facilities and within different units [16-18]. EHR implementation could be a distraction from patient care with negative impact on patient outcomes [19] and has mixed association with quality improvement [20,21].
At the same time, studies suggest that unsuccessful implementation of HIT systems could be due to poorly designed HIT, poor use of HIT by clinicians, or socioorganizational factors such as goal conflicts, lack of time, or lack of support from colleagues [22]. However, these studies lack clarity in their measures [23]. This lack of differentiation between technological and human factors thus limits the ability to apply research findings to practice in technology implementation [24].
Given MU regulations, MU requirements have commonly been used as a means to assess HIT implementation success in order to promote essential HIT functionalities [4]. For example, MU stage 2 requires providers to have certain HIT functionalities (eg, computerized provider order entry, personal health record, medication reconciliation) in order to continue to participate in the EHR incentive programs [25]. However, this approach also creates a ceiling effect, hindering the advancement of innovative utilities. While the MU program may accelerate development and implementation of certain key functions, it also slows down other functionalities [26,27]. By focusing on achieving MU, we risk missing the big picture of health care system changes. Therefore, we propose that there is a need to improve our understanding of how to appropriately assess the performance and success of HIT implementation over time to allow us to generalize to other HIT implementation contexts.
Measuring Health Information Technology Implementation Success
Successful HIT implementation is commonly evaluated using measures such as HIT adoption, technology acceptance, and clinical quality. Yet this disparate array of measures fails to account for complex sociotechnical interactions, variability across contexts, and the different trajectories within organizations that exist because of different implementation plans and timelines. Appropriate measurement of HIT implementation thus needs to take into account this variability across organizations and over time but at the same time enable us to generalize the variation across HIT implementation studies in order to inform practice. As a result, the issue of consistent measurement becomes increasingly significant.
Current measures that exist in the literature include HIT adoption, HIT acceptance, and clinical quality measures (CQMs). The first common measure, HIT adoption, is defined by the EHR MU stages outlined by the Office of the National Coordinator and measures the rate of health care systems having chosen to invest resources toward EHR implementation. It is commonly reported as an adoption rate to reflect the percentage of health care organizations with specific EHR functionalities or capabilities that are meaningful for patient care. In 2013, 59% of hospitals reported at least a basic EHR system, but only 5.1% could meet the MU stage 2 criteria [2]. The expectation is that more meaningful use of an EHR system will ultimately result in improved care and more empowered clinicians. In addition, the Healthcare Information and Management Systems Society (HIMSS) measures EHR adoption through the Electronic Medical Record Adoption Model (EMRAM), which categorizes EHR capabilities into an 8-stage scale from stage 0 to stage 7 [28]. In 2015, HIMSS Analytics’ Annual Study reported that 27% of hospitals are at stage 6 or above. Although it is helpful to recognize the EHR capabilities across organizations in the nation, it is unclear whether those functions are fully used by clinicians.
The second approach to measuring implementation success involves HIT acceptance, the extent of individual commitment to use the technology [29-33]. When assessing individual user acceptance, the technology acceptance model (TAM) [34,35] is a commonly applied and useful model, albeit with limitations [36]. TAM’s predictive power in health care is lower than what has been found in other domains [24], and some recommend that the TAM should be integrated with other adoption theories [36], particularly those that include variables related to both human and social change processes [24].
CQMs [37] are another common metric used to assess the success of HIT [38]. However, HIT implementation appears to have little impact on care quality whether measured by patient mortality, adverse drug events, or readmission rates [39]. Although CQMs are helpful for assessing the extent to which HIT can be used to monitor the quality of health care services provided, this approach to measurement does not take into account organizational or human factors that could impact HIT implementation.
Measuring HIT adoption and acceptance alone provides only a limited understanding of HIT success. Both HIT adoption rates and TAM are helpful to understand the status of HIT implementation and acceptance, but they do not inform a strategic plan for promoting successful HIT implementation in a health care organization. CQM as a proxy for HIT success also fails to take into account the organizational context of implementation. In short, as HIT implementation is a process, not an outcome, understanding implementation success requires consideration of the sociotechnical environment in which it takes place.
Sociotechnical Theory: Improving Our Understanding of Health Information Technology Implementation
Sociotechnical theory positions people-focused (socio) elements, organizational and human, and information technology elements (technical) as interdependent parts of a system that cannot be studied in isolation and therefore must be evaluated together [40]. Sociotechnical theory has been discussed as a theoretical framework that is responsive to the tenets of complex adaptive systems (CAS) [41-44]. When viewed in concert, these 2 theoretical approaches support that interdependent interactions between people and technology within the workplace have both direct impacts, in the classical cause and effect sense, and impacts through feedback, where these same people and technology attenuate, strengthen, distort, halt, or change valence over time [41,43,45].
Current sociotechnical evaluations involve assessing both the technology and the social contexts where the technology is implemented. A systematic review conducted on EHR implementations revealed that sociotechnical factors complicate HIT deployments [46]. Technical features of HIT interact with the social features of a health care work environment. Further, it has been demonstrated that the quality of the implementation process is just as important as the features and capabilities of the system being implemented [47-49].
We suggest grounding the theoretical framing of CAS that refers to adaptiveness as “the ability of components of a CAS to change their behavior as a result of interactions with the other components and the surroundings” [41]. In shifting the concept of adoption to adaptation, we frame sociotechnological change as occurring over time with system response characterized as the adaptiveness of a health care organization in the context of changes to HIT implementation [42,44]. For example, technical features are not static; rather they frequently change over time as new versions of the software are promulgated. As such, adoption is not an end state; it is the application of an arbitrary end point to facilitate our understanding. From that perspective, understanding the adaptiveness, or HIT adaptation in this process, is thus significant in our understanding of HIT implementation success [50].
Health Information Technology Adaptation
Although sociotechnical theory and CAS have been used to explain complexity in health care [51], little has been discussed that uses adaptation as a measure to evaluate the success of HIT implementation over time. We thus propose a new focus: adaptation. Adaptation is conceptualized as “a process of modifying existing conditions in an effort to achieve alignment” [52] involving workflow redesign, user trainings, and technology maintenance [53]. In the context of HIT implementation, refocusing from adoption and acceptance to adaptation illuminates factors that facilitate or hinder the connection between use of the EHR and improved quality of care. Further, by shifting to adaptation, we refocus the question of HIT adoption to one that explores the trajectory of change as an explicit component of the way we measure these issues. Table 1 presents the definitions of adoption, adaptation, and acceptance as differentiated by Cooper and Zmud [53].
Table 1.
Definitions of adoption, adaptation, and acceptance [54].
| Concept | Definition |
| Adoption | A decision is reached to invest resources to accommodate the implementation effort. |
| Adaptation | The innovation is developed, installed, and maintained. Procedures are developed and revised. Members are trained both in the new procedures and in the innovation. |
| Acceptance | Organizational members are induced to commit to the innovation’s usage. |
MU criteria [54-56] and CQMs can be seen as verification and validation steps, respectively, for HIT implementation. In product or system design, evaluation is commonly done via verification and validation. Verification serves as quality control to assess whether a system is in compliance with regulations and specifications. On the other hand, validation is a quality assurance process that establishes evidence to ensure a system accomplishes what was intended. However, no measures have been proposed to assess HIT implementation performance between the steps of system verification and validation. We suggest that this period encompasses the HIT adaptation process, requiring its own measurement approach.
In Figure 1, we illustrate the current knowledge gap between meeting the MU criteria and achieving CQMs, linking this conceptually to Donabedian’s well-known structure-process-outcomes model, a quality assessment model presented to evaluate health services outcomes [57]. Considering HIT implementation in the context of the Donabedian model, structure refers to HIT resources, which are determined by MU criteria; process refers to clinicians’ use or adaptation of HIT for their use; and outcomes refer to the effects of using HIT for the delivery of health care, as measured by CQMs. In practice, the HIT implementation journey will be impacted by frequent system upgrades and optimizations, leading to performance variability throughout the process. However, by including considerations of sociotechnical factors such as technology acceptance, communication and collaboration, work productivity, training and competency, leadership, and policy, the progress of HIT adaptation could be appropriately assessed.
Figure 1.
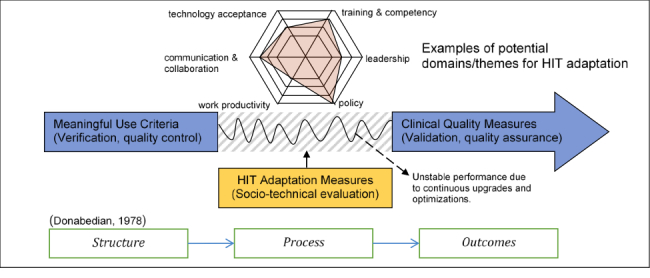
Health information technology adaptation measures as the process evaluation.
Theoretical Frameworks to Study Health Information Technology Adaptation
Two theoretical frameworks provide guidance for HIT adaptation research: the information technology (IT) implementation framework [58] and a new sociotechnical model [42]. First, the IT implementation framework [58] suggests that (1) IT use is complex, multidimensional, and influenced by a variety of factors at individual and organizational levels and (2) success in achieving change is enhanced by active participation of members from the target user group [58]. The new sociotechnical model [42] now aims to study HIT in complex adaptive health care systems and suggests investigating 8 dimensions: (1) hardware and software computing infrastructure; (2) clinical content; (3) human-computer interface; (4) people; (5) workflow and communication; (6) internal organizational policies, procedures, and culture; (7) external rules, regulations, and pressures; and (8) system measurement and monitoring [42]. Figure 2 illustrates our adapted model from the new sociotechnical model [42]. We do not include the seventh dimension, “external rules, regulations, and pressures,” as we focus on factors within the organization.
Figure 2.

Adapted from the sociotechnical model [43].
Recommendations for Future Health Information Technology Adaptation Research
We propose that HIT adaptation research should deploy multilevel and multidimensional evaluation to understand the HIT adaptation progress, drawing from both of these foundational theories. Specifically, HIT adaptation research should focus on developing fundamental and multidimensional facts that can inform the progress of HIT adaptation. Below we describe 4 directions that can drive future HIT adaptation research.
Develop Appropriate Process Measures
While the outcome measures (HIT adoption rate, acceptance, and CQMs) have been established, there is a need to develop process measures from individual and organizational perspectives and include multidimensional measures of adaptation to EHRs. These measures will need to incorporate factors such as communication channels, cultural conflict, interdisciplinary team dynamics, user satisfaction, work productivity, cost, and quality [38,59,60].
Consider the Culture and Context in Which Health Information Technology Is Implemented
Most HIT adoption or acceptance studies have used individuals or hospitals as the unit of analysis [39,61,62]. These findings are informative for identifying associated individual perceptions and experiences as well as hospital demographics. However, additional factors such as the culture of a discipline or a department, the interprofessional or multidisciplinary communication within or across departments, the training received, and workflow at the department level have not been discussed. In particular, while social support has been identified as one of the key factors for acceptance [63,64], no studies have been conducted at the department or unit level to study this factor.
Standardize the Definition and Methods for Sociotechnical Studies
Implementing a new technology into a complex environment is often disruptive, particularly in health care. Sociotechnical evaluations of HIT implementations are supported in both theory and empirically; however, little guidance exists in terms of how to conduct a sociotechnical evaluation [65]. Challenges in conducting sociotechnical evaluations include a lack of agreement on the components of the sociotechnical system, possible study designs, and data analysis strategies which may give light to both practical and conceptual challenges [65].
Study Adaptation Longitudinally and Multidimensionally
Processes are more important to study than outcomes because studying processes allows for generalizability and knowledge transfer beyond the clinical setting where the research was conducted [65]. Future studies need to employ longitudinal study designs with multiple data time periods to establish causal relationships [32,66,67]. In addition, the HIT evaluation toolkit proposed by the Agency for Healthcare Research and Quality emphasizes the advantages of conducting mixed methods studies to provide important dimensions in an evaluation study [68]. Thus, future HIT research studies should be designed as mixed methods sociotechnical evaluations focused on exploring the dynamic relationship between technology and social factors over time [65].
Conclusion
Measuring HIT adaptation can provide a more thorough understanding of the connection between HIT use and health care outcomes. Our ability to advance our understanding is predicated on good evaluation models, notably in the area of a health organization’s overall performance. As the sociotechnical environment remains a confounding problem influencing our understanding of the generalizability of research findings about HIT implementation success, there is a need to integrate issues exacerbated by workarounds, poorly designed interfaces, suboptimal functionality, and the sheer complexity of systems that contribute to HIT adoption issues as well as consider the idiosyncrasies across contexts. However, existing evaluation models are not supportive of a greater understanding of the phenomenon itself. This paper is therefore presented to provide a new perspective to shift the focus from adoption to adaptation. Future research should develop instruments to evaluate the progress of HIT adaptation in both its longitudinal design and its focus on adaptation progress rather than on a single outcome, allowing for more generalizability and knowledge transfer.
Acknowledgments
This work was supported by the Agency for Healthcare Research and Quality (R21HS024767).
Abbreviations
- CAS
complex adaptive system
- CQM
clinical quality measure
- EMRAM
electronic medical record adoption model
- HER
electronic health record
- HIMSS
Healthcare Information and Management Systems Society
- HIT
health information technology
- IT
information technology
- MU
Meaningful Use
- TAM
technology acceptance model
Footnotes
Conflicts of Interest: None declared.
References
- 1.Thompson T, Brailer D. Health IT Strategic Framework. Washington: US Department of Health and Human Services; 2004. [Google Scholar]
- 2.Adler-Milstein J, DesRoches C, Furukawa M, Worzala C, Charles D, Kralovec P. More than half of US hospitals have at least a basic EHR but stage 2 criteria remain challenging for most. Health Aff (Millwood) 2014 doi: 10.1377/hlthaff.2014.0453. [DOI] [PubMed] [Google Scholar]
- 3.DesRoches CM, Charles D, Furukawa MF, Joshi MS, Kralovec P, Mostashari F, Worzala C, Jha AK. Adoption of electronic health records grows rapidly, but fewer than half of US hospitals had at least a basic system in 2012. Health Aff (Millwood) 2013 Aug;32(8):1478–1485. doi: 10.1377/hlthaff.2013.0308. http://content.healthaffairs.org/cgi/pmidlookup?view=long&pmid=23840052. [DOI] [PubMed] [Google Scholar]
- 4.US Centers for Medicare & Medicaid Services Electronic health records (EHR) incentive programs 2017. [2017-08-18]. https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/index.html?redirect=/EHRIncentivePrograms .
- 5.DeSalvo KB, Salavitt A. Moving toward improved care through information. 2016. [2017-08-18]. https://www.healthit.gov/buzz-blog/from-the-onc-desk/moving-improved-care-information/
- 6.Manchikanti L, Helm IS, Calodney AK, Hirsch JA. Merit-based incentive payment system: meaningful changes in the final rule brings cautious optimism. Pain Physician. 2017;20(1):E1–E12. http://www.painphysicianjournal.com/linkout?issn=1533-3159&vol=20&page=E1. [PubMed] [Google Scholar]
- 7.Manchikanti L, Benyamin R, Falco F, Hirsch J. Metamorphosis of medicine in the United States: a carrot and stick policy of electronic medical records. Pain Physician. 2014;17(6):e671–e680. [PubMed] [Google Scholar]
- 8.Manchikanti L, Hirsch JA. A case for restraint of explosive growth of health information technology: first, do no harm. Pain Physician. 2015;18(3):E293–E298. http://www.painphysicianjournal.com/linkout?issn=1533-3159&vol=18&page=E293. [PubMed] [Google Scholar]
- 9.Ammenwerth E, Gräber S, Herrmann G, Bürkle T, König J. Evaluation of health information systems—problems and challenges. Int J Med Inform. 2003 Sep;71(2-3):125–135. doi: 10.1016/s1386-5056(03)00131-x. [DOI] [PubMed] [Google Scholar]
- 10.Singh R, Singh A, Singh DR, Singh G. Improvement of workflow and processes to ease and enrich meaningful use of health information technology. Adv Med Educ Pract. 2013;4:231–236. doi: 10.2147/AMEP.S53307. doi: 10.2147/AMEP.S53307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.McAlearney A, Hefner J, Sieck C, Rizer M, Huerta T. Evidence-based management of ambulatory electronic health record system implementation: an assessment of conceptual support and qualitative evidence. Int J Med Inform. 2014;83(7):484–494. doi: 10.1016/j.ijmedinf.2014.04.002. [DOI] [PubMed] [Google Scholar]
- 12.McAlearney AS, Hefner JL, Sieck C, Rizer M, Huerta TR. Fundamental issues in implementing an ambulatory care electronic health record. J Am Board Fam Med. 2015;28(1):55–64. doi: 10.3122/jabfm.2015.01.140078. http://www.jabfm.org/cgi/pmidlookup?view=long&pmid=25567823. [DOI] [PubMed] [Google Scholar]
- 13.McAlearney AS, Song PH, Robbins J, Hirsch A, Jorina M, Kowalczyk N, Chisolm D. Moving from good to great in ambulatory electronic health record implementation. J Healthc Qual. 2010;32(5):41–50. doi: 10.1111/j.1945-1474.2010.00107.x. [DOI] [PubMed] [Google Scholar]
- 14.Studeny J, Coustasse A. Personal health records: is rapid adoption hindering interoperability? Perspect Health Inf Manag. 2014;11:1e. http://europepmc.org/abstract/MED/25214822. [PMC free article] [PubMed] [Google Scholar]
- 15.D'Amore JD, Mandel JC, Kreda DA, Swain A, Koromia GA, Sundareswaran S, Alschuler L, Dolin RH, Mandl KD, Kohane IS, Ramoni RB. Are Meaningful Use Stage 2 certified EHRs ready for interoperability? Findings from the SMART C-CDA Collaborative. J Am Med Inform Assoc. 2014;21(6):1060–1068. doi: 10.1136/amiajnl-2014-002883. http://europepmc.org/abstract/MED/24970839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ford E, Pettit L, Silvera G, Huerta T. EMR implementation speed: patient safety culture paradox. J Healthc Inform Manage. 2014;28(3):24–31. [Google Scholar]
- 17.Sakata K, Stephenson L, Mulanax A, Bierman J, McGrath K, Scholl G. Professional and interprofessional differences in electronic health records use and recognition of safety issues in critically ill patients. J Interprof Care. 2016:1–7. doi: 10.1080/13561820.2016.1193479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lorenzi N, Novak L, Weiss J, Gadd C, Unertl K. Crossing the implementation chasm: a proposal for bold action. J Am Med Inform Assoc. 2008;15(3):290–296. doi: 10.1197/jamia.M2583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Afonso A, Alfonso S, Morgan T. Short-term impact of meaningful use stage 1 implementation: a comparison of health outcomes in 2 primary care clinics. J Ambul Care Manage. 2017 doi: 10.1097/JAC.0000000000000179. [DOI] [PubMed] [Google Scholar]
- 20.Grinspan Z, Bao Y, Edwards A, Johnson P, Kaushal R, Kern L. Medicaid stage 1 meaningful use EHR incentive payments are associated with higher quality but not improvements in quality. Am J Med Qual. 2016 Oct 13; doi: 10.1177/1062860616673905. [DOI] [PubMed] [Google Scholar]
- 21.Levine DM, Healey MJ, Wright A, Bates DW, Linder JA, Samal L. Changes in the quality of care during progress from stage 1 to stage 2 of Meaningful Use. J Am Med Inform Assoc. 2017 Dec 01;24(2):394–397. doi: 10.1093/jamia/ocw127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kaplan B. Evaluating informatics applications—some alternative approaches: theory, social interactionism, and call for methodological pluralism. Int J Med Inform. 2001 Nov;64(1):39–56. doi: 10.1016/s1386-5056(01)00184-8. [DOI] [PubMed] [Google Scholar]
- 23.Wears RL, Berg M. Computer technology and clinical work: still waiting for Godot. JAMA. 2005 Mar 09;293(10):1261–1263. doi: 10.1001/jama.293.10.1261. [DOI] [PubMed] [Google Scholar]
- 24.Ward R. The application of technology acceptance and diffusion of innovation models in healthcare informatics. Health Policy and Technology. 2013;2:222–228. [Google Scholar]
- 25.US Centers for Medicare & Medicaid Services Step 5: achieve meaningful use stage 2. 2014. [2017-08-18]. https://www.healthit.gov/providers-professionals/step-5-achieve-meaningful-use-stage-2 .
- 26.Botta MD, Cutler DM. Meaningful use: floor or ceiling? Healthc (Amst) 2014 Mar;2(1):48–52. doi: 10.1016/j.hjdsi.2013.12.011. [DOI] [PubMed] [Google Scholar]
- 27.Nakamura MM, Harper MB, Castro AV, Yu FB, Jha AK. Impact of the meaningful use incentive program on electronic health record adoption by US children's hospitals. J Am Med Inform Assoc. 2015 Mar;22(2):390–398. doi: 10.1093/jamia/ocu045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.HIMSS Analytics EMR adoption model. 2009. [2017-08-18]. http://www.himssanalytics.org/hc_providers/emr_adoption.asp .
- 29.Phichitchaisopa N, Naenna T. Factors affecting the adoption of healthcare information technology. EXCLI J. 2013;12:413–436. http://europepmc.org/abstract/MED/26417235. [PMC free article] [PubMed] [Google Scholar]
- 30.Venkatesh V, Sykes T, Zhang X. “Just what the doctor ordered:” a revised UTAUT for EMR system adoption and use by doctors. Proceedings of the 44th Hawaii International Conference on System Sciences; 2011; Kauai. 2011. [Google Scholar]
- 31.Patel V, Jamoom E, Hsiao C, Furukawa M, Buntin M. Variation in electronic health record adoption and readiness for meaningful use: 2008-2011. J Gen Intern Med. 2013 Jul;28(7):957–964. doi: 10.1007/s11606-012-2324-x. http://europepmc.org/abstract/MED/23371416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Steininger K, Stiglbauer B, Baumgartner B, Engleder B. Factors explaining physicians' acceptance of electronic health records. 47th Hawaii International Conference on System Science; 2014; Waikoloa. 2014. [Google Scholar]
- 33.Liu Z, Min Q, Ji S. A comprehensive review of research in IT adoption. 4th International Conference on Wireless Communications, Networking and Mobile Computing; 2008; Dalian. 2008. [Google Scholar]
- 34.Davis F. User acceptance of information technologyystem characteristics, user perceptions, and behavioral impacts. Int J Man Mach Stud. 1993;38(3):475–487. [Google Scholar]
- 35.Davis FD. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Quarterly. 1989;13(3):318–340. [Google Scholar]
- 36.Gangwar H, Date H, Raoot A. Review of IT adoption: insights from recent technologies. J Enterprise Inform Manag. 2014;27(4):488–502. [Google Scholar]
- 37.Center for Medicare and Medicaid Services Clinical quality measures. 2014. [2017-08-18]. http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/2014_ClinicalQualityMeasures.html .
- 38.Spetz J, Burgess JF, Phibbs CS. The effect of health information technology implementation in Veterans Health Administration hospitals on patient outcomes. Healthc (Amst) 2014 Mar;2(1):40–47. doi: 10.1016/j.hjdsi.2013.12.009. [DOI] [PubMed] [Google Scholar]
- 39.Agha L. The effects of health information technology on the costs and quality of medical care. J Health Econ. 2014 Mar;34:19–30. doi: 10.1016/j.jhealeco.2013.12.005. http://europepmc.org/abstract/MED/24463141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Robertson A, Cresswell K, Takian A, Petrakaki D, Crowe S, Cornford T. Implementation and adoption of nationwide electronic health records in secondary care in England: qualitative analysis of interim results from a prospective national evaluation. Brit Med J. 2010:341. doi: 10.1136/bmj.c4564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Wang Y, Gu J, Zhou Z. Complex adaptive socio-technical systems theory view of ubiquitous computing systems research. Ubiquitous Computing and Ambient Intelligence Personalisation and User Adapted Services; 2014; Belfast. 2014. pp. 216–223. [Google Scholar]
- 42.Sittig D, Singh H. A new sociotechnical model for studying health information technology in complex adaptive healthcare systems. Qual Safety Healthc. 2010;19:68–74. doi: 10.1136/qshc.2010.042085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Ellis B, Herbert S. Complex adaptive systems (CAS): an overview of key elements, characteristics and application to management theory. Inform Prim Care. 2011;19(1):33–37. doi: 10.14236/jhi.v19i1.791. [DOI] [PubMed] [Google Scholar]
- 44.Harrison MI, Koppel R, Bar-Lev S. Unintended consequences of information technologies in health care—an interactive sociotechnical analysis. J Am Med Inform Assoc. 2007;14(5):542–549. doi: 10.1197/jamia.M2384. http://europepmc.org/abstract/MED/17600093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Ellis B. Complexity in practice: understanding primary care as a complex adaptive system. Inform Prim Care. 2010;18(2):135–140. doi: 10.14236/jhi.v18i2.763. [DOI] [PubMed] [Google Scholar]
- 46.Gagnon M, Desmartis M, Labrecque M, Car J, Pagliari C, Pluye P. Systematic review of factors influencing the adoption of information and communication technologies by healthcare professionals. J Med Syst. 2012;36(1):241–277. doi: 10.1007/s10916-010-9473-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Patel V, Kannampallil T. Human factors and health information technology: current challenges and future directions. Yearb Med Inform. 2014;9(1):58–66. doi: 10.15265/IY-2014-0005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Coiera E. Putting the technical back into socio-technical systems research. Int J Med Inform. 2007;76:S98–S103. doi: 10.1016/j.ijmedinf.2006.05.026. [DOI] [PubMed] [Google Scholar]
- 49.Balka E, Tolar M, Coates S, Whitehouse S. Socio-technical issues and challenges in implementing safe patient handovers: insights from ethnographic case studies. Int J Med Inform. 2013;82(12):e345–e357. doi: 10.1016/j.ijmedinf.2012.11.001. [DOI] [PubMed] [Google Scholar]
- 50.Ludwick D, Doucette J. Adopting electronic medical records in primary care: lessons learned from health information systems implementation experience in seven countries. Int J Med Inform. 2009;78(1):22–31. doi: 10.1016/j.ijmedinf.2008.06.005. [DOI] [PubMed] [Google Scholar]
- 51.Kannampallil T, Schauer G, Cohen T, Patel V. Considering complexity in healthcare systems. J Biomed Inform. 2011;44(6):943–937. doi: 10.1016/j.jbi.2011.06.006. [DOI] [PubMed] [Google Scholar]
- 52.Majchrzak A, Rice R, Malhotra A, King N. Technology adaptation: the case of a computer-supported inter-organizational virtual team. MIS Quarterly. 2000;24(4):569–600. [Google Scholar]
- 53.Cooper R, Zmud R. Information technology implementation research: a technological diffusion approach. Manag Sci. 1990;36:123–139. [Google Scholar]
- 54.Center for Medicare and Medicaid Services EHR Incentive Programs. 2014. [2017-08-18]. http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Stage_2.html .
- 55.Blumenthal D, Tavenner M. The “meaningful use” regulation for electronic health records. New Engl J Med. 2010;363(6):501–504. doi: 10.1056/NEJMp1006114. [DOI] [PubMed] [Google Scholar]
- 56.Marcotte L, Seidman J, Trudel K, Berwick D, Blumenthal D, Mostashari F. Achieving meaningful use of health information technology: a guide for physicians to the EHR incentive programs. Arch Intern Med. 2012;172(9):731–736. doi: 10.1001/archinternmed.2012.872. [DOI] [PubMed] [Google Scholar]
- 57.Donabedian A. The quality of medical care. Science. 1978 May 26;200(4344):856–864. doi: 10.1126/science.417400. [DOI] [PubMed] [Google Scholar]
- 58.Kukafka R, Johnson S, Linfante A, Allegrante J. Grounding a new information technology implementation framework in behavioral science: a systematic analysis of the literature on IT use. J Biomed Inform. 2003;36(3):218–227. doi: 10.1016/j.jbi.2003.09.002. [DOI] [PubMed] [Google Scholar]
- 59.eHealth Observatory and School of Health Information Science University of Victoria Benefits evaluation indicators, technical report. 2012. [2017-08-18]. https://www.infoway-inforoute.ca/en/component/edocman/450-benefits-evaluation-indicators-technical-report-version-2-0/view-document?Itemid=101 .
- 60.Agency for Healthcare Research and Quality Health IT evaluation measures. 2014. [2017-08-18]. https://healthit.ahrq.gov/health-it-tools-and-resources/evaluation-resources/health-it-evaluation-toolkit-and-evaluation-measures-quick-reference .
- 61.Jamoom E, Patel V, Furukawa M, King J. EHR adopters vs non-adopters: impacts of, barriers to, and federal initiatives for EHR adoption. Healthcare. 2014;2:33–39. doi: 10.1016/j.hjdsi.2013.12.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Price M, Singer A, Kim J. Adopting electronic medical records: are they just electronic paper records? Canadian Fam Physician. 2013;59(7):e322–e329. [PMC free article] [PubMed] [Google Scholar]
- 63.Ash J, Sittig D, Guappone K, Dykstra R, Richardson J, Wright A. Recommended practices for computerized clinical decision support and knowledge management in community settings: a qualitative study. BMC. 2012;12:6. doi: 10.1186/1472-6947-12-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Hsiao J, Chang H, Chen R. A study of factors affecting acceptance of hospital information systems: a nursing perspective. J Nurs Res. 2011;19(2):150–160. doi: 10.1097/JNR.0b013e31821cbb25. [DOI] [PubMed] [Google Scholar]
- 65.Cresswell KM, Sheikh A. Undertaking sociotechnical evaluations of health information technologies. Inform Prim Care. 2014;21(2):78–83. doi: 10.14236/jhi.v21i2.54. doi: 10.14236/jhi.v21i2.54. [DOI] [PubMed] [Google Scholar]
- 66.Hameed M, Counsell S, Swift S. A conceptual model for the process of IT innovation adoption in organizations. J Engineer Technol Manag. 2012;29(3):358–390. [Google Scholar]
- 67.Spaulding A, Gamm L, Kim J, Menser T. Multiproject interdependencies in health systems management: a longitudinal qualitative study. Health Care Manag Rev. 2014;39(1):31–40. doi: 10.1097/HMR.0b013e31828265f2. [DOI] [PubMed] [Google Scholar]
- 68.Agency for Healthcare Research and Quality Health Information Technology Evaluation Toolkit. 2009. [2017-08-18]. https://healthit.ahrq.gov/sites/default/files/docs/page/Evaluation%20Toolkit%20Revised%20Version.pdf .