

Abstract
We examined the relation of interpersonal and media exposure to nonsuicidal self-injury (NSSI) among 340 university students in the southeastern United States (73.5% female, M age = 19.38 years, SD = 1.15). We also assessed interactions and main effects of each exposure and emotion dysregulation in relation to NSSI, testing the social learning hypothesis of NSSI. Most participants endorsed medium to high levels of exposure to NSSI via media sources. More than one-third of participants were somewhat or very familiar with someone who engaged in NSSI. Almost half reported occasional or frequent conversations about NSSI. Both exposure forms were significantly related to NSSI history. However, hurdle regression analyses revealed that interpersonal exposure and emotion dysregulation, but not media exposure, were significantly associated with NSSI history and frequency. We did not find evidence for an emotion dysregulation-by-interpersonal exposure interaction. We discuss implications for theoretical models of NSSI, limitations, and future directions.
Keywords: Social learning, self-injurious behavior, NSSI, emotion regulation
Social cognitive theory suggests that modeling can lead to the acquisition of unhealthy as well as healthy behaviors (Bandura, 2001). Previous work has documented the effect of social learning on suicidality, substance abuse, disordered eating, as well as positive behaviors such as exercise (e.g., Akers, 1977; DiLorenzo Stucky-Ropp, Vander Wal & Gotham, 1998; Fischer & Smith, 2008; Gould, Jamieson, & Romer, 2003; Levine & Smolak, 1998). Recently, researchers have examined social learning as an etiological mechanism underlying nonsuicidal self-injury (NSSI; e.g., Hasking, Andrews, & Martin, 2013; Heilbron & Prinstein, 2008). NSSI is defined as direct and intentional destruction of body tissue without the intent to die that is distinct from socially condoned behaviors such as tattooing or piercing (Nock, 2010). Such behaviors occur across the lifespan, but are particularly prevalent among adolescents and young adults (Nock, 2010; Swannell, Martin, Page, Hasking, & St. John, 2014). Although researchers have begun to document the effect of social learning on NSSI among adolescents, less is known about its function among young adults (e.g., Claes, L., Houben, A., Vandereycken, W., Bijttebier, P., & Muehlenkamp, 2010; Jarvi, Jackson, Swenson, & Crawford, 2013; Muehlenkamp, J. J., Hoff, E. R., Licht, J., Azure, J. A., & Hasenzahl, S.J., 2008; You, Lin, Fu, & Feung, 2013). In the current study, we measured both media and interpersonal exposure to NSSI among a sample of young adults. We then examined the social learning hypothesis of NSSI, which states that social exposure to the behavior (via media or through contact with peers) combines with underlying psychological vulnerabilities such as emotion dysregulation to impact engagement in the behavior.
Past studies highlight the high prevalence of NSSI among young adults and emphasize the importance of conducting research on the topic. A meta-analytic review of research in non-clinical populations estimated NSSI prevalence rates at 13.4% of the young adult population, with rates from individual studies ranging from as low as 3% to as high as 52% (with the majority of the variance accounted for by methodological factors; Swannell et al., 2014). NSSI has been linked to a broad range of psychopathologies including depression, anxiety, substance abuse, anger, assault, and disordered eating (e.g., Hilt & Hamm, 2014; Jarvi, Jackson, Swenson, & Crawford, 2013; Weismoore & Esposito-Smythers, 2010). Alarmingly, recent or persistent engagement in NSSI even predicted suicidal ideation in a sample of university students (Hamza & Willoughby, 2014). Given these findings, it is important to examine possible influences for the behavior, so as to guide prevention and intervention efforts.
Individuals overwhelmingly report engaging in NSSI to regulate negative affect, and emotion regulation difficulties consistently emerge as correlates of the behavior (Brickman, Ammerman, Look, Berman, & McCloskey, 2014; Gratz & Roemer, 2008; Klonsky, 2007; Zelkowitz, Cole, Han, & Tomarken, 2016). Nock’s four-function model suggests that NSSI serves as a negative reinforcer insofar as it helps to reduce unwanted emotions (Bentley, Nock, & Barlow, 2014; Nock, 2009; Nock, 2010; Nock & Prinstein, 2004.) Studies among college students have shown that the down-regulation of negative emotion is a particularly salient motivation for this population (e.g., Anderson & Crowther, 2012; Armey, Crowther, & Miller, 2011; Whitlock et al., 2011). Additional studies have further supported these findings by demonstrating that individuals often report a significant reduction in negative affect immediately after engaging in NSSI (e.g., Armey et al., 2011; Nock, Prinstein, & Sterba, 2009). Chapman, Gratz, and Brown (2006) posited that heightened negative emotions and deficits in the ability to regulate emotions predispose one to engage in NSSI. Nock’s (2009) integrated theoretical model of the development and maintenance of self-injury also highlights a potential role for emotion dysregulation in the etiology or maintenance of NSSI. Etiological theories have highlighted the interplay between distal social, biological, or demographic characteristics and proximal attributes such as emotion dysregulation in the prediction of NSSI (e.g., Nock, 2009). McKenzie and Gross (2014) also outline multiple mechanisms by which individuals may use NSSI, in lieu of more adaptive approaches, to regulate their emotions. Although research supports the statistically significant role of emotion dysregulation in NSSI, effect sizes are relatively small. In addition, other research suggests emotion regulation functions for other dysfunctional behaviors besides NSSI, such as substance abuse and disordered eating (e.g., Aldao, Nolen-Hoeksema, & Schweizer, 2010). These observations suggest the need to consider additional, NSSI-specific, etiological processes in tandem with or as moderators of emotion dysregulation.
Social exposure to NSSI represents one such process to explore. People may learn about NSSI through the media or via their own interpersonal networks (although people may also discover the behavior independently via processes such as pain offset relief; Franklin, Lee, Hanna, & Prinstein, 2013). Preliminary research suggests that both in-person and media exposure are associated with greater rates of NSSI. Work by Hasking and colleagues (2013) showed that among Australian adolescents, having friends who engaged in NSSI predicted their own NSSI one year later. In a sample of Chinese adolescents, You, Lin, Fu, and Leung (2013) found that having a best friend who engages in NSSI or belonging to a peer group in which the behavior is prevalent significantly increased risk of NSSI after six months. Additional cross-sectional studies have shown that adolescents with friends who engage in NSSI are significantly more likely to engage in NSSI themselves (e.g., Claes, Houben, Vandereycken, Bijttebier, & Muehlenkamp, 2010). The role of social learning in NSSI among university students has received comparatively less attention. In one of the few examinations of social exposure to NSSI among university students, Hasking and Rose (2016) identified a significant association between number of friends who engage in NSSI and lifetime history of the behavior; however, we know little about the means by which such interpersonal exposure occurs (e.g., via conversation or direct observation). Consequently, one goal of the current study was to obtain more nuanced information about the role that interpersonal exposure may play in initiating or perpetuating NSSI in this population.
Previous research also suggests that exposure to NSSI-related content in the media may influence behavior (e.g., Jarvi et al., 2013; Lewis, Heath, Michal, & Duggan, 2012). In studies of online references to NSSI, participants have reported feeling triggered by graphic videos of the behavior on the Web and learning strategies for engaging in NSSI from those who engage in it (Lewis & Seko, 2016; Lewis et al., 2012; Whitlock, Powers, & Eckenrode, 2006). Initial findings conflict about the impact of NSSI references in movies. Radovic and Hasking (2013) found that greater exposure to NSSI references in movies and greater identification with the movie characters related to increased likelihood of engaging in NSSI. In contrast, Hasking and Rose (2016) found no relation between number of movies with NSSI references and either probability of engaging in any NSSI or frequency of NSSI acts. Given these conflicting results, more research is clearly needed to understand how media exposure relates to behavior in this population. Consequently, a second goal of the current study was to obtain detailed information about the nature of media exposure and its relation to NSSI.
Important work has examined social exposure to NSSI via the framework of social learning and social cognitive theory (Bandura, 1977; Bandura, 1986). This work has generally focused on identifying main effects of social exposure to NSSI on the behavior and the interactions of social exposure with expectancies about the behavior (e.g., Hasking & Rose, 2016). Nock’s theory of the etiology of NSSI, however, posits social learning as one mechanism by which individuals with underlying cognitive or emotional deficits might select NSSI versus another maladaptive behavior (Nock, 2009, 2010). Empirical evidence for this hypothesis would stem from either (1) a multiplicative interaction effect, in which social exposure to NSSI increases the relation of emotion dysregulation to NSSI, or (2) a set of additive main effects, in which both social exposure to NSSI and emotion dysregulation relate significantly to NSSI.
The present study had three main aims. Our first aim was to characterize the extent of both interpersonal and media exposure to NSSI in a sample of university students by considering multiple types of media and a range of interpersonal domains. Our second major aim was to examine how such social exposures to NSSI relate to self-reported history of the behavior. Our final aim was to examine the combined effects (via either interactions or main effects) of emotion dysregulation, interpersonal exposure and media exposure on NSSI, thus presenting an initial test of Nock’s social learning hypothesis (Nock, 2010). We first tested the social exposures by emotion dysregulation interactions. Second, if the interactions were nonsignificant, we tested the main effects. As such, we aimed to complement and extend initial work by Hasking and Rose (2016) on the relation of social exposure to NSSI in a university student population.
Methods
Participants
Participants included 340 students recruited over two semesters from the research subject pool at a mid-sized private university located in the southeastern United States. Average age of the participants was 19.38 (SD = 1.15), and 73.5% of participants were female. The sample was moderately diverse: 71.5% White, 17.4% Asian or American-Asian, 10.3% Black, 7.4% Hispanic, and 2.6% other (representative of the population from which they were drawn). We used listwise deletion in response to missing data, thus sample sizes fluctuated by analyses.1 Participants excluded from the Aim 3 analysis (our most complex model) were not significantly different from those included on gender, mean scores for interpersonal exposure, media exposure, and emotion dysregulation (ps > .10).
Measures
Social Exposure to NSSI
We used the Social Exposure to Nonsuicidal Self-Injury Scale (SENS; Zelkowitz & Cole, 2014) to measure participants’ social exposure to NSSI. This is a two-part measure that assesses exposure to NSSI from media and interpersonal sources. Items were rationally derived by reviewing the literature on social exposure to NSSI, then generating stems which reflected key constructs in the literature. The first section asks all respondents, regardless of NSSI history, to endorse the degree of exposure to NSSI from media and interpersonal sources on a 1 (never) to 4 (frequently) scale, with each item representing exposure to NSSI from a particular source (e.g., movies, TV, talking with others who have engaged in NSSI, having friends who engage in NSSI, etc.). We conducted an exploratory factor analysis using oblique rotation on the items, then visually inspected scree plots and assessed for eigenvalues greater than one to guide factor extraction. Results revealed a two-factor structure. Media-focused items loaded onto Factor 1; interpersonal items loaded onto Factor 2. Table 1 shows the factor loadings for each item. Two items failed to load meaningfully on either factor. We retained these questions for item-level analysis but did not include them in the summed scores for interpersonal and media exposure to NSSI. We reproduced this factor structure using data from participants in the second semester. Internal consistency was acceptable for both the interpersonal (Cronbach’s alpha = .85) and media subscale (Cronbach’s alpha = .79). Item-total correlations for the interpersonal subscale ranged from .59 to .79 and from .53 to .74 for the media subscale.
Table 1.
Exploratory Factor Analysis of SENS Items
| Item content | Factor 1 Interpersonal | Factor 2 Media |
|---|---|---|
| 10. I have talked about NSSI with people who have done it. | .915 | −.103 |
| 1. I am personally familiar with individuals who engage/have engaged in some form of NSSI. | .883 | −.094 |
| 7. I have friends who engage in NSSI. | .772 | .018 |
| 9. I have talked about NSSI with other people (regardless of whether they engaged in the behavior). | .611 | .124 |
| 4. I have seen references to different forms of NSSI in movies. | −.009 | .860 |
| 5. I have seen, heard, or read news reports about NSSI. | −.060 | .717 |
| 6. I have seen references to NSSI on TV (sitcoms, dramas, serials - not movies on TV or news programs). | −.005 | .656 |
| 3. I have heard references to NSSI in music lyrics. | .167 | .547 |
| 2. I have seen Internet forums or blogs about NSSI. | .345 | .217 |
| 8. I have observed someone engage in a form of NSSI (in person, not on TV or in a movie). | .295 | .016 |
Note. Factors correlated .49 with each other. Factor loadings > .40 are printed in bold.
Emotion Dysregulation
We used the Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004) to assess emotion dysregulation. The DERS is a 36-item questionnaire designed to assess respondents’ difficulties in various domains of emotion regulation. Respondents indicate their agreement with items using a 1 to 5 scale (“almost never” to “almost always”). Items are coded or reverse-coded such that higher scores indicate greater difficulties in emotion regulation. Initial factor analysis and validation by Gratz and Roemer (2004) revealed six factors: Limited access to emotion regulation strategies (Strategies), nonacceptance of emotional responses (Nonacceptance), difficulties engaging in goal-directed behavior (Goals), impulse control difficulties (Impulse), lack of emotional awareness (Awareness), and lack of emotional clarity (Clarity). Although the items can also be summed to generate a total score, growing evidence indicates that the six factors do not converge onto a single, higher-order factor (Bardeen, Fergus, & Orcutt, 2012; Lee, Witte, Bardeen, Davis, & Weathers, 2016; Zelkowitz & Cole, 2016). Research on the DERS suggests the Awareness subscale, in particular, does not represent the same higher-order factor onto which the other five subscales load. Consequently, we summed the five unidimensional subscales to create a total emotion dysregulation score, as suggested by Lee, Witte, Bardeen, Davis, & Weathers (2016). Here, we use the term “DERS dysregulation composite (DERS-DC)” to refer to the composite of Strategies, Nonacceptance, Goals, Impulse, and Clarity. Internal consistency for this modified composite was excellent (Cronbach’s alpha = .93).
Inventory of Statements about Self-Injury
(ISAS, Klonsky & Olino, 2008). We used part one of the ISAS to measure self-reported NSSI. The ISAS is a two-part instrument that assesses respondents’ experience with self-injurious behaviors and reasons for engaging in those behaviors. The survey instructions specify that any self-harm behavior should be done “on purpose” and “without suicidal intent” (Klonsky & Olino, 2008). Part one then asks respondents to estimate the number of times they engaged in any of 12 different NSSI behaviors, the age at which the NSSI began, the amount of time that elapsed between urges to engage in NSSI and the behavior, and whether the individual would like to stop harming themselves. The measure has shown both adequate four-week and one-year test-retest reliability (Glenn & Klonsky, 2011; Klonsky & Glenn, 2009). Those who do not endorse any form of self-injury only complete the first of these questions. Part two of the ISAS asks those respondents who report a history of NSSI to assess its function by indicating their agreement with 39 statements (e.g., “when I self-harm, I am…”). These statements correspond to 13 subscales, which in turn load onto two higher-order factors (i.e., interpersonal and intrapersonal functions; Klonsky & Glenn, 2009). Initial validation showed strong internal consistency for these higher-order subscales (Cronbach’s alphas = .80–.88; Klonsky & Glenn, 2009). Internal consistency in the present sample was acceptable (Cronbach’s alphas = .73–.85).
As some of the milder behaviors listed on Part 1 may reflect processes other than self-injury (i.e., interfering with wound healing, hair pulling, swallowing substances), we omitted these from our analyses. Thus, the final dataset included nine NSSI behaviors. Total NSSI scores were based on summing scores for each behavior. Individuals with missing data on any of the nine behaviors were coded as missing for total NSSI score to ensure the most conservative analysis. Table 2 shows the proportion of respondents endorsing each behavior, along with frequency statistics for these behaviors. Table 3 shows the degree to which respondents with NSSI histories endorsed each function for their behavior.
Table 2.
Lifetime Prevalence and Frequency of NSSI Behaviors among Participants Endorsing any NSSI History (N = 77)
| NSSI Behavior | % of Sample Endorsing the Behavior | M (SD) |
|---|---|---|
| Pinching | 51.95 | 17.94 (49.09) |
| Banging or Hitting Self | 49.35 | 13.10 (59.21) |
| Severe Scratching | 25.97 | 1.82(4.24) |
| Cutting | 33.77 | 9.92 (58.04) |
| Biting | 23.38 | 9.36 (52.87) |
| Rubbing Skin Against Rough Surface | 9.09 | 1.86 (8.66) |
| Burning | 9.09 | 0.49 (1.85) |
| Sticking Self with Needles | 7.79 | 0.26 (0.98) |
| Carving | 5.19 | 0.08 (0.35) |
Table 3.
Means and Standard Deviations for 13 ISAS Functions and Total Intrapersonal and Interpersonal Function Scores (N = 77)
| ISAS Function | M (SD) |
|---|---|
| Affect Regulation | 2.53 (2.08) |
| Self-Punishment | 2.00 (1.81) |
| Self-Care | 0.63 (1.26) |
| Anti-Dissociation | 0.97 (1.55) |
| Anti-Suicide | 0.48 (1.23) |
| Sensation Seeking | 0.48 (1.00) |
| Peer Bonding | 0.22 (0.77) |
| Interpersonal Influence | 0.44 (1.04) |
| Marking Distress | 0.99 (1.52) |
| Toughness | 0.77 (1.41) |
| Revenge | 0.27 (0.77) |
| Autonomy | 0.56 (1.17) |
| Interpersonal | 3.88 (6.03) |
| Intrapersonal | 6.97 (5.70) |
Procedure
We distributed information about the study to undergraduate students in psychology classes and the research subject pool. The study description noted that participants would answer questions about how they dealt with emotions and about NSSI (the term “cutting” was given as an example of NSSI in the description materials). Participants independently completed all measures online using REDCap electronic data capture system (Harris et al., 2009) after reading a detailed description of the study procedures and indicating their informed consent. The consent form and survey instructions specified that participants did not have to answer any questions they did not want to and could discontinue at any time. The survey took approximately 45 minutes to complete, and participants received course credit in exchange for their time. Participants reporting elevated depressive symptoms or indicating that they wanted help with NSSI were contacted individually and given referrals to the university counseling center.
Data Analytic Plan
Our three main aims consisted were to (a) describe the extent of interpersonal and media exposure to NSSI among a sample of university students; (b) test relations of each type of social exposure to self-reported history of NSSI; and (c) test social exposure as a moderator of the relation of difficulties in emotion regulation to NSSI (thus examining the social learning hypothesis of NSSI; Nock, 2010). We addressed the first goal by reporting descriptive statistics on various forms of social exposure to NSSI among the whole sample, regardless of NSSI history. We also estimated the correlation of media and social exposure within the entire sample and tested for significant differences between these forms of exposure. To address the second goal, we divided the sample into two groups based on any lifetime NSSI history versus none. We then used multivariate analysis of variance (MANOVA) to test for differential reports of media exposure and interpersonal exposure among those with a history of NSSI versus no history of the behavior. Third, to test the social exposure as a moderator of the relation of emotion dysregulation, we standardized each social exposure variable and the total DERS score (not including the Awareness subscale) using the scale function in R Studio (R Studio Team, 2015). We then used the standardized scores to create interaction terms. We used a hurdle model to account for the extreme skewness and excessive number of 0s in the data (Hilbe, 2011). This model generates two sets of estimates. The first represents the contribution of each independent variable to whether an individual has a history of NSSI. The second assesses the relation of the independent variables to the frequency of behavior (modeled only within the context of those who have a history of NSSI). In the absence of significant interaction terms, we tested for main effects of social exposure and emotion dysregulation. Only individuals with full information on all constructs were included in the hurdle model test. Thus, these analyses were conducted on a dataset of n = 291. All other analyses were conducted on the full dataset. Hurdle model tests were conducted using the pscl package for R (Zeileis, Kleiber, & Jackman, 2008). All other statistical analyses were conducted using SPSS versions 23 and 24.
Results
Descriptive Statistics
Seventy-seven participants (22.65%) endorsed at least one instance of lifetime NSSI behavior, 70 (90.91%) endorsed at least two, and 64 (83.12%) endorsed five or more instances. Forty-two (54.55%) participants endorsed more than one method, and 24 (31.17%) participants endorsed more than two methods of self-injury. No method of injury emerged as preferred by a clear majority of those endorsing multiple methods.2 The average number of self-injury methods endorsed by those with any history of self-injury was 2.16 (SD = 1.49). Sixty individuals provided information about both age of onset and date of most recent episode. Mean age of onset was 13.53 (SD = 4.10); 62% of those who provided recency data reported episodes within one year of data collection.
Table 2 shows the rate of endorsement of each self-injury method among those with a history of NSSI, along with the mean and standard deviation of episodes reported by each method. No single method of injury was endorsed by a clear majority of participants. Table 3 reports frequencies of reasons given for engaging in NSSI. Affect regulation was the most commonly cited function of NSSI, closely followed by self-punishment. We summed the number of episodes for all nine behaviors to generate a total score, which we then used in all subsequent analyses. As anticipated, this variable was positively skewed (M = 14.41, SD = 78.45, skewness = 9.77, SD of skewness = 0.14).
Aim 1: To Characterize the Extent of Interpersonal and Media Exposure
Initial results revealed exposure to NSSI in our sample across a broad array of interpersonal and media sources. The final row of Table 3 shows the percentage of our sample endorsing “some” or “a lot” of exposure to a particular source. The most commonly endorsed source of interpersonal exposure to NSSI was talking about NSSI with others who have not engaged in the behavior. The most commonly endorsed source of media exposure was via movie references to the behavior. Interpersonal exposure to NSSI (via friends, peers, etc.) was moderately correlated with exposure to NSSI in media sources such as music, television, and movies, r = .41, p < .01. Exposure to NSSI via media sources was significantly greater than exposure via interpersonal sources (mean difference = 1.94, SD = 3.27), t(314) = 10.54, p < .001). The 95% confidence interval for the mean difference based on percentile bootstrap analysis of 10,000 samples was 1.58 to 2.31.
Aim 2: To Examine Relations Among Interpersonal Exposure, Media Exposure, and NSSI
Individuals with no history of NSSI behavior reported significantly lower levels of both interpersonal exposure to NSSI, t(313) = −4.56 and media exposure, t(313) = −2.86 (ps < .01) compared to those with a history of NSSI.
We then tested whether within-subject differences in degree of NSSI exposure via different sources (e.g., T.V. vs. the Internet) differed for those who reported a history of NSSI versus those with no such history. We conducted separate multivariate analyses of variance for items on the interpersonal and media subscales. A MANOVA showed no significant exposure source-by-NSSI history interaction for the four sources of media exposure assessed, Wilk’s exact F(280) = 1.25, p = .29.
Exposure source did, however, interact significantly with NSSI history for the interpersonal sources assessed, Wilk’s exact F(286) = 2.75, p = .04. Individual t-tests revealed that those with a history of NSSI had great exposure than those with no history to the following sources: being personally familiar with someone who engages in NSSI (mean difference = −0.55, 95% CI[ −0.85, −0.25]), having friends who engage in NSSI (mean difference = −0.39, 95% CI[ −0.58, −0.21]), observing someone engage in NSSI (mean difference = −0.39, 95% CI[ −0.58, −0.21]), and talking with others who have engaged in NSSI, mean difference = −0.52, 95% CI[ −0.76, −0.27]). See Figure 1 for graph of means for exposure source by NSSI status.
Figure 1.
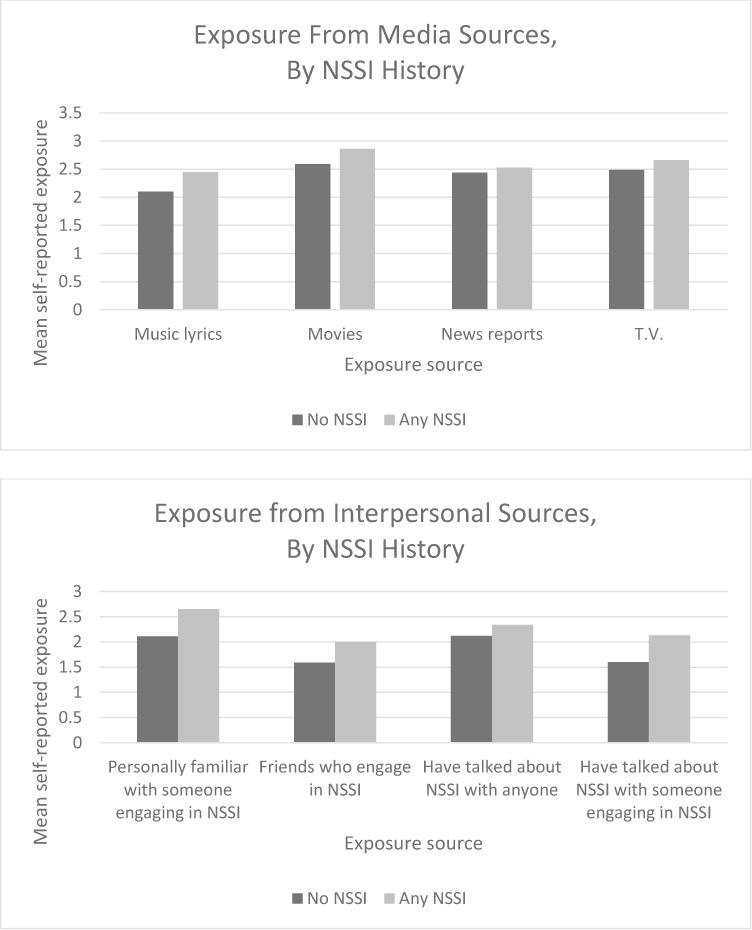
Social exposure to NSSI by source
Top panel depicts mean exposure to NSSI from four media sources. Bottom panel depicts mean exposure to NSSI from four interpersonal sources (questions about level of detail were not included in the statistical analysis). In both panels, black bars represent responses from those with no NSSI. Gray bars represent those with any NSSI history.
Aim 3: To Examine Social Exposure to NSSI as a Moderator of the Relation between Emotion Dysregulation and NSSI behavior
Our next goal was to test each exposure type as a moderator of the relation between emotion dysregulation and NSSI. Neither interpersonal exposure nor media exposure to NSSI significantly moderated the relation to emotion dysregulation to NSSI history or NSSI frequency. We then tested the main effects of each type of social exposure and emotion dysregulation, each controlling for the other (see Table 5). The top portion of the table (hurdle model) shows the contribution of each construct to lifetime history of NSSI, controlling for the other two variables. Interpersonal exposure was significantly associated with NSSI history (b = 0.40, SE = 0.12, z = 3.28, p < .01). Coefficients in the hurdle portion of the model reflect the log-odds of engaging in any NSSI. Thus, a one-unit increase in interpersonal exposure score (which corresponds to an increase of one standard deviation due to variable scaling) was associated with a 49% increase in the odds of reporting a lifetime history of NSSI. Emotion dysregulation was also significantly associated with NSSI history (b = 0.34, SE = 0.11, z = 3.12, p < .01). This indicates that a one-unit increase in DERS-DC score (again corresponding to an increase of one standard deviation) was associated with a 40% increase in odds of reporting a lifetime history of NSSI. Media exposure was not significantly associated with NSSI history after controlling for interpersonal exposure and emotion dysregulation.
Table 5.
Main Effects of Emotion Dysregulation, Interpersonal Exposure and Media Exposure on NSSI
| Variable | b | SE | z |
|---|---|---|---|
|
Relation to any NSSI history (hurdle model, n = 291)
| |||
| 1. Intercept | −1.32 | 0.13 | −10.17** |
| 2. DERS-DC score | 0.34 | 0.11 | 3.12** |
| 3. Interpersonal Exposure | 0.40 | 0.12 | 3.28** |
| 4. Media Exposure | 0.16 | 0.14 | 1.15 |
|
Relation to NSSI frequency (positive-count model) | |||
| 1. Intercept | 2.93 | 0.28 | 10.31** |
| 2. DERS-DC score | 0.78 | 0.22 | 3.47** |
| 3. Interpersonal Exposure | 0.46 | 0.23 | 1.97* |
| 4. Media Exposure | −0.20 | 0.27 | −0.74 |
Note. DERS-DC = Difficulties in Emotion Regulation Strategies Dysregulation Composite (encompassing Strategies, Clarity, Impulse, Goals, and Acceptance subscales)
p <.05;
p < .01
The bottom portion of the table (positive count) shows the contribution of each construct to NSSI frequency, controlling for the other two variables. Interpersonal exposure to NSSI was significantly related to NSSI frequency (b = 0.46, SE = 0.23, z = 1.97, p = .048). Here, the coefficient shows the effect on log counts of NSSI. Thus, a one standard deviation increase in interpersonal exposure was associated with a 58% increase in odds of an additional NSSI episode. Emotion dysregulation was also significantly associated with NSSI frequency after controlling for the other variables (b = .78, SE = .22, z = 3.47, p < .01). The exponentiated coefficient reflects that a one standard deviation increase in emotion dysregulation was associated with a 118% increase odds of an additional NSSI episode. Media exposure was again no longer significant after controlling for interpersonal exposure to NSSI and emotion dysregulation. A likelihood ratio test showed no significant difference when media exposure was dropped from the full model with emotion dysregulation, interpersonal exposure, and media exposure (X2(2, N=291) = 1.8, p = .41)
Discussion
The current study tested an application of the social learning hypothesis of NSSI by examining the relation of media and interpersonal social exposure to lifetime incidence and frequency of NSSI. Three key findings emerged. First, we found that media and interpersonal exposure to NSSI were common in this sample of university students. Second, media and interpersonal exposure were moderately correlated with each other, and each was correlated with lifetime history of NSSI. Third, both interpersonal exposure to NSSI and emotion dysregulation were significantly associated with lifetime history of NSSI and NSSI frequency after controlling for the other construct. This offers preliminary support for the social learning hypothesis in NSSI (Nock, 2009, 2010). We did not find evidence for an emotion dysregulation X social exposure interaction or for a main effect of media exposure, however. We elaborate on these findings below.
Our work builds on previous literature establishing high rates of exposure to NSSI via both interpersonal and media sources among adolescents and extends this finding to an emerging adult population. Relatively few studies have examined prevalence of NSSI exposure in university samples. Muehlenkamp, Hoff, Licht, Azure, and Hasenzahl (2008) reported that roughly 64% of their college sample (consisting of both students with a history of self-injury and those without) knew someone who had engaged in NSSI. In a smaller study consisting exclusively of undergraduates who have engaged in self-injury, 59% reported self-injuring after a friend engaged in the behavior (Heath, Ross, Toste, Charlebois, & Nedecheva, 2009). Using a continuous measure to assess degree of exposure to multiple sources of interpersonal exposure, we found that 38% of our sample reported being either somewhat or very familiar with someone who engages in NSSI (only 16% said they had at least “a few” friends who engage in the behavior). Researchers have noted an increase in references to NSSI in media/entertainment in recent years (Jarvi et al., 2013; Purington & Whitlock, 2010; Radovic & Hasking, 2013; Trewavas, Hasking, & McAllister, 2010). To our knowledge, only one study has examined both media and interpersonal exposure within the same young adult sample. Hasking and Rose (2016) found nearly universal exposure to films containing references to NSSI in their sample, whereas roughly two-thirds of participants reported having a friend who self-injured. Similarly, we found support for nearly ubiquitous exposure to NSSI (via movies and television in particular), with fewer participants reporting personal knowledge of someone who self-injures or self-injured.
Our second major finding was that both interpersonal exposure and media exposure were related to NSSI history in our sample of university students. Previous work has established interpersonal exposure to NSSI as an important predictor of the behavior among adolescents (Hasking, Andrews, & Martin, 2013; You et al., 2013) and provided mixed evidence for media exposure as a correlate of NSSI in both adolescents and young adults (Hasking & Rose, 2016, Radovic & Hasking, 2013). We confirmed a relation of interpersonal exposure to occurrence of NSSI, further supporting an interpersonal influence model of NSSI. Results suggest such exposure includes individuals with and without personal histories of the behavior; almost half of our participants reported having had somewhat detailed discussions about NSSI with people who have not engaged in the behavior themselves. We also found that greater media exposure to NSSI distinguished between people with and without a lifetime history of the behavior, contrary to findings by Hasking and Rose (2016). The fact that we assessed multiple sources of media exposure (and not just movies) and used a more continuous measure of exposure may have driven the discrepancy between our results and theirs.
Finally, our findings represent an initial test of the social learning hypothesis of NSSI, in which social exposure combines with underlying vulnerabilities (e.g., emotion dysregulation) to lead to NSSI (Nock, 2010, 2009). Heilbron and Prinstein (2008) explicitly proposed such a model in their review and theoretical conceptualization of social influences on adolescent NSSI behavior. Nock (2009) highlighted this as one possible model (among many other potential pathways) in his integrated theoretical model of NSSI. Our findings support an additive model of the impact of interpersonal exposure and emotion regulation on both overall likelihood of engaging in NSSI and NSSI frequency. That is, greater interpersonal exposure to NSSI was associated with increased likelihood of reporting any lifetime NSSI history and NSSI frequency at both low and high levels of emotion dysregulation. Similarly, increasing emotion dysregulation was associated with both likelihood of reporting any lifetime NSSI and increasing NSSI frequency after controlling for interpersonal exposure. This contrasts somewhat with findings by You, Lin, Fu, & Feung (2013) that NSSI by an adolescent’s best friend predicted engagement in but not frequency of the adolescent’s own NSSI. However, there may be slight discrepancies between a friend’s engagement in NSSI and one’s actual exposure to the same, thus accounting for our differing results.
In contrast, we did not find support for media exposure as either a moderator or main effect on NSSI after controlling for emotion dysregulation and interpersonal exposure. The fact that media exposure was so widespread in our sample may have diminished its capacity to distinguish between those with and without a history of NSSI after controlling for more salient constructs. Hasking and Rose (2013) found increased association between media exposure and NSSI when participants reported greater identification with a movie character. Thus, another possible explanation for our findings is that participants did not identify with the media depictions of NSSI to which they were exposed. Continued research will be necessary to parse the impact of media exposure on NSSI behavior throughout adolescence and emerging adulthood.
Another important next step will be to examine longitudinally the role of interpersonal exposure, media exposure, and emotion dysregulation on NSSI onset versus maintenance. Such findings could have important clinical implications (e.g., assessing a client’s exposure to others who self-injure). Alternatively, if exposure to others’ NSSI or media depictions of the behavior showed a substantial effect on its initiation only, this would suggest a need for public health-oriented programs to limit exposure to NSSI on a broad scale (e.g., as in media guidelines for covering suicide). Clinicians working with individuals who engage in the behavior might focus on targets more relevant for its maintenance, however.
We acknowledge several key limitations of the current study that present opportunities for future research. First, as previously noted, our study was cross-sectional. This precludes our capacity to make predictive statements or to distinguish the impact of social exposure at various stages of an individual’s engagement in NSSI (e.g., onset versus maintenance). Second, we assessed lifetime episodes of NSSI behaviors and exposures rather than asking respondents to reflect exclusively on a particular timeframe (e.g., past year). Consequently, recall bias could have impacted our results. Third, we also cannot determine elapsed time between social exposure and NSSI behavior. Knowing a friend who engaged in NSSI during adolescence may impact behavior differently for university students than having friends who presently engage in it. Future efforts should carefully delineate timing of exposure and behavior. Such research should also allow participants to report on interpersonal and media exposures beyond those listed here. In doing so, it may be possible to assess more comprehensively the role of Web-based exposures (e.g., chatrooms, forums, websites, etc.) on NSSI behavior. Initial evidence suggests that such exposure may be especially important among adolescents (e.g., Lewis, 2016; Reid & Weigle, 2014). Fourth, the cross-sectional nature of this study precluded our ability to examine the direction of possible prospective relations between social exposure and NSSI. Individuals who engage in NSSI may be especially likely to seek out media with NSSI content (e.g. in movies and music). Alternatively, individuals who self-injure may attract or seek out conversations about self-injury or friends who also self-injure. Both of these processes could also operate simultaneously. Finally, although our sample contained substantial numbers of people who engaged in NSSI, we recognize that results may not generalize to other emerging adult populations in larger or smaller universities, non-university settings, or non-Western cultures. Despite these limitations, however, our results support the importance of social exposure, particularly interpersonal exposure, to NSSI in university students.
Table 4.
Correlations, Means, and Standard Deviations for SENS Items1
| Social exposure source | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Personally familiar with someone engaging in NSSI | 1.00 | |||||||||
| 2. Internet | 0.34 | 1.00 | ||||||||
| 3. Music lyrics | 0.29 | 0.36 | 1.00 | |||||||
| 4. Movies | 0.32 | 0.27 | 0.57 | 1.00 | ||||||
| 5. News | 0.16 | 0.24 | 0.38 | 0.56 | 1.00 | |||||
| 6. TV | 0.21 | 0.20 | 0.36 | 0.59 | 0.48 | 1.00 | ||||
| 7. Friends | 0.70 | 0.32 | 0.33 | 0.32 | 0.25 | 0.29 | 1.00 | |||
| 8. Direct observation | 0.15 | 0.23 | 0.14 | 0.02 | 0.18 | 0.08 | 0.29 | 1.00 | ||
| 9. Talk about NSSI with non-NSSIers a | 0.51 | 0.36 | 0.37 | 0.33 | 0.26 | 0.23 | 0.46 | 0.21 | 1.00 | |
| 10. Talk about NSSI with NSSIers a | 0.73 | 0.30 | 0.34 | 0.31 | 0.16 | 0.24 | 0.65 | 0.23 | 0.61 | 1.00 |
| Total NSSI b | 0.23 | 0.14 | 0.16 | 0.15 | 0.04 | 0.07 | 0.25 | 0.26 | 0.12 | 0.25 |
|
| ||||||||||
| Means | 2.25 | 1.70 | 2.18 | 2.64 | 2.46 | 2.53 | 1.70 | 1.20 | 2.18 | 1.75 |
| SDs | 1.20 | 0.93 | 0.96 | 0.79 | 0.90 | 0.89 | 0.74 | 0.53 | 0.99 | 0.90 |
| % endorsing medium or high exposure from this source | 38% | 24% | 48% | 71% | 60% | 64% | 16% | 5% | 45% | 23% |
Note. Correlations greater than r = .14 significant at p < .05; correlations greater than r = .15 significant at p < .01
Ns for SENS vary by item, ranging from 311 to 316. Ns for correlations between SENS items and total NSSI ranged from 291 to 293.
Refers to individuals who have not engaged and engaged in NSSI, respectively.
Spearman’s rho.
Wording for each SENS item differed. However, a “3” or “4” always corresponded to medium and high levels of exposure from this source.
Acknowledgments
R.L. Zelkowitz was supported in part from National Institute of Mental Health training grant T32MH018921-26 and F31MH108241-01A1.
Footnotes
Missing data varied fluctuated by variable (total NSSI, n = 47; emotion dysregulation, n = 14; media exposure, n = 24; interpersonal exposure, n = 25).
The majority of participants who reported a history of NSSI did not provide information about preferred methods.
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
References
- Akers RL. Deviant behavior: A social learning approach. 2-nd. Belmont, CA: Wadsworth; 1977. [Google Scholar]
- Aldao A, Nolen-Hoeksema S, Schweizer S. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clinical Psychology Review. 2010;30(2):217–237. doi: 10.1016/j.cpr.2009.11.004. [DOI] [PubMed] [Google Scholar]
- Anderson NL, Crowther JH. Using the experiential avoidance model of non-suicidal self-injury: Understanding who stops and who continues. Archives of Suicide Research. 2012;16(2):124–134. doi: 10.1080/13811118.2012.667329. [DOI] [PubMed] [Google Scholar]
- Armey MF, Crowther JH, Miller IW. Changes in ecological momentary assessment reported affect associated with episodes of nonsuicidal self-injury. Behavior Therapy. 2011;42(4):579–588. doi: 10.1016/j.beth.2011.01.002. [DOI] [PubMed] [Google Scholar]
- Bandura A. Social learning theory. Oxford, England: Prentice-Hall; 1977. [Google Scholar]
- Bandura A. Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, NJ: Prentice-Hall; 1986. [Google Scholar]
- Bandura A. Social cognitive theory of mass communication. Media Psychology. 2001;3(3):265–299. doi: 10.1207/S1532785XMEP0303_03. [DOI] [Google Scholar]
- Bardeen JR, Fergus TA, Orcutt HK. An examination of the latent structure of the Difficulties in Emotion Regulation Scale. Journal of Psychopathology and Behavioral Assessment. 2012;34(3):382–392. doi: 10.1007/s10862-012-9280-y. [DOI] [Google Scholar]
- Bentley KH, Nock MK, Barlow DH. The four-function model of nonsuicidal self-injury: Key directions for future research. Clinical Psychological Science. 2014;2(5):638–656. doi: 10.1177/2167702613514563. [DOI] [Google Scholar]
- Brickman LJ, Ammerman BA, Look AE, Berman ME, McCloskey MS. The relationship between non-suicidal self-injury and borderline personality disorder symptoms in a college sample. Borderline Personality Disorder and Emotion Dysregulation. 2014;1(14):1–8. doi: 10.1186/2051-6673-1-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chapman AL, Gratz KL, Brown MZ. Solving the puzzle of deliberate self-harm: The experiential avoidance model. Behaviour Research and Therapy. 2006;44(3):371–394. doi: 10.1016/j.brat.2005.03.005. [DOI] [PubMed] [Google Scholar]
- Claes L, Houben A, Vandereycken W, Bijttebier P, Muehlenkamp J. Brief report: The association between non-suicidal self-injury, self-concept and acquaintance with self-injurious peers in a sample of adolescents. Journal of Adolescence. 2010;33(5):775–778. doi: 10.1016/j.adolescence.2009.10.012. [DOI] [PubMed] [Google Scholar]
- DiLorenzo TM, Stucky-Ropp RC, Vander Wal JS, Gotham HJ. Determinants of exercise among children: II. A longitudinal analysis. Preventive Medicine: An International Journal Devoted to Practice and Theory. 1998;27(3):470–477. doi: 10.1006/pmed.1998.0307. [DOI] [PubMed] [Google Scholar]
- Fischer S, Smith GT. Binge eating, problem drinking, and pathological gambling: Linking behavior to shared traits and social learning. Personality and Individual Differences. 2008;44(4):789–800. doi: 10.1016/j.paid.2007.10.008. [DOI] [Google Scholar]
- Franklin JC, Lee KM, Hanna EK, Prinstein MJ. Feeling worse to feel better: Pain-offset relief simultaneously stimulates positive affect and reduces negative affect. Psychological Science. 2013;24(4):521–529. doi: 10.1177/0956797612458805. [DOI] [PubMed] [Google Scholar]
- Glenn CR, Klonsky ED. One-year test-retest reliability of the Inventory of Statements about Self-Injury (ISAS) Assessment. 2011;18(3):375–378. doi: 10.1177/1073191111411669. [DOI] [PubMed] [Google Scholar]
- Gould M, Jamieson P, Romer D. Media contagion and suicide among the young. American Behavioral Scientist. 2003;46(9):1269–1284. doi: 10.1177/0002764202250670. [DOI] [Google Scholar]
- Gratz KL, Roemer L. Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the Difficulties in Emotion Regulation Scale. Journal of Psychopathology and Behavioral Assessment. 2004;26(1):41–54. doi: 10.1023/B:JOBA.0000007455.08539.94. [DOI] [Google Scholar]
- Gratz KL, Roemer L. The relationship between emotion dysregulation and deliberate self-harm among female undergraduate students at an urban commuter university. Cognitive Behaviour Therapy. 2008;37(1):14–25. doi: 10.1080/16506070701819524. [DOI] [PubMed] [Google Scholar]
- Hamza CA, Willoughby T. A longitudinal person-centered examination of nonsuicidal self-injury among university students. Journal of Youth and Adolescence. 2014;43(4):671–685. doi: 10.1007/s10964-0139991-8. [DOI] [PubMed] [Google Scholar]
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics. 2009;42(2):377–381. doi: 10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hasking P, Andrews T, Martin G. The role of exposure to self-injury among peers in predicting later self-injury. Journal of Youth and Adolescence. 2013;42(10):1543–1556. doi: 10.1007/s10964-013-9931-7. [DOI] [PubMed] [Google Scholar]
- Hasking P, Rose A. A preliminary application of social cognitive theory to nonsuicidal self-injury. Journal of Youth and Adolescence. 2016;14(8):1560–1574. doi: 10.1007/s10964-016-0449-7. [DOI] [PubMed] [Google Scholar]
- Heath NL, Ross S, Toste JR, Charlebois A, Nedecheva T. Retrospective analysis of social factors and nonsuicidal self-injury among young adults. Canadian Journal of Behavioural Science/Revue Canadienne des Sciences du Comportement. 2009;41(3):180–186. doi: 10.1037/a0015732. [DOI] [Google Scholar]
- Heilbron N, Prinstein MJ. Peer influence and adolescent nonsuicidal self-injury: A theoretical review of mechanisms and moderators. Applied and Preventive Psychology. 2008;12(4):169–177. doi: 10.1016/j.appsy.2008.05.004. [DOI] [Google Scholar]
- Hilbe JM. Negative binomial regression. 2nd. Cambridge University Press; New York, NY: 2011. [DOI] [Google Scholar]
- Hilt LM, Hamm EH. Peer influences on non-suicidal self-injury and disordered eating. In: Claes L, Muehlenkamp J, editors. Non-suicidal self-injury in eating disorders. 2014. pp. 255–272. [DOI] [Google Scholar]
- Jarvi S, Jackson B, Swenson L, Crawford H. The impact of social contagion on non-suicidal self-injury: A review of the literature. Archives of Suicide Research. 2013;17(1):1–19. doi: 10.1080/13811118.2013.748404. [DOI] [PubMed] [Google Scholar]
- Klonsky ED. The functions of deliberate self-injury: A review of the evidence. Clinical Psychology Review. 2007;27(2):226–239. doi: 10.1016/j.cpr.2006.08.002. [DOI] [PubMed] [Google Scholar]
- Klonsky ED, Glenn CG. Assessing the functions of non-suicidal self-injury: Psychometric properties of the Inventory of Statements About Self-injury (ISAS) Journal of Psychopathology and Behavioral Assessment. 2009;31:215–219. doi: 10.1007/s10862-008-9107-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klonsky ED, Olino TM. Identifying clinically distinct subgroups of self-injurers among young adults: A latent class analysis. Journal of Consulting and Clinical Psychology. 2008;76(1):22–27. doi: 10.1037/0022-006X.76.1.22. [DOI] [PubMed] [Google Scholar]
- Lee DJ, Witte TK, Bardeen JR, Davis MT, Weathers FW. A factor analytic evaluation of the Difficulties in Emotion Regulation Scale. Journal of Clinical Psychology. 2016;72(9):933–946. doi: 10.1002/jclp.22297. [DOI] [PubMed] [Google Scholar]
- Levine MP, Smolak L. The mass media and disordered eating: Implications for primary prevention. In: Vandereycken W, Noordenbos G, editors. The prevention of eating disorders. New York, NY: New York University Press; 1998. pp. 23–56. [Google Scholar]
- Lewis SP, Heath NL, Michal NJ, Duggan JM. Non-suicidal self-injury, youth, and the Internet: What mental health professionals need to know. Child and Adolescent Psychiatry and Mental Health. 2012;6(13) doi: 10.1186/1753-2000-6-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis SP, Seko Y. A double‐edged sword: A review of benefits and risks of online nonsuicidal self‐injury activities. Journal of Clinical Psychology. 2016;72(3):249–262. doi: 10.1002/jclp.22242. [DOI] [PubMed] [Google Scholar]
- McKenzie KC, Gross JJ. Nonsuicidal self-injury: An emotion regulation perspective. Psychopathology. 2014;47(4):207–219. doi: 10.1159/000358097. [DOI] [PubMed] [Google Scholar]
- Muehlenkamp JJ, Hoff ER, Licht J, Azure JA, Hasenzahl SJ. Rates of non-suicidal self-injury: A cross-sectional analysis of exposure. Current Psychology: A Journal for Diverse Perspectives on Diverse Psychological Issues. 2008;27(4):234–241. doi: 10.1007/s12144-008-9036-8. [DOI] [Google Scholar]
- Nock MK. Why do people hurt themselves? New insights into the nature and functions of self-injury. Current Directions in Psychological Science. 2009;18(2):78–83. doi: 10.1111/j.1467-8721.2009.01613.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nock MK. Self-injury. Annual Review of Clinical Psychology. 2010;63:39–363. doi: 10.1146/annurev.clinpsy.121208.131258. [DOI] [PubMed] [Google Scholar]
- Nock MK, Prinstein MJ. A functional approach to the assessment of self-mutilative behavior. Journal of Consulting and Clinical Psychology. 2004;72(5):885–890. doi: 10.1037/0022-006X.72.5.885. [DOI] [PubMed] [Google Scholar]
- Nock MK, Prinstein MJ, Sterba SK. Revealing the form and function of self-injurious thoughts and behaviors: A real-time ecological assessment study among adolescents and young adults. Psychology of Violence. 2009;1:36–52. doi: 10.1037/2152-0828.1.S.36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Purington A, Whitlock J. Non-suicidal self-injury in the media. The Prevention Researcher. 2010;17(1):11–14. [Google Scholar]
- Radovic S, Hasking P. The relationship between portrayals of nonsuicidal self-injury, attitudes, knowledge, and behavior. Crisis: The Journal of Crisis Intervention and Suicide Prevention. 2013;34(5):324–334. doi: 10.1027/0227-5910/a000199. [DOI] [PubMed] [Google Scholar]
- Reid D, Weigle P. Social media use among adolescents: Benefits and risks. Adolescent Psychiatry. 2014;4(2):73–80. doi: 10.2174/221067660402140709115810. [DOI] [Google Scholar]
- Swannell SV, Martin GE, Page A, Hasking P, St John NJ. Prevalence of nonsuicidal self-injury in nonclinical samples: Systematic review, meta-analysis and meta-regression. Suicide and Life-Threatening Behavior. 2014;44(3):273–303. doi: 10.1111/sltb.12070. [DOI] [PubMed] [Google Scholar]
- Trewavas C, Hasking P, McAllister M. Representations of non-suicidal self-injury in motion pictures. Archives of Suicide Research. 2010;14(1):89–103. doi: 10.1080/13811110903479110. [DOI] [PubMed] [Google Scholar]
- Weismoore JT, Esposito-Smythers C. The role of cognitive distortion in the relationship between abuse, assault, and non-suicidal self-injury. Journal of Youth and Adolescence. 2010;39(3):281–290. doi: 10.1007/s10964-009-9452-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whitlock J, Muehlenkamp J, Purington A, Eckenrode J, Barreira P, Baral Abrams G, Marchell T, Kress V, Girard K, Chin C, Knox K. Nonsuicidal self-injury in a college population: General trends and sex differences. Journal of American College Health. 2011;59(8):691–698. doi: 10.1080/07448481.2010.529626. [DOI] [PubMed] [Google Scholar]
- Whitlock JL, Powers JL, Eckenrode J. The virtual cutting edge: The Internet and adolescent self-injury. Developmental Psychology. 2006;42(3):407–417. doi: 10.1037/0012-1649.42.3.407. [DOI] [PubMed] [Google Scholar]
- You J, Lin MP, Fu K, Leung F. The best friend and friendship group influence on adolescent nonsuicidal self-injury. Journal of Abnormal Child Psychology. 2013;41(6):993–1004. doi: 10.1007/s10802-013-9734-z. [DOI] [PubMed] [Google Scholar]
- Zeileis A, Kleiber C, Jackman S. Regression models for count data in R. Journal of Statistical Software. 2008;27(8):1–25. doi: 10.18637/jss.v027.i08. [DOI] [Google Scholar]
- Zelkowitz RL, Cole DA. Assessing media and interpersonal exposure to non-suicidal self-injury: The Social Exposure to NSSI Scale; Abstract presented at Suicide and Self-Injury Group Data Blitz, Association of Behavioral and Cognitive Therapy Annual Meeting; Philadelphia, PA. Nov, 2014. [Google Scholar]
- Zelkowitz RL, Cole DA. Measures of emotion reactivity and emotion regulation: Convergent and discriminant validity. Personality and Individual Differences. 2016;102:123–132. doi: 10.1016/j.paid.2016.06.045.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zelkowitz RL, Cole DA, Han GT, Tomarken AJ. The incremental utility of emotion regulation but not emotion reactivity in nonsuicidal self‐injury. Suicide and Life-Threatening Behavior. 2016;46(5):545–562. doi: 10.1111/sltb.12236. [DOI] [PMC free article] [PubMed] [Google Scholar]