

Abstract
Background
Millions of individuals have used illicit anabolic-androgenic steroids (AAS), but the long-term cardiovascular associations of these drugs remains incompletely understood.
Methods
Employing a cross-sectional cohort design, we recruited 140 experienced male weightlifters aged 34–54 years, comprising 86 men reporting at least 2 years of cumulative lifetime AAS use and 54 non-using men. Using transthoracic echocardiography and coronary computed tomography angiography, we assessed 3 primary outcome measures: left ventricular (LV) systolic function (left ventricular ejection fraction [LVEF]), LV diastolic function (early relaxation velocity [E´]), and coronary atherosclerosis (coronary artery plaque volume).
Results
Compared to non-users, AAS users demonstrated relatively reduced LV systolic function (mean±SD LVEF = 52±11% vs. 63±8%; P<0.001) and diastolic function (E´ = 9.3±2.4 cm/s vs. 11.1±2.0 cm/s; P<0.001). Users currently taking AAS at the time of evaluation (N = 58) showed significantly reduced LV systolic (LVEF = 49±10% vs. 58±10%; P<0.001) and diastolic function (E´ = 8.9±2.4 cm/s vs. 10.1±2.4 cm/s; P=0.035) compared to users currently off-drug (N = 28). Additionally, AAS users demonstrated higher coronary artery plaque volume then nonusers (median [interquartile range] 3 [0, 174] mL3 vs. 0 [0, 69] mL3, P = 0.012). Lifetime AAS dose was strongly associated with coronary atherosclerotic burden (increase [95% confidence interval] in rank of plaque volume for each 10-year increase in cumulative duration of AAS use: 0.60 SD units [0.16 to 1.03 SD units]; P = 0.008).
Conclusions
Long-term AAS use appears to be associated with myocardial dysfunction and accelerated coronary atherosclerosis. These forms of AAS-associated adverse cardiovascular phenotypes may represent a previously under-recognized public-health problem.
Keywords: Anabolic-androgenic steroids, cardiology, diastolic dysfunction, cardiomyopathy, atherosclerosis, men
INTRODUCTION
An estimated 2.9 to 4.0 million Americans have used supraphysiologic doses of illicit anabolic-androgenic steroids (AAS), including testosterone and its synthetic relatives, to gain muscle mass for athletics or for personal appearance.1 About 1 million of these individuals, almost all of whom are male, have developed AAS dependence, often leading to years of chronic AAS exposure.2 Illicit AAS use did not become widespread in the general American population until the 1980s.3 Thus, the oldest AAS users, who initiated AAS as youths in the 1980s, are only now reaching middle age, when the adverse effects of long-term use may become apparent. Therefore, these effects remain incompletely understood.
Prior studies have suggested an association between AAS use and cardiovascular disease, with a pathophysiologic link first proposed by early case reports of sudden cardiac death or ischemic stroke among young AAS-using men.4–6 Subsequently, pre-clinical studies have shown that AAS exposure at supraphysiologic doses causes dyslipidemia;7–9 stimulates cardiomyocyte hypertrophy;10, 11 impairs coronary arterial function;12, 13 reduces cardiac beta-adrenoreceptor sensitivity;14 potentiates oxidative cardiac stress;15 lowers arrhythmic thresholds;16 and induces myocyte apoptosis.17 Most recently, investigations utilizing non-invasive cardiac imaging in human users have demonstrated preliminary evidence of AAS cardiotoxicity in the forms of myocardial dysfunction,18–22 myocardial fibrosis,23 and increased coronary artery calcification.24
In aggregate, data from these prior studies suggest that illicit AAS use may cause a form of cardiomyopathy characterized by decreased LV function,18, 19, 21–23, 25, 26 and may increase the risk of atherosclerotic disease.1, 7, 8, 24 To date, definitive associations between AAS exposure and either myocardial or coronary artery disease have yet to be demonstrated in a large human study. To address this issue, we conducted comprehensive cardiovascular evaluations of 86 long-term AAS users and 54 non-users.
METHODS
Study Design
We conducted an observational study using a cross-sectional cohort design. We have previously presented the formal properties of this design,27 which has been used both explicitly28–31 and implicitly32, 33 in many prior studies. This method identifies a dynamic cohort of individuals, drawn from a given source population, who in principle could have been enumerated in the past and followed to the present (termed the “conceptual cohort”). Instead of sampling from the conceptual cohort, one samples in the present from those currently available (the “study cohort”). With this design, estimates of effects derived from the study cohort are valid with respect to the conceptual cohort, subject to similar conditions for validity as other retrospective designs (e.g., retrospective cohort and case-control studies).27 We chose the cross-sectional cohort design because it can efficiently assess the association of outcomes with an uncommon exposure (e.g., AAS use), in the same manner that a case-control design can efficiently assess the association of exposures with an uncommon outcome.
For the present study, we sampled from a source population of men who lift weights in gymnasiums, and then compared exposed (i.e., AAS-using) and non-exposed (i.e., non-AAS-using) men from this group. We chose this source population because almost all long-term AAS users are male2 and lift weights regularly.1, 34 We did not recruit from sporting venues, since most AAS users are not competitive athletes, but simply recreational weightlifters.1, 35, 36
Although this approach minimized the effects of confounding variables inherent to weightlifting, we considered that weightlifting or its associated lifestyle might be associated with specific cardiovascular characteristics. Therefore, in an ancillary study, we recruited a group of non-weightlifting and non-AAS-using men (frequency-matched in age to the weightlifters, but never weightlifting more than 30 minutes per week at any time since age 18), drawn from a roster of potential study volunteers maintained by Massachusetts General Hospital, and compared these non-weightlifters to the subgroup of non-AAS-using weightlifters from the primary study. These 2 groups (AAS non-users and non-weightlifting and non-AAS-using men) exhibited no scientifically important or statistically significant differences on measures of cardiovascular physiology or pathology (Supplemental Tables 1–3), indicating that weightlifting per se, of the duration and intensity selected by our recruitment techniques, was associated with little or no cardiovascular adaptation or pathology.
Participants
As described in our prior cross-sectional cohort studies involving AAS,28, 29 we advertised in gymnasiums for men age 34–54 who “could bench-press 275 pounds for at least one repetition, currently or in the past” to recruit AAS users and non-users. On telephone screening, advertisement respondents were invited to participate without inquiring about AAS use, to minimize selection bias that might arise if they knew in advance the exposure variable of interest. Notably, AAS are typically ingested in courses or “cycles,” with deliberate intervening “off-drug” intervals.1 Thus our design anticipated that the AAS-using weightlifters would include 2 subgroups, those on-drug and those off-drug, at the time of evaluation. We excluded AAS users reporting less than 2 years of cumulative lifetime AAS exposure. We imposed no specific exclusions for medical or psychiatric history.
Evaluation
Qualifying participants were evaluated at a screening interview, where they provided written informed consent for the study as approved by the McLean Hospital Institutional Review Board. We then obtained demographic data, lifetime exercise history (i.e. exercise modalities, duration, intensity, and consistency), and fat-free mass index, a validated measure of muscularity.29, 37, 38 Psychiatric and substance-use histories were obtained using the Structured Clinical Interview for DSM-IV.39 We next assessed history of AAS use, including age at onset of use; maximum weekly dose of AAS (calculated as mg of testosterone equivalent);40 cumulative lifetime years of use; lifetime dose ingested; time of most recent use; and types and doses of AAS taken during most recent (or current) use. We also assessed use of other performance-enhancing substances, including over-the-counter substances (e.g., creatine) and illicit drugs (e.g., human growth hormone, clenbuterol). Participants then provided urine samples to be tested for AAS,29, 38 and head or axillary hair to be tested for opiates, cannabis, phencyclidine, amphetamines, and cocaine.29, 38 Men showing urine or hair findings inconsistent with their reported substance-use history were excluded from further evaluation. We also excluded men denying AAS use, but exhibiting a fat-free mass index greater than 26 kg/m2 together with body fat below 10%, based on prior work showing that a combination of leanness and muscularity beyond these limits strongly suggests surreptitious AAS use.37, 41
Men found to qualify after the screening interviews were then referred for a cardiovascular evaluation, performed by investigators blinded to AAS status, to characterize LV structure, LV function, and coronary atherosclerosis. Two-dimensional transthoracic echocardiography (iE33, Philips Medical Systems, Andover, MA) was used to develop profiles of LV structure and function as previously detailed by our group.42 The primary outcome variables for LV systolic and diastolic function were left ventricular ejection fraction (LVEF) as measured using the modified bi-plane method of disks,43 and early LV relaxation velocity (E´; average of basal septum and lateral wall values44), respectively. Second, coronary computerized tomography angiography (CTA) was performed using a dual-source 128-slice CT scanner (Definition Flash, Siemens Medical Systems, Erlangen, Germany) with a primary outcome variable of total coronary artery plaque volume.45 Secondary CTA measures included number of atherosclerotic coronary segments, degree of stenosis of the worst segment, and Agatston calcium score.46 Detailed echocardiographic and CTA methods are provided in the online-only Data Supplement (Supplemental Methods).
Statistical analysis
Based on our pilot data18 and those of others,1, 24 our primary hypotheses were that AAS users would exhibit: 1) decreased LVEF, 2) decreased E´, and 3) increased coronary plaque volume compared to non-AAS-using weightlifters. We further hypothesized that within the AAS-user group, greater pathology on these variables would be associated with currency of AAS use (i.e., on-drug versus off-drug status at the time of evaluation) and with cumulative lifetime duration of AAS exposure.
Using linear regression, we estimated the mean difference between groups on the outcome measures (technically, the estimated mean difference was the estimated beta coefficient corresponding to group status in a linear model that also included a set of covariates and was fitted using ordinary least-squares linear regression). To control for confounding, our primary analysis adjusted for a set of plausible confounding variables including: age; race/ethnicity (modeled as African-American versus all others); history of tobacco use, cocaine dependence, and alcohol dependence; weekly hours of aerobic activity in the last 10 years (modeled in tertiles of the distribution); and reported family history of coronary artery disease as defined by the presence of angina, myocardial infarction, angioplasty/stent, or coronary bypass surgery in a first-degree relative. For echocardiographic measures, we additionally adjusted for body surface area as calculated by the Mosteller formula. To explore the relationship between LV mass, a potentially important mechanistic mediator of LV functional impairment, and our primary functional outcome variables, we performed post-hoc analyses examining the association of LV mass index with LVEF and E´ among AAS users and non-users. Specifically, we used linear regression with the same set of potential confounding variables and the addition of a term for AAS user versus non-user group status to examine the relationships between LV mass index (LV mass in g / body surface area in m2) and the primary cardiac function outcomes. Also, because resting heart rate could influence cardiac functional outcomes, we performed additional analyses of the primary cardiac functional outcomes by adding resting heart rate as a covariate. Note that heart rate not only may influence functional outcomes, but also might itself be affected by current AAS use. In the latter eventuality, the estimated mean difference between groups adjusted for resting heart rate would likely be biased towards the null (that is, would potentially represent an “overadjustment”), thus producing an underestimate of the effect of AAS use.
In subsequent sensitivity analyses assessing the influence of adjustments using alternative sets of potential confounders, we repeated all comparisons 1) with no adjustment for any covariates; 2) with the adjustment covariates reduced to only age and race (plus body surface area for echocardiographic measures) and 3) with the adjustment covariates augmented to include hypertension and dyslipidemia (as defined in the Supplemental Tables). Note that the augmented set of covariates would be expected to yield underestimates of the effect of AAS use, since hypertension and dyslipidemia are often effects of AAS use,1, 7, 9, 47 and adjustment for these variables would consequently “adjust out” effects of AAS mediated by these variables.
Because the distributions of coronary CTA measures contained many zero values (i.e., no measurable coronary artery disease), we used ranked data for these analyses. Within the AAS-user group, we evaluated the association of all outcome measures with duration of use and currency of use (i.e., on-drug vs. off-drug) using linear regression with adjustment for the same set of covariates. To aid in interpretation of comparisons between groups and associations within groups involving rank-transformed data, we used standard deviation (SD) units to express the estimated difference in ranks for binary predictor variables and the estimated change in ranks for each 1-unit increase in continuous predictor variables. The SD units were calculated by dividing the estimated beta coefficient for the predictor variable from the linear regression model by the SD of the ranks for the entire sample used for a given model.
All models were fitted using Stata 14.1 software (StataCorp, College Station, TX). We set α=0.05, 2-tailed. We did not perform corrections for multiple comparisons, so that the statistical significance of P-values for secondary outcomes, particularly those between 0.01 and 0.05, should be interpreted with caution.
RESULTS
Participants
Sample
We screened 165 men, of whom 25 were excluded from medical evaluation as follows: 10 qualified for participation but withdrew prior to medical evaluation (9 AAS users, 1 non-user); 12 reported AAS use of less than 2 years duration; and 3 showed findings on drug testing or fat-free mass index inconsistent with their self-reports. The remaining sample comprised 86 AAS users and 54 non-users. Among the AAS users, 58 (67%) were on-drug and 28 (33%) off-drug at evaluation. The off-drug users had last used AAS a median [interquartile range] of 15 [5, 70] months prior to evaluation.
Characteristics
AAS users and non-users were similar on most characteristics (Table 1), but users showed higher body mass index and fat-free mass index, consistent with known effects of AAS.
Table 1.
Characteristics of Anabolic-Androgenic Steroid Users and Non-Users.*
| Characteristics | AAS Users (N = 86) |
Non-Users (N = 54) |
P Value |
|---|---|---|---|
|
|
|||
| Demographic features | |||
| Age, yr | 42 (39–47) | 43 (38–49) | 0.79 |
| Race† | |||
| White | 80 (93) | 41 (76) | |
| Black | 6 (7) | 12 (22) | 0.006 |
| Asian | 0 | 1 (2) | |
| Ethnic background† | |||
| Not Hispanic | 76 (89) | 52 (96) | 0.13 |
| Hispanic | 10 (11) | 2 (4) | |
| Anthropomorphic measures | |||
| Height, m | 1.8 (1.7–1.8) | 1.8 (1.7–1.8) | 0.16 |
| Body surface area, m2‡ | 2.2 (2.1–2.3) | 2.2 (2.0–2.3) | 0.19 |
| Body mass index§ | 31 (29–33) | 29 (27–31) | < 0.001 |
| Fat-free mass index║ | 26 (24–28) | 23 (21–25) | < 0.001 |
| Exercise measures | |||
| Age at onset of regular weightlifting, yr | 16 (14–20) | 16 (15–20) | 0.97 |
| Lifetime duration of regular weightlifting, yr | 21 (15–26) | 20 (12–28) | 0.78 |
| Time spent in aerobic exercise per week# | |||
| 0–30 minutes | 30 (35) | 19 (35) | |
| 31–120 minutes | 24 (28) | 22 (41) | 0.18 |
| Greater than 120 minutes | 32 (37) | 13 (24) | |
| Other potential cardiovascular risk factors | |||
| Family history of coronary artery disease** | 25 (29) | 12 (22) | 0.37 |
| Lifetime history of substance use | |||
| Regular cigarette smoking†† | 27 (31) | 19 (35) | 0.64 |
| Alcohol dependence‡‡ | 12 (14) | 7 (13) | 0.87 |
| Cocaine dependence‡‡ | 13 (15) | 5 (9) | 0.31 |
| AAS use | |||
| Age at onset of AAS use, yr | 23 (19–30) | — | |
| Cumulative lifetime total duration of AAS use, yr | 7.4 (4.0–11.6) | — | |
| Cumulative lifetime dose of AAS, grams | 366 (166–608) | — | |
Data are reported as median (IQR) or n (%) as appropriate. P values were obtained from a Wilcoxon rank sum test or Fisher’s exact test. AAS indicates anabolic-androgenic steroids
Race and ethnic background were self-reported.
By Mosteller formula.
The body mass index is the weight in kilograms divided by the square of the height in meters.
The fat-free mass index is calculated as: (W(1-BF)/H2) + 6.1(1.8-H), where W = weight in kilograms, H = height in meters, and BF = percent body fat.37
Any self-reported aerobic exercise beyond ordinary daily activities.
At least one first-degree relative reported to have had "coronary artery disease, angina, heart attack, angioplasty/stent, or coronary artery bypass surgery."
Any cigarette smoking beyond brief experimentation.
By the Structured Clinical Interview for DSM-IV.39
Cardiometabolic features
Compared to non-users, AAS users displayed higher blood pressure (mean±SD systolic, 118±11 vs. 115±10 mmHg; diastolic, 76±9 vs. 72±9 mmHg) and a higher prevalence of dyslipidemia (N [%] with low-density lipoprotein cholesterol >160 mg/dL: 20 [23%] vs. 7 [13%]).
Cardiac structure and function
For the primary outcome variables of LVEF and E´, AAS users showed significant deficits compared to non-users (Table 2). In models further adjusted for resting heart rate, the estimated mean differences between groups were reduced by 15%, and this change had no impact on the statistical significance of these findings (P<0.001 for both). On other measures, AAS users exhibited higher LV mass index, thicker LV walls, and more concentric LV geometry than non-users. On subsequent analyses examining the association of outcomes with duration and currency of AAS use, currency of use was strongly associated with greater pathology (Figure 1 and Supplemental Table 4). Specifically, 41 (71%) of the 58 on-drug users showed LVEFs falling below the normal threshold of 52%,43 whereas off-drug users showed largely normal LVEFs. Twenty-nine (50%) on-drug users fell below the normal E´ threshold of 8.5 cm/s,44 with off-drug users showing only partially normalized E´. Similar associations with currency of AAS use were found across other echocardiographic measures (Supplemental Table 4). In contrast, we found no significant associations between duration of AAS use and the primary outcome variables (for each additional 10 years of AAS exposure, the estimated mean change [95% CI] in LVEF was −3.3% [−8.3% to 1.6%], P=0.19; and the estimated mean change in E´ was 0.1 cm/s [−1.0 to 1.2 cm/s], P=0.90).
Table 2.
Echocardiographic Findings in Anabolic-Androgenic Steroid Users and Non-Users.*
| Variable | Comparison
|
|||
|---|---|---|---|---|
| AAS Users | Non-Users | Estimated difference (95% CI) † |
P value | |
|
| ||||
| (N = 86) | (N = 54) | |||
| Primary outcomes | ||||
| Left ventricular ejection fraction, % | 52±11 | 63±8 | −10 (−14 to −7) | <0.001 |
| Average early left ventricular relaxation velocity (E´), cm/s | 9.3±2.4 | 11.1±2.0 | −1.9 (−2.7 to −1.0) | <0.001 |
| Secondary outcomes | ||||
| Resting heart rate, beats/min | 65±5 | 62±6 | 2.7 (0.7 to 4.7) | 0.008 |
| Left atrial diameter, cm‡ | 3.6±0.5 | 3.5±0.5 | 0.1 (−0.1 to 0.2) | 0.42 |
| Longitudinal 4-chamber strain§ | −16±4 | −20±3 | 4.6 (3.2 to 6.0) | <0.001 |
| Early lateral ventricular relaxation velocity (E´), cm/s | 10.6±3.1 | 12.5±2.3 | −1.8 (−2.9 to −0.8) | <0.001 |
| Early septal ventricular relaxation velocity (E´), cm/s | 8.0±2.2 | 9.8±2.1 | −1.9 (−2.7 to −1.1) | <0.001 |
| Left ventricular end diastolic internal diameter, cm | 5.0±0.6 | 4.8±0.5 | 0.1 (−0.1 to 0.3) | 0.30 |
| Left ventricular end systolic internal diameter, cm‡ | 3.6±0.7 | 3.2±0.5 | 0.3 (0.0 to 0.5) | 0.018 |
| Left ventricular end diastolic volume, mL | 125±38 | 119±28 | −0.5 (−13 to 12) | 0.94 |
| Left ventricular end systolic volume, mL | 61±27 | 45±15 | 13 (5 to 21) | 0.003 |
| Interventricular septum thickness, cm | 1.2±0.2 | 1.1±0.1 | 0.2 (0.1 to 0.2) | <0.001 |
| Posterior wall thickness, cm | 1.2±0.2 | 1.1±0.2 | 0.1 (0.0 to 0.2) | 0.003 |
| Left ventricular mass, g | 245±62 | 192±40 | 44 (24 to 63) | <0.001 |
| Left ventricular mass/body surface area, g/m2 | 111±61 | 89±18 | 21 (11 to 30) | < 0.001 |
| Left ventricular mass/height, g/m | 138±33 | 107±22 | 27 (16 to 38) | <0.001 |
| Left ventricular mass/height2.7, g/m2.7 | 52±13 | 40±8 | 11 (7 to 16) | <0.001 |
| Relative wall thickness | 0.49±0.11 | 0.45±0.08 | 0.050 (0.014 to 0.087) | 0.007 |
Data are reported as means±SD. AAS indicates anabolic-androgenic steroids; CI, confidence interval.
Estimated mean differences between groups, adjusted for age, race, family history of coronary artery disease, cocaine dependence, regular tobacco use, alcohol dependence, aerobic exercise in the past 10 years, and body surface area by the Mosteller formula.
N = 85 AAS users
N = 84 AAS users
Figure 1. Left Ventricular Systolic and Diastolic Function in Anabolic-Androgenic Steroid Users and Comparison Non-Users.
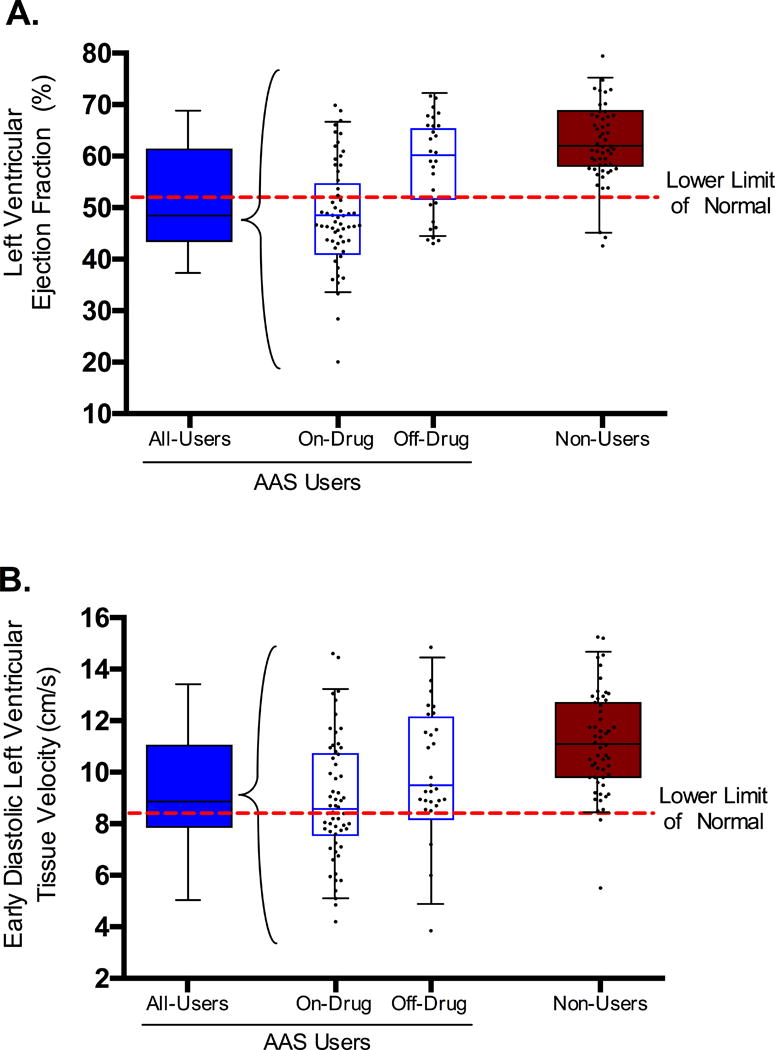
Panel A shows boxplots of left ventricular ejection fraction in anabolic-androgenic steroid (AAS) users (N=86), shown as an entire group (left side of figure) and as subgroups of individuals who were on-drug (N=58) and off-drug (N=28) at the time of evaluation (middle of figure). Non-users (N=54) appear on the right. On this variable, the estimated mean difference (95% confidence interval) between on-drug AAS users and off-drug AAS users, adjusted for covariates as described in the text, is −9.5% (−13.8% to −5.2%); P<0.001; for on-drug AAS users versus non-users, the difference is −13.6% (−17.3% to −9.8%); P<0.001; and for off-drug AAS users versus non-users, the difference is −4.1% (−8.6% to 0.3%); P=0.072. Panel B shows left ventricular early relaxation velocity in the same 4 groups. On this variable, the mean difference between on-drug AAS users and off-drug AAS users is −1.1 (−2.1 to −0.1) cm/s, P=0.035; for on-drug AAS users versus non-users, the difference is −2.2 (−3.1 to −1.4) cm/s, P<0.001; and for off-drug AAS users versus non-users, the difference is −1.1 (−2.2 to −0.1) cm/s; P=0.035.
Since LVEF and E´ differed by group (i.e., AAS user vs. non-user) and by subgroup based on currency of use (i.e., current vs. past AAS users), we further tested for interactions of group and subgroup status with LV mass index for each of these associations and found evidence for a significant interaction with AAS user group status (P=0.046 and P=0.016 for LVEF and E´, respectively), but not for currency of use among AAS users (P=0.21 and P=0.86, respectively). Therefore we assessed the associations separately for AAS users and non-users. Examining LVEF, among AAS users, there was a significant association between increased LV mass index and decreased LVEF (estimated mean change [95% CI] in LVEF for each 10 g increase in LV mass index −1.6% [−2.4 to −0.8%], P<0.001). In contrast, among the non-users, there was no significant association between LV mass index and LVEF (estimated mean change in LVEF for each 10 g increase in LV mass index –0.2% [–1.5 to 1.2%], P=0.80). Examining E´, among AAS users, there was a significant association between increased LV mass index and reduced E´ (estimated mean change in E´ for each 10 g increase in LV mass index −0.31 cm/s [−0.49 to −0.13 cm/s], P<0.001). Among non-users, the relationship was of approximately equal magnitude, but in the opposite direction, with a significant association between increased LV mass index and increased E´ (estimated mean change in E´ for each 10 g increase in LV mass index 0.36 cm/s [0.04 to 0.68 cm/s], P<0.001).
Coronary artery atherosclerosis
AAS users showed significantly higher coronary plaque volume than non-users (Table 3 and Figure 2). Upon examining the association of CTA measures with currency and duration of AAS use, we found strong associations between lifetime duration of use on all angiographic measures of coronary pathology (Table 4 and Figure 3). However, we found no significant association between currency of use and plaque volume (estimated mean difference between on-drug and off-drug users in ranks: −0.07 SD units [−0.56 to 0.41]; P=0.76). Notably, 3 (3%) AAS users had experienced prior myocardial infarctions due to underlying atherosclerotic disease, documented by cardiac catheterization, occurring at ages 38 (ST-segment myocardial infarction with complete occlusion of left anterior descending artery), 43 (Non ST-segment myocardial infarction with 99% occlusion of both the right coronary and left circumflex coronary arteries), and 46 (ST-elevation myocardial infarction with complete occlusion of a 2nd obtuse marginal artery), and after 17, 11, and 5 years of cumulative lifetime AAS exposure, respectively. In addition, one AAS user had presented at age 42, after 20 years of cumulative lifetime AAS exposure, with congestive heart failure and underwent stenting of the left circumflex and 1st obtuse marginal arteries. None of the 54 non-users had a history of myocardial infarction or stenting.
Table 3.
Computed Tomography Coronary Angiography Findings in Anabolic-Androgenic Steroid Users and Non-Users.*
|
|
Comparison
|
|||
|---|---|---|---|---|
| AAS Users (N = 84) |
Non-Users (N = 53) |
Estimated difference in standardized ranks (95% CI) † |
P Value |
|
|
|
||||
| Variable | ||||
| Primary outcome | ||||
| Plaque volume, mm3 ‡ | 3 (0–174) | 0 (0–69) | 0.46 (0.10 to 0.82) | 0.012 |
| Secondary outcomes | ||||
| Degree of stenosis for most severe stenosis§ | 0.5 (0–1) | 0.5 (0–1) | 0.37 (−0.00 to 0.75) | 0.052 |
| Number of diseased coronary artery segments║ | 0.5 (0–2) | 1 (0–1) | 0.36 (−0.01 to 0.74) | 0.059 |
| Agatston calcium score‡ | 0 (0–25) | 0 (0–1) | 0.18 (−0.17 to 0.52) | 0.31 |
Data are shown as median (IQR). AAS indicates anabolic-androgenic steroids, CI, confidence interval.
Estimated mean difference between groups in rank, measured in standard deviation units, adjusted for age, race, family history of coronary artery disease, cocaine dependence, alcohol dependence, tobacco use, and aerobic exercise in the past 10 years (see text).
Four AAS users had received percutaneous coronary interventions, and thus their plaque volume and calcium score could not be quantified accurately. However, all 4 men showed extensive plaque as evidenced by their number of diseased segments and degree of stenosis for most severe stenosis. Therefore, for purposes of calculation, they were assigned the median values for plaque volume and calcium score, respectively, from among all study participants with nonzero plaque volume and calcium scores. If these cases were omitted entirely, the estimated mean difference (95% CI) between groups in standardized rank would be 0.43 (0.04 to 0.81) for plaque volume and 0.13 (−0.26 to 0.51) for calcium score.
Represents the worst degree of stenosis of any coronary artery, on a scale of 0–4, where 0 = 0% stenosis; 1 = 1–25%; 2 = 26–49%; 3 = 50–69%; and 4 = 70–99%.
Represents the number of coronary artery segments showing any disease, with scores ranging from 0 to 10 diseased segments.
Figure 2. Distribution of Computed Tomography Coronary Angiography Measures in Anabolic-Androgenic Steroid Users and Non-Users.
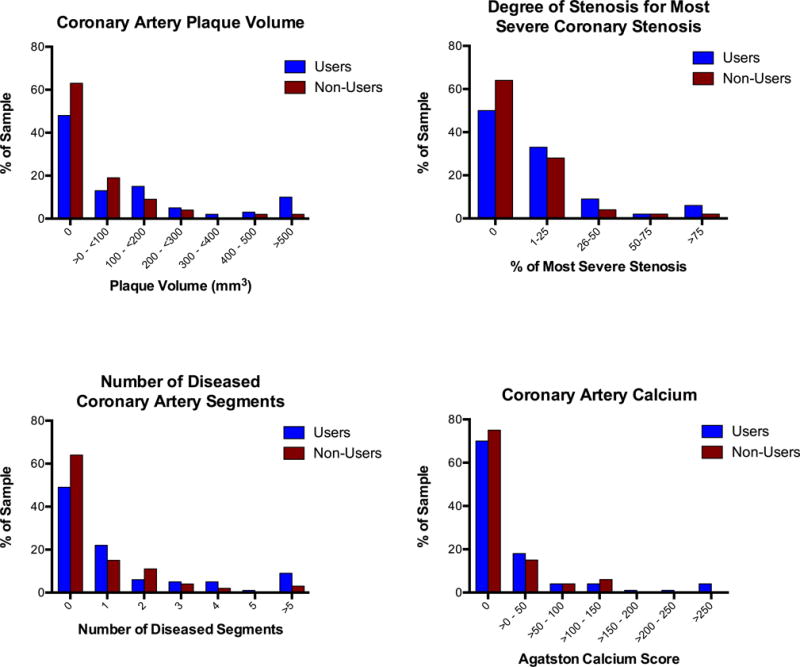
Histograms displaying distribution of coronary artery plaque volume, degree of stenosis for most severe stenosis, number of diseased coronary artery segments, and coronary artery calcium for anabolic-androgenic steroid (AAS) users (N=84) and non-users (N=53). Note that the histograms for plaque volume and calcium score include for men with imputed values, as described in the footnote to Table 3.
Table 4.
Association of Computed Tomography Coronary Angiography Variables with Lifetime Duration of Anabolic-Androgenic Steroid Use.*
| Variable | Increase in standardized rank per 10-yr increase in duration of lifetime AAS use (95% CI) † |
P Value |
|---|---|---|
| Primary outcome | ||
| Plaque volume, mm3‡ | 0.60 (0.16 to 1.03) | 0.008 |
| Secondary outcomes | ||
| Degree of stenosis for most severe stenosis§ | 0.68 (0.26 to 1.10) | 0.002 |
| Number of diseased coronary artery segments║ | 0.75 (0.31 to 1.19) | < 0.001 |
| Agatston calcium score‡ | 0.49 (0.06 to 0.92) | 0.025 |
AAS indicates anabolic-androgenic steroids; CI, confidence interval.
Represents the estimated increase in rank, measured in standard deviation units, for each 10-year increase in cumulative lifetime duration of AAS use, adjusted for age, race, family history of coronary artery disease, cocaine dependence, alcohol dependence, tobacco use, and aerobic exercise in the past 10 years (see text).
Four AAS users had received prior percutaneous coronary interventions, and thus their plaque volume and calcium scores could not be measured accurately. However, all 4 of these men exhibited extensive plaque as evidenced by their number of diseased segments and degree of stenosis for most severe stenosis. Therefore, for purposes of calculation, they were assigned the median values for plaque volume and calcium score, respectively, from among all study participants with nonzero plaque volume and calcium scores. If these cases were omitted entirely, the increase (95% CI) in standardized rank per 10 years of AAS exposure would be 0.61 (0.11 to 1.12) for plaque volume and 0.48 (−0.04 to 0.99) for calcium score.
Represents the worst degree of stenosis of any coronary artery, on a scale of 0–4, where 0 = 0% stenosis; 1 = 1–25%; 2 = 26–49%; 3 = 50–69%; and 4 = 70–99%.
Represents the number of coronary artery segments showing any disease, with scores ranging from 0 to 10 diseased segments.
Figure 3. Relationship between Coronary Artery Plaque Volume and Cumulative Lifetime Duration of Anabolic-Androgenic Steroid Exposure.
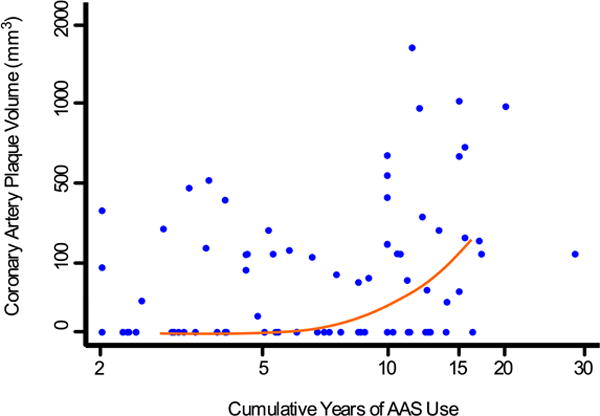
Scatter plot displaying coronary artery plaque volume and cumulative years of lifetime anabolic-androgenic steroid (AAS) exposure, with a median spline (red line) fitted to the data to aid in the visualization of the relationship between these variables. Because of the highly right-skewed distributions, the data are presented on a transformed scale (square root transformation for coronary artery plaque volume; logarithmic transformation for cumulative years of AAS use).
Sensitivity analyses
Assessing the influence of alternative sets of potential confounders, using models with both reduced and augmented sets of covariates, we obtained results similar to those of the primary analysis, with less than 15% change in the estimates for the primary outcomes and preservation of statistical significance for all results identified as such in the primary analysis (Supplemental Tables 5–7). We also reanalyzed the echocardiographic findings while omitting the three men with prior myocardial infarctions. This analysis produced negligible changes in the findings, with the estimated mean differences between users and nonusers on the two primary outcome variables changing by less than 2% when these three men were excluded.
DISCUSSION
Illicit AAS use is widespread, but its long-term adverse effects remain poorly understood. A growing literature, largely comprised of case reports and small observational studies, suggests that AAS use may cause cardiovascular disease. We undertook the present study to examine cardiovascular health measures among long-term AAS users and otherwise similar non-users with the following four key findings. First, AAS users demonstrated substantial impairment of LV systolic function, as assessed by LVEF and longitudinal strain. This finding was driven almost entirely by those AAS users who were on-drug at the time of evaluation, suggesting that LV dysfunction may be a dynamically related to AAS-use patterns. Second, AAS users also showed impaired LV diastolic dysfunction, both relative to non-users and also as defined by current diagnostic criteria.44 In contrast to systolic function, which appeared largely normal among off-drug AAS users, LV diastolic function was impaired both in on-drug and off-drug users, suggesting a more permanent form of acquired pathology. Third, AAS users had significantly more LV hypertrophy, as reflected by LV mass index, than non-users, suggesting an anabolic effect on cardiac muscle mass. In addition, the magnitude of LV hypertrophy among AAS users was directly related to the degrees of both systolic and diastolic function, suggesting a mechanistic link between LV hypertrophy and functional deterioration. Fourth, AAS use was associated with increased coronary atherosclerosis, and the severity of atherosclerotic disease was strongly associated with cumulative lifetime duration of AAS use. In aggregate, our findings suggest that long-term AAS use is associated with adverse cardiovascular phenotypes characterized by both myocardial pathology and coronary artery pathology, that may represent a clinically substantial and largely unrecognized public health problem.
Several scientific and clinical implications emerge from this study. First, improved identification of the adverse cardiovascular associations of AAS use may deter potential future users. Second, clinicians may be better informed about the potential adverse cardiovascular effects of AAS. Importantly, participants in the current study were not elite or professional athletes, the small subset of the general population most commonly tied to AAS exposure, but rather a sample of middle-aged men representing a reasonably broad socioeconomic and racial/ethnic distribution. Thus, when comparable men are found to have impaired LV function or premature coronary artery disease, it seems prudent for clinicians to now include AAS use on the differential diagnosis of possible causes. Third, data derived from the present cross-sectional study provide a foundation for critical future work. The hypothesis that some cardiovascular phenotypes associated with AAS use may wax and wane with drug exposure (e.g., LV systolic dysfunction) while others may be more permanent, perhaps irreversible (e.g., LV diastolic dysfunction and coronary atherosclerosis), deserves rigorous assessment. Longitudinal studies of illicit AAS users with hard clinical endpoints, and with interventions to impact drug exposure patterns and treat detected disease, are also of importance.
Limitations
Several threats regarding the internal validity of this study, as previously delineated in general for cross-sectional cohort studies,27, 29 deserve consideration. First, bias might arise through exiting from the underlying conceptual cohort (that is, becoming unavailable for study in the present) that is differential with respect to exposure status. For example, AAS users might be more likely than non-users to develop cardiovascular morbidity, stop weightlifting, and hence be unavailable for recruitment. Any resulting bias, however, would likely underestimate the effects of AAS use. Second, as in all observational studies, we cannot exclude residual confounding. However, given the lack of confounding seen with our measured potential confounders—as evidenced by similar estimates in sensitivity analyses using both reduced and augmented sets of potential confounders—it is unlikely that there remains substantial residual bias due unmeasured confounders. Third, because both AAS users and non-users were weightlifters, the effects of AAS might be clouded if weightlifting contributed to cardiovascular pathology. However, our ancillary study comparing non-AAS-using weightlifters with non-weightlifters demonstrated that weightlifting alone (of the duration and intensity exhibited by our sample) had little effect on cardiac adaptation or pathology. Fourth, bias could arise from measurement error, particularly in the exposure variables (e.g., misclassifying surreptitious AAS users as non-users or inaccurately assessing the type, duration, dose, and currency of use). In particular, AAS users provided retrospective accounts, often spanning many years of time, of the use of illicit drugs of uncertain potency or authenticity. As such, estimates of participants’ lifetime duration of AAS use and total lifetime AAS dose were only approximations. The effect of these various sources of measurement error would be expected to be differential for between-group comparisons (due to the potential for inclusion of surreptitious AAS users in the non-user group, and the much less likely inclusion of individuals falsely reporting AAS use in the user group) and random for within-group comparisons among AAS users (due to the low likelihood of an association between cardiac outcomes and error in the predictor variables). Both of these sources would likely bias results towards the null, thereby yielding an underestimate of the effects of AAS use.
Potential threats to external validity (generalizability) also require consideration. First, we recruited AAS users from gymnasiums. Thus our results might not generalize to other AAS-using groups (e.g., elite athletes). However, most AAS users are recreational weightlifters, and thus our results likely generalize to the population of AAS users of greatest public health importance. Second, despite the demographic diversity of our sample, white non-Hispanic men were overrepresented, and therefore our results might not generalize to the full racial/ethnic spectrum of AAS users. Overall, however, these potential threats to internal and external validity appear modest. Thus, our findings likely represent reasonably unbiased estimates of the associations of AAS exposure with adverse cardiovascular phenotypes.
Conclusions
Our findings suggest that AAS use is associated with LV dysfunction and premature coronary artery disease. These findings may inform public health initiatives to curb drug exposure and provide clinicians with information that will translate into improved patient care.
Supplementary Material
Clinical Perspective.
What is new?
Millions of individuals have used anabolic-androgenic steroids (AAS) to gain muscle for athletic purposes or for personal appearance.
Preliminary findings have suggested that long-term AAS exposure may lead to both cardiomyopathy and atherosclerotic disease, but prior studies have been small or methodologically limited.
Here, in the first large controlled study of its type, we demonstrate that long-term AAS use is associated with both systolic and diastolic myocardial dysfunction, as well as coronary atherosclerosis.
Although systolic functional deficits appear to recover following AAS discontinuation, diastolic dysfunction appears less reversible.
Atherosclerotic disease appears strongly associated with lifetime duration of AAS exposure.
What are the clinical implications?
Widespread illicit AAS use first appeared in the general population in the 1980s, and thus most AAS users are still young or middle-aged today.
Thus, when clinicians encounter young or middle-aged men who exhibit evidence of unexplained left ventricular dysfunction or premature coronary artery disease, the possibility of cardiotoxicity due to long-term AAS use should be considered in the differential diagnosis.
Notably, about 80% of contemporary AAS users are simply recreational weightlifters rather than competitive athletes, and thus the possibility of AAS use should be considered even in individuals who do not identify themselves as athletes.
Acknowledgments
None
SOURCES OF FUNDING
This study was supported by a grant from the National Institute on Drug Abuse (to Drs Pope, Kanayama, Hudson, Baggish, Weiner, and Hoffmann).
Drs Pope, Kanayama, Hudson, Baggish, Weiner, and Hoffmann have received grant support for this study from the National Institute on Drug Abuse. Dr Hoffmann has received grants from HeartFlow and KOWA. Dr Pope has received expert witness fees for cases involving anabolic-androgenic steroids from the McNeil, Leddy & Sheahan Law Firm and the US District Attorney for Eastern New York.
Footnotes
CONFLICT OF INTEREST DISCLOSURES
Drs Kanayama and Weiner report no additional conflicts of interest. Dr Lu reports no conflicts of interest.
References
- 1.Pope HG, Wood R, Rogol A, Nyberg F, Bowers L, Bhasin S. Adverse health consequences of performance-enhancing drugs: an Endocrine Society scientific statement. Endocr Rev. 2014;35:341–375. doi: 10.1210/er.2013-1058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pope HG, Kanayama G, Athey A, Ryan E, Hudson JI, Baggish A. The lifetime prevalence of anabolic-androgenic steroid use and dependence in Americans: current best estimates. Am J Addict. 2014;23:371–377. doi: 10.1111/j.1521-0391.2013.12118.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kanayama G, Hudson JI, Pope HG., Jr Long-term psychiatric and medical consequences of anabolic-androgenic steroid abuse: a looming public health concern? Drug Alcohol Depend. 2008;98:1–12. doi: 10.1016/j.drugalcdep.2008.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.McNutt RA, Ferenchick GS, Kirlin PC, Hamlin NJ. Acute myocardial infarction in a 22-year-old world class weight lifter using anabolic steroids. Am J Cardiol. 1988;62:164. doi: 10.1016/0002-9149(88)91390-2. [DOI] [PubMed] [Google Scholar]
- 5.Bowman S. Anabolic steroids and infarction. BMJ. 1990;300:750. doi: 10.1136/bmj.300.6726.750-c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ferenchick GS, Adelman S. Myocardial infarction associated with anabolic steroid use in a previously healthy 37-year-old weight lifter. Am Heart J. 1992;124:507–508. doi: 10.1016/0002-8703(92)90620-b. [DOI] [PubMed] [Google Scholar]
- 7.Garevik N, Strahm E, Garle M, Lundmark J, Stahle L, Ekstrom L, Rane A. Long term perturbation of endocrine parameters and cholesterol metabolism after discontinued abuseexposure of anabolic androgenic steroids. Journal Steroid Biochem Molec Biol. 2011;127:295–300. doi: 10.1016/j.jsbmb.2011.08.005. [DOI] [PubMed] [Google Scholar]
- 8.Hartgens F, Kuipers H. Effects of androgenic-anabolic steroids in athletes. NZ Sports Med. 2004;34:513–554. doi: 10.2165/00007256-200434080-00003. [DOI] [PubMed] [Google Scholar]
- 9.Thompson PD, Cullinane EM, Sady SP, Chenevert C, Saritelli AL, Sady MA, Herbert PN. Contrasting effects of testosterone and stanozolol on serum lipoprotein levels. JAMA. 1989;261:1165–1168. [PubMed] [Google Scholar]
- 10.Cabral AM, Vasquez EC, Moyses MR, Antonio A. Sex hormone modulation of ventricular hypertrophy in sinoaortic denervated rats. Hypertension. 1988;11:I93–97. doi: 10.1161/01.hyp.11.2_pt_2.i93. [DOI] [PubMed] [Google Scholar]
- 11.Malhotra A, Buttrick P, Scheuer J. Effects of sex hormones on development of physiological and pathological cardiac hypertrophy in male and female rats. The Am J Physiol. 1990;259:H866–871. doi: 10.1152/ajpheart.1990.259.3.H866. [DOI] [PubMed] [Google Scholar]
- 12.Tagarakis CV, Bloch W, Hartmann G, Hollmann W, Addicks K. Anabolic steroids impair the exercise-induced growth of the cardiac capillary bed. Int J Sports Med. 2000;21:412–418. doi: 10.1055/s-2000-3835. [DOI] [PubMed] [Google Scholar]
- 13.Tagarakis CV, Bloch W, Hartmann G, Hollmann W, Addicks K. Testosterone-propionate impairs the response of the cardiac capillary bed to exercise. Med Sci Sports Exerc. 2000;32:946–953. doi: 10.1097/00005768-200005000-00011. [DOI] [PubMed] [Google Scholar]
- 14.Norton GR, Trifunovic B, Woodiwiss AJ. Attenuated beta-adrenoceptor-mediated cardiac contractile responses following androgenic steroid administration to sedentary rats. Eur J Appl Physiol. 2000;81:310–316. doi: 10.1007/s004210050048. [DOI] [PubMed] [Google Scholar]
- 15.Frankenfeld SP, Oliveira LP, Ortenzi VH, Rego-Monteiro IC, Chaves EA, Ferreira AC, Leitao AC, Carvalho DP, Fortunato RS. The anabolic androgenic steroid nandrolone decanoate disrupts redox homeostasis in liver, heart and kidney of male Wistar rats. PloS One. 2014;9:e102699. doi: 10.1371/journal.pone.0102699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Medei E, Marocolo M, Rodrigues Dde C, Arantes PC, Takiya CM, Silva J, Rondinelli E, Goldenberg RC, de Carvalho AC, Nascimento JH. Chronic treatment with anabolic steroids induces ventricular repolarization disturbances: cellular, ionic and molecular mechanism. J Mol Cell Cardiol. 2010;49:165–175. doi: 10.1016/j.yjmcc.2010.04.014. [DOI] [PubMed] [Google Scholar]
- 17.Zaugg M, Jamali NZ, Lucchinetti E, Xu W, Alam M, Shafiq SA, Siddiqui MA. Anabolic-androgenic steroids induce apoptotic cell death in adult rat ventricular myocytes. J Cell Physiol. 2001;187:90–95. doi: 10.1002/1097-4652(2001)9999:9999<00::AID-JCP1057>3.0.CO;2-Y. [DOI] [PubMed] [Google Scholar]
- 18.Baggish AL, Weiner RB, Kanayama G, Hudson JI, Picard MH, Hutter AM, Jr, Pope HG., Jr Long term anabolic androgenic steroid use is associated with left ventricular dysfunction. Circ Heart Fail. 2010;3:472–476. doi: 10.1161/CIRCHEARTFAILURE.109.931063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.D’Andrea A, Caso P, Salerno G, Scarafile R, De Corato G, Mita C, Di Salvo G, Severino S, Cuomo S, Liccardo B, Esposito N, Calabro R, Giada F. Left ventricular early myocardial dysfunction after chronic misuse of anabolic androgenic steroids: a Doppler myocardial and strain imaging analysis. Br J Sports Med. 2007;41:149–155. doi: 10.1136/bjsm.2006.030171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Krieg A, Scharhag J, Albers T, Kindermann W, Urhausen A. Cardiac tissue Doppler in steroid users. Int J Sports Med. 2007;28:638–643. doi: 10.1055/s-2007-964848. [DOI] [PubMed] [Google Scholar]
- 21.Luijkx T, Velthuis BK, Backx FJ, Buckens CF, Prakken NH, Rienks R, Mali WP, Cramer MJ. Anabolic androgenic steroid use is associated with ventricular dysfunction on cardiac MRI in strength trained athletes. IntJ Cardiol. 2013;167:664–668. doi: 10.1016/j.ijcard.2012.03.072. [DOI] [PubMed] [Google Scholar]
- 22.Nottin S, Nguyen LD, Terbah M, Obert P. Cardiovascular effects of androgenic anabolic steroids in male bodybuilders determined by tissue Doppler imaging. Am J Cardiol. 2006;97:912–915. doi: 10.1016/j.amjcard.2005.10.026. [DOI] [PubMed] [Google Scholar]
- 23.Angell PJ, Ismail TF, Jabbour A, Smith G, Dahl A, Wage R, Whyte G, Green DJ, Prasad S, George K. Ventricular structure, function, and focal fibrosis in anabolic steroid users: a CMR study. Eur J Appl Physiol. 2015;114:921–928. doi: 10.1007/s00421-014-2820-2. [DOI] [PubMed] [Google Scholar]
- 24.Santora LJ, Marin J, Vangrow J, Minegar C, Robinson M, Mora J, Friede G. Coronary calcification in body builders using anabolic steroids. Prev Cardiol. 2006;9:198–201. doi: 10.1111/j.1559-4564.2006.05210.x. [DOI] [PubMed] [Google Scholar]
- 25.Hassan NA, Salem MF, Sayed MA. Doping and effects of anabolic androgenic steroids on the heart: histological, ultrastructural, and echocardiographic assessment in strength athletes. Hum Exper Toxicol. 2009;28:273–283. doi: 10.1177/0960327109104821. [DOI] [PubMed] [Google Scholar]
- 26.Kasikcioglu E, Oflaz H, Umman B, Bugra Z. Androgenic anabolic steroids also impair right ventricular function. Int J Cardiol. 2009;134:123–125. doi: 10.1016/j.ijcard.2007.12.027. [DOI] [PubMed] [Google Scholar]
- 27.Hudson JI, Pope HG, Jr, Glynn RJ. The cross-sectional cohort study: an underutilized design. Epidemiology. 2005;16:355–359. doi: 10.1097/01.ede.0000158224.50593.e3. [DOI] [PubMed] [Google Scholar]
- 28.Kanayama G, DeLuca J, Meehan WP, 3rd, Hudson JI, Isaacs S, Baggish A, Weiner R, Micheli L, Pope HG., Jr ruptured tendons in anabolic-androgenic steroid users: a cross-sectional cohort study. Am J Sports Med. 2015;43:2638–2644. doi: 10.1177/0363546515602010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Pope H, Kanayama G, Hudson J. Risk factors for illicit anabolic-androgenic steroid use in male weightlifters: A cross-sectional cohort study. Biol Psychiatry. 2012;71:254–261. doi: 10.1016/j.biopsych.2011.06.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Arnold B, Arana B, Mausezahl D, Hubbard A, Colford JM., Jr Evaluation of a pre-existing, 3-year household water treatment and handwashing intervention in rural Guatemala. Int J Epidemiol. 2009;38:1651–1661. doi: 10.1093/ije/dyp241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ljungman C, Kahan T, Schioler L, Hjerpe P, Wettermark B, Bostrom KB, Manhem K. Antihypertensive treatment and control according to gender, education, country of birth and psychiatric disorder: the Swedish Primary Care Cardiovascular Database (SPCCD) J Hum Hypertens. 2015;29:385–393. doi: 10.1038/jhh.2014.100. [DOI] [PubMed] [Google Scholar]
- 32.Kessler RC, Borges G, Walters EE. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Arch Gen Psychiatry. 1999;56:617–626. doi: 10.1001/archpsyc.56.7.617. [DOI] [PubMed] [Google Scholar]
- 33.Whitlock G, Norton R, Clark T, Pledger M, Jackson R, MacMahon S. Motor vehicle driver injury and socioeconomic status: a cohort study with prospective and retrospective driver injuries. J Epidemiol Commity Health. 2003;57:512–516. doi: 10.1136/jech.57.7.512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Bahrke MS, Yesalis CE, Kopstein AN, Stephens JA. Risk factors associated with anabolic-androgenic steroid use among adolescents. Sports Medicine (Auckland, NZ. 2000;29:397–405. doi: 10.2165/00007256-200029060-00003. [DOI] [PubMed] [Google Scholar]
- 35.Ip EJ, Barnett MJ, Tenerowicz MJ, Perry PJ. The Anabolic 500 survey: characteristics of male users versus nonusers of anabolic-androgenic steroids for strength training. Pharmacotherapy. 2011;31:757–766. doi: 10.1592/phco.31.8.757. [DOI] [PubMed] [Google Scholar]
- 36.Parkinson AB, Evans NA. Anabolic androgenic steroids: a survey of 500 users. Med Sci Sports Exerc. 2006;38:644–651. doi: 10.1249/01.mss.0000210194.56834.5d. [DOI] [PubMed] [Google Scholar]
- 37.Kouri EM, Pope HG, Jr, Katz DL, Oliva P. Fat-free mass index in users and nonusers of anabolic-androgenic steroids. Clin J Sport Med. 1995;5:223–228. doi: 10.1097/00042752-199510000-00003. [DOI] [PubMed] [Google Scholar]
- 38.Kanayama G, Pope HG, Cohane G, Hudson JI. Risk factors for anabolic-androgenic steroid use among weightlifters: a case-control study. Drug Alcohol Depend. 2003;71:77–86. doi: 10.1016/s0376-8716(03)00069-3. [DOI] [PubMed] [Google Scholar]
- 39.First M, Spitzer R, Gibbon M, Williams J. Structured Clinical Interview for DSM-IV Axis I Disorders – Patient Edition. New York: Biometrics Research Department, New York State Psychiatric Institute; 2001. [Google Scholar]
- 40.Pope HG, Katz DL. Psychiatric effects of exogenous anabolic-androgenic steroids. In: Wolkowitz OM, Rothschild AJ, editors. Psychoneuroendocrinology: The scientific basis of clinical practice. Washington, DC: American Psychiatric Press; 2003. pp. 331–358. [Google Scholar]
- 41.Pope HG, Kanayama G. Can you tell if your patient is using anabolic steroids? Curr Psychiatry Prim Care. 2005;1:28–34. [Google Scholar]
- 42.Weiner RB, Wang F, Isaacs SK, Malhotra R, Berkstresser B, Kim JH, Hutter AM, Jr, Picard MH, Wang TJ, Baggish AL. Blood pressure and left ventricular hypertrophy during American-style football participation. Circulation. 2013;128:524–531. doi: 10.1161/CIRCULATIONAHA.113.003522. [DOI] [PubMed] [Google Scholar]
- 43.Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, Flachskampf FA, Foster E, Goldstein SA, Kuznetsova T, Lancellotti P, Muraru D, Picard MH, Rietzschel ER, Rudski L, Spencer KT, Tsang W, Voigt JU. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28:1–39 e14. doi: 10.1016/j.echo.2014.10.003. [DOI] [PubMed] [Google Scholar]
- 44.Nagueh SF, Smiseth OA, Appleton CP, Byrd BF, 3rd, Dokainish H, Edvardsen T, Flachskampf FA, Gillebert TC, Klein AL, Lancellotti P, Marino P, Oh JK, Popescu BA, Waggoner AD. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2016;29:277–314. doi: 10.1016/j.echo.2016.01.011. [DOI] [PubMed] [Google Scholar]
- 45.Maurovich-Horvat P, Ferencik M, Bamberg F, Hoffmann U. Methods of plaque quantification and characterization by cardiac computed tomography. J Cardiovasc Comput Tomogr. 2009;3(Suppl 2):S91–98. doi: 10.1016/j.jcct.2009.10.012. [DOI] [PubMed] [Google Scholar]
- 46.Hoffmann MH, Shi H, Schmitz BL, Schmid FT, Lieberknecht M, Schulze R, Ludwig B, Kroschel U, Jahnke N, Haerer W, Brambs HJ, Aschoff AJ. Noninvasive coronary angiography with multislice computed tomography. JAMA. 2005;293:2471–2478. doi: 10.1001/jama.293.20.2471. [DOI] [PubMed] [Google Scholar]
- 47.Hartgens F, Rietjens G, Keizer HA, Kuipers H, Wolffenbuttel BH. Effects of androgenic-anabolic steroids on apolipoproteins and lipoprotein (a) Br J Sports Med. 2004;38:253–259. doi: 10.1136/bjsm.2003.000199. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.